
Human-centred Design of Self-management Health Systems with and for
Older Adults: Challenges and Practical Guidelines
Ine D’Haeseleer
a
, Karsten Gielis
b
and Vero Vanden Abeele
c
KU Leuven, e-Media Research Lab, Belgium
Keywords:
Human-centred Design Process, Older Adults, Challenges, Health, Self-management, Recommendations.
Abstract:
Human-centred design approaches that involve older adults are becoming more and more commonplace in the
development of digital systems to support self-management of health and well-being, ultimately contributing
to ageing in place. In order to understand and design effective solutions, it is important to involve older
adults from the beginning and throughout the iterative development process. However, conducting studies
with this target population presents challenges and therefore requires specific adaptations. In this study, we
reflect on the different human-centred methods, e.g., focus group discussions, interviews, and user-tests, that
were conducted with older adults. In total, 81 participants (aged 65 to 97) were involved in a four-year
human-centred design process. On the basis of a thematic analysis, we reflect on the different methodological
intricacies encountered and identify four themes: ‘a life course marked by grand experiences’, ‘a discomfort
with unknown digital technologies’, ‘impact of age-related impairments’, and ‘relatedness as core to research
participation’. Finally, insights and practical guidelines are formulated to help future researchers undertake
more effective and useful human-centred study designs with older adults.
1 INTRODUCTION
Increasingly, older adults are involved in the design
and development of digital systems to manage their
health and well-being (Lindsay et al., 2012; Xie et al.,
2012; Davidson and Jensen, 2013b; Mehrotra et al.,
2016; Volkmann et al., 2016; Sengpiel et al., 2019;
Cornet et al., 2020; Czaja et al., 2019). A scoping
review
1
of studies with older adults in the ACM Dig-
ital Library (Association for Computing Machinery,
2021) revealed 1288 studies, a number that has been
increasing exponentially during the last decade. In its
slipstream, researchers have directed their attention
to the intricacies of involving older adults in the de-
sign of interactive technologies, specifically to man-
age their health (Lindsay et al., 2012; Chaudhry et al.,
2016; Sengpiel et al., 2019; Cornet et al., 2020). Most
recently, Sengpiel et al. (2019) introduced HCD+ as
‘human-centred design for aging’, a specific approach
to address how HCD-methods need to be adapted in
a
https://orcid.org/0000-0001-5455-3581
b
https://orcid.org/0000-0002-7660-8544
c
https://orcid.org/0000-0002-3031-9579
1
Query: ((“user-centred design”) OR (“participatory
design”) OR (“human-centred design”)) AND ((“older
adults”) OR (“elderly”)) AND (“health”))
order to involve older adults as experts of their own
age group. Hence, the body of studies on how to adapt
an HCD process to older adults is continually grow-
ing.
Nevertheless, to date, recommendations and
guidelines on including older adults in the design of
health systems are still few and fragmented. Most of-
ten, research studies focus on the outcomes of HCD
methods, e.g., the majority of studies focus first and
foremost on the product, i.e., the designed system
or service, with the lessons learned on working with
older adults as an afterthought to be discussed (Xie
et al., 2012; Davidson and Jensen, 2013b; Mehrotra
et al., 2016; Volkmann et al., 2016). Notwithstanding
the value of such studies, they may be limited in their
reflection on the HCD methodology. Moreover, most
studies are not specifically geared towards interactive
technologies supporting self-management of health,
but towards ICT in general.
Self-Management Health Systems (SMHS) have
gained increasing interest from researchers; in partic-
ular to empower older users and contribute ageing-
in-place (Sintonen and Immonen, 2013; Heart and
Kalderon, 2013; Peek et al., 2016; Kononova et al.,
2019; D’Haeseleer et al., 2019). Yet, SMHS present
specific challenges as they may relate to sensitive is-
90
D’Haeseleer, I., Gielis, K. and Abeele, V.
Human-centred Design of Self-management Health Systems with and for Older Adults: Challenges and Practical Guidelines.
DOI: 10.5220/0010529100900102
In Proceedings of the 7th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2021), pages 90-102
ISBN: 978-989-758-506-7
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

sues, and bring a limited biomedical focus on age-
related decline (Vines et al., 2015; Nunes et al., 2015).
The aim of this study is to contribute to the grow-
ing body of HCD+ in health, by presenting a thematic
analysis of methodological observations and reflec-
tions on an HCD process of an SMHS, that encom-
passed all phases (inspiration, ideation, implementa-
tion, and evaluation), involving 81 older adults with
ages ranging from 65 to 97 (median=83) over a pe-
riod of four years. In this paper, we present this
analysis and provide lessons learned, transformed into
practical guidelines, to help future researchers set up
more effective and useful study designs for conduct-
ing HCD processes with older adults.
2 BACKGROUND AND RELATED
WORK
There is an increasing interest in executing HCD pro-
cesses for and with older adults and health systems
in particular. In the paragraphs below, we first dis-
cuss the different understandings of human-centered
design. Next we present studies on that involved older
adults in the design process. We end this section with
existing guidelines related to older adults, HCD, and
health.
2.1 Involving End-users in the Design
Process
Different methodological approaches have been pro-
moted to involve older adults in the design and evalu-
ation of interactive, digital systems, labelled among
others as User-Centred Design (UCD), Human-
Centred Design (HCD) or Participatory Design (PD).
