
Data driven process modelling for a
hospital emergency department
Andrzej CEGLOWSKI, Leonid CHURILOV, Jeff WASSERTHIEL
Monash University Melbourne, Australia
Abstract. This paper describes how key activities in the emergency department
of a major hospital were extracted from workflow history. Analysis of these
activities help with modification of both administrative and clinical actions for
improved efficiency and effectiveness. Extraction of process from data is a
relatively new field. This paper’s contributes the innovative determination of
processes through data mining, rather than the algorithm-driven approach used
to date. Data about patients who present to a major hospital emergency
department were used to define clusters of patients who follow common
pathways through the emergency department. It is discussed how these
“process based” clusters can be used for performance management of the
emergency department through evaluation of process inputs, outputs and costs.
1 Introduction
Australian federal and state governments provide funding for public hospitals
determined primarily on performance or output, rather than negotiation, history or
politics. Clinical and resource homogeneous groups of patients are determined from
stored information about patient visits and related to the resources required (Duckett
1998). Homogenous grouping of patients have become known as “casemix” to
emphasise the grouping based on similar patient “cases”.
The casemix approach has been reasonably successful in predicting resource
requirements for inpatient acute care settings, and it now forms a significant part of
improvement and management activities (Australian Department of Health and Aging
2003). However, classification of patients who present to emergency departments (a
hospital department that specialises in providing care for people who are in need of
urgent care) has proven to be difficult, with the best groupings only accounting for
some 60% of cost (Bond et al. 1996).
Casemix for emergency department (ED) patients is important because the ED is
one of the main routes for admission into Australian hospitals and is becoming a
primary source of health care. There have been large increases in presentations to
EDs in recent years (Acute Health Division 2001), leading to longer waiting times,
patients being directed to alternate facilities, and other issues that have the potential to
affect the ability of the ED to save lives. Analyses that treat the ED as a component
within a complex healthcare system and the simulation of patient flows within EDs
CEGLOWSKI A., CHURILOV L. and WASSERTHIEL J. (2004).
Data driven process modelling for a hospital emergency department.
In Proceedings of the 1st International Workshop on Computer Supported Activity Coordination, pages 61-70
DOI: 10.5220/0002667800610070
Copyright
c
SciTePress

have contributed greatly to understanding of ED dynamics (Lane et al. 2000), but the
absence of an acceptable patient classification limits the accuracy of these methods
and ability to satisfactorily account for resource use.
Traditionally, casemix has been based on a combination of clinical information
(diagnoses and procedures) and demographic information (age and sex), to result in
homogeneous groups with respect to a target variable such as pattern of illness or
treatment (Jelinek 1995). Generally the similarities between patients relate to
diagnosis, working under the assumption that patients with related diagnoses follow a
matching course of treatment and utilise comparable resources. Essentially, casemix
strives to yield treatment pathways for patients without explicitly defining the
processes incorporated in those pathways – patients are grouped by function
(diagnosis), yet the groups are expected to yield a process perspective with associated
inputs, outputs and resource requirements.
Since the ED forms such a significant part of the healthcare chain, both in terms of
number of patients and potential for life-critical incidents, it is the objective of this
paper to present a more effective approach to classification of ED patients. This
approach takes a process view. Patients who follow similar processes are likely to
consume similar resources. A process based classification can be used to improve
understanding of patient flows through the ED, and help with facility design,
information system design, resource allocation, reengineering of processes, and
training of staff.
The approach described in this paper is a fundamental departure from existing
casemix for ED patients, presented as follows: Section 2 provides background to the
problem, and looks at related research. The data and methodology is explained in
Section 3. Section 4 supplies the clustering results and compares them to existing
proposals. Section 5 discusses the insights supported by these results and mentions
extensions to the work. The paper concludes with a caution about ED process
modification.
2 Background and previous work
There has been much simulation and systems research into hospitals and healthcare
(Jun et al. 1999; Preater 2002) in an effort to prevent excessive patient waiting times
and the redirection of patients and ambulances to other ED facilities. The general
conclusion has been that ED problems cannot be treated in isolation as this simply
moves the pressure point within the healthcare system. (Lane et al. 2000; Acute
Health Division 2001).
