
MULTI-MODAL PLATFORM FOR IN-HOME HEALTHCARE
MONITORING (EMUTEM)
Wided Souidene, Dan Istrate, Hamid Medjahed
ESIGETEL – LRIT, 1,Rue du Port de Valvins, 77210 Avon, France
Jérôme Boudy, Jean-Louis Baldinger, Imad Belfeki, François Delavault
EPH/Telecom Sud Paris, 9, Rue Charles Fourier, 91011 Evry, France
François Steenkeste
INSERM U558 Toulouse France
Keywords: Telemedicine, Design and development methodologies for Healthcare IT, Interoperability, Semantic
interoperability, Databases and datawarehousing, Datamining, Support for clinical decision-making,
Wearable health informatics.
Abstract: This paper describes a multimodal platform dedicated to in-home healthcare monitoring. This platform
consists in three heterogeneous and complementary systems which are designed to provide a sense of safety
and connectedness for those being monitored. In this article we present a detailed description of the multiple
sensors used to remotely monitor elderly or a patient health. These are: a set of microphones suitably placed
in the home, a wearable device and a set of infrared sensors. This platform is remotely used by the medical
staff in order to help them to take the right decision about the patient and/or elderly situation. It has a couple
of great advantages. First, its good acceptance by the end-users since it is less intrusive than other healthcare
systems. Second, it is reliable and robust since it performs the fusion of outputs of three complementary
healthcare systems.
1 INTRODUCTION
The proportion of elderly is increasing in all
societies throughout the world. As they are
becoming older, they want to preserve their
independence, autonomy and way of life. It is
therefore our duty of scientists to provide the
necessary devices to allow them to live at home
while being safe and in good condition. Thus,
several research teams have developed a number of
systems for in-home healthcare monitoring and
prevention towards day life risks. These systems are
based on the deployment of several sensors in the
care receiver home in order to prevent and/or detect
critical situations. They offer the comfort and
independence of staying at home, the security of
daily monitoring and proper medical attention.
However, there are few reliable systems capable of
preventing critical situations of the elderly before it
takes place. In particular, rare or not reliable are the
systems which predict or detect the fall of the person
with good sensitivity and good specifity.
To provide one answer to this problem, we
assembled a group of researchers from different
background within a consortium (QuoVADis Cf.
Acknowledgment) in order to develop a platform for
several uses and to meet the needs identified above.
The platform developed within this project manages
a system consisting in:
A set of microphones disposed into the
living rooms of the home of the elderly.
A portable device that can measure
ambulatory pulse heart rate, detect posture
and possibly the fall of the person
equipped.
A set of infrared sensors that detect the
presence of the person in a given home part
381
Souidene W., Istrate D., Medjahed H., Boudy J., Delavault F., Baldinger J., Belfeki I. and Steenkeste F. (2009).
MULTI-MODAL PLATFORM FOR IN-HOME HEALTHCARE MONITORING (EMUTEM).
In Proceedings of the International Conference on Health Informatics, pages 381-386
DOI: 10.5220/0001780603810386
Copyright
c
SciTePress
and also the standing posture of the person
in question.
The output of these three heterogeneous systems
are collected, processed and fused through a
multimodal platform (EMUTEM).
In this article, we propose a detailed description
of the multimodal platform called EMUTEM which
could have several uses among them Telemedicine,
healthcare and monitoring. This platform provides a
sense of safety and connectedness for those being
monitored. It also reassures the care-receiver family
and gives them some peace of mind. It could also be
arguably less expensive than the cost of live-in
helpers and caregivers. The proposed platform
collects and analyses the output of three distinct
systems and makes a fusion of 3 modalities in order
to help medical staff to take the right decision about
the monitored person situation.
In the following, we describe in section 2 the
operation of each system above and we detail the
configuration of the EMUTEM platform. In Section
3, we analyze the process of data acquisition.
Finally, we present our findings and perspectives.
2 MULTI-MODAL PLATFORM
FOR IN-HOME HEALTHCARE
MONITORING
It was found that the fall is one of the major causes
of death among the elderly. In France, people aged
65 and over are victims each year of 550 000
accidents with recourse to emergencies. They
account for more than three-quarters to 20 000
deaths annually from Normal Day Life Accidents
(NDLA). A large majority of these NDLAs are the
result of falls.
Faced with this scourge identified as hazardous
to health, safety and lives of the elderly, we tried to
develop a system of in-home healthcare monitoring
to prevent and detect a fall. We brought together the
efforts of three teams to establish a multimodal
platform. The platform manages three heterogeneous
systems: a sound system, a portable device and
infrared sensors.