The term UCD was promoted already in Gould and
Lewis’ (1985) seminal paper on ‘Designing for Us-
ability’. In this work, the authors present three pil-
lars for any UCD process: involving users early, us-
ing empirical measurement, and conducting an itera-
tive design. In 1999, the ISO standard on HCD was
launched, embodying the aforementioned pillars of a
UCD process, and further detailing how to involve
end-users in the different phases. Moreover, con-
ceptually the ISO-standard also emphasises the hu-
man rather than the user, thus “putting people before
machines” (Cooley, 1996; Brown et al., 2008; ISO,
2019).
In parallel to UCD and HCD processes, also PD
grew in importance, originating from the premise that
those who ultimately have to use or are affected by
the implementation of technology should have a criti-
cal role in their design (Muller and Kuhn, 1993). PD
is, above all, an ideology that aims for empowerment
of end-users, and considers any design process as a
dialectic process between the different stakeholders
(end-user, designer, project owner, etc.) that serves
to unearth conflicting values. Co-design is also fre-
quently used to point to practices where end-users
are invited to collaboratively design and prototype
(Sanders, 2002). This term is often used interchange-
ably with PD, although with the term co-design, the
emphasis shifts to the actual methods used and less
the ideology.
Despite the different origins and delineations, re-
searchers often hold an idiosyncratic interpretation of
the methodological approaches, and apply them in a
lenient manner. As a consequence, in practice, the
boundaries between UCD, HCD, PD, and co-design
are fuzzy, yet they are united in the central premise
that stakeholders, i.e., here older adults, need to be
involved in the design.
2.2 Involving Older Adults in the
Design Process
Involving older adults is a recurrent topic in Human-
Computer Interaction (HCI), e.g., (Czaja et al., 2019;
Lindsay et al., 2012; Xie et al., 2012; Davidson
and Jensen, 2013b; Sengpiel et al., 2019; Cor-
net et al., 2020). Most recently, Sengpiel et al.
(2019) introduced HCD+, or ‘human-centered de-
sign for ageing’, a new approach that specifically
“considers older adults’ requirements and abilities
throughout the development process, adapting estab-
lished HCD-methods to accommodate the participa-
tion of older adults as experts for their own age
group”. The authors applied their HCD+ approach
to a project that centred on “Historytelling”, including
183 older adults (mean age=66.6, SD=7.5) within dif-
ferent HCD+ activities, i.e., focus group discussions,
workshops, interviews, and evaluations. From this,
the following guidelines were derived: ‘engage with
group leaders’, ‘emphasise reciprocity when recruit-
ing’, ‘plan for social engagement’, ‘overestimate the
scheduled time’, ‘accommodate participants’ wishes’,
‘establish (low-technology) fall-backs’, and ‘use ab-
stract descriptions of technology’ (Sengpiel et al.,
2019).
Notwithstanding, Sengpiel and colleagues were
the first to coin the term HCD+ (Volkmann et al.,
2016; Sengpiel et al., 2019), they are not the first to
propose frameworks or guidelines on how to include
older adults in the design process. Already in 2012,
Lindsay et al. (2012) investigated how to engage older
adults in PD processes. They identified in particular
Human-centred Design of Self-management Health Systems with and for Older Adults: Challenges and Practical Guidelines
91

four challenges: ‘maintaining focus and structure in
meetings’, ‘representing and acting on issues’, ‘envi-
sioning intangible concepts’, and ‘designing for non-
tasks’ (Lindsay et al., 2012). To address these chal-
lenges they suggested a new approach (termed OA-
SIS) that highlights the importance of ‘stakeholder
identification and recruitment’, ‘the usage of video
prompts’ to illustrate usage scenarios, followed by
‘exploratory meetings’ to explore the problem do-
main, and finally ‘low-fidelity prototyping sessions’,
here to be understood as co-design sessions to gener-
ate further requirements.
Two recent systematic literature reviews (Duque
et al., 2019; Amaro et al., 2020) further corrobo-
rate the growing number of studies on involving older
adults in the design process; one on user-centred and
participatory design with older adults (Duque et al.,
2019), and one on engaging older adults in participa-
tory and intergenerational design teams (Amaro et al.,
2020). Their findings echo the same considerations
stated above, highlighting the need for a better un-
derstanding and proper integration of older adults in
UCD and PD in general. Additionally, in their future
work, Duque et al. (2019) articulate the need for more
research in the domain of health self-medication.
2.3 Human-centred Design of Health
Technology
Given the prevalence of studies on older adults and
health technology, myriad studies have also applied
HCD processes in the domain of self-management of
health and well-being by older adults. In this section,
we limit ourselves to recent studies of SMHS that pro-
vide a detailed account of the process and method-
ological challenges, followed by recommendations.
The aforementioned OASIS process was also ap-
plied in the context of mobile health applications with
18 older adults (Davidson and Jensen, 2013b). Based
on their findings, researchers suggested additional
considerations. In particular, ‘short design sessions’,
‘allow for socialising among participants’, ‘encour-
age active participation’ by calling upon specific peo-
ple, and ‘finding a balance between input from re-
searchers and participants’ were added during the dif-
ferent workshops.
Chaudhry et al. (2016) conducted a UCD with
older adults and caregivers (mean age=66, SD=9.2)
to design and evaluate a tablet-application to promote
successful ageing called seniorHealth. Focus group
discussions, interviews, and pilot studies were con-
ducted. Both methodological and ethical challenges
encountered during the design and deployment of the
application, e.g., ‘difficulties in forming a design’,
‘high learning curve’ for using technology, and the
‘need for social support’.
