
NEWBORN’S
BIOMETRIC IDENTIFICATION: CAN IT BE DONE?
Daniel Weingaertner, Olga Regina Pereira Bellon, Luciano Silva
Department of Informatics, Universidade Federal do Paran
´
a, Curitiba, Brasil
M
ˆ
onica Nunes Lima Cat
Department of Pediatrics, Universidade Federal do Paran
´
a, Curitiba, Brasil
Keywords:
Identification, newborn, palmprint, footprint, dermatoglyph.
Abstract:
In this article we propose a novel biometric identification method for newborn babies using their palmprints.
A new high resolution optical sensor was developed, which obtains images with enough ridge minutiae to
uniquely identify the baby. The palm and footprint images of 106 newborns were analysed, leading to the con-
clusion that palmprints yield more detailed images then footprints. Fingerprint experts from the Identifcation
Institute of Paran
´
a State performed two matching tests, resulting in a correct identification rate of 63.3% and
67.7%, more than three times higher than that obtained on similar experiments described on literature. The
proposed image acquisition method also opens the perspective for the creation of an automatic identification
system for newborns.
1 INTRODUCTION
Identification of newborns is one of the main tasks of
the medical team following birth. Especially in devel-
oping countries like Brazil, where security in public
maternity wards is not very tight, and overcrowding
is common, the risks of a baby swap or kidnap are
above acceptable.
According to a speech by Police Officer Nilma
Azevedo (Azevedo, 2005), another frequent problem
is illegal adoption. Police Department of Pernam-
buco State is trying to increase controll over moth-
ers fingerprint verification, in order to avoid situa-
tions in which they enter the maternity using identi-
fication documents of another person, to which they
afterwards sell/give the newborn child.
Situations like these could be avoided, or strongly
reduced, if reliable and fast methods for identification
of newborns were made available and used inside ma-
ternities and hospitals, as well as on airports or bus
stations. Thus it is surprising that so little research
regarding newborn identification is published, while
biometric identification of adults receives so much at-
tention and funding.
There are a variety of commercially available
systems for adult biometric identification (Mainguet,
2007; Maltoni et al., 2003), but to the best of our
knowledge, there is not a single biometric system de-
veloped for identification of newborn babies, so that
most maternities still rely on bracelets and/or stamps
for this purpose. Most published articles about this
subject date from the beginning of the 20th century,
and usually only evaluate the usefullness of footprint-
ing with ink and paper, without new identifition meth-
ods proposals or evaluations.
The purpose of this article is to propose a novel
biometric identification method for newborn babies
using their palmprint. We make a survey of the new-
born identification techniques based on dactyloscopic
impressions and then present a newly developed digi-
tal sensing equipment capable of providing high defi-
nition images of the baby’s palms and soles. These
images, collected moments after the birth, can be
used by an expert for confrontation in case of identity
doubt and for the development of automatic identifi-
cation systems. They can also be used for confronta-
tion during the adult life of the individual.
Work on this project involved a multidisciplinary
team composed of computer scientists, medical doc-
tors, nurses and police officers. We are also grateful
for the parents that gave their consent to the testing of
the new equipment on their newborn babies.
200
Weingaertner D., Regina Pereira Bellon O., Silva L. and Nunes Lima Cat M. (2008).
NEWBORN’S BIOMETRIC IDENTIFICATION: CAN IT BE DONE?.
In Proceedings of the Third International Conference on Computer Vision Theory and Applications, pages 200-205
DOI: 10.5220/0001093302000205
Copyright
c
SciTePress

2 NEWBORN IDENTIFICATION
2.1 Fingerprints and Palmprints
Very few articles refering to the use of fingerprints or
palmprints on newborns were found. Worth mention-
ing is Sir F. Galton’s work (Galton, 1899) where he
presented a study of newborn fingerprinting with ink
and paper, concluding that fingerprints taken before
17 months after birth are not usefull for identication.
Morgan and Pauls (1939) presented a technique
for collecting palmprints of newborns, and stated that
they resulted in images good enough to be used for
identification, although no objective analysis of the
resulting images were provided, nor did they perform
a matching test to support their statement.
