
DIABETES SCREENING DATABASE
A Comprehensive Electronic Patient Record for Global Risk Assessment in a
Rural Community
E. Pecoul
1
and H. F. Jelinek
2
1
IUP Génie Physiologique et Informatique, Faculté des Sciences Fondamentales Appliquées
Université de POITIERS, France
2
School of Community Health, Charles Sturt University, Albury, Australia
Keywords: Diabetes Screening, Access database, interdisciplinary health care.
Abstract: Interprofessional health care is becoming more prevalent with an increase in chronic diseases such as
diabetes and cardiovascular disease. In addition preventative models often require large numbers of risk
factors for identification of preclinical cases. CSU has established a diabetes screening clinic augmented by
an ACCESS database. The novelty of our work is that the ACCESS database integrates into the public
health sector and provides a more comprehensive review of health/disease indicators. Information on
traditional health indicators in addition to autonomic nervous system function tests, fundus examination and
foot assessment results as well as pro-inflammatory, pro-coagulation and antioxidant biochemistry can be
added by the university-based screening clinic as well as by diverse primary health care practitioners and
specialists that would otherwise not have access to this detailed information for patient assessment and
treatment. Our results are in favour of this interdisciplinary database indicating that over one year we have
identified 16.2% of people with no previous medical condition to have pre-diabetes, 2% had retinal disease
and 21.5% had foot problems. Moderate to severe ECG anomalies were identified in 19.3% of the
participants. Of these, 68.8% were either commenced on treatment, had their treatment changed or received
surgery. Our results indicate that a comprehensive EPR manager as part of an interdisciplinary health
screening initiative is able to track people that require intervention but were missed in the current public
health system as implemented in our community.
1 INTRODUCTION
For optimal health care, providers need the
necessary
information when they give treatment.
Health care provider and patient information and
decision
support needs can be satisfied if primary
care providers
use electronic patient records that are
comprehensive and provide the necessary
information to the general practitioner or specialist
at the time of consultation (EPRs) (Bates et al.,
2003). Often electronic records may indicate that a
patient has attended a specialist for an assessment
but the results may not be available to the general
practitioner nor to other primary health care
providers and specialists. In addition many rural
areas experience a lack in specialists and allied
health professionals as well as general practitioners.
Electronic patient records (EPRs) provide a
powerful opportunity for health assessments yob re
integrated as part of an integrated interdisciplinary
primary health network. Universities with additional
resources in rural communities can also to support
this initiative by establishing screening clinics as
part of their health professional courses. University-
based teaching and research can provide
screening/assessment results especially for tests not
routinely carried out in the community due to lack of
available services. With additional risk assessment
results during consultation, the GP's EPR is valuable
in identifying patients at risk for undiagnosed type 2
diabetes, cardiovascular disease or other illness.
Previous research on use of electronic patient
records (EPR) indicated that general practitioners
are able to utilise information on additional risk
factor assessment from the EPR during regular
consultation (Klein Woolthuis et al., 2007). EPR
recall systems based on HbA1c levels showed that
the median practice-specific proportions of patients
13
Pecoul E. and F. Jelinek H. (2008).
DIABETES SCREENING DATABASE - A Comprehensive Electronic Patient Record for Global Risk Assessment in a Rural Community.
In Proceedings of the First International Conference on Health Informatics, pages 13-19
Copyright
c
SciTePress

with HbA1c recorded annually increased from a
median 65% to 77% when using an EPR (Mohiddin
et al., 2006). An Australian study conducted by
Burns et al. using the CARDIAB®
TM
register recall
system evaluated the process of care of patients for
nine parameters critical to quality of
care in diabetes:
glycaemic control (HbA1c), blood pressure,
body
mass index, total cholesterol levels,
triglyceride
levels, high density lipoprotein
levels (HDL),
microalbumin level, foot checks and eye checks.
They demonstrated the potential
of CARDIAB®
TM
to provide support to
general practice in the
management of diabetes (Burns et al., 2004).
