
EXTRACTION OF FETAL ECG FROM ABDOMINAL SIGNAL
D. V. Prasad and R. Swarnalatha
Department of Electronics & Instrumentation Engineering, BITS, PILANI, Dubai, U.A.E.
Keywords: fECG, mECG, TECG, Adaptive filtering.
Abstract: Fetal ECG monitoring is essential for identification of fetal distress. The assessment of the QRS waveform
of fetal ECG is good analysis tool. Extraction of fetal ECG from abdominal signals is difficult. This paper
presents a method for extracting fetal ECG (FECG) from composite abdominal signal. This method is
applied to composite abdominal signal containing maternal ECG and fetal ECG. Adaptive filtering
techniques along with denoising techniques were used to extract fECG. This method leads to enhancement
of fetal ECG by cancelling maternal ECG. The results were validated using real signals. The thoracic signal
is purely that of mother (mECG) while the abdominal signal contains both mothers and fetus ECG signals
(mECG + fECG). The results clearly show the effectiveness of the method in extracting fECG.
1 INTRODUCTION
The fetal electrocardiogram (FECG) is the electrical
activity of the fetal heart and first demonstration was
carried out in 1906 by Cremer (Jenkins, 1986). Fetal
electrocardiogram fECG provides clinically
significant information about the physiological state
of a fetus. Anoxia is known to alter the balance
between the electrical polarization and repolarization
of the heart. Similarly arrhythmias show the
maturity of fetal cardiac activity (Symonds EM,
Sahota T, and Chang A, 2001). Many experiments
were performed using invasive techniques to record
fECG. Non invasive techniques appeared in the
seventies. These methods use recorded signals from
maternal abdominal wall. These signals contained
not only maternal electrocardiogram (mECG) but
also fetal ECG (fECG) and other signals. The
maternal signal level is much higher than fetal ECG
and hence has to be suppressed from the composite
signal. With advent of technology and analysis tools
many methods of maternal ECG suppression were
developed.
Adaptive filtering was used with thoracic
signals as the reference inputs, combined to cancel
the maternal ECG in the abdominal signals (Widrow
et al, 1975). A weighted addition of four or more
abdominal signals was calculated to suppress the
maternal ECG (Bergveld P and Meijer JH, 1981).
Singular value decomposition was used successfully
to separate maternal ECG and fetal ECG (Callaerts
D, De Moor B, Vanderwalle J and Sansen W, 1990).
Blind source separation algorithms have also been
applied to extract fECG (Zarcoso and Nandi A K,
2001).
Fetal ECG contains information about the health
status of the fetus. It gives an early diagnosis of any
cardiac defects before delivery (Mazzo J R, 1994).
Non invasive techniques of fetal monitoring are
Doppler ultrasound, fetal electrocardiography and
fetal magneto cardiography. Among these methods
the most commonly used is Doppler ultrasound.
However this method produces an averaged heart
rate and therefore cannot give beat to beat
variability. This method cannot provide
electrophysiological information such as
arrhythmias. Fetal electrocardiogram offers the
advantage of monitoring beat to beat variability.
(Fukushima T, Flores CA, Hon EH, Davidson EC,
1985). There are many technical problems with non
invasive extraction of fECG. The fECG signal is
corrupted by different sources of interferences such
as maternal EMG, 50 Hz power line interference and
base line wander. The low amplitude of the signals,
the different types of noise and overlapping
frequencies of mother and fetal ECG make the
extraction of fECG a difficult task (Godddard B A,
1966). Projective filtering techniques were also used
to extract fetal ECG (Kotas M, 2007)
The fetal heart rate variations during pregnancy
and labour have been used as an indirect indicator of
fetal distress. Observation over longer periods may
245
Prasad D. and Swarnalatha R. (2009).
EXTRACTION OF FETAL ECG FROM ABDOMINAL SIGNAL.
In Proceedings of the International Conference on Bio-inspired Systems and Signal Processing, pages 245-248
DOI: 10.5220/0001510502450248
Copyright
c
SciTePress

yield more information about the status of the fetus.
