
ECGAWARE: AN ECG MARKUP LANGUAGE FOR
AMBULATORY TELEMONITORING AND DECISION MAKING
SUPPORT
Bernardo Gonçalves, José G. Pereira Filho
Computer Science Department, Federal University of Espírito Santo (UFES), Vitória, Brazil
Rodrigo V. Andreão
Electrical Engineering Department, Federal University of Espírito Santo (UFES), Vitória, Brazil
Keywords: Telecardiology, Telemonitoring, ECG data, Interoperability, Context-Awareness, Emergency and decision
support.
Abstract: The ambulatory electrocardiogram (AECG) can be acquired and transmitted through mobile and wireless
technologies and devices to foster heart’s telemonitoring anytime, anywhere. This sort of service is
purposeful when combined with ECG analysis systems and infrastructural support for providing context-
aware services. Such setting makes efficient emergency services possible as well as improves the support to
physician’s decision making. This paper presents an ECG XML-based markup language that extends ECG
reference standards in order to cover patient’s heart telemonitoring during his/her daily activities. The ECG
data format we propose is then applied in a real scenario.
1 INTRODUCTION
The rapid expansion of ICT has been allowing the
creation of new services on Healthcare. The
Telecardiology, in particular, has developed itself
mainly through the transmission of the
electrocardiogram (ECG). On one side, the ECG is
fast, cheap and non-invasive when compared with
other cardiology examination procedures. On the
other side, the analysis of the ECG waveform can
identify a wide range of heart illnesses, which are
distinguished by specific modifications on ECG
elementary waveforms. These are the reasons why
ECG is the most frequently applied test for
measuring heart activity in Cardiology. According to
estimates, more than 100 million ECG’s are
recorded yearly in Western Europe (Fischer and
Zywietz, 2003).
The storage and transmission of all these data
have then been object of some initiatives concerning
ECG format standardization. The oldest standards
are AHA/MIT-BIH (Goldberger et al., 2000) and
SCP-ECG (SCP, 2002), regarding records’ storage
and transmission respectively. In face of the Internet
popularization, however, novel standards have been
conceived in order to integrate interoperable and
user-driven solutions, standing out FDADF (Brown
et al., 2002) and ecgML (Wang et al., 2003), both
based on the XML markup language.
Nonetheless, such standards do not take into
account heart’s telemonitoring, which calls for the
representation and transmission of the ambulatory
electrocardiogram (AECG). The portable device that
records the AECG was invented by Norman Holter
in 1957. Since then, the ICT advances in addition to
improvements in the accuracy of ECG software-
based analysis systems have opened new potential
uses to the AECG. Indeed, it is largely employed by
the medical community, mostly for diagnosis and/or
therapeutic treatment of the myocardial ischemia,
which constitutes a pre-infarct. Since most ischemia
episodes are related to increases in heart rate
possibly associated to day-to-day variability of
physical or emotional activities, AECG is indicated
for patient’s heart monitoring throughout his or her
daily activities. With this in mind, the most suitable
duration of a recording session to detect and
quantify ischemia episodes is probably 48 hours.
Some experiments point out that most patients are
quite comfortable wearing the recorder for 48 hours
(Crawford et al., 1999).
Besides, with the advent of a new Computing
paradigm, the Pervasive Computing, context-aware
37
Gonc¸alves B., G. Pereira Filho J. and V. Andre
˜
ao R. (2008).
ECGAWARE: AN ECG MARKUP LANGUAGE FOR AMBULATORY TELEMONITORING AND DECISION MAKING SUPPORT.
In Proceedings of the First International Conference on Health Informatics, pages 37-43
Copyright
c
SciTePress

systems provide new features, standing out for
collaboration among professionals, systems, and
action triggering from the detection of changes in
the context of the user. This can be verified with the
growth of initiatives dedicated to patient’s
monitoring, whether at home or in emergency
situations wherever they take place. An example is
the Awareness project (Awareness, 2007). Such
efforts have taken advantage of the latest advances
in mobile and wireless technologies and devices, in
general, and may rely on signal processing
algorithms, in particular, in order to provide both
alarms generation and decision making support.
In face of all these aspects, we advocate that an
ECG data format should cover the particular issues
concerning telemonitoring through AECG, such as
the ones related to emergency assistance (e.g.
patient’s location), or the activities performed by the
patient during the ECG recording session (e.g. rest,
physical exercise, routine activities, etc.). In this
article we propose a novel ECG data format that
extends former reference standards in order to cope
with real-time telemonitoring and decision making.