Divisions of General Practice, universities and
other primary health care providers have
a key role
to play in supporting general
practitioners (GPs) to
provide proactive, preventive care for
their patients
with cardiovascular disease
(CVD) and diabetes
(Penn et al., 2004). They can achieve this by
providing them with global risk marker information
and health assessment results. Risk stratification is
currently based on the Framingham cardiovascular
risk equation and therefore include factors such as
blood pressure, diabetes, age, gender and HDL
(Sheridan et al., 2003). However research has
suggested that a more global approach to
identification of diabetes and cardiovascular disease
may be appropriate (Michos et al., 2006). In addition
the risk status of persons
without CHD varies
greatly, and this variability mandates a
range in the
intensity of interventions. Effective primary
prevention
thus requires an assessment of risk to
categorize patients for
selection of appropriate
interventions and a more comprehensive screening
/health assessment that includes additional factors
provided by combining the information obtained
from an interdisciplinary health care system and
available via an EPR (Jelinek et al., 2006,
Woodward et al., 2006).
The major and independent risk factors for CHD
are cigarette
smoking, elevated blood pressure,
elevated serum
total cholesterol and low-density
lipoprotein cholesterol (LDL-C),
low serum high-
density lipoprotein cholesterol (HDL-C), diabetes
mellitus, and advancing age. Other factors are
associated with increased risk for
CHD. These
include obesity, physical inactivity, elevated
homocysteine, pro-coagulation and pro-
inflammatory factors. An assessment of global risk
based on the summation
of all major risk factors can
be clinically useful for in identification of high-risk
patients who require immediate
attention and
intervention and changes in intervention based on
the global risk estimate (Grundy et al., 1999).
Health assessment and determination of risk
factors included in a global risk equation is often not
possible in rural communities where there is a lack
of general practitioners, allied health practitioners
and specialists. University-based teaching and
research has the opportunity to integrate with the
public health system (Jelinek et al., 2006). An
electronic patient record system that spans from
university-based teaching and research to public
health care and that incorporates data obtained from
an interprofessional health care system is required.
The EPR must integrate medical, nursing, and
allied health worker data as well as the results from
pathology laboratories that may be shared by the
health care team. The EPM needs to be secure,
provide relevant template forms, incorporate a recall
system and specific reports, and a means of tracking
interventions by diverse health care professionals.
The majority of databases meet this criterion but are
mainly specific for certain medical specialities such
as general practice. The DiScRi database discussed
here extends these fundamental principles to address
the needs of an interdisciplinary health care team
with emphasis on identification and follow-up of
people with and without diabetes or cardiovascular
disease as well as identification of those at risk of
diabetes and cardiovascular disease based on a
global risk assessment. Information of outcomes
following referral to general practitioners, allied
health and medical specialists provides information
to of global health care and the status of the patient.
The database allows access to all biochemistry and
pathology results as well as the retinal photography,
12-lead ECG and Doppler peripheral vessel blood
flow velocity traces that is collected by diverse
health care professionals that would otherwise not be
available in a coherent form.
2 METHODS
2.1 Database
The Diabetes Screening Research Initiative (DiScRi)
application was designed using Microsoft ACCESS
(under Microsoft Windows), SQL (Select Query
Language) and VBA (Microsoft Visual Basic)
languages. The CDM (Conceptual Data Model) and
LDM (Logical Data Model) were designed using
MERISE theories. The database contained 22
entities and 153 attributes (Table 1).
Accurate information is available for
demographics, medical history, biochemistry, urine
analysis as well as lifestyle, medication, foot, eye
HEALTHINF 2008 - International Conference on Health Informatics
14
and heart health including antioxidant levels, pro-
inflammatory and pro-coagulation factors for a
patient. There is also a direct access to files such as
retinal and ECG pictures, and a resume of most
important health information (BP, age, cholesterol,
diabetes status, medication).
The body-mass index (BMI), the ankle-brachial
pressure index (ABPI) for assessment of peripheral
vascular disease, the Ewing score, which indicates
presence and severity of cardiac autonomic
neuropathy as well as absolute 5 year CVD risk are
automatically calculated. Cover letters for the
general practitioner or specialist, if required, are
automatically generated with a link between
Microsoft Access and Microsoft Word (an update in
the database will update the Word document) and
can be sent by e-mail (using Word mail function), or
printed for mailing and/or storage as hard copy.