Martin-Hammond et al. (2018) conducted a PD
involving 18 older adults (mean age=76, SD=8.25)
including seven phases: background survey, app cri-
tique, team presentation, current health info man-
agement practices, co-design, another team presenta-
tion, and a Q&A. Based on their findings, challenges
were encountered and strategies were shared: ‘enlist-
ing allies in recruitment’, ‘incorporating a design cri-
tique’, ‘use of common vocabularies’, ‘accommodat-
ing schedules and adapting the protocol’, and ‘partic-
ipation in creating tangible artefacts’.
Harrington et al. (2018) used co-design sessions
to design fitness apps with 25 older adults (mean
age=72.1, SD=4.25). These authors highlight in par-
ticular the differences between those familiar with
and those new to the technology, resulting in a tension
between the need to familiarise a participant with a
technology and the importance of not biasing a partic-
ipant through technology exposure. The authors also
found that continued use of the assigned application
led to more robust and detailed feedback in design
sessions, suggesting that long-term prior use of sam-
ple technologies is an important prerequisite to ideat-
ing useful features for new health technology.
Finally, a recent study on mobile health appli-
cations for older adults with heart failure indicated
the importance of tailoring the UCD process to older
adults (Cornet et al., 2020). Based on the authors’ ex-
periences, 12 practical challenges were enumerated,
including, but not limited to, ‘managing UCD logis-
tics’, ‘determining timing and level of stakeholder
involvement’, ‘overcoming designers’ assumptions’,
and ‘adapting methods to end-users’. In addition, au-
thors provided suggestions on how to overcome these
challenges.
Table 1 summarises the different challenges and
recommendations provided by the aforementioned
studies. While informative, certain guidelines seem
to conflict, e.g., overestimating time (Duh et al., 2016;
Sengpiel et al., 2019) versus to keeping sessions short
(Davidson and Jensen, 2013a), or providing tangi-
ble examples (Lindsay et al., 2012; Martin-Hammond
et al., 2018) versus using abstract descriptions of tech-
nology (Sengpiel et al., 2019). Moreover, most guide-
lines were not formulated in the context of SMHS.
Finally, not all studies report on the age of the partic-
ipants that were included, e.g., (Lindsay et al., 2012;
Cornet et al., 2020). Others reported findings where
mean ages typically varied from 65 to 75 years old
(Chaudhry et al., 2016; Harrington et al., 2018; Seng-
piel et al., 2019). Therefore, in this research study we
set out to perform a rigorous analysis of methodolog-
ICT4AWE 2021 - 7th International Conference on Information and Communication Technologies for Ageing Well and e-Health
92

Table 1: A chronological overview of the studies encountered in the related work section, summarising the research study
methodology along with the challenges and guidelines.
Research Study Participants Study Design Challenges & Guidelines
Engaging Older People using
Participatory Design (Lindsay
et al., 2012)
[not specified] PD OASIS approach: identification
and recruitment of stakeholders,
video prompt creation, exploratory
meetings, low fidelity prototyping
maintaining focus and structure in meetings (challenge), represent-
ing and acting on issues (challenge), envisioning intangible concepts
(challenge), designing for non-tasks (challenge), stakeholder identifica-
tion and recruitment (guideline), the usage of video prompts (guide-
line), exploratory meetings (guideline), low-fidelity prototyping ses-
sions (guideline)
Participatory Design with
Older Adults: An Analysis
of Creativity in the Design of
Mobile Healthcare Applications
(Davidson and Jensen, 2013a)
18 older adults aged
65 to 88 years
OASIS approach: identification and
recruitment of stakeholders, video
prompt creation, exploratory meet-
ings, low fidelity prototyping
Keep design sessions short: trade-off between design quick and effi-
ciently, and lower novelty score (guideline), allow for informal socialis-
ing: informal socialising prior to design sessions (guideline), encourage
participation: call on specific people (guideline), balancing researcher
and participant input: allow questions but encourage to work together
(guideline)
Developing Health Technolo-
gies for Older Adults: Method-
ological and Ethical Considera-
tions (Chaudhry et al., 2016)
40 older adults
(M=66, SD=9.2)
UCD with focus group discussions,
interviews, and pilot studies
design: limited technology-based suggestions as participants were
novices (challenge), learning curve: difficulties on learning using tech-
nology (challenge), social support: interpersonal interactions between
participants (challenge), knowing the user: busy lives, distracted during
training, curious and eager to learn (challenge), sustainability: support
network after the study ended (ethical reflection)
Designing Health and Fitness
Apps with Older Adults: Exam-
ining the Value of Experience-
Based Co-Design (Harrington
et al., 2018)
25 older adults
aged 65 to 80 years
(M=72.1, SD=4.25)
co-design in seven sessions and
semi-longitudinal deployment
leverage pre-study experience (guideline), facilitate longer-term tech-
nology use (guideline), use varied materials and instruments for co-
creation engagement (guideline), establish a collaborative and com-
fortable approach to reviewing brainstormed ideas (guideline), stratify
group participants by experience levels (guideline)
Engaging Older Adults in
the Participatory Design of
Intelligent Health Search Tools
(Martin-Hammond et al., 2018)
18 older adults
aged 61 to 93 years
(M=76, SD=8.25)
PD with background surveys, app
critique, team presentation, co-
design, and Q&A
