
MEASURING THE FORCES APPLIED TO A VIRTUAL
REALITY LAPAROSCOPIC SURGICAL SIMULATOR WITH
QUANTUM TUNNELLING COMPOSITE SENSORS
I. W. Mack, K. McMenemy, R. S. Ferguson
The Queen’s University of Belfast, Belfast, United Kingdom
S. Potts, A. Dick
The Royal Belfast Hospital for Sick Children, Belfast, United Kingdom
Keywords: Laparoscopic simulator, low cost, PIC microcontroller, quantum tunnelling composite, force feedback.
Abstract: Abdominal surgery performed by laparoscopy requires a very high degree of skill in the surgeon. This skill
level can only be acquired through practice and training. However, a virtual reality (VR) training simulator
commands a high price. There is no reason for a VR simulator to be expensive, as a modern personal
computer can produce high-quality graphics. If all that was required was good graphics, every surgeon
could have a training tool within their laptop computer. What is missing is suitable low-cost human
interface hardware – the equivalent of the computer game ‘joystick’. This paper presents a design for a low
cost device to address this issue. In order to provide force feedback, the forces exerted on the surgical
instruments have to be measured by sensors mounted at various points. The sensors are constructed from
quantum tunnelling composite pills which measure the pressure applied to them by the surgeon. The force
feedback is produced by small direct current motors. The low cost design has been tested by both specialist
laparoscopic surgeons and non surgical personnel to assess its benefits in training at different levels of
expertise. A preliminary qualitative report is given which documents the findings from these initial tests.
1 INTRODUCTION
Laparoscopic, or minimally invasive, or keyhole
surgery is well established among surgeons as a
technique used to carry out surgery through small
incisions as compared to larger incisions required for
traditional surgery. However, while a singer, for
example, can practice before a concert, a surgeon
does not always have available the means to sharpen
his/her skills before performing an operation.
The quality of the training equipment to which a
surgeon has access largely depends on the amount of
money a hospital has available for that purpose. At
the low cost end of the market, a plastic box with a
fabric top represents the body, with holes through
which real surgical instruments are pushed to
operate on rubber body parts. A camera looks
through the side of the box and displays the
‘operation’ on an ordinary video monitor.
At the top end of the market the laparoscopic
surgical trainer can be a pair of pseudo surgical
instruments with force feedback and virtual reality
software running on a computer which displays a
depiction of the inside of a virtual patient and VR
tool tips. The LapVR system from the Immersion
Corporation allows the surgeon to learn essential
skills through virtual reality training. The VEST
systems from Select-IT VEST Systems AG allow for
training in gall bladder removal and surgery in
gynaecology. The SurgicalSim Education Platform
from Simsurgery can be used for a wide range of
training scenarios including trocar placement,
camera navigation, suturing and knot tying.
VR training systems like these, and the one
shown in Figure 1, can cost many thousands of
dollars. However, the cost of such simulators need
not be prohibitive, as personal computer (PC) game
technology can deliver excellent, high quality, real
time interactive 3D graphics that can easily meet any
29
W. Mack I., McMenemy K., S. Ferguson R., Potts S. and Dick A. (2008).
MEASURING THE FORCES APPLIED TO A VIRTUAL REALITY LAPAROSCOPIC SURGICAL SIMULATOR WITH QUANTUM TUNNELLING
COMPOSITE SENSORS.
In Proceedings of the First International Conference on Biomedical Electronics and Devices, pages 29-34
DOI: 10.5220/0001046700290034
Copyright
c
SciTePress

requirements of a VR laparoscopic simulator. If it
was only an issue of graphics, then every surgeon
could have a training and practicing tool on their
laptop PC. It is suitable human interface hardware,
the equivalent of the computer game ‘joystick’ or
‘flight simulator yolk’ that is missing.
Figure 1: A VR laparoscopic surgery application
displaying a representation of the abdomen and two simple
instruments.