Improving the efficiency and effectiveness of public hospital services in Victoria is
being addressed by the “Designing Care” program which aims to redesign processes
across the whole health system (Victorian Department of Human Services 2002a).
The ED component of “Designing Care” emulates and duplicates ED initiatives that
have been successful in other countries and at other hospitals in Australia. These
include “fast tracking” of certain patients, decreasing ED volume, and providing
62
increased supervision of junior medical staff (Victorian Department of Human
Services 2002b).
Much work has been done in Australia on determination and agreement of casemix
for inpatient classification (Hanson 1998; Australian Healthcare Association 1999;
Funding & Financial Policy Branch 2002). Work started in late 2002 on a national
ED patient classification, with initial efforts concentrating on identification of
appropriate ED data to include (McAlister 2003). Patient classifications have been
proposed to aid with ED performance evaluation (Cameron et al. 1990).
Characteristically, proposals have grouped ED patients according to combinations of
age, urgency of complaint, diagnosis, time in ED and outcome of visit.
A Perth study recorded diagnoses and urgency for ED patients attending four
hospitals to develop the typical casemix for the hospitals. In a second phase, resource
use was measured for patient attendees to ED and related to the typical casemix
(Jelinek 1995). In a later Flinders study, costs were measured for some 17800
patients. Key variables were identified by univariate analysis as cost drivers for ED
patient attendance. The cost drivers were urgency, outcome, age, diagnosis and
treatment time. A classification tree was built from the cost drivers to determine the
minimum number of clusters that could account for most costs (Bond et al. 1996).
These classifications are inadequate to describe a significant number of activities
within EDs (Table 1).
Data mining and neural networks offer alternative approaches to data analysis.
Cullen (2001) used data mining for intelligent feature selection in healthcare. Other
data mining in healthcare research relates to investigation of symptoms and treatment
(Brossette et al. 2000; Riano and Prado 2000; Lin et al. 2001; Richards et al. 2001;
Isken and Rajagopalan 2002; Lee et al. 2002; Williams et al. 2002; Chae et al. 2003).
Abston (1999) applied neural networks and other methods to model the
pharmacological management of acute myocardial infarction in an emergency
department and concluded that the data most descriptive of and pertinent to clinical
decision-making seems to be left out of data collected each day in the clinical setting.
Abston’s conclusion highlights the difficulty of grouping ED patients according to
clinical decisions and underscores the need for a change in approach from classic
casemix models.
Since this paper involves a process-driven approach to clustering, it is necessary to
introduce the relatively new area of process mining. Process mining involves the
analysis of data about a process to learn about underlying patterns of activity (List et
al. 2001). The result of this analysis are patterns of activity that are objective because
they are based on the actual things that took place (Department Technology
Management 2003). It is possible to identify the most frequent pathways through a
process. Each of these key pathways may be viewed as recurring patterns of activity
that may be analysed to identify inputs, outputs and cost structures, or to identify
clusters of transaction types.