enlisting allies in recruitment (guideline), incorporating a design cri-
tique (guideline), use of common vocabularies (challenge), accommo-
dating schedules and adapting the protocol (challenge), participation in
creating tangible artifacts (challenge)
Considering older adults
throughout the development
process – The HCD+ approach
(Sengpiel et al., 2019)
183 older adults aged
46 to 93 (M=66.6,
SD=7.5)
HCD+ with focus group work-
shops, interviews, evaluations
engage with group leaders (guideline), emphasise reciprocity when re-
cruiting (guideline), plan for social engagement (guideline), overesti-
mate the scheduled time (guideline), accommodate participants’ wishes
(guideline), establish (low-technology) fall-backs (guideline), use ab-
stract descriptions of technology (guideline)
Untold Stories in User-Centred
Design of Mobile Health: Prac-
tical Challenges and Strategies
Learned From the Design and
Evaluation of an App for Older
Adults With Heart Failure (Cor-
net et al., 2020)
older adults aged
over 65 (see study
design for number
of participants),
along with clinicians
and external UCD
experts
UCD including patient interviews
(n=24), patient advisory meetings
(n=2), clinician advisory board
(n=0), individual interviews with
2 cardiologists (n=0), observation
of clinical encounters with a pa-
tient in the device clinic, usability
evaluation (n=4), usability evalua-
tion (n=12), and heuristic evalua-
tion (n=0)
Deciding on number of iterations (challenge), managing UCD logistics
(challenge), collaborating as multidisciplinary team (challenge), deter-
mining timing and level of stakeholder involvement (challenge), choos-
ing stakeholder representatives (challenge), fostering interactions be-
tween stakeholders and designers (challenge), overcoming designers’
assumptions (challenge), managing project scope and complexity (chal-
lenge), maintaining the innovation equilibrium (challenge), conduction
laboratory or in-the-wild usability sessions (challenge), adapting meth-
ods to end users (challenge), deciding on the number of concurrent eval-
uation methods (challenge)
Human-centred Design of Self-management Health Systems with and for Older Adults: Challenges and Practical Guidelines
93

ical observations to yield recommendations for con-
ducting an HCD for SMHS involving older adults,
equally including the oldest old (von Humboldt and
Leal, 2015).
3 METHOD
In this study, a complete HCD process, i.e., inspira-
tion or analysis of context of use and requirements,
ideation of design & prototypes, implementation, and
evaluation (Brown et al., 2008), was conducted in an
iterative manner over the course of four years, from
2016 to 2020.
3.1 Participants
Participants were healthy older adults, being at least
65 years old, and were still able to live independently
at home or in a service flat. In total, 81 participants
(30 identified as male, 51 identified as female) with
ages ranging from 65 to 97 (median=83), and six
moderators and researchers attended at least one of
the different HCD activities.
Participants were recruited in Belgium from 2016
to 2020 via local organisations, i.e., InnovAge (In-
novAge, 2016), service centres (Zorg Leuven, 2020),
and Triamant (Triamant, 2020). In addition, we em-
ployed a snowball technique where participants also
brought us in contact with family, friends, or neigh-
bours who also wanted to participate.
All studies were approved by either the Medical
Ethics Committee (CTC-S60250) or Social and Soci-
etal Ethics Committee (G-2019121931).
3.2 Study Design
Figure 1 gives an overview of the different HCD
phases and the specific activities that were carried out.
3.2.1 Inspiration
During the inspiration phase, the context of use and
requirements were analysed by means of three focus
group discussions, semi-structured interviews, and
questionnaires.
Focus Group Discussion. Three focus group dis-
cussions were organised to discuss the problem do-
main. Focus group 1 and 2 discussed several topics
related to maintaining a healthy lifestyle, ICT use in
general, and use of SMHS (activity trackers, health
apps, etc). Focus group 3 discussed attitudes towards
a high-fidelity prototype in addition to the topics of
focus group 1 and 2.
Requirements Specification. Based on these prior
focus groups, requirements were enlisted during the
analysis specification. Additionally, a persona and a
context scenario were created to guide the design. A
persona or user model is a “composite user archetype
that represent distinct groupings of behaviours, at-
titudes, aptitudes, goals, and motivations that are
observed and identified during the research phase”
(Cooper et al., 2007).
Interviews. Upon the evaluation of the final appli-
cation, semi-structured interviews with participants
were organised in order to gain insights into their at-
titudes and usage of the system. Additionally, a struc-
tured interview was carried out to understand older
adults attitudes towards motivational designs embed-
ded in SMHS.
3.2.2 Ideation
During the ideation phase, low-fidelity prototypes,
high-fidelity prototypes, and an interactive prototype
were first designed and discussed with project part-
ners at the university and afterwards with the partici-
pants.
Low-Fidelity Prototypes. Low-fidelity prototypes
were used to represent concepts and functionalities
without risking to lose focus due to distracting visual
details. Figure 2 represents a sketch that was made
with pencil and paper.
High-Fidelity Prototypes. Next, a high-fidelity proto-
type was created to represent the look and feel of the
application using the digital design toolkit Sketch
2
.
An example can be found in figure 3.
Interactive Prototypes. The final prototype was made
interactive with Invision prototyping software
3
.