The detection of fetal QRS complex on surface
records is very difficult task which is mainly due to
overlapping of mothers ECG. The mECG and fECG
are partly uncorrelated. Also the mECG signal is
very much stronger than the fECG signal embedded
in it. The noise in which fECG is embedded is also
stronger depending on the gestation age.
In this paper an improved method of extracting
the P QRS T waves of the fetal ECG from composite
abdominal signal is proposed. The proposed method
uses cancellation of mothers ECG and denoising
methods to improve the extracted signal quality.
Real abdominal signals were used to test the
algorithm.
2 METHOD
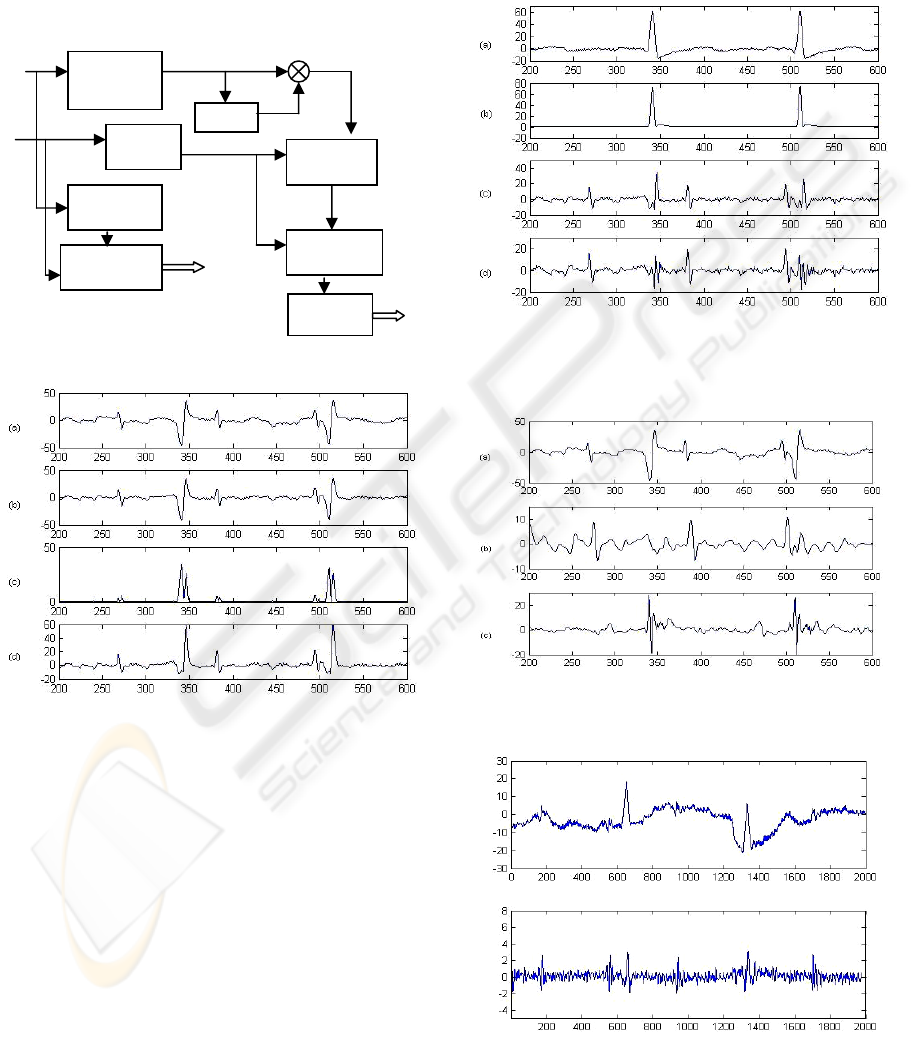
The block diagram of the proposed algorithm is
shown in Fig 1. The proposed method detects fetal
QRS wave by preprocessing and denoising of
abdominal ECG (AECG) and subsequent
cancellation of maternal ECG in the abdominal
ECG. The thoracic signal (TECG) which is mECG is
used to cancel mECG and the fetal ECG detector
extracts the fECG. This method uses multistage
adaptive filtering.