2.2 Screening Participants
To assess the utility of the DiScRi database, patients
were recruited through the media and the research
had Charles Sturt University Human Ethics
approval. All participants had their height, weight
and waist circumference measured. A urine sample
was analysed and a blood sample used to determine
levels of glucose, electrolyte, cholesterol, HbA1c,
antioxidants, pro inflammatory and pro-coagulation
markers. Retinal photographs of the posterior pole
are used to determine presence of diabetic
retinopathy and risk of CVD. Heart function was
determined by 12-lead ECG including calculation of
corrected QT interval (QTc), QT dispersion (QTd),
frequency and time domain analysis results. The
latter are indicators of preclinical cardiac autonomic
neuropathy (CAN). CAN is also assessed using the
Ewing battery. Foot health assessment includes
ABPI, monofilament for peripheral neuropathy
(PN), ankle and knee reflexes, and muscle tone.
Thus the university screening simulated an
interdisciplinary health provision system.
3 RESULTS
3.1 Database Characteristics
From the introductory screen, the database allows
access the demographic data, clinical history,
follow-up, biochemistry, eye, heart and foot
assessment results.
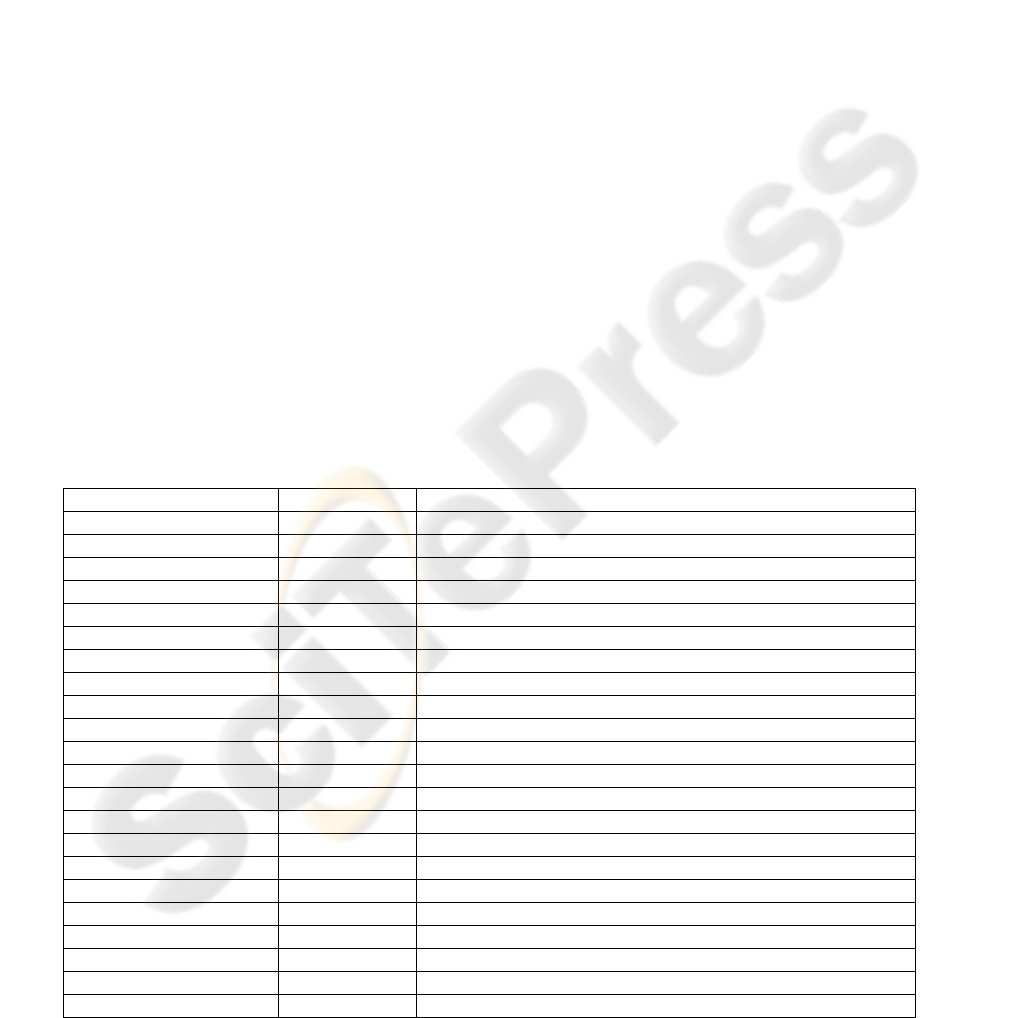
Figure 1 shows an example of a test recording
screen. For the ECG analysis, the 12-lead ECG trace
can also be accessed. The 3-lead recording indicates
the results for the assessment of cardiac autonomic
neuropathy based on the Ewing score.