3.2.3 Implementation
An online web-application was developed using
CodeIgniter web framework
4
, a lightweight PHP
framework that supports a Model-View-Controller
approach. The user interfaces were built with the
Bootstrap framework
5
to provide a responsive layout
and ensure high-quality interaction through pre-built
components and JavaScript plugins. Data was stored
in a MySQL database
6
. Figure 4 illustrates the final
SMHS application.
2
Sketch B.V. (2021). The digital design toolkit.
3
Invision Inc. (2021). Digital product designplatform
4
EllisLab (2021). CodeIgniter web framework.
5
MIT. (2021). Bootstrap.
6
Oracle Corporation. (2021). Mysql.
ICT4AWE 2021 - 7th International Conference on Information and Communication Technologies for Ageing Well and e-Health
94
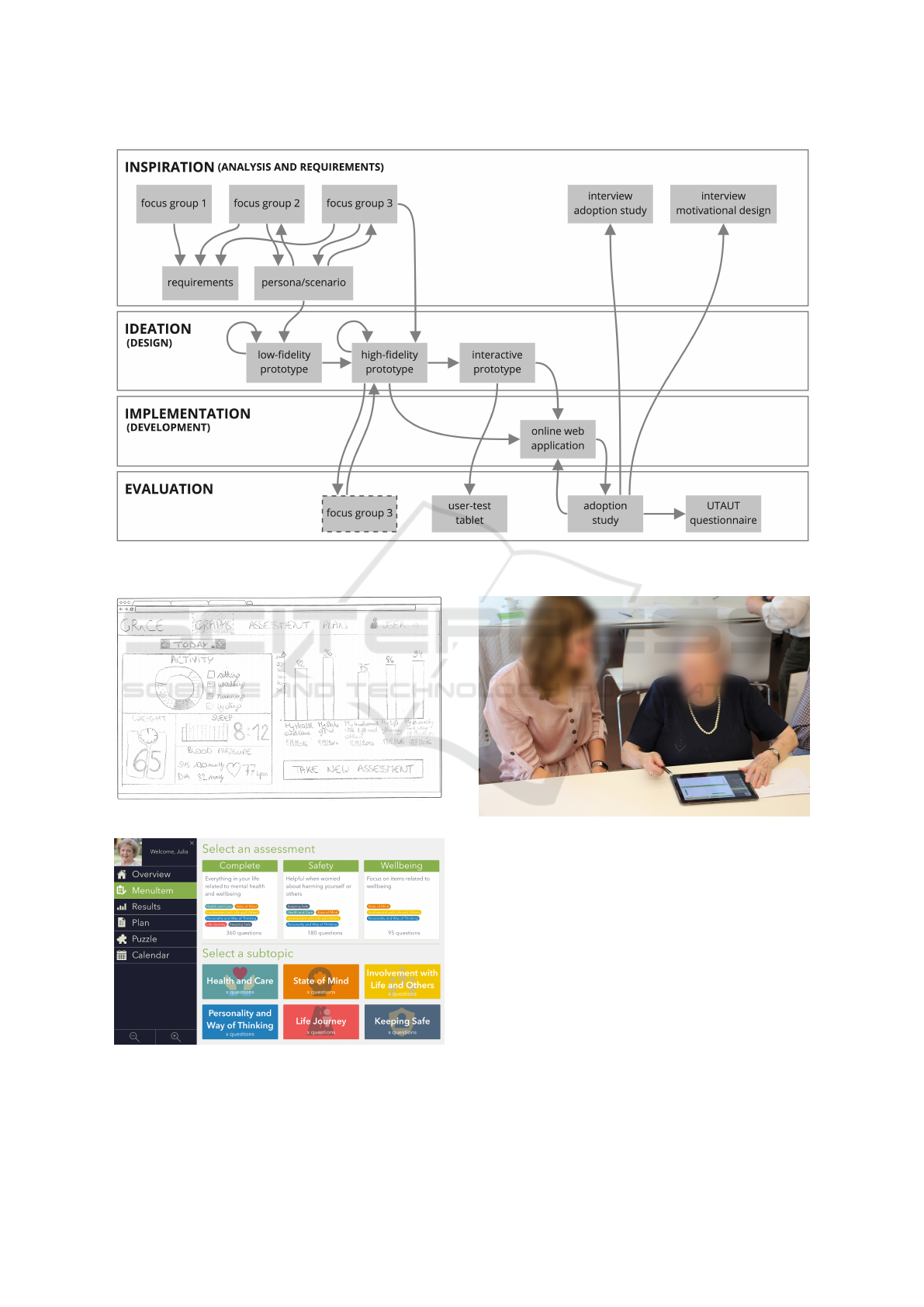
Figure 1: Overview of the different activities that were part of the human-centred design process of self-management health
systems with older adults.
Figure 2: Low-fidelity prototype.
Figure 3: High-fidelity prototype.
3.2.4 Evaluation
The evaluation phase consisted of formative usabil-
ity testing, summative usability testing, an adoption
Figure 4: Older adult using the online web-application in
tablet mode.
study, and the Unified Theory of Acceptance and Use
of Technologies (UTAUT) questionnaire to poll for
acceptance.
Formative Usability Test. Formative usability tests
were carried out using high-fidelity prototypes. For-
mative usability tests are rapid and more informal user
tests; users are given realistic tasks and asked to think
aloud while carrying them out. As designers gain in-
sights into the user’s mind while interacting with the
prototype (Cooper et al., 2007). These tests help to
give form to the design.