2.1 Preprocessing
The preprocessing consists of the following steps
(Prasad DV, Swarnalatha R, 2007).
(a) Read the abdominal ECG
(b) Separate the high resolution components
and low resolution components
(c) Compensate for the phase
(d) Derive the noise component
(e) Separate the noise from the original signal
(f) Reconstruct the signal back
(g) Repeat the construction iteratively.
The high resolution components are the components
which are well defined in the abdominal signal.
These are the maternal QRS wave having large
amplitude and the fetal ECG whose amplitudes are
much smaller than maternal ECG. The low
resolution components are the components which do
not directly contribute to the fetal ECG or maternal
ECG.
2.2 Material
The testing of the algorithm was done by using data
from SISTA/DAISY and Physionet. The data from
SISTA/DAISY has abdominal data of 5 channels
and thoracic data of 3 channels. Physionet has 2
channels of thoracic signals and 4 channels of
abdominal signals. However for verification of the
algorithm only one channel of abdominal signals
was used. The gestation period varies from 22 to 40
weeks. DAISY data and Physionet data have
different sampling frequencies. The algorithm has
been tested with both the data.
2.3 Fetal QRS Detection
The aim of the algorithm is to enhance the fetal ECG
by suppressing the other components of the signal.
The enhanced signal contains mostly fetal ECG and
EMG noise. The proposed method detects fetal QRS
waves by canceling the maternal ECG.
Fetal ECG
detection was done by improving signal to noise
ratio (SNR) of fetal QRS complex to the other
components of the signal using a nonlinear operator
defined by equation 1. This reduces the maternal P
and T waves. The operator is defined as follows.
Ψ = DS (DS-1) (1)
where DS is the preprocessed and denoised signal
obtained from the original abdominal ECG. Fig 2 (a)
shows the abdominal signal to be analyzed and the
maternal ECG recorded from thoracic region is
shown in Fig 3(a). Fetal ECG can be extracted by
direct application of blind source separation (BSS)
(De Lathauwer L, De Moor B, and Vanderwalle J,
2000). However such methods fail to give precise
extraction. In order to reduce the mothers ECG
effects on extraction, mECG was eliminated by
using two stage adaptive filtering. The reference
signal taken is shown in Fig 3(b) which is the
squared signal of the thoracic signal corresponding
to mECG Fig 3(a).The advantage of this method is
that the reference signal need not closely mimic the
signal to be cancelled. If such a reference signal
could be generated, than this method can be applied
where only the mothers ECG is available. The
adaptive filter used behaves as an exponential
averager (Laguna P, Jane R, Meste et al, 1992).
The output of the adaptive filter 1 is again adaptive
filtered with (TECG)
2
to obtain the signal shown in
Fig 3(d).To obtain better results the adaptive filter
design plays an important role. The selection of the
step size of the adaptive filter is very important as
the signal to be extracted is highly sensitive to the
BIOSIGNALS 2009 - International Conference on Bio-inspired Systems and Signal Processing
246
step size. The resultant signal depends on the value
for the constant of adaptation. The output 3(d) is
applied to fECG detector and extracted fECG and
mECG are shown in Fig 4(b) and 4(c). The signal
quality is high enough to recognize fetal QRS
complexes.
Figure 1: Block Diagram of the proposed algorithm.
Figure 2: (a)Original abdominal ECG (b) Preprocessed
signal (c) Square of preprocessed signal (d) signal
obtained after adding b and c.
3 RESULTS
The proposed algorithm was assessed by using real
composite signal comprising of mECG and fECG.
The noise is to due to mother’s electromyogram
activity. The performance of the method is seen
from the extracted waveforms centering on R wave
peak. The P and T waves can also be seen. Fig 4
gives the extracted fECG and mECG. Fig 6 shows
the power spectrum of the original signal and the
extracted fECG and mECG. The results show that
the P, R and T waves are clearly visible in the
extracted signals. Two cases have been studied. Case
1 has a sampling rate of 250 samples/sec and case 2
has a sampling rate of 1000 samples/sec. Fig 4a
shows the results for case 1 and Fig 5b shows the
results for case 2.
