
PATIENT-CENTRED LABORATORY VALIDATION
USING SOFTWARE AGENTS
John McGrory, Frank Clarke
Dublin Institute of Technology, Dublin 8, Ireland
Jane Grimson
School of Computing, Trinity College Dublin, Dublin 2, Ireland
Peter Gaffney
Adelaide & Meath Hospital, Incorporating the National Children's Hospital (AMNCH), Tallaght, Dublin 24, Ireland
Keywords: Clinical laboratory validation, patient-centred, patient-focused, agents, computer-interpretable-guideline
(CIG), guidelines and protocols.
Abstract: Guidelines are self-contained documents which healthcare professionals reference to obtain knowledge
about a specific condition or process. They interface with these documents and apply known facts about
specific patients to gain useful supportive information to aid in developing a diagnosis or manage a
condition. To automate this process a series of Standard Operating Procedures (SOP) and workflow
processes are constructed using the contents of these documents in order to manage the validation flow of a
patient sample. These processes decompose the guidelines into workflow plans, which are then called using
condition triggers controlled by a centralised management engine. The software BDI agent offers an
alternative dynamic which more closely matches the modus operandi of narrative based medical guidelines.
An agent’s beliefs capture information attributes, plans capture the deliberative and action attributes, and
desire captures the motivational attributes of the guideline in a self-contained autonomous software module.
Agents acting on behalf of guidelines which overlap and interweave in similar domains can collaborate and
coordinate in a loosely coupled fashion without the need for an all encompassing centralised plan.
1 INTRODUCTION
The primary role of a clinical laboratory is to
support frontline healthcare professionals who are
licensed to deal with patients (McLoughlin, 2006).
Their function is to accept appropriate patient
samples, analyse them, and report their findings
back to the ordering clinician (Marshall et al., 1995).
The reported results are not considered a diagnosis,
but used by clinicians to deliver patient specific care.
In the majority of cases these results are use to aid in
planning treatments, quantifying medication
amounts and monitoring patient responses, which
could all have a detrimental affect on the patient if
incorrect information was used (Witte et al., 1997).
Therefore, the single most important activity
performed by the laboratory technologists is to
ensure their generated results are valid and plausible
for the specific patient from whom the sample was
taken.
Clinical guidelines are condition focused
documents through which domain specific aims,
goals, procedures, plans and normal reference ranges
are disseminated to healthcare professionals. The
purpose of these documents are to guide the reader,
and streamline activities around a particular medical
condition or process using evidence based
supportive information. When a clinical or
laboratory guideline is developed by an expert group
they focus on best practice for the specific condition
or process. They include all relevant knowledge,
logic and motivational aspects they deem necessary
to adequately describe the domain.
274
McGrory J., Clarke F., Grimson J. and Gaffney P. (2008).
PATIENT-CENTRED LABORATORY VALIDATION USING SOFTWARE AGENTS.
In Proceedings of the First International Conference on Health Informatics, pages 274-279
Copyright
c
SciTePress

Clinicians and laboratory technologists care for
patients not diseases or processes, therefore it is their
responsibility to filter through these guidelines
acting on a patient’s behalf. They must try interface
with these documents, to make use of the maximum
decision-making support for healthcare delivery
based on the known facts about their individual
patient. To automate this process of searching
through guidelines on a patient’s behalf, the
laboratory technologists in association with the
clinicians construct a series of Standard Operating
Procedures (SOP), and workflow processes using the
contents of these documents in order to manage the
validation flow of a patient sample. This is
accomplished by decomposing each guideline in to a
series of separate workflow activity paths. Then
develop a set of centralised management rules to
link these activities based on the presented patient
data. However, these procedures are not truly
patient-centred but process-centred. The guidelines
knowledge, logic and motivation can no longer be
accessed as a standalone resource, but as a series of
workflow triggers managed by a centralised
software package, which no longer resembles the
author’s guideline. This process is fundamentally
different to the true operation of a medical guideline,
where guidelines are used to provide supporting
information based on their holistic view of the
domain, rather than a series of linked activities
relating to a process. So is there an alternative
approach where the process can be distributed and
the guidelines retain logic, knowledge and
motivation as a standalone self-contained unit.