When interacting with a 3D virtual environment the
experience not only depends on the type of device
used to provide the human interaction, but also on
external factors such as feedback, whether this is
visual, audio or tactile. Other factors also have to be
considered, such as the number of degrees of
freedom of the user interaction device, as well as
subjective and ergonomic aspects. For example,
(Kontarinis and Howe, 1995) demonstrated that high
frequency vibrations played a significant role in
manipulation tasks. (Lindeman, Sibert and Hahn
1999) showed that adding passive-haptic feedback to
precise manipulation tasks appreciably improved
user performance. (Lindeman, Templeman, Sibert
and Cutler, 2002) demonstrated that adding
vibrotactile feedback to visual and auditory feedback
improved the user experience of virtual
environments.
Force reflecting interfaces such as the
PHANTOM Desktop Device from Sensable
Technologies provide useful feedback, but their
utilization is limited by their cost and the fact that it
is difficult to customize them to fulfill a specific
task.
Vibrating motors, like the ones in mobile
telephones, can be used to provide low-cost
vibrotactile feedback as demonstrated by (Cheng,
Kazman and Robinson, 1996). Indeed vibration
elements have been attached to a standard computer
mouse by (Hughes and Forrest, 1996) to provide
tactile feedback.
This research reflects the belief that integrated
tactile and visual feedback must be implemented in
surgical simulators. The visual feedback is readily
available in real time and at low cost using advanced
computer graphics. The tactile feedback is much
more difficult to integrate into the simulator at low
cost. This paper aims to resolve this issue by
documenting the development of a low cost haptic
device for use in a surgical simulator. Following on
from this introduction, section 2 will outline the
basic design of the mechanical hardware. Sections 3
and 4 describe the electronic system and interface
protocols. The quantum tunnelling sensors are
introduced in section 5 and section 6 illustrates how
the concept was initially tested. Section 7 will then
present conclusions from our work to date.
2 THE SURGICAL TOOLS
This section outlines the design and development of
low-cost haptic devices for interaction with a
surgical simulator.
2.1 The Mk1 Surgical Instruments
The hand grips, and spatial positions used in the
pseudo-instruments, were constructed to match
dimensions taken from actual surgical instruments.
The instruments (the surgical tools) were mounted
on pillars attached to a base. They could rotate from
the horizontal to point down by 45 degrees, and
from facing forward to point inwards by 45 degrees.
These instruments had no electronics attached, as
they were produced solely to verify that the
measurements taken had been translated into an
accurate 3D model. Following initial field trials it
was decided to make some alterations to the position
of the pillars because, during an operation the tool-
tips mostly remain within a 4cm diameter spherical
volume. These changes had the advantage of
allowing more space at the tool-tip end to mount
some electronics in the Mk2 instruments.
2.2 The Mk2 Surgical Instruments
From our earlier research, Mack, Ferguson, Potts
and McMenemy (2006), and discussions with
practicing surgeons it was decided that each joystick
or surgical tool should have six degrees of freedom.
That is, they should allow for movement in the X, Y
and Z axes, rotation about the Z-axis, rotation of the
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
30

tool-tip about the Z-axis, and the opening and
closing of the tool-tip. A Binary-Coded Decimal
(BCD) thumbwheel switch was used to simulate the
actual method of rotating the tool-tip. Five small
rotary potentiometers were used to detect movement
in the X, Y and Z axes, rotation about the Z axis and
the opening and closing of the tool-tip.
For increased stability the instruments were
mounted on a heavy wooden base as shown in
Figure 2.
Figure 2: A pair of Mk2 instruments mounted on a
wooden base.
3 THE USB INTERFACE
This section outlines the design and development of
the Universal Serial Bus (USB) which was chosen to
interface the instruments to the PC.
3.1 The Electronics
The 16C765 USB microcontroller from Microchip
was selected for the interface because Microchip’s
MPLAB and Crownhill’s Proton Development Suite
provide a stable and comprehensive Integrated
Development Environment (IDE). The PICs are
cheap and employ re-usable re-programming
technology, and require little in the way of
additional external components to implement a
working circuit. They have low power requirements
and can therefore draw their power from the
Universal Serial Bus itself.
Members of the Human Interface Device (HID)
Class such as USB keyboards and mice are low-
speed devices, and use interrupt data transfer.
The maximum possible transfer rate of data for
this combination is 8 bytes per 10 milliseconds.