Figure 3: (a) Thoracic ECG (b) square of Thoracic ECG
(c) Output of Adaptive filter 1 (d) Output of Adaptive
filter 2.
Figure 4: (a) Original abdominal ECG of patient 1 (b)
Extracted fECG (c) Extracted mECG.
Figure 5: (a) Original abdominal ECG of patient 2 (b)
Extracted fECG.
AECG
DS
2
+
(TECG)
2
TECG
Adaptive
Filter 1
Adaptive
Filter 2
Cancelling
mECG
fECG
detecto
r
Adaptive
Filter 1
Adaptive
Filter 2
mECG
Preprocessin
g &
Denoising
FECG
Ψ=DS (DS-1)
Denoised
signal (DS)
-
EXTRACTION OF FETAL ECG FROM ABDOMINAL SIGNAL
247
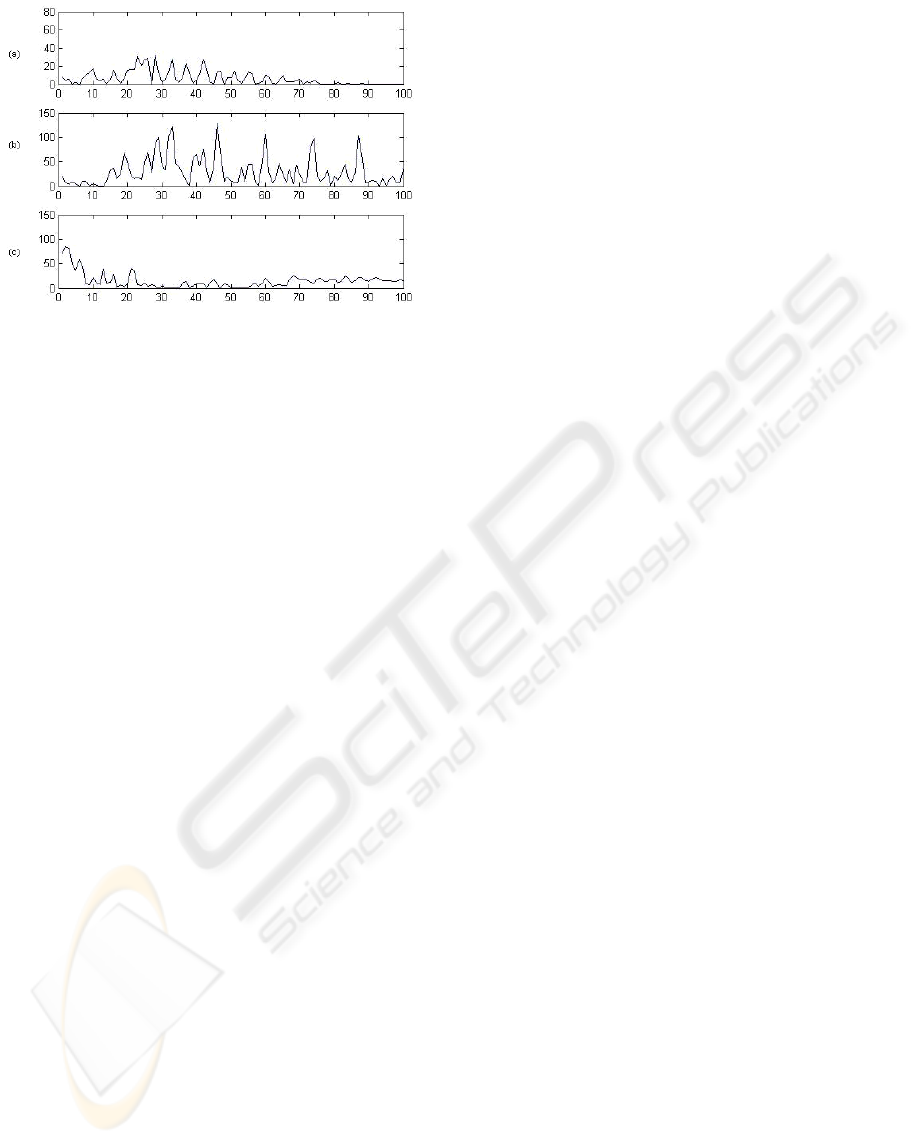
Figure 6: Power spectrum of (a) Original Abdominal ECG
(b) Extracted fECG (c) Extracted mECG.