2.2 Footprints
Acquisition of newborns footprints at birth is used as
means of identification in many countries since the
beginning of the 20th century (Shepard et al., 1966;
Cat, 2003; Vaesken, 2006). Usually the footprints are
collected with ink spread on the foot with a cylinder
and then printed on the newborns’ medical record,
along with the mothers fingeprint. That way, it is
expected that any identity doubt about the baby or
his/her mother can verified.
Unfortunately, due to illegibility problems, the use
of these footprints for identification purposes is not
possible in the majority of cases. According to several
studies (Cat, 2003; Shepard et al., 1966; Pel
´
a et al.,
1975; Lomuto and Duverges, 1995; Thompson et al.,
1981), the main reasons for illegible footprints are:
• Use of inadequate materials (ink, paper, cylinder);
• Untrained personal for footprint acquisition;
• Baby’s skin covered with an oily substance;
• Reduced thickness of the newborn epidermis, eas-
ily deforming the ridges upon contact and filling
the valleys between ridges with ink;
• Reduced size of the newborns ridges, which are
three to five times smaller than on adults.
Montgomery (Montgomery, 1926) is the only au-
thor who said that he could get footprints of newborns
with clearly visible ridges, using a technique (not de-
scribed) developed (but not published) by Prof. J.H.
Mathews, of the Wisconsin University. He collected
footprints of 191 newborns, at one to seven days af-
ter birth, and most of them had visible ridges, allow-
ing him to classify the footprints using a system pro-
posed on the same article. Unfortunatelly this foot-
printing technique was not found on our revision, nor
any other reference to it.
After the beginning of the 20th century, there were
no new publications on techniques for obtaining good
newborn dactiloscopic prints. Most articles only eval-
uate footprinting with ink and paper, arguing about
their usefullness for identification purposes.
Wierschem (Wierschem, 1965) described a study
in which footprints collected by Chicago’s hospitals
(USA) were analysed, concluding that 98% could not
be used for identification. After providing trainment
and the right equipment to the medical team, a new
analysis of the collected footprints was performed,
showing that 99% allowed the newborn’s identifica-
tion. But this identification was not based on dactilo-
scopic ridges. It used the flexion creases of the foot,
which change during the first months of life.
Shepard et.al. (Shepard et al., 1966) collected
footprints of 51 newborns, one at birth and another
5 to 6 weeks after, sending the resulting 102 impres-
sions to the California State Justice Department of
Criminal Investigation and Identification (USA) for
analysis. There, expert fingerprint technicians anal-
ysed the sample and were only able to identify 10
babies, resulting in approximately 20% identifiable
footprints. However it was felt that the majority of
these 20 correctly matched prints would not stand up
under legal scrutiny in the courts.
Pel
´
a et.al. (Pel
´
a et al., 1975) made a large scale
analysis of footprints in order to verify their quality
and the usefulness of collecting them. They analysed
1,917 footprints collected during a year in a Brazil-
ian maternity ward, and concluded that none provided
details that could be used for identification purposes,
although they were collected by trained personel.
Thompson et.al. (Thompson et al., 1981) col-
lected 100 footprints of 20 newborns and verified that
only 11% where technically acceptable, and only one
footprint (1%) had all elements needed for a legal
identification. They also acquired the footprints of 20
premature babies weighting less than 1500g at birth.
Many prints were obtained from each baby: at birth
and then 4 to 8 weeks later, and the best pair of prints
were chosen for a matching attempt. Conclusion was
that none of these footprints were suitable for identi-
fication purposes.
Thus, most authors concluded that it is safe to
state that footprinting as currently done is not use-
ful for identification purposes, and that the acquisi-
tion of footprints should be abandoned because it only
generates unnecessary work and costs. These authors
also state that even with well-trained personnel, good
materials and appropriate techniques, it is impossi-
ble to obtain good footprints. A recent email discus-
sion between biometric researchers
1
also showed that
1
Biometric Consortium’s Electronic Discussion Group
NEWBORN’S BIOMETRIC IDENTIFICATION: CAN IT BE DONE?
201

it is considered to be impossible to obtain any dac-
tiloscopic impressions from newborns, because of in-
complete ridge formation, their skin being covered by
an oily substance and their extremely fragile ridges.