This is quite sufficient for joysticks and similar
devices such as the custom-made Mk2 pseudo
surgical instruments because each surgical
instrument’s interface has only to send 6 bytes of
data, one byte for each potentiometer and one byte
for the thumbwheel switch on the pseudo surgical
instrument.
The PIC was initially configured as a Human
Interface Device without force feedback for the Mk2
joystick. Descriptor details for a HID device can be
found in our earlier paper (Mack et al., 2006).
With the addition of force feedback, each
interface would have to send force data to the PC
and receive force feedback data from the PC. It was
apparent that a HID class interface could not handle
the data rates required. For a Mk3 joystick another
method would have to be found to send and receive
larger data bursts.
Other classes of USB devices were investigated
to determine if any would be suitable for use in a
force feedback interface. The Communications
Device Class (CDC) specification from USB.org
indicated that it could be used for bulk data transfer.
However, the 16C765 could only operate as a
HID class device, so the 18F4550 was selected as it
could operate as a Communications Class Device.
A PCB very similar to the one used for the Mk2
joysticks was designed for the new microcontroller
on the Mk3 joysticks. Two of these circuit boards
are required, one for each surgical instrument, and
are mounted underneath the base of the instrument.
3.2 The PIC Descriptors
The Universal Serial Bus interface uses a serial
protocol, and depending on how it is configured, can
be low, full or high speed. The maximum data rates
are 800 bytes per second for low speed, 1.2
Megabits per second for full speed and 53 Megabits
per second for high speed.
When a USB interface is connected to a PC a
procedure called enumeration takes place. During
enumeration the interface must send descriptors to
the PC which completely define the USB device’s
capabilities and how the device will be used.
MEASURING THE FORCES APPLIED TO A VIRTUAL REALITY LAPAROSCOPIC SURGICAL SIMULATOR
WITH QUANTUM TUNNELLING COMPOSITE SENSORS
31
If a USB device can be incorporated into a standard
USB device class then there is a good chance that it
can be made to work using the standard device
drivers included with the Windows operating
system. Configuring the interfaces as members of
the Communication Device Class results in a
twofold advantage. Firstly, the Proton+ compiler is
able to use customizable descriptors provided by
Microchip which allows the Communications
Device to emulate RS232 serial protocol over a USB
connection. Secondly, the device enumerates as a
COM port on the PC and allows the use of a
standard Windows device driver to establish
communications with the device.
Although the descriptors define the interfaces as
standard COM ports, this is only used as a
convenient way to input data to and output data from
the PC application via the Universal Serial Bus.
Details of the descriptors used in the Mk2 and
Mk3 surgical instruments are explained in detail in
internal documents entitled, “Descriptors required
for a HID USB Interface”, and, “Descriptors
required for a CDC USB Interface”, respectively.
4 THE PIC PROGRAM
However, to have any purpose, the USB devices
must each run an application program.
The surgical instruments were originally
developed without force feedback, and only fed
position information to a Windows VR application,
which can be seen in Figure 1. A different PIC
application was developed for use with an
experimental rig to test the setup for force feedback
in one degree of freedom.