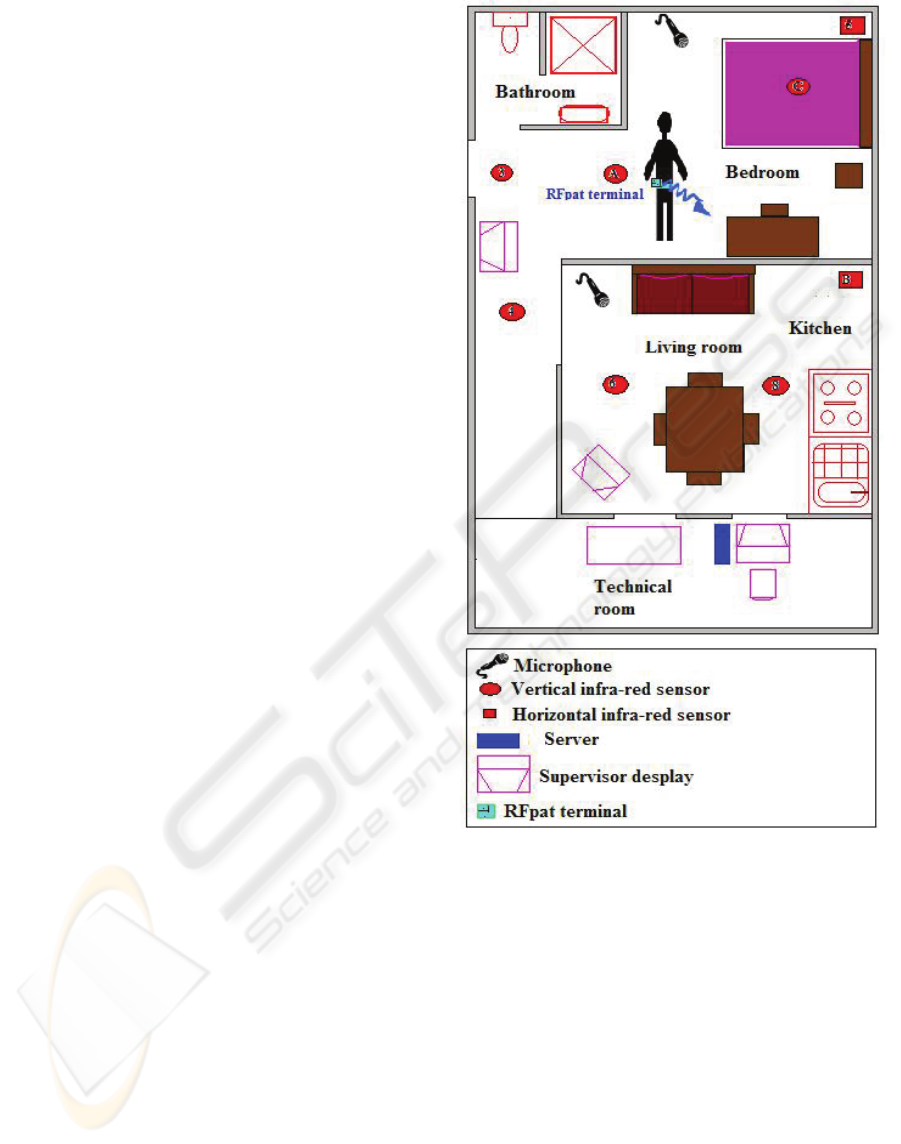
Figure 1 shows a proposed set of
sensor to be installed at home.
In the following each one of these systems will
be described and its contribution to the whole
healthcare monitoring system will be emphasized.
Figure 1: In-home sensor disposal.
2.1 The Wearable Device (RFPAT)
The wearable device named RFPAT consists in two
fundamental elements (Figure 2):
A mobile terminal: This is a waist wearable
device that the patient or the elderly clips,
for instance, to his belt all the time he is at
home. It measures the person’s vital data
and transmits to a reception home station.
In this article we will use the
denominations wearable device, mobile
device, mobile terminal indifferently to
address the mobile terminal.