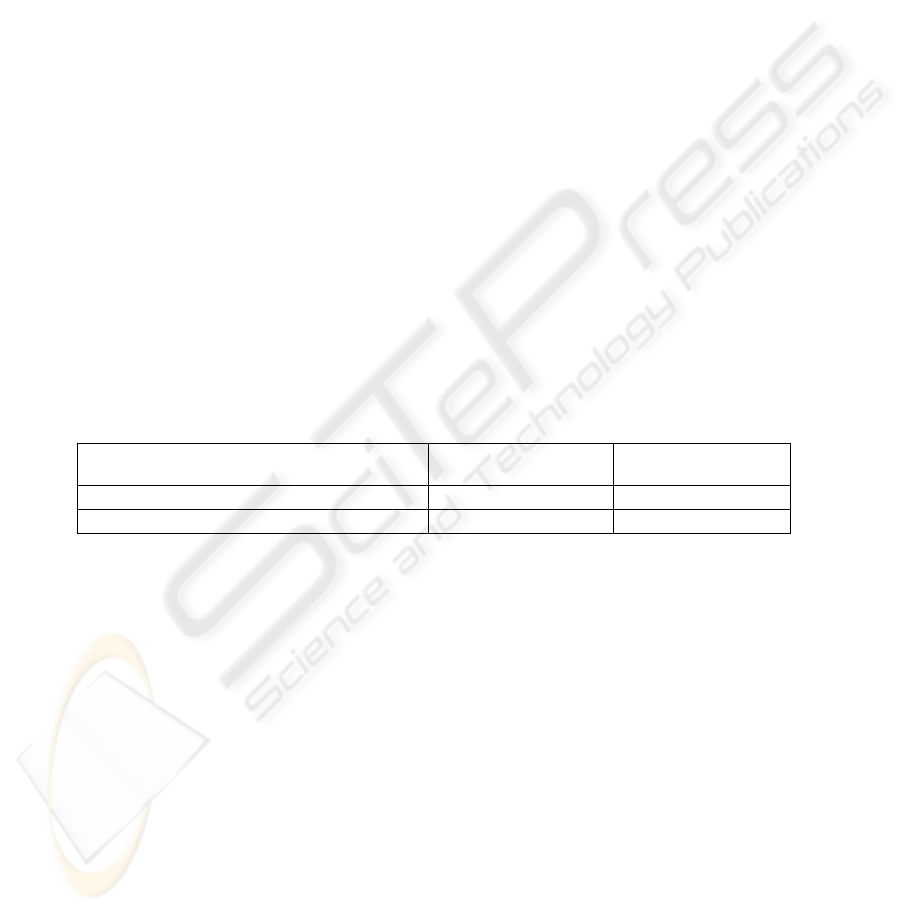
Table 1: Comparison of cost variance reduction in ED casemix (Bond et al. 1996)
ED Casemix system Flinders Medical
Centre Study (1996)
Perth Study (1992)
Urgency and Disposition groups (UDGs) 43.9% 47.4%
Urgency Related Groups (URGs) 55.3% 57.6%
63

The context of the problem and the preceding works led to questioning whether
clusters of activity could be extracted from ED data to yield homogenous clusters of
ED patients. The activities involved in treatment would be the same for each cluster
so each cluster could be considered to have matching inputs, outputs and resource
consumption. The activities associated with each cluster would comprise activities in
the process of treating patient instances within that cluster, so process and workflow
perspectives could be used to improve understanding of patient flows through the ED.
This is process mining with a view to achieving casemix outcomes. The data used
and methodology is discussed in the next section.
3 Methodology
The data came from a major city hospital who is partner in this project. The data was
comprised of de-identified records of all ED presentations between 1999 and 2002.
These records uniquely identified each visit by an ED reference number, and retained
codes that permitted identification of repeat visits. The records contained
demographic information plus details of the visit such as apparent severity of
complaint, key time points and outcome. Initial investigations were limited to
random samples within the 56906 records in the 2002 cohort to limit effects of inter-
year changes to activities within ED.
It has been seen in the preceding section that previous attempts at identifying
casemix for ED patients grouped patients by cost based on urgency and diagnosis,
sometimes combined with demographic information, such as age. Since cost data was
not available, it was not possible to duplicate past studies, however effort was made to
emulate the groupings using Classification and Regression Trees (CART) and Self
Organising Maps (SOM).
CART and SOM are nonparametric grouping methods that seek to minimise
diversity within groups and maximise differences between dissimilar groups. The
grouping is algorithm-driven, not supervised, so is often referred to as “self-
organisation”. Nonparametric grouping relies on data, rather than domain-specific
expertise. The methods generally employ large datasets, work well with many input
variables and produce arbitrarily complex models unlimited by human comprehension
(Kennedy et al. 1998).
• The CART algorithm builds a binary decision tree through brute force. It performs
splits based on an exhaustive search of all variables to find an optimal splitting rule
for each node. The resultant tree is then pruned to improve overall classification
accuracy (Kennedy et al. 1998).