Agent oriented architectures operate on similar
principles to elements found in human decision-
making by combining attributes (beliefs), methods
(plans) and desires (goals). The BDI agent approach
in particular is based on the principle of a belief
capturing the informational attributes, the desire
capturing motivational attributes and the intention
capturing the deliberative attributes of an agent (Rao
et al., 1995). Therefore, agents can be considered
self-contained knowledge sources (KS), with a
social communication interface and have the ability
to act autonomously, or as part of a larger group. In
research completed by the authors it was shown that
a software agent can successfully capture and be
encoded with the knowledge, logic and motivation
of a guideline (McGrory_a et al., 2008). In
additional research completed by the authors it was
shown that although agent communications provide
a facility to transmit data between agents, it is also
used to provide a social and collaborative aspect
(McGrory_b et al., 2008). This allows the separate
agents work in groups and collaborate on shared
goals. This later research also demonstrated that
agent communication was capable of being adapted
to comply with a medical standard for
communication (i.e. CEN ENV 13606-4:1999).
The thrust of this paper is to illustrate that
software agents offer an alternative approach to
reproduce the function of medical guidelines than
the more commonly used centralised approaches.
This paper also presents an operation of a
framework which allows these agents coordinate and
collaborate to validate a patient sample in a
distributed fashion, without the need for a
centralised all encompassing plan.
2 ANALYSIS OF GUIDELINE
REPRESENTATION FORMATS
The traditional approach to combining separate
bodies of knowledge (such as guidelines) together is
to decompose the knowledge and logic into separate
workflow activities and link these activities together
using a centralised inference engine. Three
commonly used techniques are rule base, direct
coupling or blackboard systems.
The rule-base approaches are designed around a
nodal tree, where expert knowledge in the form of a
workflow activity is the branch, and the selecting of
a particular branch at each node is based on patient
information or process data. Although selecting rules
based on presented facts during execution can be
indicative of an illness, the rules which link them
directly to a diagnosis do not reflect anything deeper
than a casual understanding of human physiology.
These systems are centralised and the original
guideline knowledge is now absorbed within a
labyrinth of rules.
Direct coupling architectures are made up of a
group of separate expert knowledge modules. Each
expert knowledge module contains local storage, a
KS and a control switch to link to the other software
modules according to their data-flow requirements
using a direct call or link (Corkill, 2003).
Complications arise when specific modules are
subject to change and/or when the ordering of
module control switching cannot be determined until
run-time (Kavanagh et al., 2002). As the system
expands and evolves the links change and the
process becomes unwieldy and unmanageable. In
addition to the aforementioned issues, the direct
coupling model does not provide a clear
PATIENT-CENTRED LABORATORY VALIDATION USING SOFTWARE AGENTS
275
representation of the overall problem, and there is
nothing more than relationship links used.
The blackboard model is based around three
components: KS, control element and the blackboard
(Turban et al., 2005). The KS is an expert at solving
specific elements of the overall problem. The
blackboard, acts as a central repository for data,
partial solutions and control information. The
blackboard also acts as a communication medium
for the transfer of information, and a KS triggering
mechanism. The control element directs the
problem-solving process by allowing KS’s to
respond to blackboard changes, and it selects the
most appropriate KS to be executed next, as shown
in Figure 1. After completing a task the KS reports
back to the blackboard and returns control to the
control element. KS’s are not aware, and cannot
communicate with other KS’s directly. They know
nothing about the other experts (e.g., what
parameters they use, what processes they perform, or
what services they provide). The blackboard
architecture tends to be a labyrinth of different
configurations, levels of abstraction, and partial
solutions which are orchestrated to provide a flexible
problem solving mechanism. The blackboard system
eliminates the communication issues raised by the
directly coupled monolithic model, and gives a
representation of the problem to be solved to all
participants. But the blackboard does not have the
capacity to indicate how group members can
collaborate to solve a problem, but can only select
from partial solutions it already possesses.
Dietician
Knowledge
Source
Diabetes
Knowledge
Source
GP
Knowledge
Source
Renal
Knowledge
Source
Interaction
Interaction
Interaction
Interaction
Blackboard Control
Plans
& Logic
Local
Blackboard
Manager
Dietician
Knowledge
Source
Diabetes
Knowledge
Source
GP
Knowledge
Source
Renal
Knowledge
Source
Interaction
Interaction
Interaction
Interaction
Blackboard Control
Plans
& Logic
Local
Blackboard
Manager
Figure 1: Blackboard Management Communications.