A fixed reception base station: This is a
receiver connected to a personal computer
HEALTHINF 2009 - International Conference on Health Informatics
382
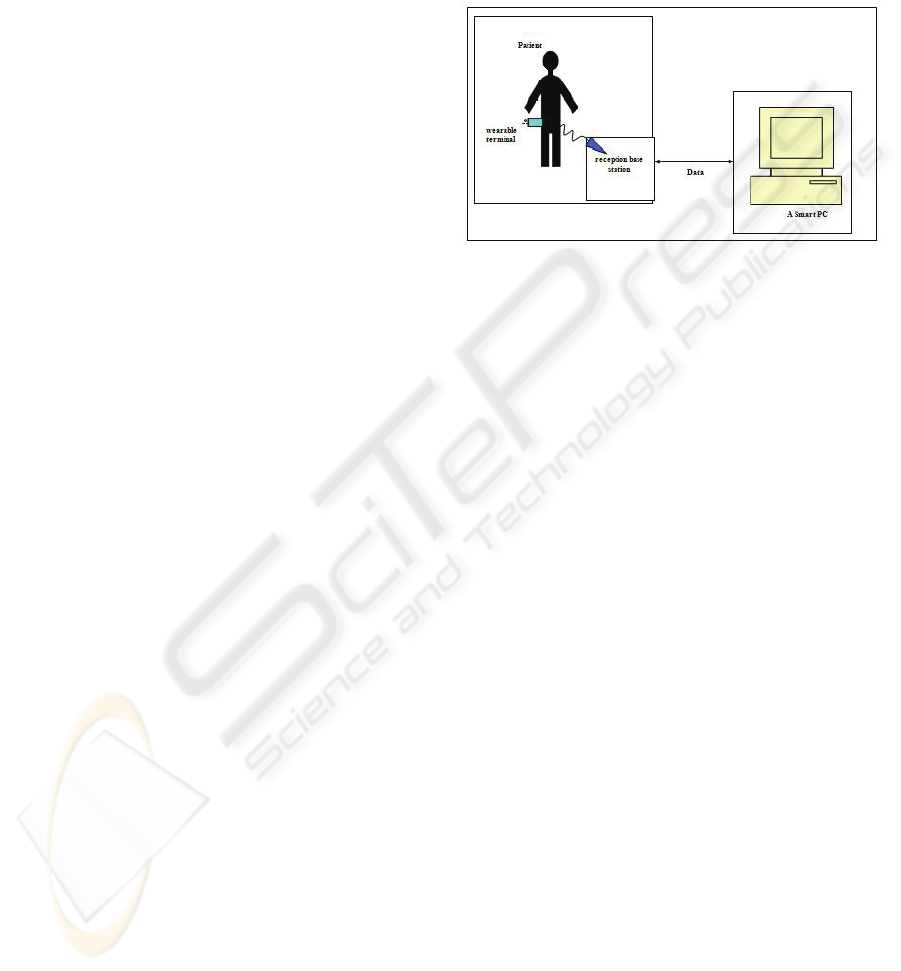
(PC). It receives vital signals from the
patient’s mobile terminal,
All the data gathered from the different RFPAT
sensors are processed within the wireless wearable
device. To ensure an optimal autonomy for the
latter, we designed it using low consumption
electronic component
s. Namely, the circuit
architecture is based on different micro-controllers
devoted to acquisition, signal processing and
emission. Hence, the mobile wearable terminal
encapsulates several signal acquisition and
processing modules:
It records various physiological and
actimetric signals
It pre-processes the signals in order to
reduce the impact of environmental noise or
user-motion noise.
This latter point is an important issue for in-
home healthcare monitoring. In fact, monitoring a
person in ambulatory mode is a difficult task to
achieve.
For the RFPAT system, we made the choice to
come up with the noise problem in the acquisition
stage. Then, some digital noise reduction filters and
algorithms were implemented within the portable
device. These filters and algorithms were applied
respectively to all acquired signals: movement data,
posture data and namely the pulse signal (heart rate).
Movement data describes the movement of the
monitored person. It gives us information like: ‘she
is lying’, ‘she is immobile’, ‘she is sitting/standing
up’ etc. Movement data consists also in the
percentage of movement, it computes the total
duration of the movements of the monitored person
for each time slot of 30 seconds (0 to 100% during
30 seconds). The posture data is information about
the person posture: standing up / laying down.
The posture data is a quite interesting
measurement which gives us useful information
about the person’s activity. Thanks to an actimetric
system embedded in the portable device, we can
detect the situations where the person is approaching
the ground very quickly. This information is
interpreted as a ‘fall’ when the acceleration goes
through a certain threshold in a given situation.
The pulse signal is delivered by a
photoplethysmographic sensor connected to the
wearable device. After pre-conditioning and
algorithmic denoising it gives us information about
the heart rate every 30 seconds.