• SOM provide a visual understanding of patterns in data through a two dimensional
representation of all variables. Records that have similar characteristics are
adjacent in the map, and dissimilar records are situated at a distance determined by
degree of dissimilarity. The SOM algorithm repeatedly repositions records in the
map until a classification error function is minimised (Kohonen 1995).
In order to facilitate a process-focused approach, a separate data file was obtained
that contained the ED reference number linked to one of 57 procedures (investigations
such as blood analyses and x-rays, or activities related to treating the patient such as
suturing). This data was combined with the records of ED presentations so that each
64
record now contained demographic and visit information, plus all procedures
undertaken during that visit. Working under the presumption that resource use for
each patient could be linked to number and type of procedures, it was hoped that
discrete groups of procedures could be identified across all records with two or more
procedures (Table 2) that would result in “primary pathways” patients take through
the ED, in essence providing a set of core processes that account for the majority of
work performed in the ED. Patients could be clustered according to the pathways
they followed.
A second attempt was made to confirm past groupings. These process-based
clusters were associated with demographic variables and details about the ED visit,
such as whether the patient was injured or not, time spent in ED and outcome.
The ED records were manipulated within SPSS (2001) and SOM investigations
were done using Viscovery SOMine software (1999). The results of the above three
investigations are presented in the next section.
4 Results
In trying to emulate previous studies, no satisfactory clustering could be achieved,
regardless of the variable(s) used in clustering, whether urgency, diagnosis, presenting
problem, outcome or other data. Clusters contained a full demographic sweep of
patients without any definitive variables. There were isolated pockets of correlation
but these were insufficient to satisfy casemix requirements.
When a process-mining approach was tried, 41 clusters of procedures were found.
21 of these clusters accounted for 96.6% of presentations, while just 14 clusters
accounted for over 90% of ED presentations. This means that 14 “primary pathways”
could be identified that 90% of patients follow. In addition to this remarkable result,
18 procedures could be omitted from future analysis because they did not contribute
to the primary clusters. New maps were generated after removing the 18 procedures
and 27 clusters identified. Once again just 14 clusters incorporated key pathways for
some 90% of ED visits (Table 3).
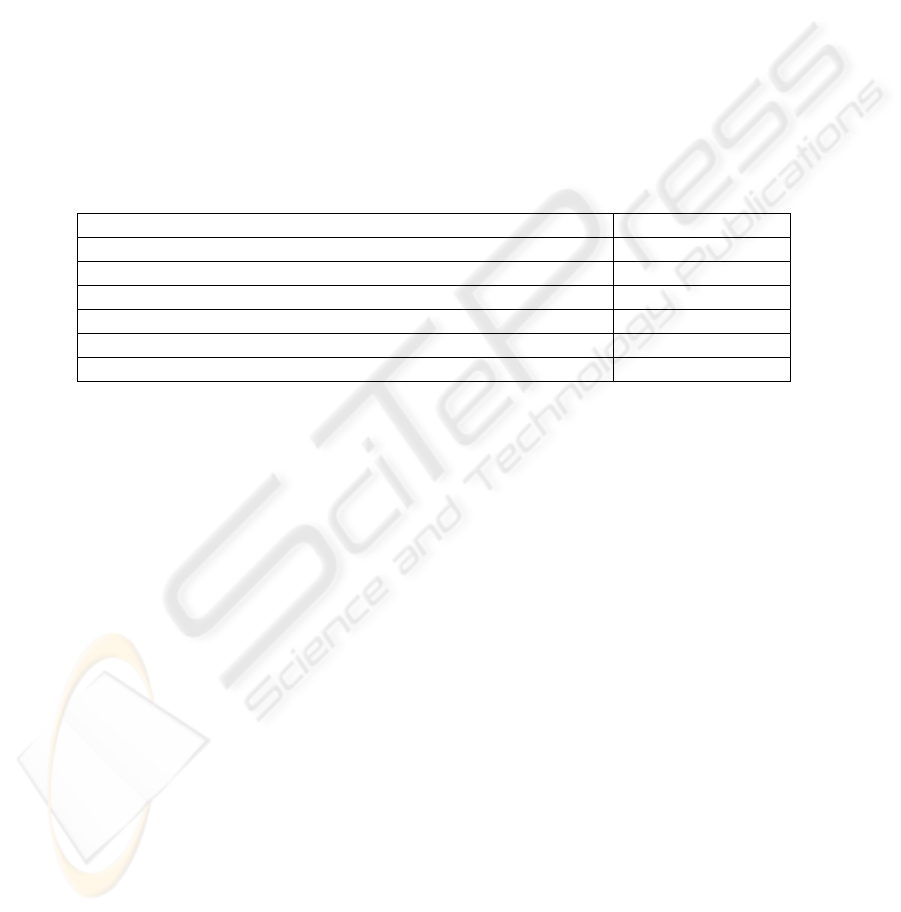
Table 2: Overview of ED data used in defining core ED activities. Note that 10
procedures account for the majority of presentations in patients who
underwent only 1 procedure.