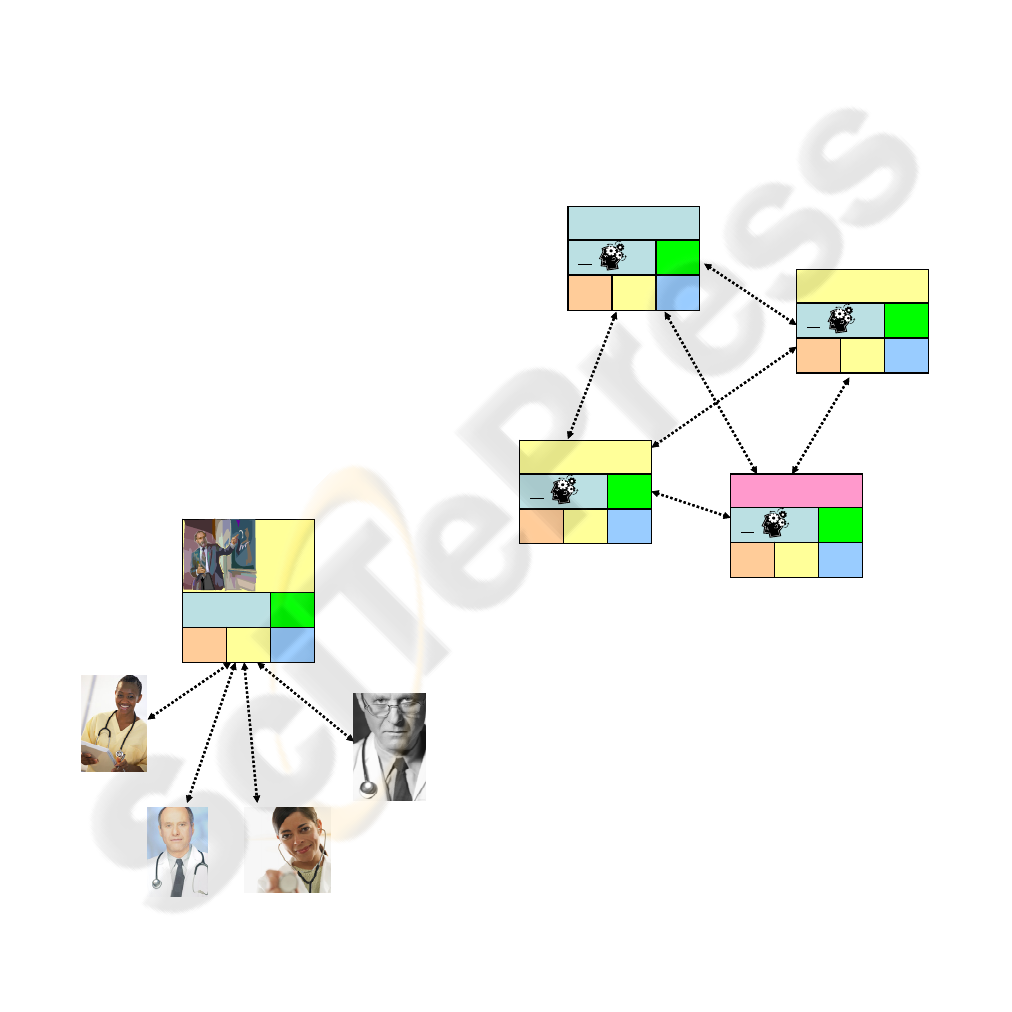
3 DESIGN OF A GUIDELINE
AGENT
The agent approach is based on the principle that
each agent can represent a single guideline. It
captures all the guidelines knowledge, logic and
motivation. In addition to this the agent has a rich
communication facility where data and social
interaction between separate agents can take place.
But how does each agent know what the other is
doing since there is no centralised all encompassing
plan? If the blackboard is simply a repository of
information, although layered to some degree, there
is no absolute necessity for it to be in a single
location. Therefore, it is possible to replicate a copy
of the blackboard within each Autonomous
Socialising Knowledge agent (ASK-agent) as shown
in Figure 2.