The paper is organized as follows. Section 2
discusses the background of ECG data standards as
well as aspects of telemonitoring; Section 3 presents
the ECG data format we propose in this paper;
Section 4 introduces a usage scenario where the
format proposed is applied; and, finally, Section 5
concludes the paper and depicts future work.
2 BACKGROUND
Throughout the last thirty years, we can notice a
regular evolution of standards regarding ECG
record’s representation and transmission. One may
state that each standard resembles its purpose and
the ICT environment at the time of its arising.
Since 1975, the Massachusetts Institute of
Technology (MIT) together with laboratories of the
Beth Israel Deaconess Medical Center have carried
out research concerning medical examinations
analysis and related points. As a result, in 1980 the
MIT-BIH Arrhythmia Database was deployed after
testing and standardization for arrhythmia detection
and evaluation. Also at this time, the American
Heart Association (AHA) has deployed the AHA
Database for Evaluation of Ventricular Arrhythmia
Detectors (
Goldberger et al., 2000). Together, those
databases have been largely used and played an
important role on research in the field of Cardiology
(Moody and Mark, 2001).
The AHA/MIT-BIH standard has focused on
bringing in an ECG records’ library for providing
input for developers of ECG analysis systems. It, in
fact, is responsible for substantial advances on ECG
data processing. This standard, however, does not
aid interoperation over the Internet due to its tight
coupling with programming language. Moreover, it
is not human readable, which is a desirable
requirement with respect to the analysis of
electrocardiography’s domain experts.
Later, there was a great effort to conceive the
SCP-ECG - Standard Communications Protocol for
Computer-Assisted Electrocardiography (SCP,
2002). SCP-ECG is a specification concerning ECG
data format as well as transmission procedure from
the acquisition device to the host where the message
is stored and retrieved. From 1989 to 1990, it was
carried out a survey on ECG compression methods
that has as a result led to an original approach for
signal compression (Fischer and Zywietz, 2003).
Nonetheless, despite the SCP-ECG allows
suitable data compression, the elements of the
format are defined at the bit level. This obstructs
changes on the format, either for updating or
customization, as well pushes final applications (i.e.,
ECG viewers) to be familiar with SCP codes. As per
(Clunie, 2004), SCP implementation is an
awkwardly task especially on the compression
mode. Considering that computational resources are
currently more accessible than at the creation of the
SCP, bandwidth over the networks, memory
capacity and disc space are not main concerns as
they were before. Meanwhile, other concerns have
taken place on Telemedicine scenarios, such as the
need for platform- and application-independent
solutions involving human readable data models.
In this trend, and also as a result of the grown
popularity of the Internet, XML-based formats as
FDADF and ecgML have been increasingly used on
Telecardiology research. The Extensible Markup
Language (XML) has played an important role on
data exchange over the web, especially by providing
the separation of data content and presentation. After
XML has became a W3C recommendation in 1998,
several domain specific languages were created from
a XML Schema. In this way, several committees of
Health organizations such as CEN/TC251, Health
Level Seven (HL7), American Society for Testing
and Materials (ASTM), etc, have worked on the
development of recommendations for using XML on
Telemedicine research.
The Food and Drug Administration (FDA) has
carried out a survey on ECG standards and has
chosen the XML technology for data representation
based on the HL7 ECG annotation message v3
(HL7, 2003). As a result, in 2002 it has produced the
FDA XML Data Format (FDADF). The FDADF is
HEALTHINF 2008 - International Conference on Health Informatics
38

an effort to reach the standardization of ECG data
representation for all stakeholders share the same
view (Brown et al., 2002). Looking for addressing
requirements previously defined, the scope of the
FDADF specification covers ECG data as much as
significant submission information. FDADF has
achieved a significant progress on ECG data
representation by using XML. Nevertheless, as per
(Wang et al., 2003), it does not exploit as far as
possible XML features. That is because, on account
of ECG viewer applications’ concerns, it has
incorporated elements related to data presentation in
its metamodel, rather than to cope only with data
content.
More recently, in 2003, the ecgML was
developed in face of the increased demand for a
standardized application- and platform-independent
ECG format. This one has been conceived from the
former standards (especially the FDADF), reusing
then concepts and nomenclature. The ecgML allows
ECG data analysis and transmission between
heterogeneous platforms (Wang et al., 2003).