All data is divided into tables that can be
Table 1: Entities contained in the DiScRi database.
Entities # values Examples
GP 4 Name, address, telephone, email
Patient 5 Name, address, telephone, DOB
Analysis 2
Medications 2 Current medications, change medications
Clinical history 5 Diabetes, HT, CVD, medical information
Foot history 3 Presence of ulcers, general pain, numbness
Heart history 10 Angina, fainting, heart attack, stroke, chest pain
Eye history 2 Glaucoma, cataract, diabetic retinopathy
Other history 6 Kidney, bladder, GIT
Lifestyle 7 Smoking, alcohol, family history for diabetes/CVD, diet, exercise
Consultation history 6 Attendance to health care professionals; details of consultations
3lead ECG Ewing 7 Lying to standing HRV change
3lead ECG HRV 17 Frequency and time domain results for HRV
12lead ECG 8 HR , QTc, QTd, interpretation,
Neuropathy 7 Monofilament, ABPI,
BMI 4 Height, weight, waist circumference
ABPI 5 Systolic blood pressure at arm and ankle
Glucose 5 time since last meal, glucose level at screening
BP 5 Lying and standing BP
Urine 12 Glucose, protein, albumin
Biochemistry 26 Cholesterol, antioxidants, pro-inflammatory, pro-coagulation markers
Eye analysis 5 Eye pathology, AVR diagnosis, photograph
DIABETES SCREENING DATABASE - A Comprehensive Electronic Patient Record for Global Risk Assessment in a
Rural Community
15
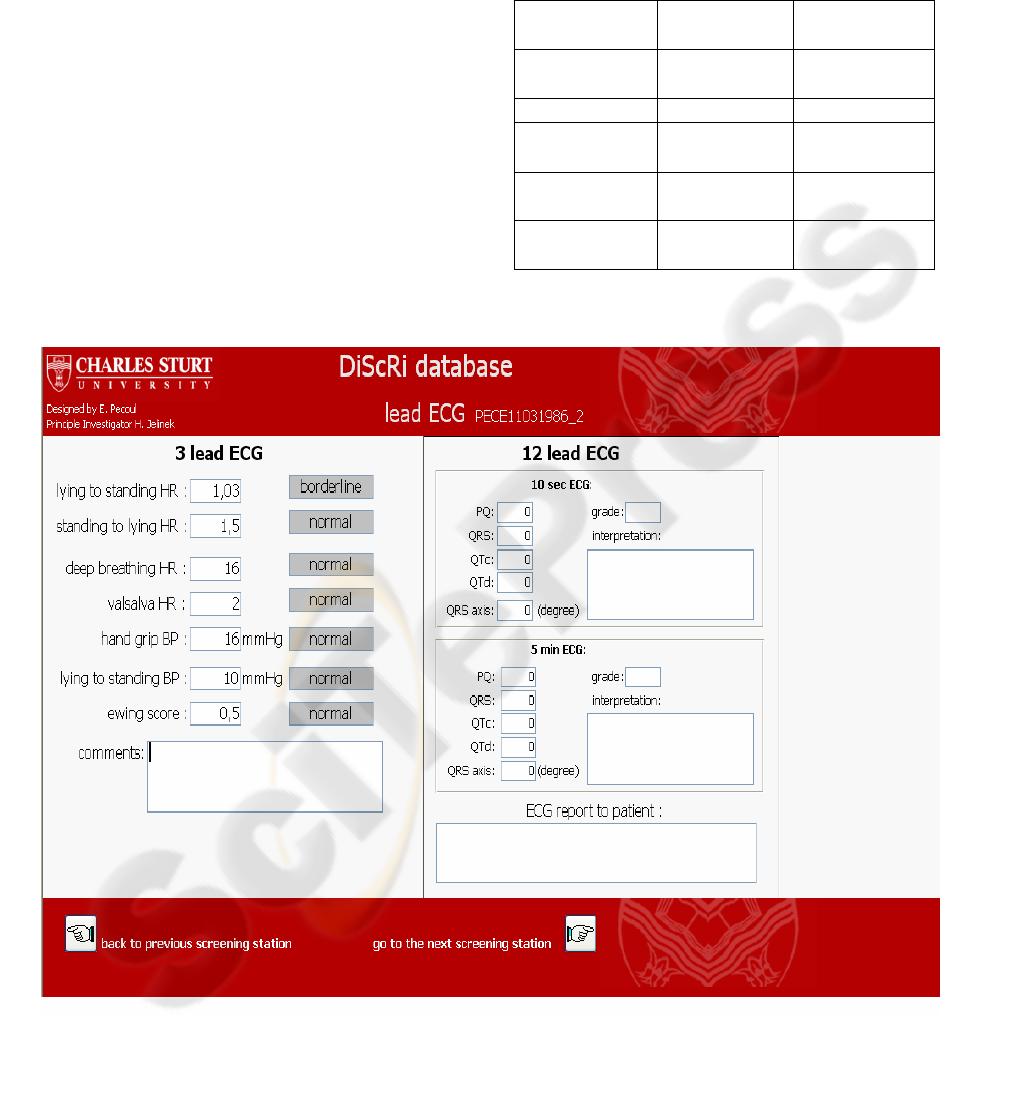
separately accessed, However for a quick overview
during a consultation, the global information page
indicates the date of last visit and includes the
possibility of accessing the eye photographs of the
retinal posterior pole, the 12-lead ECG trace and
information on glucose and cholesterol levels as well
as blood pressure and BMI (Figure 2). From this
page the user can also move to any of the analysis