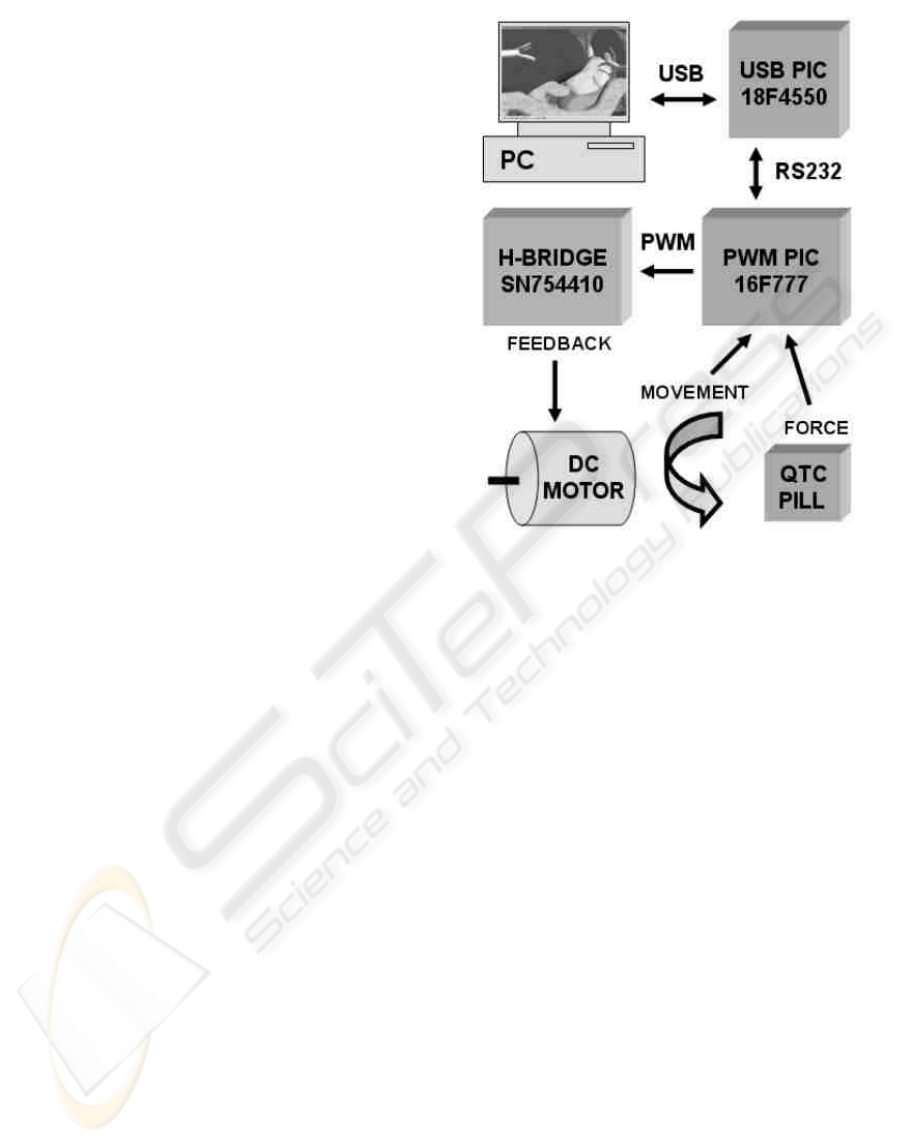
The data flow for one degree of freedom can be
seen in Figure 3. The force feedback in the surgical
instruments will be provided by small DC motors,
which will provide a more tactile feel for the
surgeon. A potentiometer at each pivot point
provides position data. The force exerted by the
user is measured by the use of pressure sensors
produced from Quantum Tunnelling Composite
(QTC) pills manufactured by Peratech.
Excluding the thumbwheel switch input, which is
not suitable for force sensing or force feedback, four
sets of data are required for the operation of each
degree of freedom. Position data has to be sent from
the joystick to the PC application, as does data
regarding the force exerted by the user in two
directly opposing directions. Force feedback data
has to be sent from the PC application to the pseudo
surgical instruments.
Figure 3: Data flow for one degree of freedom.
Small DC motors have been used in the
development process. The motors have to operate in
both forward and reverse, and this can be achieved
by the use of an H-bridge circuit. The motor torque
can be controlled by using Pulse Width Modulation
(PWM) to vary the average current. A motor can be
controlled by varying the duty cycle and/or the
frequency of the PWM pulse train applied to it.
Some PICs, such as the 16F777 used here, have
hardware PWM channels which allow the pulse train
to be produced in the background while the program
is executing other instructions.
It was decided to produce separate modules
which could control three degrees of freedom, with
each module being controlled by a 16F777 PIC. The
PIC also has the nine Analogue-To-Digital (A/D)
converters required to sample three position and six
force sensors. Each module sends data to the USB
interface PIC and receives data from it to control the
torque on three force feedback motors.
At this stage of the research it was decided to
work on only one degree of freedom on one surgical
instrument.
The applications for the USB and 16F777
module PICs were written in Basic and compiled
using the Proton Development Suite.