Indeed, rather than FDADF, the ecgML has
comprised only data content. It holds benefits such
as flexibility, readability and descriptiveness.
Nonetheless, as remarked by the authors themselves,
there are issues left to evaluation, such as concepts
still not covered in ecgML (Wang et al., 2003).
As a matter of fact, the more is the emergence of
new technologies increasing the usage potential of
computer systems, the more there are usage
scenarios foreseen. As a result, further information
can be explored promoting then more useful
services. In this way, a data format for wrapping
biomedical signals, in fact, constitute an interface
between data acquisition and data usage systems
(see Figure 1). Therefore, such a data format should
not be a restrictive mean for useful data acquired
from sophisticated devices. As opposed, it should
abstract the complexity related to biomedical signals
acquisition to the health professionals’ environment.
This concern is particularly worth in context-aware
telemonitoring of patients’ heart relying on both
wireless and mobile technologies and devices and
the transmission of AECG. The existing ECG
standards, however, lack this concern and neither
were conceived from advanced modeling techniques
such as domain ontologies.
Figure 1: Separation between data acquisition and usage.
As an effort to cover this gap in literature, we
have carried out an extensive research on the
Electrocardiography domain. At this time, we have
developed an ECG domain ontology which is
presented elsewhere (Gonçalves et al., 2007), and
the ecgAware, a XML-based ECG data format
which is the focus of this article. The ecgAware
extends former standards especially by covering
AECG aspects related to context-aware
telemonitoring. On the next section we elaborate on
the ecgAware markup language, remarking the main
issues we have previously mentioned.
3 ECGAWARE
The ecgAware has a tree hierarchical structure which
is described in the following in a prefix way, i.e.,
expanding each significant XML complex element
on the left. The main elements are depicted on
diagrams in the figures 2 to 5. XML elements and
attributes are both referenced in bold and italic, (the
elements have the first letter capitalized); optional
elements or attributes are dotted in the diagrams.
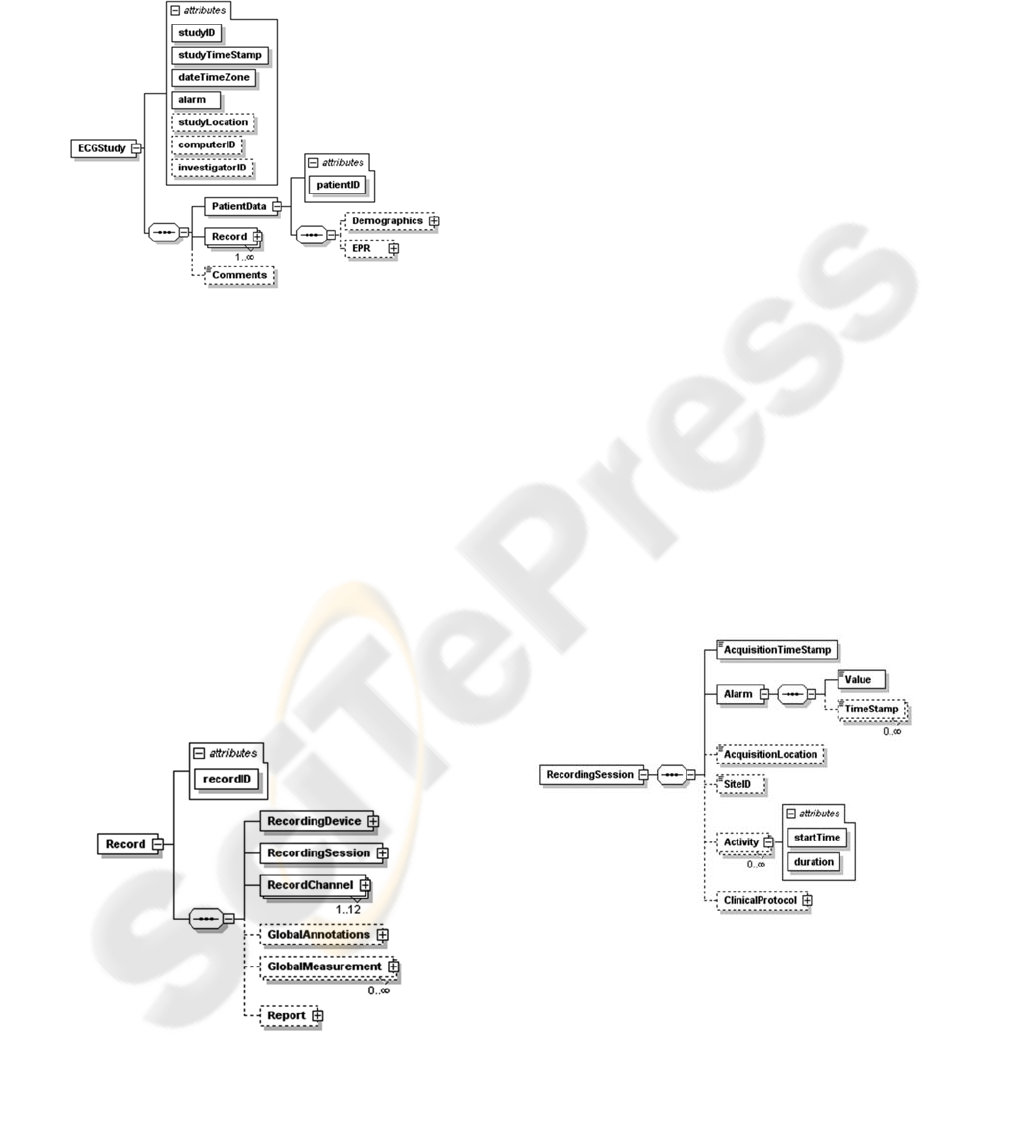
The ecgAware model constitutes an ECGStudy
(see Figure 2) of a single patient, which integrates
attributes that provide some prior data. These data
are studyID, a unique ID; studyTimeStamp, i.e.,
date and start time of the latest ECG record present
in the message; dateTimeZone, which supplies the
acquisition local time zone (based on SCP);
studyLocation, holding the latest location obtained;