Description Count of records
Two or more procedures (including duplicated procedures) 44600
One or no procedures (*) 12211
Top 10 procedures in records with 1 procedure (99% of *) (11537)
Top 30 procedures in records with 1 procedure (99.9% of *) (12199)
Missing or corrupted records 95
Total number of records 56906
65
Demographic and ED visit details were overlaid on the process-based clusters to
check whether past casemix groupings correlated to the process-based groups. There
was almost no correlation between number and type of procedures (which act as
proxies for resource use) and factors such as age, sex, injury, urgency, time in ED and
outcome. The impact of these results on ED processes are discussed in the next
section.
5 Discussion
The failure to find discrete groupings of ED patients based on traditional casemix
approaches highlights the reason behind the inability of these groupings to account for
even 60% of ED patient costs. Although it may seem logical to link patients
according to diagnosis, it is likely that the treatments (and resource use) vary
considerably, even within diagnosis groups.
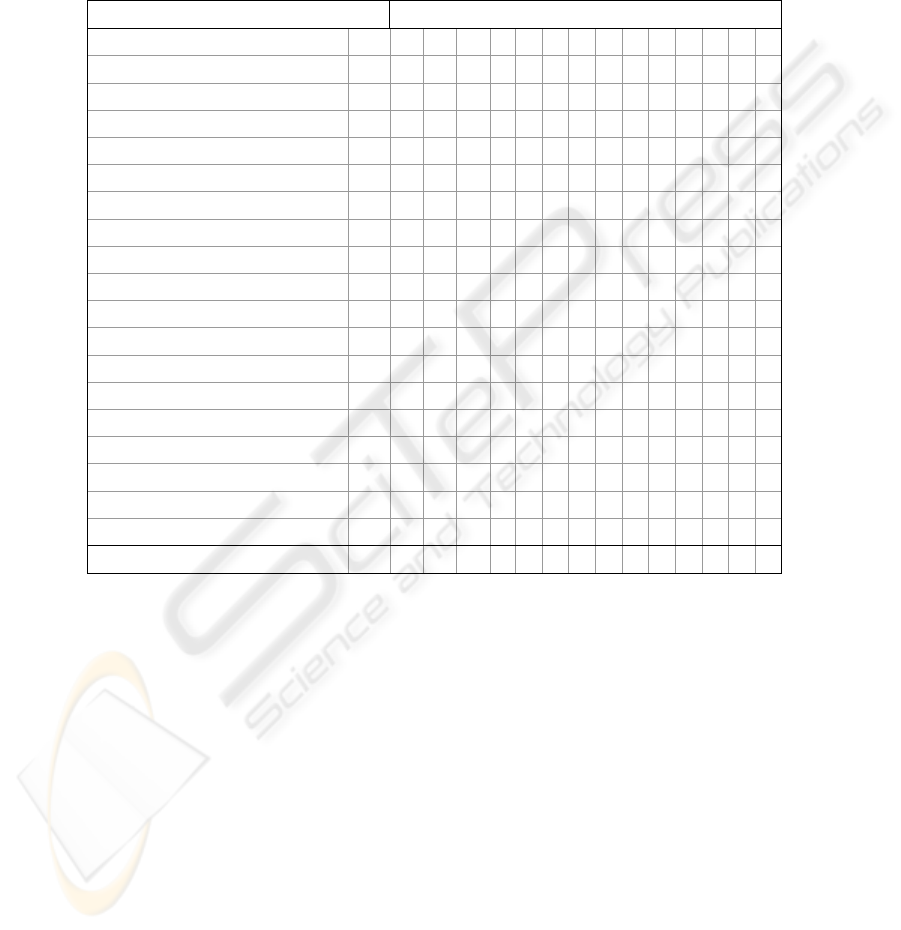
Table 3: Primary clusters for patients who have 2 or more procedures
Clusters for patients with 2 or more procedures
Description Abrv. A B C D E F G H I J K L M N
Observation o X X + x x + + X x + + + +
Venipuncture vb
x
X +
x
X+
x
X
x
Drug (Oral/Sublingual/Optical/Rectal) drug + X
x
x
+ +
x
+ +
x
+ + + +
X-ray xray + + + +
x
+ + + X +
Peripheral IV Catheter iv + X
x
x
X
x
+
12 Lead ECG ecg + + X +
x
Infusion of IV fluid (not blood) inf X +
Full ward test of urine fwt X
CT Scan ct X
Dressing drs X
x
ECG Monitoring ecgm X
Head Injury Observation hio X
IV Drug Infusion ivi X
Nebulised Medication neb X
Plaster of Paris pop X
Random Blood Glucose rbg X
Suture, Steristrip, Glue sut X
Ultrasound uls X
Patients with 2 or more procedures (%) 20.3 14.8 10.6 8.1 4.6 3.7 5.8 3.1 4.4 4.7 2.0 2.6 4.2 2.5
Key:
X: Over 80% Patients in this cluster underwent this procedure
x: Between 60% and 80% of patients in this cluster underwent this procedure
+: Between 40% and 60% of patients in this cluster underwent this procedure
66

While there is not space to discuss the process-based clustering results at length, a
few points of interest may be indicated. Common sense would dictate that X-rays and
Plaster of Paris would frequently be paired as activities of a single process, and this is