Interaction
Blackboard Control
Knowledge
Source
BDI
Local
Dietician Guidelines
AGENT
Blackboard Control
Knowledge
Source
BDI
Local
GP Guidelines
AGENT
Blackboard Control
Knowledge
Source
BDI
Local
Diabetes Guidelines
AGENT
Blackboard Control
Knowledge
Source
BDI
Local
Renal Guidelines
AGENT
Interaction
Blackboard Control
Knowledge
Source
BDI
Local
Dietician Guidelines
AGENT
Blackboard Control
Knowledge
Source
BDI
Local
GP Guidelines
AGENT
Blackboard Control
Knowledge
Source
BDI
Local
Diabetes Guidelines
AGENT
Blackboard Control
Knowledge
Source
BDI
Local
Renal Guidelines
AGENT
Figure 2: Autonomous Socialising Knowledge agent
model.
Each ASK-agent now contains a localised
blackboard, knowledge source, localised beliefs,
localised control and its own inference engine. The
retention of the motivational component of the
guideline within the ASK-agent is fundamentally
different to the centralised approach of other
systems. This allows the ASK-agent to act
autonomously on behalf of the guideline in a self-
contained capacity. When patient specific
information is presented to the individual agents,
they have the ability to apply their encoded
knowledge and logic, and provide a supportive
response based solely on that information. Using this
approach an ASK-agent module can make use of the
maximum supportive response from the other
HEALTHINF 2008 - International Conference on Health Informatics
276
separate ASK-agent’s based on the known facts
about the individual patient. By providing a
framework which allows separate ASK-agent
broadcast supportive communications to each other,
the agent approach offers the opportunity for the
data to be validated in a patient-centred fashion. But
how can these separate, autonomous, self-contained
ASK-agent modules share data, work in groups or
collaborate to solve a problem.
3.1 Agent to Agent based Activity
A theory which can aid issues relating to
collaborating guidelines is Activity Theory (AT)
which emanated through the social sciences. AT
focuses on the collaborative nature of separate
autonomous systems such as individuals (Engestrom
et al., 1999), on which agents are based, and have
the capability to perform certain tasks as part of a
group. Agents synthesise human decision-making
through their goal, plan and belief elements, but do
not explicitly detail how they can socialise or
collaborate. AT in itself does not provide an output
which can be exactly transposed into computer
software, but does provide a useful framework based
around interfacing interaction and collaboration of
software modules. These interfaces can be used to
develop an increased sense of interaction and
collaboration ability in autonomous modules using a
software program independent approach.
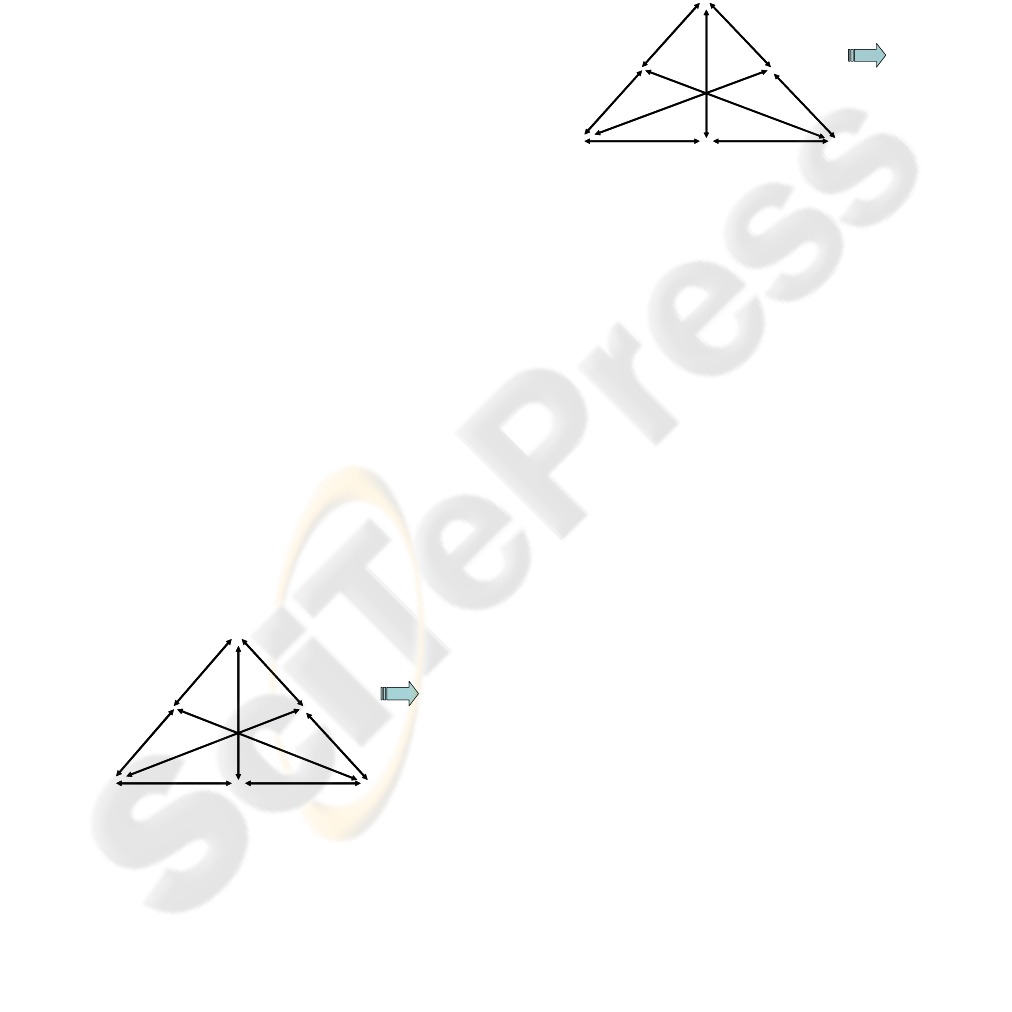
The structure of human activity according to
Engestrom can be compartmentalised using rules,