Besides footprinting, other identification methods
are also used, such as: bracelets, signals with chem-
ical solutions or ink, and the withdrawal of genetic
material to allow the DNA examination. The prob-
lem is that the bracelets or inks serve only for the pe-
riod of permanence of the child in the hospital unit,
and even during this period these IDs can be removed
or altered. On the other hand, the DNA examination
is proven to be efficient in the univocal identification
of individuals, but it comes at high cost and cannot
be used in real time applications, demanding sophis-
ticated laboratory procedures.
The use of the iris as identification feature, even
though it is increasingly used in adults (Bolle et al.,
2003), is a difficult method for newborns, especially
the premature, because they hardly open their eyes,
they do not have the ability of looking into a scanning
device, and touching their eyelids to collect an image
could hurt them. Besides, the iris pattern only stabi-
lizes after the child’s second year (Jain et al., 2004).
The format of the ear is a biometric feature of easy
acquisition, but possesses little discriminatory capac-
ity (Bolle et al., 2003; Victor et al., 2002) and changes
throughout the life of the individual.
Given the limitations of these and other identifica-
tion methods, the idea of using dermatoglyphic prints
continues to be very attractive, since it is a non in-
vasive method, of easy applicability, high availabil-
ity, wide acceptance and has effectively been used for
more than 100 years.
2.3 Ridges On Newborns
The ridges of the fingers, palms and soles of the hu-
man embryo are formed between the 12th and 16th
week of gestation, first appearing in the tip of the fin-
gers and finally in the sole of the feet. They do not
change in the subsequent months or during the adult
life of the individual (except in case of some illnesses
or physical wounds). After the 18th week of intrauter-
ine life the embryo has its ridges completely formed
and they become visible in the surface of the epider-
mis (Cummins and Midlo, 1943; Castellanos, 1953;
Holt, 1973; K
¨
ucken and Newell, 2005).
Despite being fully formed and invariant in num-
bers of lines, drawings or details (minutiae), ridges do
change in size throughout the growth of the child, be-
coming thicker and widening the gap between them
(biometrics@peach.ease.lsoft.com) on may/2005.
(Cummins and Midlo, 1943; Castellanos, 1953). Ac-
cording to Castellanos (1953), the ridges of the fingers
of newborns are 3 to 5 times smaller than in adults,
and are very fragile, easily deforming upon contact.
Figure 1 illustrates this difference showing the finger
of a newborn and an adult side by side.
Figure 1: Comparison between the forefinger of a newborn
and an adult.
The automated fingerprint identification systems
(AFIS) homologated by the FBI for use in adults de-
mand a minimum resolution of 500d pi (Maltoni et al.,
2003). As the ridges of adults measure, on average,
0.45mm − −0.5mm, its safe to assume that for new-
borns, whose ridges measure 0.1 − −0.15mm (Cum-
mins and Midlo, 1943; Castellanos, 1953), a resolu-
tion of at least 1500d pi is necessary.
3 FOOT/PALMPRINT IMAGES
ACQUISITION
In order to develop a new footprint acquisition
method, the first step was to appropriately prepare the
newborns’ skin, in order to remove the oily substance
covering it and provide a clean surface.
First tested was the traditional ink and paper
method: carefully collected footprints of newborns
were taken and analysed, with help from fingerprint
experts from the Identification Institute of Paran
´
a
State (IIPR). This test confirmed the knowledge that
very few prints show visible ridges, and none were
suitable for identification.
As a second step, some commercially available
optical finger/palmprint sensors, ranging from 250d pi
to 500d pi, were tested, but in neither case the images
obtained showed any usable ridge patterns.
The next attempt was to use a high resolution light
scanner to scan the babies sole and palm, in order to
VISAPP 2008 - International Conference on Computer Vision Theory and Applications
202
test if a greater resolution would yield better results.
Images were obtained at 1200d pi and 2400dpi.