seen in Cluster K. Similarly, it would be expected that ECG and ECG monitoring
occur as part of the same process, as seen in Cluster G. The principal procedures
(indicated by “X” in Table 3) of the 14 main clusters do not overlap with the most
common procedures in patients that had only a single procedure (with the exception
of “Observation” and “Drug administration” procedures, which are rather generic), so
the clusters reflect complete processes, rather than extensions of individual
procedures.
Differentiation between clusters may seem trivial if only principal procedures
within each cluster are compared, but it must be remembered that the secondary
procedures within each cluster (indicated by “x” and “+” in Table 3) provide insight
about underlying patterns and similarities between patients in that grouping. It is
these patterns that supply the necessary information about the overlap of process and
clinical activities. For example, in Cluster K, patients often receive some form of
drug (clinical treatment), are transported to the X-ray department (an activity
supported by typical process views), are examined and have bones set and Plaster of
Paris applied (clinical treatment).
The results have shown that discrete groups of ED patients can be identified that
satisfy the casemix requirements of “a reasonable number of clinically meaningful
resource homogenous groups based on data that is simple and easy to collect” (Bond
et al. 1996):
– The 14 clusters compare well in number to the dozen or so used in previous works,
yet account for over 70% of visits to the ED. Over 90% of all visits to the ED can
be accounted for by supplementing these 14 clusters with data about the 10 most
frequently used single procedures.
– The clusters are certainly clinically meaningful, since they reflect an “as is”
analysis of activity in the ED.
– The clusters are resource homogenous in terms of number and types of procedures.
Variations within procedures themselves may contribute to some variance, but the
clusters allow this variation to be analysed in a meaningful way.
– Since the data is currently being routinely collected, no extra load is placed on staff
to collect data, and the variables are defined in a standard and clear manner. The
data is formatted to standards that will soon be national, so collation and
comparison of datasets should be simple.