the alarm attribute indicates that at least one record
inside the study contains an abnormal event, which
may be either detected by an ECG analysis system
or triggered by the patient. In case it is flagged true,
the ecgAware message supports an efficient
emergency service by the studyTimeStamp and
studyLocation attributes. Finally, computerID
identifies the machine where signal processing takes
place (based on SCP) and investigatorID is a unique
ID of the health professional which blames for the
ECG study (based on FDADF). ECGStudy has three
child elements: (i) PatientData, for patient’s
demographics data and electronic record; (ii)
Record, the ECG record produced in each recording
session; and (iii) Comments, for free text.
The Demographics element then comprises data
for identifying and contacting the patient (inspired
on ecgML); its child elements are Name, Sex, DOB
(date of birthday), Address, Phone, Fax and Email.
Meanwhile, EPR represents a basic patient’s
electronic record; it is composed by patient’s Height
and Weight; the boolean elements Hypertension,
Diabetes, Smoker and Alcohol
; Other for inserting
ECGAWARE: AN ECG MARKUP LANGUAGE FOR AMBULATORY TELEMONITORING AND DECISION
MAKING SUPPORT
39
other clinical data; and Comments, a free text field.
Demographics and EPR may be obtained by means
of a simple anamnesis. Those data are optional
because there may be situations (e.g. an emergency)
where there is no time for collecting them.
Figure 2: The ECGStudy root element.
ECG data are laid in the Record element (see
Figure 3). A recordID attribute identifies the record;
The RecordingDevice element describes the
acquisition device used to obtain the record (based
on FDADF) and filtering technique(s) performed by
it (based on SCP); RecordingSession bears the
recording session context, and is especially useful
for emergency services and decision support;
RecordChannel (min. one, max. twelve) constitutes
the ECG signal acquired through a channel;
GlobalAnnotations and GlobalMeasurement in turn
(inspired on FDADF and SCP respectively) are
annotations and measurements related to all leads;
and lastly, Report is a record finding carried out
either by a physician that interacts with a system or
by an analysis system to be further verified by a
confirming physician.
Figure 3: The Record element.
RecordingDevice has a deviceID to identify the
device by a serial number. It has also a Type, a
Manufacturer and a Model (e.g. Holter, Space Labs,
90205). The BaselineFilter, LowpassFilter and zero
or many OtherFilter elements constitute noise
filtering to overlook signal frequency components
over superior bounds and other filtering possibly
performed on the signal, respectively.