However the scanned images were not deemed
suitable for large-scale utilisation, the reasons being:
firstly that the scanning process takes almost 2 min-
utes, during which the baby should not move his/her
foot/hand, or the image is corrupted. Secondly, the
scanned images have a low contrast, making it diffi-
cult to segment the valleys and ridges. And thirdly,
the pressure that has to be applied on the foot/hand to
keep it quiet cause blood vessels on the skin surface
to be emptied, reducing the contrast even further.
3.1 Optical Sensor for Newborn
Foot/Palmprints
To the best of our knowledge, and based on the dis-
cussion above, there is no available method or equip-
ment that allows the acquisition of high definition
palm/sole images from newborns. Furthermore, there
is no market-available equipment capable of satisfy-
ing this application’s requirements. We thus devel-
oped a sensor (Figure 2) consisting of a 8 megapixels
digital camera attached to a rectangular optical glass
prism, capable to generate images of approximately
1400d pi with a capture area of 35mm ×45mm.
Figure 2: Optical sensor with capture area of 35mm×45mm
and approximate resolution of 1400d pi, used to acquire
newborn palm and footprints.
The working principle of the sensor is the same
as other existing optical fingerprint sensors, based on
the total reflection characteristic of a prism. When a
palm or sole is placed on top of the prism’s inclined
surface, light is absorbed by the ridges touching the
prism, yielding dark points on the image, while at the
valleys light is reflected into the camera. This method
provides high contrast images, and the main advan-
tages of the developed sensor are its high resolution.
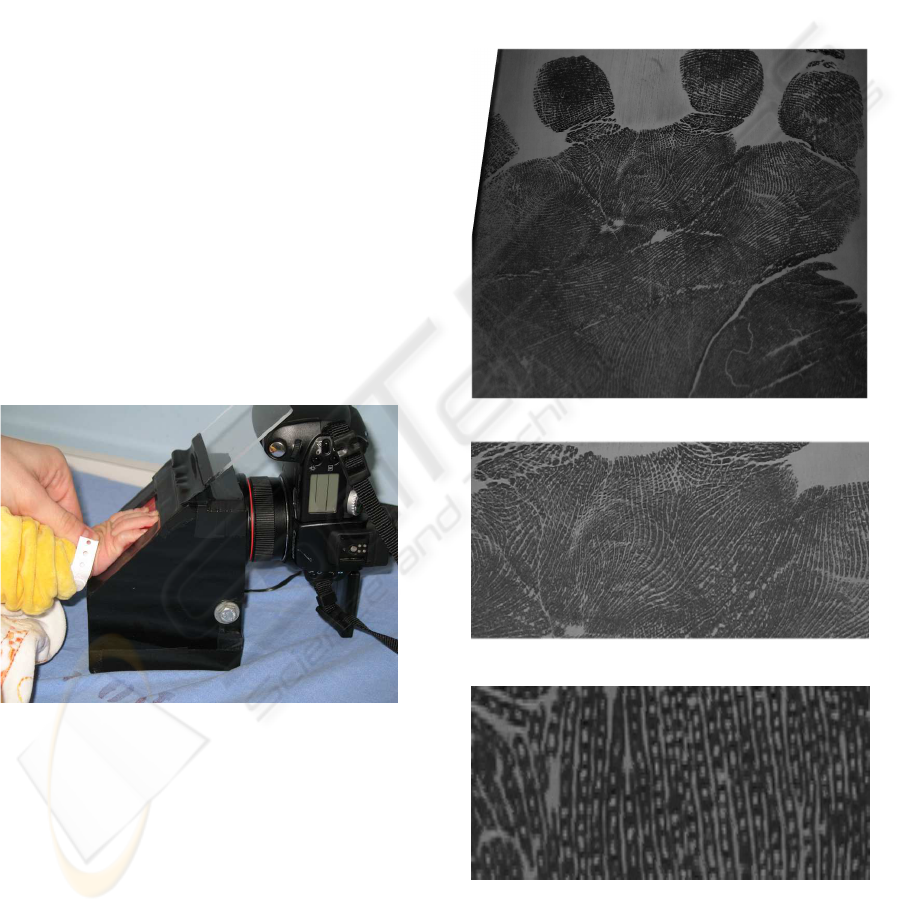
Acquisition of good quality images requires that
the newborns palm and sole be cleaned and mois-
turised. Figure 3a shows the image of a newborns
palm as provided by the sensor (after distortion cor-
rections). Figures 3b and 3c are magnifications of
that image for better visualisation. It is possible to ob-
serve well defined ridges and some pores. The ridges
are relatively close to each other (with narrow valleys)
due to deformation caused by the pressure applied to
the hand. But the image has the typical high contrast
obtained with this kind of sensor, and allows the iden-
tification of minutiae points and even pores.