There is little potential for manipulating casemix for profit, or gaming. Since the
clusters reflect current activities, any sudden change in activities could be detected by
referring to earlier data.
The casemix requirements above overlap with requirements for definition of
business processes, and there are a number of process related implications. In
general, it may be considered that each patient visit to an ED triggers a sequence of
activities aimed at improving their well-being while meeting multiple other objectives
such as economic sustainability, disaster contingency and minimal stress for staff.
These activities have a business process component that relates to patient
administration and workflow, and a clinical component that is complex and variable.
Although the primary pathways identified by the process mining approach in this
paper are not processes as defined by Davenport (1990), in that there are no
67

predecessor/successor relationships, they do provide groups of procedures whose
individual and cumulative inputs, outputs and costs can be evaluated.
While the immediate benefits to the ED of this work (in terms of real process
modifications) have yet to be realised, extensions to the work exist. Clinical business
processes for this ED have been modelled in detail using ARIS (Djordan and Churilov
2003), and there is a large library of “clinical pathways” that represent best practice in
treatment of numerous diagnoses (Lin et al. 2001). The key pathways identified in
this work provide a link between many business and clinical process. It is likely that
a “matrixed” view of the ED may be modelled that combines these process and
clinical views.
Patient flows in this ED have been modeled using discrete event simulation (Liew
et al. 2003). The logical groupings of patients provided in this work will be used to
enhance the “granularity” of this simulation model to improve understanding of
patient flows and the impact of emergencies on resources.
6 Conclusion
EDs strive for balance between efficiency (more patients may be treated), and
effectiveness (quality of care and rapid patient recovery). Previous attempts to
identify urgency-related casemix groups that allow for measurement of efficiency and
effectiveness in the ED have not been successful. The complexity of clinical
treatment and the patient well-being imperative make pure process driven views of
ED clinical operations impossible. This paper explained the melding of process and
casemix approaches to determine a small number of “primary pathways” – core sets
of activities for the ED.
It should be remembered that the intention of ED facilities is to provide timely
care, given the urgency of the case, and to retain quality of care, even when the ED is
operating at capacity. Any modifications to EDs must be examined in light of these
clinical prerogatives. Unlike casemix approaches that artificially group patients based
on cost and clinical observations, the data driven approach presented in this paper
provides insight into actual core procedures, so provides a low-risk avenue for re-
engineering of ED processes.
References
Viscovery SOMine Standard Edition 3.0 (1999) Wien Eudaptics Software Gmbh
SPSS for Windows Release. 11.5.1 (2001) Chicago SPSS Inc.
Abston K C (1999) PhD Using the electronic medical record to predict the pharmacological
management of acute myocardial infarction Salt lake City University of Utah
Acute Health Division (2001) Emergency Demand Management: A new approach Melbourne,
Victorian Government Department of Human Resources: Feb
Australian Department of Health and Aging (2003) Annual Report 2002-'03
http://www.health.gov.au/index.htm (Australian Department of Health and Aging)
Accessed: 5 Dec 2003
68

Australian Healthcare Association (1999) "Special Issue on the George Palmer Symposium"
Australian Health Review 22 (2)
Bond M, Baggoley C and Erwich-Nijhout M (1996) Costings in the Emergency Departments A
Report for the Commonwealth Department of Health and Family Services, South Australia
Brossette S E, Sprague A P, Jones W T and Moser S A (2000) "A data mining system for
infection control surveillance" Methods Inf. Med. 39 (4-5): 303-310
Cameron J, Baraff L and Sekhon R (1990) "Case-mix classification for emergency