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
32
5 THE QTC SENSORS
When deformed, Quantum Tunnelling Composites
transform from a near perfect insulator to a
conductor similar to metal. This transformation can
be as a result of compression, stretching or twisting
the composite.
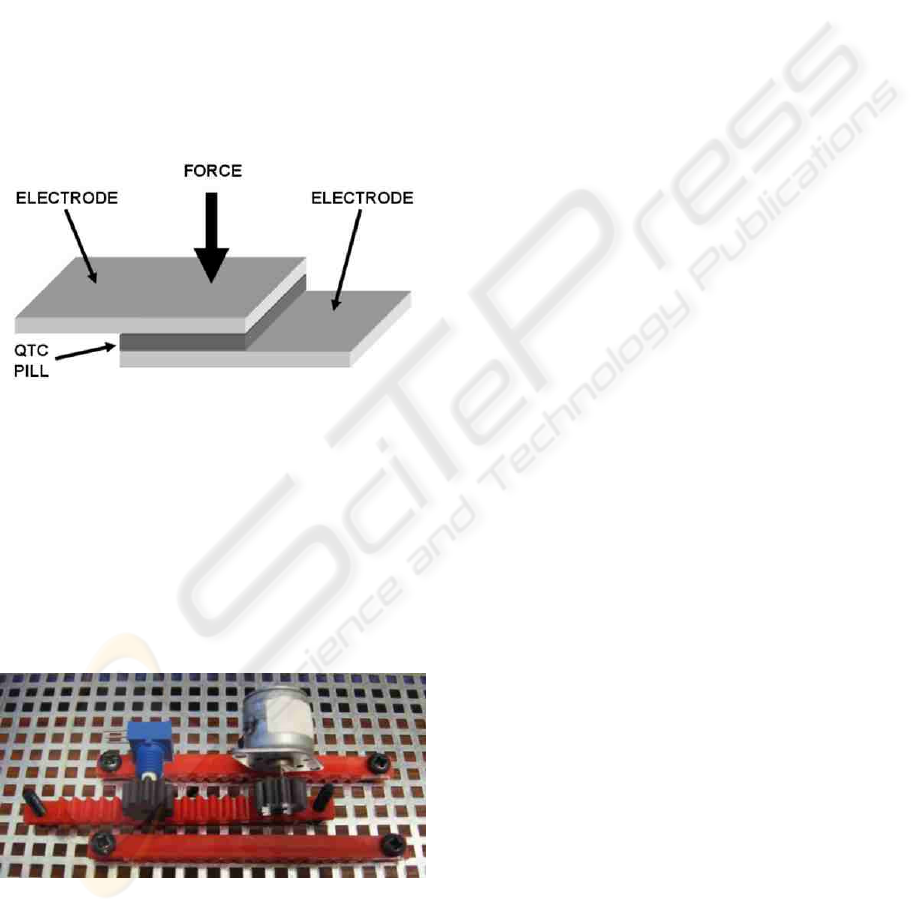
Each QTC pill is sandwiched between two
electrodes, and the user force applied
perpendicularly to the flat face of the pill, as shown
in Figure 4.
The circuit for measuring user force is a simple
potential divider with the sensor in series with a
current limiting resistor. Under no pressure the
sensor appears open circuit, while under pressure it
appears short circuit.
Figure 4: A QTC sandwich sensor.
6 TESTING THE CONCEPT
Figure 5 shows the rig used to evaluate the force
feedback setup. For the sake of clarity it is shown
before wiring.
A simple front-end program, written in Visual
Basic (VB) is used to control and display the output
from the experimental test rig.
Figure 5: The force feedback test rig.
Four bytes of data specify the motor behaviour. The
application program allows forward or reverse
motion to be selected. It is also possible to
interactively control the PWM signal sent to the
motor through the simulated RS232 protocol over
the USB interface to the 18F4550 PIC. The
18F4550 sends the data to the 16F777, to configure
the H-bridge and hence control the DC motor, thus
providing force feedback.
The tests proved that a single personal computer
could act as output generator for force specification
and simultaneously acquire and act upon signals
from the pressure sensors in real-time.