community, subject, object, division of labour and
instruments. AT is an iterative process where an
activity is developed from a simple low level
activity to a higher level activity.
Instruments
Artifacts i.e. laboratory results
Division of
Labour
Using message content
such as LiverDisease
alerts other agents to get involved
Rules
Rules acted by the ALK_P agent
By the community
By the object
Community
Liver experts
GGT agent, ALT agent, Protein Agent
Subject
ALK_P agent
Object
The human body
Outcomes
Instruments
Artifacts i.e. laboratory results
Division of
Labour
Using message content
such as LiverDisease
alerts other agents to get involved
Rules
Rules acted by the ALK_P agent
By the community
By the object
Community
Liver experts
GGT agent, ALT agent, Protein Agent
Subject
ALK_P agent
Object
The human body
Outcomes
Figure 3: Low level activity.
In terms of medical guidelines the iterative
process dynamic exists by virtue of the design of
guidelines and their focus on a condition, disease or
organ. Consider for example, a low level
implementation activity being the guideline behind
the validation of a single analyte result, say Alkaline
Phosphates as shown in Figure 3. A higher level
implementation is where the result is combined with
some other single analyte results, such as Bilirubin
and GGT, to perform and aid in the reporting of a
Liver Function Test as shown in Figure 4. The Liver
Function Test is then part of a higher level suite of
tests for other medical disorder classifications.
Instruments
Artefacts i.e. diagnosis liver dysfunction
or indication LiverDisease
Division of
Labour
Using message content
such as Hepatitis
alerts other agents to get involved
Rules
Rules acted by the Liver Expert
By the community
By the object
Community
Experts associated with the liver
Dietician expert agent, Kidney expert agent
Haematology Expert agent
Subject
Liver Expert agent
Object
The human body
Outcomes
Instruments
Artefacts i.e. diagnosis liver dysfunction
or indication LiverDisease
Division of
Labour
Using message content
such as Hepatitis
alerts other agents to get involved
Rules
Rules acted by the Liver Expert
By the community
By the object
Community
Experts associated with the liver
Dietician expert agent, Kidney expert agent
Haematology Expert agent
Subject
Liver Expert agent
Object
The human body
Outcomes
Figure 4: High level activity.
One guideline does not cover the whole body,
but more specifically focuses on an abstract
conceptualisation of body components (e.g., liver
function in a group of male diabetes patients).
Another guideline relates to the same body
component but from a different abstract
conceptualisation viewpoint (e.g., kidney function in
a group of male diabetes patients). Although the two
guidelines are separate autonomous documents they
are linked by virtue of their domain of discourse.