Adoption Study. Finally, an adoption study was set
up. Older adults used the application over the course
Human-centred Design of Self-management Health Systems with and for Older Adults: Challenges and Practical Guidelines
95

of two weeks, in order to investigate the users’ actual
interactive behaviours through user metrics.
Questionnaires. As the experience of this adoption
study shaped their attitudes towards SMHS, a UTAUT
questionnaire (De Witte and Van Daele, 2017) was
provided to all participants. This UTAUT ques-
tionnaire polled for behavioural intention to use the
SMHS and in particular investigated perceived ease-
of-use, usefulness, social influence, and facilitating
conditions.
3.3 Analysis
Noteworthy methodological findings were docu-
mented and discussed with the present researchers af-
ter every phase. In addition, methodological annota-
tions were made during the analysis of the transcripts
which included focus group discussions and inter-
views. Based on this information related to method-
ological observations, a thematic analysis (Clarke and
Braun, 2014) was conducted. First, all transcripts
were studied and nodes were created individually by
two researchers (ID and VVA) who went through the
entire HCD process. In the second iteration, ID de-
fined patterns and clustered nodes in initial themes
which were reviewed by VVA. Afterwards, both ID
and VVA discussed findings until an agreement was
reached and a thematic map created. Finally, these
themes and thematic map were revised by two other
researchers (JG and KG), who were also present dur-
ing at least one phase of the HCD process. This re-
sulted in the final set of themes.
4 RESULTS
Four themes were developed based on the thematic
analysis of methodological observations made during
the HCD process: ‘a life course marked by grand ex-
periences’, ‘a discomfort with unknown digital tech-
nologies’, ‘impact of age-related impairments’, and
‘relatedness as core to research participation’.
4.1 A Life Course Marked by Grand
Experiences
The first theme addresses the full lives lived by older
adults, characterised by joy, but equally misfortune
and grief. Shared naturally and unprompted, these
life experiences often carried significant emotional
weight and permeated all activities of the HCD pro-
cess. For example, during the introduction round of
the focus groups discussion, participants introduced
themselves by name and in one breath recounted per-
sonal details on dramatic events that occurred during
their lifetime.
“Eh... What could I say. Yes, I ended up here be-
cause my wife got a stroke, four years ago. Four
years, well let’s say it started in 2009, at Easter
[tells story of wife who fell ill, was hospitalized and
then moved into a nursing home]. Then they asked
me, why do you keep travelling between here and
your home to take care of your wife, there is a flat
available; and so, since 2013, I reside here.” – man
aged 90
Many participants had lost a loved one and shared
their sorrow. Others talked about the impact of a
chronic or life-threatening disease.
“This morning for example, I went to the hospital
for a consultation concerning my heart. I have to
go every year, and when the results are ready, my
GP will give them to me [...]” – woman aged 81
Naturally, researchers then paused to offer a mo-
ment of thought or consolation. As a consequence,
sufficient time was needed for welcoming and small
talk, e.g., an introductory round during a focus group
discussion was estimated to take up 15 minutes, but
took up 45 minutes to welcome all nine participants.
In addition, a particular recurring pressing topic
was their dire financial situation and related chal-
lenges, brought forward by a lack of a proper pension.
“They can say ‘you have to eat healthy’, but what
is healthy? Five pieces of fruit a day? You have to
buy five pieces of fruit in the store, that is expensive,
you know. We will not get there with our pension
alone...” – woman aged 79
“These are more serious problems, financial prob-
lems for example. Our pension is not sufficient.
[conversation on not having sufficient money]” –
woman aged 65
In some participants’ opinion, this was a much
more pressing problem in their life than the need for
an SMHS. This once again impacted the HCD pro-
cess, as it was difficult for some participants to relate
to a technological solution that was perceived as un-
affordable.
In sum, their tense personal histories, associated
with end of life, were introjected in the different activ-
ities of the HCD process and necessitated researchers
to adapt by making room for them.
4.2 A Discomfort with Unknown Digital
Technologies
The second theme addresses the anxieties and distrust
related to the struggle of older adults with current day
computing technologies that resurfaced in the discus-
sions and evaluations of SMHS.
ICT4AWE 2021 - 7th International Conference on Information and Communication Technologies for Ageing Well and e-Health
96

The majority of participants in our study had lit-
tle to no experience with current day ICT technol-
ogy such as tablets, activity trackers, smartphones,
etc. Often, this was voiced as a conscious rejection
of these technologies by older adults, propelled by a
distrust towards a society that enforces using technol-
ogy.
“I have chosen to spend no, or as little time as pos-
sible, on the computer, because otherwise people
will become a slave of it.” – woman aged 89
Especially during the focus group discussions, it
was noticeable that some participants showed more
interest in discussing the health topics addressed by
SMHS than the technology itself.
“But I thought this session was about other topics
too, not just about computers.” – man aged 88
“Yes, I thought so too, about nutrition and stuff,
what should improve [for a healthy lifestyle].” –
woman aged 65
“We have also other problems than [using] com-
puters, huh.” – man aged 88
If they had realised beforehand, they might not
have participated.
Similarly, some participants were uncomfortable
during the usability evaluations. Some of them had
not realised they would be interacting with an online
application on a tablet and became somewhat anxious
when they heard about having to test an online tool.
So I just have to do this [cf. take blood pressure
measurements] and then I actually do not have to
use [the tablet]? – woman aged 67
This lack of awareness was initially surprising to
researchers as the informed consent did clearly men-
tion the focus on technologies. However, in hindsight,
the lack in technological proficiency may equally ex-
plain a limited understanding of the different activities
that take place as part of an HCD process.