departments" Medical care 28: 146-158
Chae Y M, Kim H S, Tark K C, Park H J and Ho S H (2003) "Analysis of healthcare quality
indicators using data mining and decision support system" Expert Syst. Appl. 24 (2): 167-
172
Cullen P (2001) Ph.D Feature selection methods for intelligent systems classifiers in healthcare
Chicago, Loyola University of Chicago
Davenport T H and Short J E (1990) "The new industrial engineering: information technology
and business process redesign" Sloan Management Review 31 (4): 11-27
Department Technology Management (2003) Process Mining http://tmitwww.tm.tue.nl
/research/process_mining.shtm (Technische Universiteit Eindhoven) Accessed: 8 Dec 2003
Djordan V and Churilov L (2003) "Business interactions in an acute emergecy department in
Australia: A clinical process modeling perspective" The 6th Pacific Asia Conference on
Information Systems (PACIS 2002) Tokyo, The Japan Society for Management Information
Duckett S J (1998) "Casemix funding for acute hospital inpatient services in Australia" The
Medical Journal of Austalia 168: S17-21
Funding & Financial Policy Branch (2002) Casemix Funding in Victoria
http://casemix.health.vic.gov.au/index.htm (Victorian Department of Human Services)
Accessed: 4 Dec 2003
Hanson R M Ed. (1998) Casemix: Moving forward The Medical Journal of Australia Sydney,
The Australian Medical Association
Isken M W and Rajagopalan B (2002) "Data mining to support simulation modeling of patient
flow in hospitals" J. Med. Syst. 26 (2): 179-197
Jelinek G A (1995) A Casemix information system for Australian Hospital Emergency
departments A Report to the Commissioner of Health, Western Australia
Jun J B, Jacobson S H and Swisher J R (1999) "Application of discrete-event simulation in
health care clinics: A survey" Journal of the Operational Research Society 50 (2): 109-123
Kennedy R, Lee Y, Van Roy B, Reed C and Lippmann R (1998) Solving data mining problems
through pattern recognition, Prentice Hall
Kohonen T (1995) Self-organizing maps Berlin ; New York, Springer
Lane D C, Monefeldt C and Rosenhead J (2000) "Looking in the wrong place for healthcare
improvements: A system dynamics study of an accident and emergency department" Journal
of the Operational Research Society 51
: 518-531
Lee I N, Liao S C and Embrechts M J (2002) "Important variable selection techniques with
multiple solutions for medical information applications" Med. Inform. Internet Med. 27 (4):
253-266
Liew S K, Churilov L and Brailsford S (2003) "Treating ailing emergency departments with
simulation: an integrated perspective" International Conference on Health Sciences
Simulation Orlando, Florida, The Society for Modeling and Simulation International
Lin F R, Chou S C, Pan S M and Chen Y M (2001) "Mining time dependency patterns in
clinical pathways" Int. J. Med. Inform. 62 (1): 11-25
List B, Schieder J, Min Tjoa and Quirchmayr G (2001). "Multidimensional business process
analysis with the business warehouse" Knowledge discovery for business information
systems Abramowicz W and Zurada J Eds. Boston, Kluwer Academic Publishers: xvii, 431
McAlister S (2003) Work on the National Minimum Data Set for Non- Admitted Patient
Emergency Department care (NAPED NMDS) Personal communication to Ceglowski A
69

Preater J (2002) "A Bibliography of Queues in Health and Medicine" Health Care Management
Science
Riano D and Prado S (2000). "A data mining alternative to model hospital operations" Medical
Data Analysis. Berlin, Springer-Verlag. 1933: 293-299
Richards G, Rayward-Smith V J, Sonksen P H, Carey S and Weng C (2001) "Data mining for
indicators of early mortality in a database of clinical records" Artif. Intell. Med. 22 (3): 215-
231
Victorian Department of Human Services (2002a) Designing Care http://
designingcare.health.vic.gov.au/ (Victorian Department of Human Services) Accessed: 6
May 2003
Victorian Department of Human Services (2002b) Summary of findings from project annual
reports: Hospital demand management strategy 2001–2002 Melbourne, Metropolitan
Health & Aged Care Services Division: Nov
Williams G, Baxter R, Kelman C, Rainsford C, He H X, Gu L F, Vickers D and Hawkins S
(2002). "Estimating episodes of care using linked medical claims data" Al 2002: Advances
in Artificial Intelligence. Berlin, Springer-Verlag. 2557: 660-671
70