As we previously mentioned, patient’s heart
continuous telemonitoring can support diagnosis
and/or therapeutic treatment of the myocardial
ischemia. This is possible by means of a long-term
AECG RecordingSession (see Figure 4). With this
in mind, we included the Activity element, which
lays up a description of each activity performed by
the patient during the recording session (e.g. rest,
physical effort, etc). This information can be either
obtained by user interaction with the ECG
acquisition system (in replacement of the paper in
which patients used to populate his/her activity/time
over the recording session); or much better, acquired
by a sensor device such as a video camera jointly
with an eye-tracking system (Zhai, 2003), or by
other sensing techniques (Boudy et al 2006).
Still from a context-awareness standpoint, the
patient’s context during a recording session may be
used, for example, to guide an ambulance to the
patient’s location whenever an emergency takes
place. This sort of feature is possible thereby small
mobile devices which permit, nowadays, patient’s
vital signs and location telemonitoring even in
outdoor scenarios. That is why we included the
AcquisitionLocation element, which holds the latest
patient’s location acquired in a RecordingSession
from a device such as GPS.
Figure 4: The RecordingSession element.
Besides, AcquisitionTimeStamp hands over date
and start time of each session; Alarm flags on a true
or false Value for abnormal event(s) either identified
by an ECG real-time analysis system or triggered by
the patient, and keeps on zero or many TimeStamp
elements date and time of the detected event(s). In
case Alarm is true, on one side, an ecgAware
HEALTHINF 2008 - International Conference on Health Informatics
40

message comprising a partial record must be
transmitted as far as the abnormal event was
detected; on the other side, the whole ECG must be
recorded including all alarm events occurred during
the recording session related to it. Lastly, SiteID is
an abstract description of the place whereby the
session took place (e.g. domicile).
ClinicalProtocol, rather than in other ECG data
formats, is placed in the RecordingSession element.
Indeed, it is related to the meantime of a session
instead of a range of sessions. It then is composed by
DiastolicBP and SystolicBP, taken in the session at
some timestamp under a value unit; Medication,
specifying drugs which the patient has been using;
and finally, Sweaty and Pale (based on ecgML)
indicating true or false for abnormal sweat and
abnormal looking skin on the face, respectively.
The ECG signal is obtained from correlated
observation series taken at the same time by
electrodes placed on some positions on the human
body. These placements, when combined, provide
different viewpoints of the heart electrical activity,
i.e., the ECG leads. In Electrocardiography twelve
leads were standardized.
ECG data is thus laid up on
one or more (max. twelve) RecordChannel elements
(see Figure 5) standing for the leads. The Channel
element identifies the lead (e.g. Lead II); Waveform
contains the XY signal; ChannelAnnotations and
zero or many Measurement elements, in turn, are
annotations and measurements related to a lead (all
inspired on FDADF and ecgML).
The ECG samples are obtained from the
observations performed by the device over the time,
and thus constitute XY values. They are situated in
the Waveform element by XValues and YValues.
However, since observations are evenly spaced in
time, we do not need to store time values (XValues)
in the XML document. They rather can be easily
obtained by the Xoffset, Duration (of the record)
and SampleRate elements (all of them holding a
unit attribute). The sample values (YValues),
otherwise, must be covered in the XML Document,
even though there are different options to get it
done. Those values have also a unit and may be laid
up either (i) in an external file, which the link path is
indicated by FileLink; or (ii) by an integer series
IntValue (which can be easily converted to float by
using a scale); or even (iii) by a binary encoding
(BinaryData). Both IntValue and BinaryData are
composed by the From, To, Data and Scale
elements. They are respectively the beginning and
ending of the waveform in the X axis, the sample
values, and a scale factor to obtain the real number
of each value. The BinaryData has also a data
encoding attribute (e.g. Base64).
Figure 5: The RecordChannel element.
ChannelAnnotations mark significant events
identified on the waveform. They are carried out by
an author, which may be either a system or a
physician. Annotations may be either about points
(PointNotation) or time intervals (WaveNotaion).
The former involves a PointLabel describing the
point, an XValue, an YValue, and a Comment. The
latter in turn marks beginning, peak and ending time
values of one or more waves by the Onset, Peak and
Offset elements, respectively. Moreover, it holds
also an Interpretation (e.g. abnormal) of the
waveform in this time interval. It is worth to say the
WaveNotation element is basically addressed by the
elementary forms, or waves, which compose the
heart beat. They were defined by Einthoven in 1895
as PQRST; we can abstract the elementary forms by
Pwave, QRScomplex and Twave. Zero or many
OtherWave elements may also be considered. On
different leads, a specific elementary form can be
viewed in a better or worse way, exception by the
QRS complex, which can be well viewed through
whichever lead. This is the reason why we made
only the QRScomplex element required on
WaveNotation.