In the ambulatory mode, the challenging process
consists in noise reduction. In (Baldinger, et al.
2004) we afford to reduce the variations of pulse
measurement lower than 5% for one minute
averaging, which remains in conformity with the
recommendations of medical professionals.
Data gathered from the different sensors are
transmitted, via an electronic signal conditioner, to
low power microcontroller based computing unit,
embedded in the mobile terminal.
Figure 2: RFPAT module configuration.
Currently, a fall-impact detector is added to this
system in order to make the detection of falls more
specific.
2.2 The Smart Sound Sensor
In-home healthcare devices face a real problem of
acceptance by end users and also caregivers. Sound
sensors are easily accepted by care receivers and
their family, they are considered are less intrusive
then cameras, smart T-shirts, etc… In order to
preserve the care-receiver privacy while ensuring his
protection and safety, we propose to equip his house
with some microphones. In this context, the
environmental sound is not continuously recorded.
This microphone array allows sound remote
monitoring of the acoustical environment of the
monitored person. The main advantage of this
system consists in carrying in real time (Istrate, et al.
2006a). Hence, we continuously ‘listen’ to the sound
environment in order to detect distress situations and
distress calls. This smart sound sensor described in
(Istrate, et al. 2006b) is made up four modules as
depicted in
Figure 3.
2.2.1 M1 Module: Sound Event Detection
and Extraction
The first module M1 listens continuously to the
sound environment in order to detect and extract
useful sounds or speech. The signal extracted by the
M1 module is processed by M2 module.
MULTI-MODAL PLATFORM FOR IN-HOME HEALTHCARE MONITORING (EMUTEM)
383

2.2.2 M2 Module: Sound/Speech
Classification Module
The second module M2 is a low-stage classification
one. It processes the sound received from module
M1 in order to separate the speech signals from the
sound ones.
Figure 3: ANASON smart sensor.
2.2.3 M3 Module: High-stage Classification
This module operates within each class determined
by the M2 module. It consists in two sub-modules.
In the case of sound label attributed to the signal by
module M2, the sound recognition sub-module M3.1
classifies the signal between eight predefined sound
classes. In case of speech label, the extracted signal
is analyzed by a speech recognition engine in order
to detect distress sentences (M3.2 module).
For both cases, if an alarm situation is identified
(the sound or the sentence is classified into an alarm
class) this information is sent to the data fusion
system. This is done in order to check whether the
other sensors (RfPat and Gardien) detected or not an
alarm.
2.3 The Infrared Motion Sensor
(GARDIEN)
The in-home healthcare monitoring systems have to
solve an important issue of privacy. When
developing our multi-modal platform, we chose the
monitoring modules such that they have the less
intrusive incidence on the monitored elderly
(Banerjee et al., 2003). We equipped our test
apartment with infrared sensors which have two
functionalities:
Localize the person at home: the sensors
are activated by the presence of the person
in a certain room. Only the living rooms
and the bedroom are equipped.
Detect the vertical position of the person: A
specific infra-red sensor is installed in the
living room and/or the kitchen in order to
detect whether the monitored person is
standing up or not. Actually it detects
movement in a fixed altitude of one meter
and a half.
Figure 4: GARDIEN system.
The second functionality is quite useful in order
to confirm or infirm a fall detection from the RFpat
or the ANASON module. These sensors and the
software and hardware which is used to perform the
localization and the vertical position detection is
called GARDIEN (Steenkeste. et al., 1999). Figure 4
represents the GARDIEN system.
2.4 General Interface of the
Multimodal Platform (EMUTEM)
In order to configure and manage the three
modalities above described, we developed a
platform which has different functionalities and that
could be easily used by a caregiver or even by
several members of the monitored person family.
Now, this platform is only used to control and
synchronise the different data acquisition processes.
The front panel of the developed platform is
presented in Figure 5.