for specific and more comprehensive results.
An important addition to this database is the
opportunity for detail follow-up provided by diverse
health care practitioners as shown in Figure 3.
3.2 Screening Outcomes
A review of the outcomes for the university-based
simulation study that measured health/disease
indicators indicated that in this rural area the
prevalence is worse compared to the national
average for all tests in the diabetes cohort and
elevated for the ABPI and ECG in the non diabetes
group (Table 2).
Table 2: Prevalence of pathology in a rural cohort
determined through a university-based screening initiative.
Measure* % Non
diabetes
% National
Average
PN 8.13 19.4 (foot
ulcer)
ABPI 11.6 unknown
BMI 25 20
(>30kg/m2)
HT 28 30
(140/90)
ECG 13 12(diab) /
3(control)
Figure 1: ECG assessment form.
HEALTHINF 2008 - International Conference on Health Informatics
16
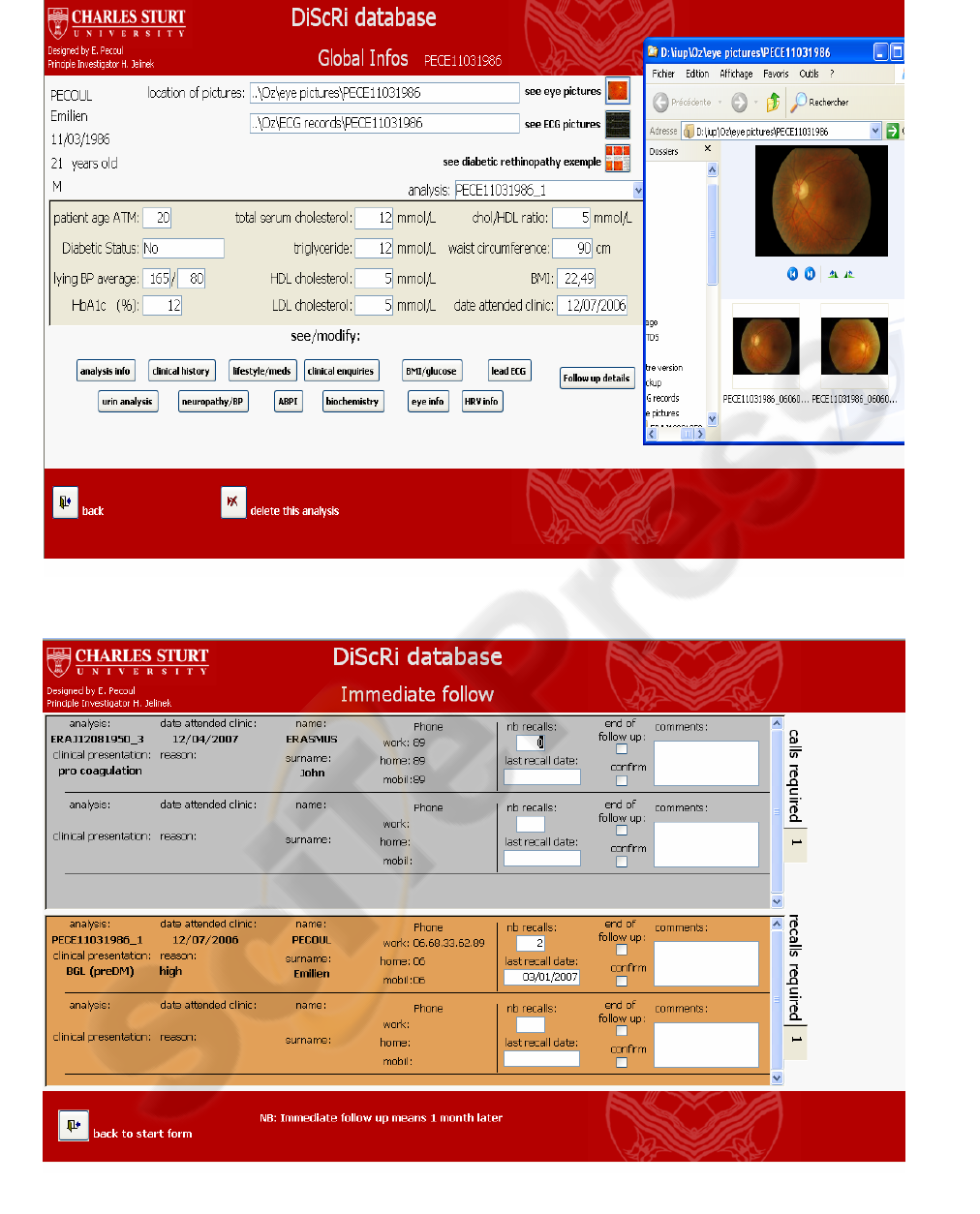
Figure 2: Global information screen with eye photograph.
Figure 3: Recall screen.
DIABETES SCREENING DATABASE - A Comprehensive Electronic Patient Record for Global Risk Assessment in a
Rural Community
17

4 DISCUSSION
In Australia, general practitioners play an important
role in the management of diabetes. This involves
careful monitoring of behavioural risk factors, blood
pressure, glycaemic control and lipids; early
detection of complications; and management
according to evidence-based guidelines (NHMRC,
2004, Newnham et al., 2004). However, a
comprehensive health review can only be provided
by an interdisciplinary health care team. With the
rapid advances in information technology in the last
decade, various diabetes information systems have
evolved in different parts of the world. Availability
of new technologies and information systems for
monitoring and treating diabetes is critical to