From these observations we understood that un-
derneath many usability issues was the complete lack
of a mental model on interactive (tablet-based) appli-
cations. The majority of participants did not under-
stand the concepts of touch interactions or logging
into a system. For the same reason, formative user
evaluations with paper prototypes or screenshots on
paper were hard to interpret for some participants.
The lack of mental models made it difficult to hypoth-
esise about future usage situations or different kinds
of features they would prefer.
Additionally, we encountered a language barrier
while testing the application. In Dutch, English terms
are common when using digital and networked ap-
plications, e.g., account, password, login. However,
these mongrel words were not part of participants’ vo-
cabulary and therefore not understood.
“an account has always been a [bank] account for
me. Don’t tell me anything else, because I knew an
account in banking, but not in here [cf. the appli-
cation]. And then login...” – man aged 88
The absolute lack of a mental model also sub-
verted our intention to apply a typical usability test-
ing protocol which recommends starting with a non-
obtrusive part, i.e., refraining from guiding users.
In contrast, in our HCD process, our participants
stressed the importance of receiving help.
“I always like them to show me exactly what I have
to do.” – woman aged 79
In sum, this theme foregrounds the need to adapt
HCD processes to compensate for a lack in experience
in using digital technologies to mitigate anxiety and
discomfort.
4.3 Impact of Age-related Impairments
This third theme addresses the diverse manifestations
of age-related decline, as an interplay of mentally,
physically, and emotional effects. During the differ-
ent research activities of the HCD process, we en-
countered participants who had a broad range of im-
pairments. These impairments included, but were not
limited to, impaired vision, reduced hearing, mobility
limitations, and ailments as a consequence of chronic
diseases. More often than not, participants had sev-
eral of these ailments. As a consequence, and perhaps
most characteristically, we found our HCD process
characterised by a slowness in actions. However, at
the same time this was giving way to tranquillity and
ample time for reflection.
The age-related impairments necessitated several
accommodations. With respect to mobility, it was
paramount that studies were organised nearby partic-
ipants. For one-on-one interviews or user-tests, the
researcher went to the participant’s home. For fo-
cus group discussions or user-tests with multiple par-
ticipants, a room in a local services centre was re-
served. It was ascertained that these rooms were on
the ground floor, thus easily accessible for everyone.
In addition, for participants who wanted to join a ses-
sion but had problems reaching the location, transport
was provided by one of the researchers who picked up
and dropped off participants at home.
In addition, to address visual impairments, we
found it essential to provide all documents, i.e., in-
formation, informed consents, feedback forms, and
increased font size. Furthermore, when testing pro-
totypes, designs were made sufficiently large to make
them apprehensible despite visual impairments. As
such, screenshots were printed in A3 format by de-
fault.
Human-centred Design of Self-management Health Systems with and for Older Adults: Challenges and Practical Guidelines
97

Finally, participants also indicated the importance
of talking loud and clear and in isolation. This was
particularly demanding in the moderation of focus
group discussions. The moderator had to ensure that
only one person was talking at the same time, but
equally that everyone talked loud enough or repeated
arguments when necessary.
Repeating and paraphrasing also helped partic-
ipants in processing information and mitigated the
times that attention fleeted.
“What is the actual question, because...” – man
aged 82
This slower processing of information and lesser
cognitive load manageable by the participants became
particularly prominent when conducting evaluations
by means of questionnaires; the shape of the question
and the length of the questionnaire presented difficul-
ties. In the scientific validated questionnaires that we
used, the same construct was often polled using multi-
ple items. This makes these questionnaires quite long
and, in turn, harder for the older participants to sus-
tain attention and complete them in a reliable man-
ner. In addition, negatively formulated questions were
found problematic, as we noted that participants often
marked the opposite answer of what they intended to
answer.
Therefore, it was paramount to orally present
questions and verify answers in a structured interview
format. It helped when participants could verbally
rate their experiences. This also allowed researchers
to rectify errors due to negative phrasing.
As a result, there was a need for a slower pace,
which also brought a sense of perspective. Partici-
pants were often relaxed about these limitations and
adopted a mindset that embraced a lifespan perspec-
tive on ageing.
“Glad we’re still alive.” – woman aged 84
Overall, this theme highlights that every activ-
ity in the HCD process took more time because of
the diverse age-related impairments. This also meant
that less ‘content’ could be dealt with. However, the
slower pace also brought along a relaxing atmosphere.
4.4 Relatedness as Core to Research
Participation
The final theme addresses the inherent social nature
of the HCD process, as a sense of relatedness was a
primordial motive for participants to take part in the
research. At the same time, this need for relatedness
risked obscuring the actual research activities that re-
searchers intended to carry out.
Since it was important to put participants at ease,
a familiar and pleasant setting was chosen to conduct
all research studies; activities took place at the par-
ticipant’s home or a local service centre familiar to
the participants. Moreover, we ensured everyone was
welcomed personally and were offered coffee and bis-
cuits to create a setting in which participants would
feel comfortable. However, the downside of this in-
formal atmosphere was that the actual research pur-
pose was less clear and perhaps less respected. Dur-
ing focus group discussions, participants often devi-
ated from the subject, and it was not always easy to
bring them back to focus on the matter at hand. Dur-
ing interviews, participants seemed unburdened by
the researchers’ agenda. This unawareness of the situ-
ation showed in some participants arriving 25 minutes
late and subsequently explaining their entire life story.