Therefore, a link between different guidelines
already exists within the guideline document itself.
The overlapping knowledge is provided in two main
forms. The first is in the form of similar domain
knowledge that uses alternative inference
mechanisms in order to derive a result (i.e. both
statistical and rule-based inference engines being
able to validate the same result). The second is in the
form of overlapping knowledge which observes
different viewpoints of the same domain. For
example, the kidney filters toxins from the blood
passing it to the urinary tract. As the kidney is such
an integrated organ in the body there are many
guidelines describing its operation from different
viewpoints such as blood filtering, urinary tract,
autoimmune disorders etc. Using this approach the
organ disease or condition is described from
different viewpoints through various guidelines.
Each guideline describes different knowledge, logic
and motivational aspects associated with the organ.
Therefore supportive information can be exchanged
between these guidelines in order to aid in
PATIENT-CENTRED LABORATORY VALIDATION USING SOFTWARE AGENTS
277
describing the operation of the organ, or in the
validation of a sample result.
3.2 ASK-agent Model
To utilise this overlapping knowledge link a social
structure was developed to manage the interfacing
between agents. This social interface took the form
of a mandatory set of searchable service
descriptions, beliefs and actions. The service
descriptions (i.e. Name, Type, Ownership,
GuidelineReference, InformationNeeded,
ValidationType, EndResultType, Ontology and
Language) permitted each agent to be located within
the agency platform through the Directory
Facilitator (DF) (a feature of the Foundation for
Intelligent Physical Agents (FIPA) standard offering
searchable goldenpages facility to locate agents)
(McGrory_a et al., 2008). The beliefs (i.e.
CurrentlyValidating, PlausibilityScore and localised
blackboard) permit the ASK-agent to interact with
other group members. The actions relate to
automated responses the ASK-agent must return to
other agents when queried (e.g.
CurrentlyValidating), and the sending of
information to other agents it believes should be
reported (e.g. it determined the presence of liver
disease during its deliberation). Therefore, each
ASK-agent only needs to know its overlapping
neighbours, which it can find and interact with using
the agent platforms DF and message passing. With
access to supportive and overlapping knowledge it is
not necessary to have a single all-encompassing rule
set to manage the ASK-agents interaction.
The fundamental concept of the ASK-agent
system proposed in this paper is to allow
components to collaborate and share supportive
information without having to explicitly disclose
their position as part of the large encompassing
community. An ASK-agent does not need to identify
exactly what every other agent is doing; only what
its neighbours (i.e. neighbours it interfaces with) are
doing. To illustrate this point further and
demonstrate some boundaries, consider the example
of a jigsaw with 500 pieces. A jigsaw piece has two
discrete dimensions: the irregular shaped edge
containing four sides, and the image printed on the
face. To solve the puzzle, a person directly matches
individual jigsaw pieces onto the jigsaw image, say
the image shown on the box. Each piece is identified
using the image on its face and placed in the
appropriate position. This method requires a view of
the whole system to be presented before starting, but
involves no greater skill than straightforward pattern
matching. An alternative approach is to use a
combination of the localised image on the face of the
piece and its four corners to match it to a suitable
neighbour (i.e. matching the shape of the pieces
together). Jigsaw assembly using these interfaces do
not require the full picture to be known. Using the
jigsaw example as a solution metaphor, the heart and
lungs image depicted in Figure 5 is a symbolic
representation of the heart and lungs as a whole, not
just the image it represents. The agent was not
intended to be a large all encompassing structure,
but a group of loosely coupled autonomous expert
knowledge sources (represented by each jigsaw
piece) which could be readily and easily interfaced
with as shown in Figure 5. The ASK-agent only
needs to know its neighbours (i.e. the expert it
interfaces with), in a similar way the jigsaw piece
only needs to know another piece with similar edge
profile and compatible image, not the whole picture.
The ASK-agent does not need to know anything
about any other piece of the jigsaw only its
interfacing neighbours. The interface can be
considered the ontology, overlapping facts, common
laboratory results and various viewpoints of the
universe of discourse. This is analogous to the
jigsaw edge shape profile.
Figure 5: Jigsaw metaphor representing agent components
of the heart and lungs.