Besides annotations, zero or many
Measurement(s) can be made either of the duration
or of the amplitude of elementary forms. We can
distinguish that by means of the label and unit
attributes, e.g. P-duration and ms (based on ecgML
and SCP).
Global annotations and measurements, as
opposed to the channel ones, are related to all leads.
This sort of annotations then can be performed either
by a physician marking a vertical line correlating the
same XValue on all leads through an ECG viewer
application, or simply by a system from an average
of the correlated channel annotations. The
GlobalAnnotations element (inspired on FDADF)
thus discriminates itself from ChannelAnnotations
only by, on the former, all elementary forms are
required. The GlobalMeasurement element
(inspired on SCP), otherwise, has exactly the same
structure of the channel Measurement. The former,
however, is obtained from an average of the
correlated channel measurements.
ECGAWARE: AN ECG MARKUP LANGUAGE FOR AMBULATORY TELEMONITORING AND DECISION
MAKING SUPPORT
41
Finally, we have admitted a Report element to
provide a finding about the ECG record. This report
is carried out by an author which may be either a
system or a physician that has saw the record
through an application and then has edited it. The
finding comprises HeartRate, ElectricalAxis of the
heart, and Diagnosis.
4 USAGE SCENARIO
As part of a research program in healthcare and
bioengineering technologies at UFES, in Brazil, we
have been developed in the TeleCardio project a
context-aware system for remote monitoring patients
with cardiological syndromes (Andreão et al.,
2006a). In TeleCardio, the patient can have his/her
heart activity monitored anytime either in domicile,
ambulance, or outdoor scenarios. The TeleCardio
system carries out the transmission of the AECG in
combination with contextual data (e.g. location) in
order to allow physicians follow their patients’
condition in real-time and report diseases remotely.
TeleCardio, in fact, is a rich field for applying
ecgAware to wrap and deliver ECG signals, related
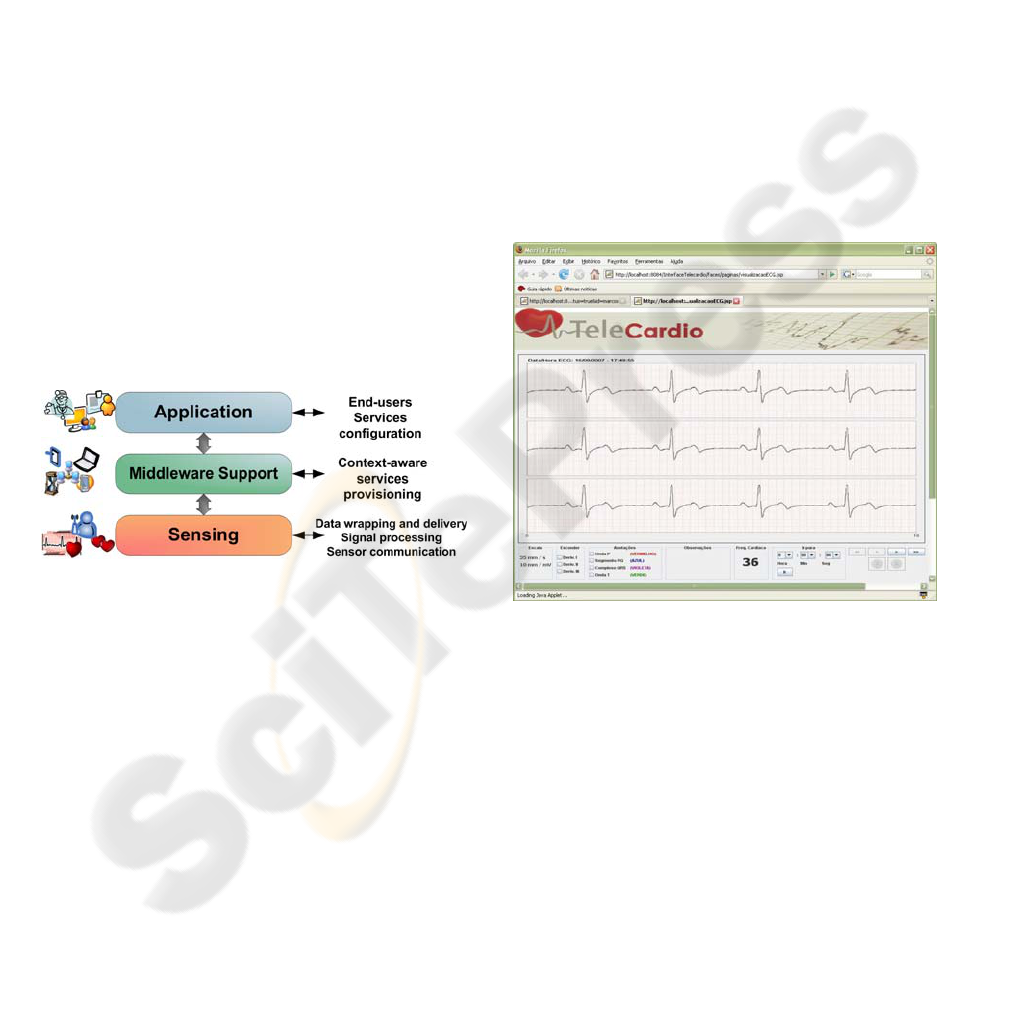
data and contextual data. The Figure 6 depicts the
TeleCardio architecture.