(a)
(b)
(c)
Figure 3: (a) Palmprint of a newborn, (b) and (c) subsequent
magnifications of a region in (a).
NEWBORN’S BIOMETRIC IDENTIFICATION: CAN IT BE DONE?
203
4 EXPERIMENTAL RESULTS
In order to test the effectiveness of the proposed
method for identification purposes, palmprints and
footprints of 106 newborns were collected at the ma-
ternity ward of the University Hospital (Universidade
Federal do Paran
´
a). The images were collected during
the first 24 hours following birth (T24h), and again
before the babies completed 48 hours (T48h). Each
time two prints of the hand and two of the sole were
collected, so that each baby had four images of its
palm and four of its sole.
Analysis of the images was performed simultane-
ously by two observers. The best footprint and palm-
print of each newborn, out of two collected at T24h,
was classified into one of five categories, according to
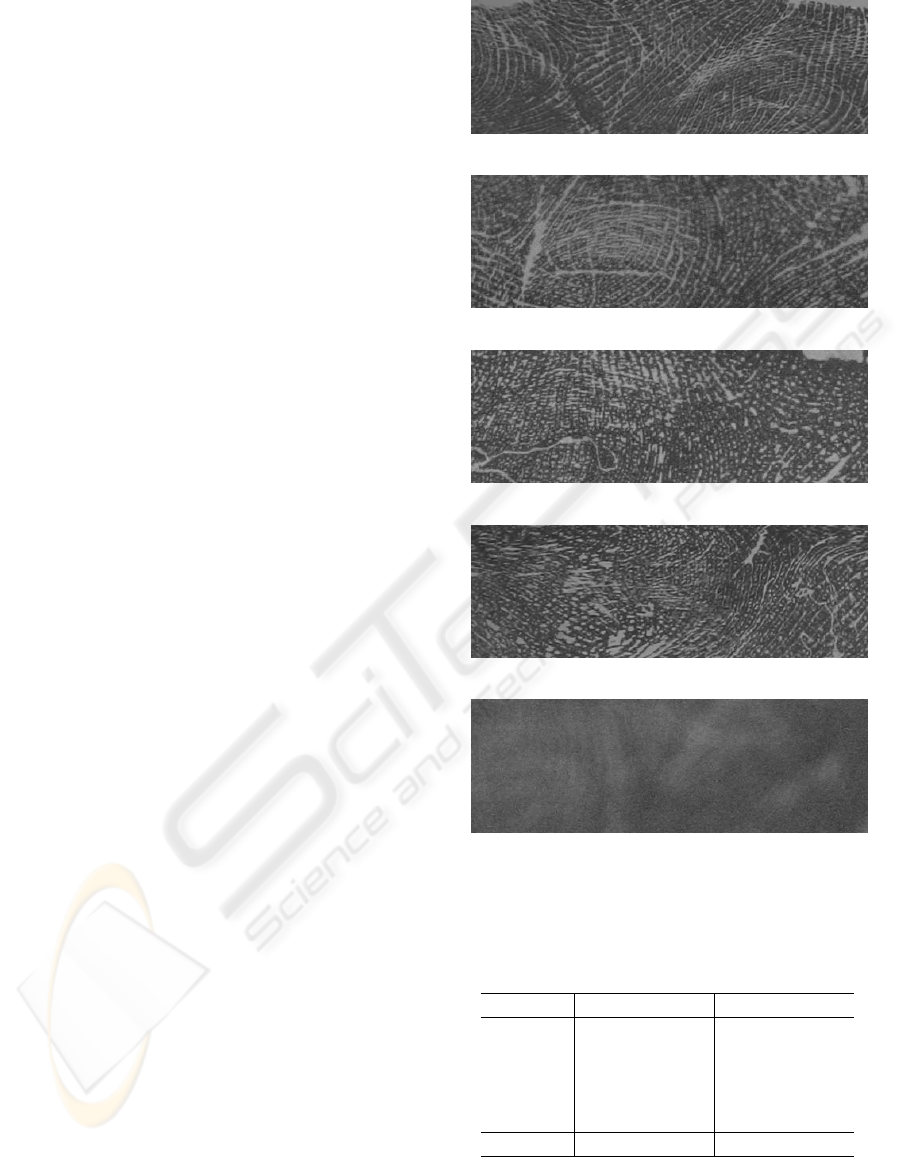
its quality:
• Excelent: a) When the figure(s) or form(s) were
clearly visible (arch, whorl or loop); b) the der-
matoglyph lines were visible; c) one or more tri-
radi (or delta(s)) were found; and d) minutias were
visible (Figure 4a);
• Good: a) When the figure(s) or form(s) were
clearly visible; b) the dermatoglyph lines were
visible; and c) one or more triradi (or delta(s))
were found (Figure 4b);
• Regular: a) When the figure(s) or form(s) were
clearly visible; and b) the dermatoglyph lines
were visible; or c) one or more triradi (or delta(s))
were found (Figure 4c);
• Bad: When only the dermatoglyph lines were vis-
ible (Figure 4d);
• Doodle: No visible dermatoglyphs (Figure 4e).
The results of the quality analysis (Table 1), show
that palmprints yield better quality images than foot-
prints, since 83% of the babies provided palmprints
classified as Excelent or Good (suitable for identifi-
cation), whilst 37.7% of the footprints were classi-
fied into these categories. This is quite surprising,
especially if considered that newborns do not want-
ingly open their hands, which makes palmprint acqui-
sition more difficult. But according to the fingerprint
experts, obtaining the palmprint at birth is of much
greater use for comparisons in later adult life, since it
is the usual identification procedure in most countries