4 CONCLUSIONS
This research demonstrates the agency approach
offers a facility to manage and interface with
medical guidelines electronically, in a similar modus
operandi to original guideline documents. This is
because of the synergy between the knowledge base,
plans, decisions, action, goals and the self-contained
nature components between guidelines and agents.
HEALTHINF 2008 - International Conference on Health Informatics
278
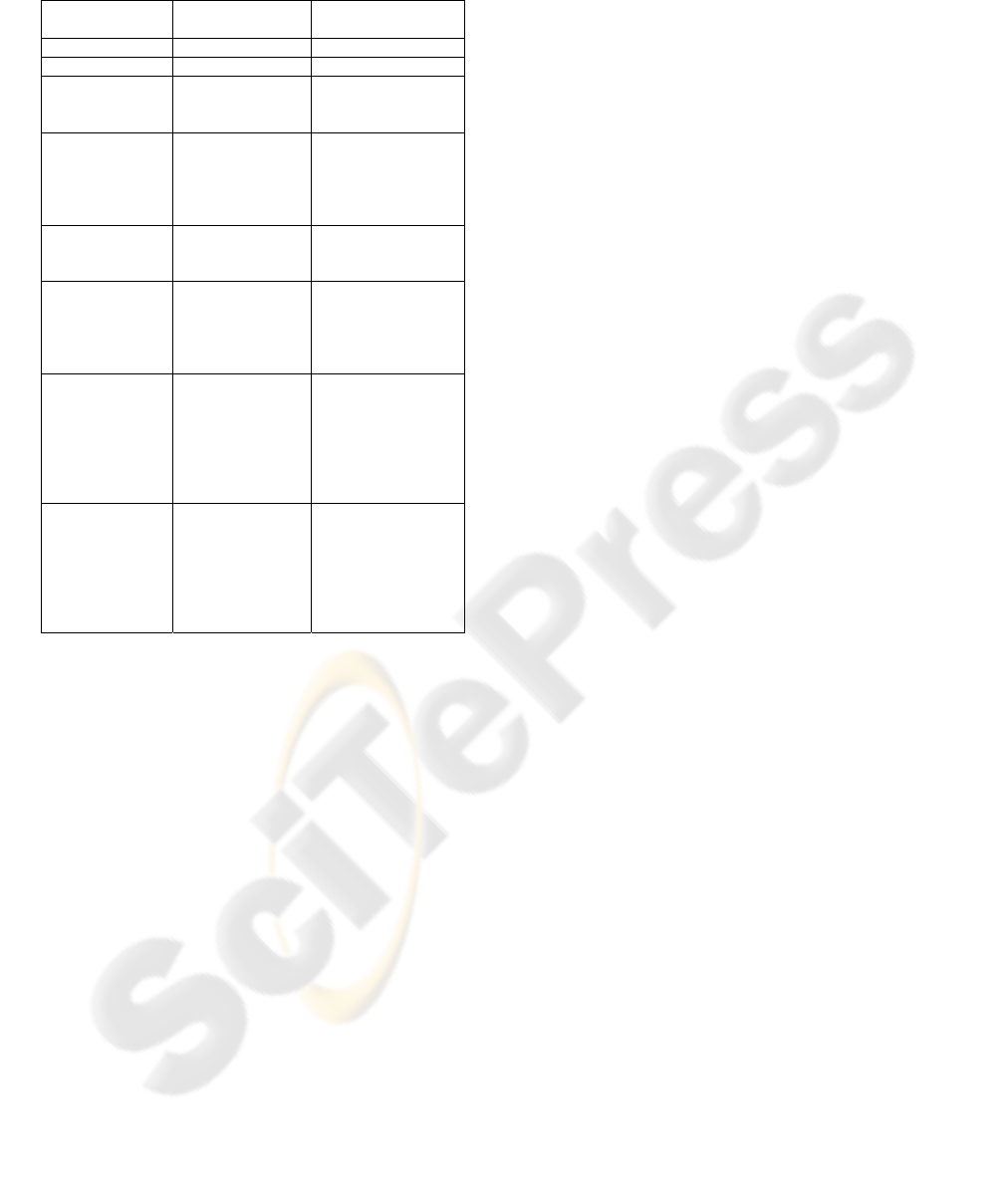
Table 1: Summary of centralised and ASK-agent
approach.