HEALTHINF 2009 - International Conference on Health Informatics
384
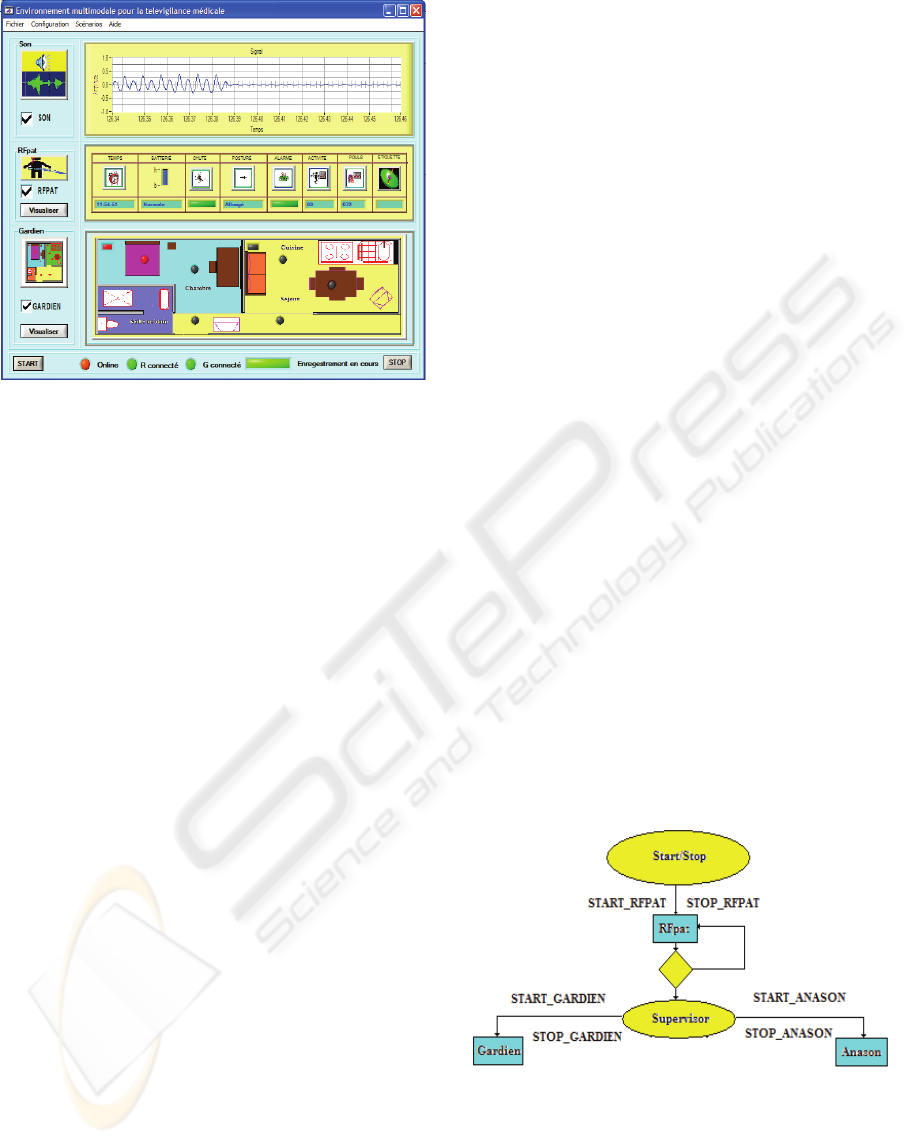
Figure 5: EMUTEM platform front panel.
Thanks to this platform, the platform manager
can supervise the multimodal data acquisition stage.
The platform manager must first select the
modality to record and then configure its parameters
if needed. For RFpat and Gardien systems, we only
need to specify the IP address and the TC/IP port
number. For ANASON sensor, we need to select the
sound card to be used for data analysis and recording
(if several ones are available). We also specify the
sampling rate and the location of the backup file. For
a final target use, this configuration is only done
once during the very first time the system is installed
in the patient’s or the elderly home.
3 DATA ACQUISITION
3.1 Data Acquisition Protocol
Data acquired using the different systems described
below is stored on the embedded Master PC within a
folder which has a specific name. For our case, we
attribute to the folder a name which is an
identification code number for the patient. Each
recording consists in five files corresponding to the
different modalities. These files are:
A personal table named personnel.xml,
contains the patient’s identifier and some
personal information like age, native
language, usual drugs treatment...etc. All
these data relative to the care-receiver are
protected for his privacy and their use and
transmission is let to his agreement.
A descriptive file named scenario.xml,
describes the reference scenario. This file is
stored during the test phase of the platform.
It is used further to analyse the performance
of each modality.
A sound file which contains sound data
saved in real time, in a wav file with 16 bit
of resolution and a sampling rate of 16
KHz, a frequency usually used for speech
applications.
A clinical data file which contains
physiological and motion data acquired
from RFpat. It stores information about
patient’s posture (laid down or
upright/seated), his agitation (between 0%
and 100%), his cardiac frequency, fall
events and emergency calls. The
acquisition sample rate is 0.03 Hz.