along with fingerprinting.
Table 1 also shows that only 8 newborns (7.5%)
would not be identifiable with the palmprints col-
lected at birth, which is a far better result than in any
previous method.
In addition to the test above, two palmprints of
30 randomly choosen newborns, collected on subse-
quent days (T24h and T48h) were randomly numer-
(a) Excelent
(b) Good
(c) Regular
(d) Bad
(e) Doodle
Figure 4: Illustration of different palm/footprint image
quality.
Table 1: Quality evaluation of the best palmprint and foot-
print of each newborn.
Quality Palmprint Footprint
Excelent 33 31.1% 16 15.1%
Good 55 51.9% 24 22.6%
Regular 10 9,4% 57 53.8%
Bad 8 7.5% 9 8.5%
Doodle 0 0.0% 0 0.0%
Total 106 100.0% 106 100.0%
ated (from 1 to 60) and given to three fingerprint ex-
perts from the IIPR, which had to match the pairs.
VISAPP 2008 - International Conference on Computer Vision Theory and Applications
204

They were able to correctly identify 19 pairs out of
30, a score of 63.3%. From the 11 misclassified, two
were considered classification errors, which means
both images were Good but were incorrectly matched
by mistake. The matching test was then repeated with
another set of 30 newborns, randomly choosen from
the remaining 76, and the experts were able to cor-
rectly identify 20 pairs out of 30 (67.7%), confirming
the previous identification rate.
5 CONCLUSIONS
In this article we presented a newborn palmprint ac-
quisition technique that uses a high-resolution opti-
cal sensor and provides an identification rate at least
three times higher than ink and paper based footprints.
Whilst most authors have concluded that footprints
taken at birth do not provide good images, with cor-
rect identification rates ranging from 0% to 20%, the
method developed in this paper was able to correctly
identify 63.3% and 67.7% of the babies, and 83%
had palmprints with enough quality to allow identi-
fication.
Results also show that palmprints yield better
quality images than footprints despite having a more
difficult acquisition, since babies do not willingly
open their hands.
Finally, the images obtained with this method are
still not as good as adult fingerprints returned by
500d pi sensors. Reasons for this include the fragile
constitution of newborn’s ridges and their dry skin.