Figure 6: TeleCardio Architecture.
The Sensing layer comprises the ECG Wrapper,
an integrated system (hardware and software) for
acquiring the ECG signal from a Holter device. This
system handles wireless communication with the
device, signal processing, data wrapping and
delivery. One of the components of such system is
an ECG analysis software (Andreão et al., 2006b),
which makes use of an enhanced approach for ECG
classification and segmentation. This software thus
produces the ECG enhanced data for populating the
ecgAware model. The ECG Wrapper, in fact, hides
all complexity related to biomedical signals
acquisition for the middleware and application
layers by delivering ecgAware data to them.
The middleware layer, named Infraware (Filho et
al., 2006), provides context-aware services for
supporting client applications. Examples of such
services are: (i) to supply subscription management
for the health client applications as well as to
manage the interactions between these applications
and the ECG Wrapper; (ii) to guarantee privacy and
access control to patients, physicians, etc; (iii) to
guide an ambulance from the patient’s domicile to a
hospital by choosing the best traffic routes; and (iv)
interpretation of pieces of information in order to
trigger emergency services, e.g. when alarm is
flagged true.
The Application layer in turn addresses services
configuration, users’ profile and so on. The Figure 7
shows a web application that we have developed in
the TeleCardio project whereby physicians can view
the patients’ ECG signals and take advantage of the
ecgAware features. By means of such an application,
the physician can follow his/her patient’s heart
activity anywhere, anytime. In case an emergency
takes place, the physician is notified both by the
application (in case he/she is online on the system)
and by a SMS message his/her cellular phone.
Figure 7: Snapshot of the TeleCardio’s ECG viewer.
Because we are speaking of telemonitoring in
real-time, the ECG Wrapper has then to pack the
AECG record into small pieces of ecgAware data for
delivery by each 30 seconds. This time interval is
related to hardware optimal operation as well as the
emergency procedure. In fact, one could argue that
the XML format do not meet computational
efficiency as much as a binary format. Nonetheless,
we can overcome this either by using a binary file to
store and transmit the ECG XY data (see the
FileLink element) or by developing a compression
procedure in order to reduce the XML file. In
(Erfianto, 2004), for example, the compression
scheme has reached a reduction of up to 53% for
ECG data and 87,5% for patient data. The technique
HEALTHINF 2008 - International Conference on Health Informatics
42

used parses the XML document to an ASN.1 format
and, in the sequel, to a binary-encoded format.
5 FINAL CONSIDERATIONS
Currently we have advanced wireless and mobile
technologies and devices as well as systems that
carry out biomedical signal’s analysis through signal
processing algorithms. In this work we have argued
on the worth of taking advantage of such resources
in order to improve emergency services and decision
making support in the Healthcare domain. In this
way we can make the acquired sensor data much
more useful.
In the scope of Telecardiology, in particular, we
have elaborated in this paper how the existing ECG
data format standards lack this concern. We have
then proposed a novel ECG model striving not only
for application- and platform-independence and
focusing data content, but also admitting elements to
address telemonitoring concerns. As a result, we can
provide better emergency services and decision
making support, meeting then the requirements
related to pervasive scenarios in Healthcare.