A motion data file acquired every 500 ms
by Gardien subsystem and saved in a
separate text adapted file format. Each line
of this file contains the infra-red sensors
which are excited (they are represented by
hexadecimal numbers from 1 to D) and also
the corresponding date and hour.
As the acquired signals corresponding to the
different modalities (ANASON, RFpat and Gardien)
have different sample rates, we developed a
synchronisation procedure in order to make the
acquisition protocol synchronous. This operation is
depicted on
Figure 6. It uses the TCP/IP Protocol.
The RFpat modality is launched first, because of his
low acquisition rate. Then, supervisor software
launches Gardien and Anason applications with
TCP/IP commands (Figure 6).
Figure 6: Synchronisation operation between our three
proposed modalities.
3.2 EMUTEM Database Recording
In order to precisely evaluate the performance of
EMUTEM platform, we first use it to record a
MULTI-MODAL PLATFORM FOR IN-HOME HEALTHCARE MONITORING (EMUTEM)
385

multimodal medical database. Our multimodal
database acquisition software described below
provides a very helpful and well-targeted application
to elaborate and assess the data fusion-based
decision methods. The low level data recorded by
our system will be useful for the development of
each modality processing algorithms and their
combination strategies.
In order to index our multimodal database, we
have retained the SAM standard indexing file (Well,
et al., 1992) generally used for Speech Databases
descriptions. The SAM labelling of a sound file
indicates information about the file and describes it
by delimiting the useful part to be used for file
content analysis and processing. For each modality
of the database a corresponding indexation file is
created, we have adapted this type of files to the
specificity of each modality, and we have added
another indexation file for the entire database. This
conceptual indexation model is guided by a-priori
knowledge and the reference scenarios. This aims to
obtain the reference information for our Multimodal
Database, and therefore to generate a novel type of
database to validate different modality signal
processing techniques and approaches of multimodal
data fusion algorithms.
Nowadays, we have enriched our database with
several scenarios played by actors. We already have
the permission of a smart home designer to install
our platform in his facilities which are apartments
with elderly people living in. This will allow us to
better evaluate our developed system and record real
data.
4 CONCLUSIONS AND FUTURE
WORK
During this first step of our collaborative research
work, we developed a multimodal platform which
performs in-home healthcare monitoring and
especially distress situation detection and prediction.
We put together three different modalities in order to
ensure elderly person security in comfortable, non-
intrusive way. We propose a wearable device able to
acquire and process physiological signals, a smart
sound sensor which analyses the environmental
home sounds in order to detect distress situations
and sentences and an infrared sensor array which
localizes the person at home and detects her vertical
position.
Nowadays, we are developing several techniques
in order to fuse different inputs of these systems.
Our ultimate target is to make this in-home
healthcare system more robust towards false alarms
and non detected hazardous situations. This platform
could help medical staff to take the right decision
about the person situation even if they are distant.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the contribution
of French National Research Association (ANR),
QuoVADis Project.
REFERENCES
Baldinger, J., Boudy, J., Dorizzi, Levrey, J., Andreao, R.,
Perpre, C., et al. (2004). Tele-surveillance system for
patient at home: The medeville system. ICCHP.
Banerjee, S., Steenkeste, F., Couturier, P., Debray, M., &
Franco, A. (2003). Telesurveillance of elderly patients
by use of passive infra-red sensors in a smart home.
Telemed-Telecare.
Istrate, D., Castelli, E., Vacher, M., Besacier, L., &
Serignat, J. (2006a). Information extraction from
sound for medical telemonitoring. IEEE Trans. on
Information Technology in Biomedecine, (pp. 264-
274).
Istrate, D., Vacher, M., & Serignat, F. (2006b). Generic
implementation of a distress sound extraction system
for elder care. IEEE EMBS, (pp. 3309-3312). New
York.
Reynolds, D. (1995). Speaker identification and
verification using gaussian mixture speeker models.
Speech Communications , 91-108.
Schwarz, G. (1978). Estimating the dimension of a model.
Annals of statistics , 461-464.
Steenkeste, F., Bocquet, H., Chan, M., & Vellas, B.
(1999). Remote monitoring system for elders in a
geriatric hospital. International Conference on aging.
Arlington.
Well, D., Barry, J., Grice, W., Fourcin, M., & Gibbon, A.
(1992). SAM ESPRIT PROJECT2589-multilingual
speech input/output assessment, methodology and
standardization. University College London: Final
report. Technical Report SAM-UCLG004.
HEALTHINF 2009 - International Conference on Health Informatics
386