Improvements in the technique could be attained by
changing or applying less moisturiser; modifying the
sensor so that images can be analysed straightaway
after acquisition, and making it more comfortable for
newborns hand, so that less pressure has to be applied.
Future research should focus on two remaining
tasks: (1) improve the image acquisition method and
sensor; and (2) develop a software to automatically
identify newborns using these images.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the contribution
of the Secretaria de Seguranc¸a P
´
ublica do Estado do
Paran
´
a for indicating fingerprint experts Ademir Jos
´
e
Menegazzo, M
´
arcia de Loyola Heridas Thomaz and
Vivian Carvalho Ruzik, from the IIPR, who helped on
data collection and analysis of the images. The nurses
working at the maternity ward of the University Hos-
pital, whom contributed significantly while caring for
the babies, and CAPES, CNPq and FINEP for their
financial support for the project.
REFERENCES
Azevedo, N. (2005). Identificac¸
˜
ao neonatal. Bel
´
em – PA.
XVIII Congresso Nacional de Criminal
´
ıstica. Oral
presentation.
Bolle, R., Connell, J., Pankanti, S., Ratha, N., and Senior,
A. (2003). Guide to Biometrics. Springer Verlag.
Castellanos, I. (1953). Dermopapiloscopia Clinica. Imp. P.
Fern
´
andez y C
´
ıa, Havana, Cuba.
Cat, M. N. L. (2003). M
´
eodo FootScanAge para
Determinac¸
˜
ao da Idade Gestacional. PhD thesis, Uni-
versidade Federal do Paran
´
a, Curitiba, Brasil.
Cummins, H. and Midlo, C. (1943). Finger Prints, Palms
and Soles. Dover Publications, Inc., New York.
Galton, F. (1899). Finger prints of young children. British
Association for the Advancement of Science.
Holt, S. B. (1973). The significance of dermatoglyphics in
medicine. Clinical Pediatrics, 12(8):471–484.
Jain, A. K., Ross, A., and Prabhakar, S. (2004). An intro-
duction to biometric recognition. IEEE Trans. Circuits
and Systems for Video Technology, 14(1):4–20.
K
¨
ucken, M. and Newell, A. C. (2005). Fingerprint forma-
tion. Journal of Theoretical Biology, 235:71–83.
Lomuto, C. and Duverges, C. (1995). Identificacion del
recien nacido y medidas de prevencion para evitar
su robo de las maternidades. Revista del Hospital
Materno Infantil Ram
´
on Sard
´
a, 14(3):115–124.
Mainguet, J.-F. (2007). Biometrics.
http:
//perso.orange.fr/fingerchip/biometrics/
biometrics.htm
, accessed in 11/2007.
Maltoni, D., Maio, D., Jain, A. K., and Prabhakar, S. (2003).
Handbook of Fingerprint Recognition. Springer-
Verlag New York, Inc., Secaucus, NJ, USA.
Montgomery, R. (1926). Sole prints of new born babies.
American Journal of Medical Science, 169:830–837.
Pel
´
a, N. T. R., Mamede, M. V., and Tavares, M. S. G.
(1975). An
´
alise cr
´
ıtica de impress
˜
oes plantares de
rec
´
em-nascidos. Revista Brasileira de Enfermagem,
29:100–105.
Shepard, K. S., Erickson, T., and Fromm, H. (1966). Limi-
tations of footprinting as a means of infant identifica-
tion. Pediatrics, 37(1).
Thompson, J. E., Clark, D. A., Salisbury, B., and Cahill, J.
(1981). Footprinting the newborn: not cost-effective.
Journal of Pediatrics, 99:797–798.
Vaesken, C. C. S. (2006). Impresiones digitales.
http://www.monografias.com/trabajos7/imdi/imdi.shtml.
Victor, B., Bowyer, K., and Sarkar, S. (2002). An evaluation
of face and ear biometrics. Proceedings. 16th Interna-
tional Conference on Pattern Recognition, 01:10429.
Wierschem, J. (1965). Know them by their feet. Medical
Record News, 168:158–160.
NEWBORN’S BIOMETRIC IDENTIFICATION: CAN IT BE DONE?
205