achieving recommended metabolic control. A
comprehensive EPR that includes data for global
risk assessment and patient review and provides
mechanisms for practitioners to gain information on
performance and results from a diverse primary
health care team that would otherwise not be
integrated is essential for evidence-based practice
and improvement in health care provision.(Joshy and
Simmons, 2006) The DiScRi study indicates that an
EPR that incorporates information across the health
care sector arising from annual consultations in the
university
setting such as test results and
outcome of
referrals, as well as lifestyle data such as smoking
status, exercise
and body mass index is of benefit to
both the health care providers and the patients.
Effective EPR implementation and
networking
could eventually save more than $81 billion
annually—by
improving health care efficiency and
safety—and that HIT-enabled
prevention and
management of chronic disease could eventually
double those savings while increasing health and
other social
benefits.(Hillestad et al., 2005) DiScRi
data provides important baseline information
for
health care quality improvement at local, state and
national levels. Including pro-coagulation and pro-
inflammatory factors improves overall health care
planning as the physician has additional
information.(Navab et al., 2006) Similarly, options
for viewing retinal images that indicate early signs
of diabetes or presence of CVD seen on 12-lead
ECG or peripheral pulse wave analysis can be of use
to general practitioners. The database allows access
to all biochemistry and pathology results as well as
the retinal photography, 12-lead ECG and Doppler
peripheral vessel blood flow velocity traces. Making
the DiScRi EPR the most comprehensive primary
health care database available in Australia.