The first usage results remarks ecgAware is
suitable for its purpose. After all, throughout the
TeleCardio evaluation we will test such data format
under an intensive usage by one or more medical
communities. Hence, we will have statistical metrics
to better evaluate it.
Former usage scenarios in Telemedicine, e.g.
remote reporting, are still covered by the ecgAware
data format. In fact, it embraces features of the
former ECG reference standards. Future usage
scenarios may cover other vital signs telemonitoring.
This is feasible by using the same research
methodology, i.e. exploring each biomedical signal
domain as we did in this work with the ECG.
Moreover, the XML technology provides flexibility
such that we can incorporate several XML schemas
to a root one. We thus can keep the elements
regarding telemonitoring, in general, and to design a
record structure for each biomedical signal we
choose to bear.
ACKNOWLEDGEMENTS
This work has received financial support from
FAPES (grant no. 31024866/2005) and CNPq (grant
no. 50.6284/04-2). The first author would like to
express his gratitude to Giancarlo Guizzardi for his
invaluable contribution to the progress of this work.
REFERENCES
Andreão, R. V., Filho, J. G. P., et al., 2006a. TeleCardio –
Telecardiologia a serviço de pacientes hospitalizados
em domicílio. In X Brazilian Conference in Health
Informatics (CBIS’06), Florianópolis, Brazil.
Andreão, R. V., et al., 2006b. ECG signal analysis through
hidden Markov models. In IEEE Transactions on
Biomedical Engineering, v. 53, n. 8.
Awareness project, 2007. http://www.freeband.nl/.
Boudy, J., Andreão, R. V., et al., 2006. Telemedicine for
elderly patient at home: the TelePat project. In
International Conference on Smart Homes and Health
Telematics. Belfast, Northern Ireland.
Brown, B., Kohls, M., Stockbridge, N., 2002. FDA XML
data format design specification. Retrieved August 9,
2006 from http://www.cdisc.org/discussions/EGC/
FDA_XML_Data_Format_Design_Specification_DR
AFT_B.pdf.
Clunie, A., 2004. Extension of an open source DICOM
toolkit to support SCP-ECG waveforms. In 2nd
OpenECG Workshop. Berlin, Germany.
Crawford, M., et al, 1999. ACC/AHA Guidelines for
ambulatory electrocardiography. In Journal of the
American College of Cardiology.
Erfianto, B., 2004. Design of a Vital Sign Protocol Format
Using XML and ASN.1. M. Sc. Thesis, University of
Twente, The Netherlands.
Filho, J.G. P., et al., 2006. Infraware: um middleware de
suporte a aplicações móveis sensíveis ao contexto. In
Proceedings of the 24
th
Brazilian Symposium of
Computer Networks, Curitiba, Brazil.
Fischer, R., Zywietz, C., 2003. SCP How to Implement -
Part I. Retrieved August 8, 2006, from
http://www.openecg.net/.
Goldberger A., et. al., 2000. PhysioBank, PhysioToolkit,
and PhysioNet: components of a new research
resource for complex physiologic signals. In
Circulation 101(23):e215-e220.
Gonçalves, B., et al., 2007. An electrocardiogram (ECG)
domain ontology. In Proc. of the 2
nd
Workshop on
Ontologies and Metamodels for Software and Data
Engineering (WOMSDE’07), João Pessoa, Brazil.
HL7 ECG Annotation Message v3, 2003. Retrieved
August 9, 2006, from http://wwwhl7.org/V3AnnECG/
index.htm.
Moody, G., and Mark, R., 2001. The impact of the MIT-
BIH arrhythmia database. In IEEE Engineering in
Medicine and Biology Magazine.
Standard communication protocol – Computer-assisted
electrocardiography N02-15, 2002. CEN/TC251
Secretariat. Retrieved August 8, 2006, from
http://www.centc251.org/.
Wang, H., Azuaje, F., Jung, B., Black, N., 2003. A
markup language for electrocardiogram data
acquisition and analysis (ecgML). In BMC Medical
Informatics and Decision Making 3:4.
Zhai, S., 2003. What's in the eyes for attentive input. In
Communications of the ACM, 46(3).
ECGAWARE: AN ECG MARKUP LANGUAGE FOR AMBULATORY TELEMONITORING AND DECISION
MAKING SUPPORT
43