The agents can be encoded to reproduce the beliefs,
desires and intentions of the narrative guideline and
act accurately, faithfully and autonomously on
behalf of that document. This body of knowledge
and logic can then be interfaced with, whenever that
information needs to be accessed. The addition of
activity theory and in particular the iteration model
concept showed that the guideline documents
already contain aspects that link them together.
Using these links and the developed social
communication the ASK-agents can locate, access,
communicate, collaborate and coordinate activities
between each other. This allows supportive
information exchanges to be completed between
separate expert agents about an individual patient,
without the need for an all encompassing centralised
plan. In cases where there is an inconsistency in held
patient specific information, this agent approach
offers an advanced, robust and efficient patient
centred validation alternative to existing approaches.
However, if overlapping knowledge between
guidelines is not available the links created using
this approach are not present and the separate
guidelines are standalone islands of information. The
guidelines knowledge, logic and motivations are still
accessible as a standalone entity, but other agents
would need to be created to provide the links.
Developing a system using the latter approach still
permits distributed processing to be accomplished,
but not without a source of knowledge to provide the
links. A summary of the differences between the
centralised and ASK-agent approach are given in
Table 1.
REFERENCES
Corkill D., 2003. Collaborating Software Blackboard and
Multi-Agent Systems & the Future. Accessed via
www.cs.umass.edu, Proceedings of the International
Lisp Conference published in October 2003.
Engestrom Y., Miettinen R., Punamaki R. Perspectives on
Activity Theory. Published by Cambridge University
Press January 1999. ISBN13: 9780521437301.
Kavanagh M., Price S., “The quest for a computerized
guideline standard: The process, its history, and an
evaluation of the most common and promising
methods used today”, Capstone Project documentation
2002.
Marshall W.J., Bangert S.K., 1995. Clinical Biochemistry,
Metabolic and Clinical Aspects, ISBN 0 443 043 418,
published in 1995 by Churchill Livingstone.
McGrory_a J., Grimson J., Clarke F., Gaffney P., “Agents
representing medical guidelines”, HEALTHINF 2008
International Conference on Health
informatics, Funchal, Madeira, Portugal, January
2008.
McGrory_b J., Grimson J., Clarke F., Gaffney P.,
“Communication of medical information using
agents”, HEALTHINF 2008 International Conference
on Health informatics, Funchal, Madeira, Portugal,
January 2008.
McLoughlin V., Millar J., Mattke S., Franca M., Jonsson
P., Somekh D. and Bates D., 2006. Selecting
indicators for patient safety at the health system level
in OECD countries. International Journal for Quality
in Health Care 2006 18(Supplement 1):14-20.
Rao A., Georgeff M., 1995. BDI Agents: From Theory to
Practice, proceedings of the first international
conference on multi agent systems (ICMMAS-95) San
Francisco USA 1995.
Turban E., Aronson J.E., Liang TP., Decision Support
Systems and Intelligent Systems. published in 2005 by
Pearson Prentice Hall, Seven Edition, ISBN 0-13-
123013-1, Chapter 10, pgs 538-570.
Witte D.L., VanNess S., Angstadt D., and Pennell B.J.,
1997. Errors, mistakes, blunders, outliers, or
unacceptable results: how many? Published by
Clinical Chemistry 1997; Vol:43 pgs 1352-1356.
Element Centralised
Approach
ASK-Agent
Multi-ontologies No Yes
Processing Centralised Distributed
Requirement for
overlapping
knowledge
None Required to provide
the links.
Addition,
altering or
removal of
guidelines from
the system
Any changes
require
centralised
inference to be
recompiled.
Each ASK-agent is
independent and
loaded separately.
System
resilience
None Yes, all ASK-agents
have a copy of the
blackboard.
Independent
accessible
knowledge
None. All access
to information
through the
centralised
engine.
Yes, all ASK-agents
are independent.
Information
accessed via
message passing.
Clinician having
access to
specific
guideline
knowledge
A clinician
cannot access
knowledge
directly.
A clinician can
access each ASK-
agent via a message
and directly access
the specific
guideline
knowledge.
Method of
collaboration
Direct links using
the centralised
engine.
Using the
mandatory beliefs,
action and
descriptions in the
agent platforms
Directory
Facilitator.
PATIENT-CENTRED LABORATORY VALIDATION USING SOFTWARE AGENTS
279