REFERENCES
Bates, D. W., Ebell, m., Gotlieb, E., Zapp, J. & Mullins,
H. C. (2003) A Proposal for Electronic Medical
Records in U.S. Primary Care. J Am Med Inform
Assoc, 10, 1-10.
Burns, J. R., Bonney, M.-A., Davies, P. G. P. & Harris, M.
F. (2004) Utilization of the CARDIAB(R)TM
database system to promote quality of care in
Australian general practice. Health Informatics
Journal, 10, 177-184.
Grundy, S. M., Pasternak, R., Greenland, P., Smith, S., Jr.
& Fuster, V. (1999) Assessment of Cardiovascular
Risk by Use of Multiple-Risk-Factor Assessment
Equations : A Statement for Healthcare Professionals
From the American Heart Association and the
American College of Cardiology. Circulation, 100,
1481-1492.
Hillestad, R., Bigelow, J., Bower, A., Girosi, F., Meili, R.,
Scoville, R. & Taylor, R. (2005) Can Electronic
Medical Record Systems Transform Health Care?
Potential Health Benefits, Savings, And Costs. Health
Aff, 24, 1103-1117.
Jelinek, H. F., Wilding, C. & Tinley, P. (2006) An
innovative multi-disciplinary diabetes complications
screening programme in a rural community: A
description and preliminary results of the screening.
Australian Journal of Primary Health, 12, 14-20.
JOSHY, G. & SIMMONS, D. (2006) Diabetes
Information Systems: A Rapidly Emerging Support
for Diabetes Surveillance and Care. Diabetes
Technology & Therapeutics, 8, 587-597.
Klein Woolthuis, E. P., De Grauw, W. J. C., Van Gerwen,
W. H. E. M., Van Den Hoogen, H. J. M., Van de
Lisdonk, E. H., Metsemakers, J. F. M. & Van Weel, C.
(2007) Identifying people at risk for undiagnosed type
2 diabetes using the GP's electronic medical record.
Fam. Pract., 24, 230-236.
Michos, E. D., Nasir, K., Braunstein, J B., Rumberger, J
A., Budoff, M. J., Post, W. S. & Blumenthal, R. S.
(2006) Framingham risk equation underestimates
subclinical atherosclerosis risk in asymptomatic
women. Atherosclerosis, 184, 201-206.
Mohiddin, A., Naithani, S., Robotham, D., Ajakaiye, O.,
Costa, D., Carey, S., Jones, R. H. & Gulliford, M. C.
(2006) Sharing specialist skills for diabetes in an inner
city: A comparison of two primary care organisations
over 4 years. Journal of Evaluation in Clinical
Practice, 12, 583-590.
Navab, M., Anantharamaiah, G. M., Reddy, S. T., Van
Lenten, B. J., Ansell, B. J. & Fogelman, A. M. (2006)
Mechanisms of disease: proatherogenic HDL - an
evolving field. National Clinical Practice,
Endocrinology and Metabolism, 2,
504-511.
Newnham, H., Colagiuri, S., Hepburn, A., Chen X. M. &
Colagiuri, R. (2004) National Evidence Based
Guidelines for Type 2 Diabetes: Prevention and
Detection of Macrovascular Disease. Canberra,
NHMRC.
HEALTHINF 2008 - International Conference on Health Informatics
18

NHMRC (2004) National Health and Medical Research
Council. National evidence based guidelines for the
management of type 2 diabetes mellitus: prevention
and detection of macrovascular disease. Sydney,
Australian Centre for Diabetes Strategies.
Penn, D. L., Burns, J. R., Georgiou, A., Davies, P. G. P. &
Harris, M. F. (2004) Evolution of a register recall
system to enable the delivery of better quality of care
in general practice. Health Informatics Journal, 10,
165-176.
Sheridan, S., Pignone, M. & Mulrow, C. (2003)
Framingham-based Tools to Calculate the Global Risk
of Coronary Heart Disease. A Systematic Review of
Tools for Clinicians. Journal of General Internal
Medicine, 18, 1039-1052.
Woodward, A., Wallymahmed, M., Wilding, J. & Gill, G.
(2006) Successful cardiovascular risk reduction in
Type 2 diabetes by nurse-led care using an open
clinical algorithm. Diabetic Medicine, 23, 780-787.
DIABETES SCREENING DATABASE - A Comprehensive Electronic Patient Record for Global Risk Assessment in a
Rural Community
19