4 CONCLUSIONS
Fetal ECG extraction with out disturbing the
morphology is a difficult task. The limitations of
conventional methods led to the design of this
extraction system which improves the estimate the
fetal ECG and maternal ECG. A two stage adaptive
filter system is shown to retrieve fetal ECG from
actual patients maternal ECG. It is not easy to see
how well the fECG extraction is
achieved by
looking at a large number of samples. Thus a frame
of 400 samples is taken for patient 1 and 2000
samples for patient 2, to illustrate the effectiveness
of the algorithm. In this frame there are both
overlapping and non overlapping between maternal
and the fetal components in the abdominal signal.
This is a significant challenge to the extraction
algorithm. The results show that the algorithm was
able to successfully extract the fECG signal. It can
be noted the visual quality of the extracted fECG is
much better. The advantage of this method is that
the reference signal need not closely mimic the
signal to be cancelled. The algorithm was able to
reveal complete fetal ECG such QRS complex, its
shape and duration. This also allows for beat to beat
detection of the fetal R waves. This feature allows us
to investigate fetal heart rate fluctuations. This
feature of the algorithm can be used in early stages
of pregnancy. Consequently, it is possible to
understand the fetal heart rate fluctuations as a
function of gestational time. The algorithm was able
to overcome noise due to sources such as maternal
muscle activity, uterine contractions and external
electrical interference.
ACKNOWLEDGEMENTS
The authors would like to thank Prof. M.
Ramachandran, Director, BITS, Pilani-Dubai for his
constant encouragement and support. We would also
like to thank Physionet.org and SISTA/DAISY for
the fetal ECG data.
REFERENCES
Bergveld P. and Meijer J. H, 1981, “A newtechnique for
the suppression of the MECG”, IEEE Trans. Biomed.
Eng, 28,348-354
Callaerts D., De Moor B., Vanderwalle J and Sansen W,
1990, “Comparision of SVD methods to extract the
foetal electrocardiogram from cutaneous electrode
signals”, Med. Biol. Eng & Comput, 28, 217-224
De Lathauwer L., De Moor D. and vanderwalle J., 2000,
“Fetal electrocardiogram extraction by blind source
subspace separation”, IEEE Trans. Biomed. Eng, vol
47, No 5, pp. 567-572
Fukushima T., Flores C. A., Hon E.H, Davidson E.C, Jr,
1985, “Limitationsof autocorrelation in Fetal heart rate
monitoring”, Am J Obstet. Gynecol.;153(6):685-92
Goddard B. A., 1996, “A clinical fetal electro-
cardiograph”, Med. Biol. Eng, vol 4, pp 159-167
Jenkins H. M. L., 1986, “Technical progress in fetal
electrocardiography – a review”, J Perinatal. Med.,
14, 365-370
Kotas M., 2007, “Projective filtering of time aligned beats
for foetal ECG extraction”, Bulletin of Polish
Academy of Sciences, vol 55, No 4
Laguna. P, Jane. R, Meste. O et al, 1992, “Adaptive
filter for event related bioelectric signals using an
impulse correlated reference input: comparision with
signal averaging techniques”, IEEE Trans. Biomed.
Eng., 39(10):1032-44
Mazzeo J. R., 1994, “Non invasive fetal
electrocardiography”, Med. Prog. Technol.,20
Prasad D. V., Swarnalatha R, 2007, “A new method to
detect subtle changes in ECG”, WACBE World
Congress on Bioengineering, Bangkok, Thailand.
Symonds E. M., Sahota D. and Chang .A, 2001, “Fetal
electrocardiography”, London, Imperial College
press.
Widrow B. et al, 1975, “Adaptive noise canceling:
principles and the applications”, Proc. IEEE, 63:1692-
1716
BIOSIGNALS 2009 - International Conference on Bio-inspired Systems and Signal Processing
248