7 CONCLUSIONS
This paper presented a design for, and practical
realization of, a low-cost laparoscopic surgical
training tool that offers the possibility of
incorporating force sensing through the novel use of
quantum tunnelling composite force sensors.
Several electronic interfaces have been
developed, culminating in a fully implemented USB
design that emulates a traditional PC COM port. A
test rig for a one degree of freedom force feedback
axis has been produced which sends position and
force data via one of these USB interfaces to a driver
program in a host PC. Data from the driver program
has been returned to the test rig to control a force
feedback motor. It is the ultimate aim of this
research to have twelve such motors controlled in
the final version of the surgical instruments.
Two instruments give a surgeon the opportunity
to practice realistic procedures, and our design offers
the possibility of highly accurate force sensing and
feedback in the future. The tight interaction between
force sensing and feedback afforded by the quantum
tunnelling sensors will alleviate some of the
problems that arise in conventional haptic rendering
applications, for example the need for a very high
sampling rate in the servo loop.
When combined with the realistic graphics that
current Graphics Processing Unit (GPU) based
rendering hardware offers it will be possible to offer
a very effective training package that could be made
widely available.
Two surgeons and two non-specialists tested the
Mk2 instruments in conjunction with the virtual
reality software and they were very favourably
received. Both groups found the instruments easy to
use, with the surgeons able to perform simulated
surgery on a gall bladder. With force sensing, force
feedback and collision detection algorithms,
surgeons will be able to practice realistic surgical
procedures with a good level of authenticity.
The development of force feedback systems that
are actually used by surgeons requires close
MEASURING THE FORCES APPLIED TO A VIRTUAL REALITY LAPAROSCOPIC SURGICAL SIMULATOR
WITH QUANTUM TUNNELLING COMPOSITE SENSORS
33

teamwork between medical staff and researchers. It
is hoped that the development of this VR trainer will
result in a laparoscopic simulator which will be
acknowledged by the medical profession and lead to
an enhancement in the safety of patient care.
The original aim of making a pair of low-cost
pseudo surgical instruments for a VR laparoscopic
simulator is well on the way to a successful
conclusion. The component cost of the Mk2
instruments is approximately 0.4% of the cost of the
Virtual Endoscopical Surgery Training (VEST)
simulator without force feedback from Select-IT
VEST Systems AG. The Mk3 training instruments,
when they have force sensing and force feedback
implemented will have a projected component cost
of 1.1% of the cost of the VEST force feedback
system. While our costs do not include the cost of
manufacturing the instruments they compare very
favourably with commercial equipment. Indeed we
could include a laptop computer with pre-installed
laparoscopic simulation software, which could also
be used independently as an ordinary PC, and still
cost only 1.5% and 1.7% of the commercial non
force feedback and force feedback systems
respectively.
REFERENCES
Cheng, L.-T., Kazman, R., & Robinson, J. (1996).
Vibrotactile Feedback in Delicate Virtual Reality
Operations. Paper presented at Fourth ACM
International Conference On Multimedia. Boston,
MA.
Hughes, R., & Forrest, A. (1996). Perceptualisation Using
a Tactile Mouse. Paper presented at Visualization ’96.
San Francisco, CA.
Kontarinis, D., & Howe, R. (1995). Tactile Display of
Vibratory Information in Teleoperation and Virtual
Environments. Presence: Teleoperators and Virtual
Environments, 4(4), 387-402.
Lindeman, R., Sibert, J., & Hahn, J. (1999). Towards
Usable VR: An Empirical Study of User Interfaces for
Immersive Virtual Environments. Paper presented at
ACM CHI ’99. Pittsburgh, PA.
Lindeman, R., Templeman, J., Sibert, J., & Cutler, J.
(2002). Handling of Virtual Contact in Immersive
Virtual Environments: Beyond Visuals. Virtual
Reality; 6(3), 130-139.
Mack, I.W., Ferguson, R.S., Potts, S., & McMenemy, K.
(2006). Adding tactile realism to a virtual reality
laparoscopic surgical simulator with a cost effective
human interface device. Paper presented at Electronic
Imaging 2006. San Jose, CA.
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
34