At the same time, many participants seemed
driven by an altruistic motive to participate in the
study .
“I am doing this for you, and to support your re-
search study.” – man aged 69
During the different contact moments, it was re-
markable that almost all older adults were volunteer-
ing or were a volunteer in the past. They all spend
quite a lot of their time helping other people. This
equally reflected in the research study, as participants
often indicated that they wanted to help out on our
research.
“Pleased I was able to help you; I am glad that it
is over, as you are always thinking about it, but I
will also miss being able to follow up everything
[cf. blood pressure, sleep, activities].” – woman
aged 66
Besides helping out as a volunteer, many older
adults equally had other hobbies or activities like
babysitting, going for a walk, or petanque. As a con-
sequence, many of them had quite the busy schedule.
“For 22 years now, I do not have a job, um, yes,
that’s it. I’ll say it in one sentence: It is wonderful
to be retired.” – man aged 82
Remarkably, many older adults endeavoured such
a busy schedule to fill their days.
Many activities they tend to do have a social as-
pect: joining a walking club, going on a group va-
cation, or being a volunteer. They also emphasised
the importance of social interactions. Therefore, we
suspect that some older adults participated in these
studies primarily to maintain social contact.
“contact, social contact is very important. It is for
that reason that I am also a volunteer. I’m out of
the house for about 70 to 80%, just to forget the
grief of my wife who passed away... and that helps
a lot. I even play petanque with my grandchildren
ICT4AWE 2021 - 7th International Conference on Information and Communication Technologies for Ageing Well and e-Health
98

three times a week. Those are all things that take
time.” – man aged 76
In sum, this last theme indicates that the different
research activities were primarily a means for relat-
ing to other participants or the researchers for many
participants. During the HCD process, there needed
to be sufficient room for small talk. As mentioned
before, participants found it important to share per-
sonal experiences, with conversations often deviating
to chitchat. As a consequence, formalities faded and
adhering to research protocols was challenging.
5 DISCUSSION
In this study, we investigated the intricacies of involv-
ing older adults in the design of SMHS. The different
themes confirm the need for adaptation of an HCD
process when designing health technologies for the
group of older adults including the oldest old.
The first theme identifies that older adults bring
a life marked by grand experiences with them that
interweave into the diverse HCD experiences. Sec-
ond, we unearthed a strained relationship with digital
technologies, often unknown and unwanted. Third,
we found that different age-related impairments man-
ifest in myriad ways, bringing slowness and tranquil-
lity into the HCD activities. Finally, we found that a
sense of relatedness was essential to participate in the
HCD activities that sometimes complicated the actual
research. The four themes highlight the need for tun-
ing the HCD process and brings the specific role of the
HCD researcher to the foreground. Below, we discuss
this further and relate our findings to prior work.
The Importance of Careful Recruitment and En-
listing of Participants. Given that older adults lack
mental models on interactive technologies, it also im-
plied that it is more difficult for them to understand
what an HCD study actually entails. According to
(Sengpiel et al., 2019; Martin-Hammond et al., 2018;
Czaja et al., 2019), it is therefore important to ensure
a proper understanding before signing up, which was
confirmed in our study. At the same time, this en-
tails the risk of involving only the more tech-savvy
participants with a pre-existing interest in health or
technology, resulting in a biased sample. Moreover,
verbose and lengthy informed consent forms are un-
likely to help. It is therefore important to adjust the
expectations of both researchers and participants prior
to signing up and before each research activity, in or-
der to provide a respectful and useful framework for
everyone. The use of video prompts that illustrate
the problem space (Lindsay et al., 2012) may support
this communication. Pilot testing to identify possible
threats or problems can equally help to gain additional
insights and optimise the recruitment process (Czaja
et al., 2019).
The Challenge of Abstraction in Prototypes. Due
to participants often having low mobile device profi-
ciency and lacking a mental model on using technolo-
gies, it was found difficult to hypothesise about future
innovations. These findings are in line with previous
work (Duh et al., 2016; Lindsay et al., 2012),yet con-
trast with (Sengpiel et al., 2019), who suggested to
rather use abstract descriptions of technology.
The Need for Conscientious HCI Researchers.
Given the vulnerabilities and personal histories of this
older population, there is a need for HCI researchers
who are both empathetic and direct. Researchers
need sensitivity and integrity, to show respect and
give room to dire experiences, yet need to ensure that
structured sessions are kept on track and research fo-
cus is maintained. Moreover, researchers need to en-
sure that all participants are involved during the ses-
sion. When topics fade due to participants trailing off,
it is the role of the researcher to redirect them to the
study in a clear yet empathetic way.
The importance of making room for small talk and
support socialising confirms previous work (Sengpiel
et al., 2019; Davidson and Jensen, 2013a; Chaudhry
et al., 2016). It is at all costs necessary to avoid that
participants get the feeling that they have to pass a
(medical or neuropsychological) test; even more than
with any other age category, the emphasis should be
on ‘do not blame the user’ (Crumlish and Malone,
2009). The crucial role of the researcher is to bal-
ance informal small talk with adequate structure and
guidance, which also confirms results from (Xie et al.,
2012; Lindsay et al., 2012).
Research from (Davidson and Jensen, 2013a; Sen-
gpiel et al., 2019) therefore indicates that it is impor-
tant to be flexible and to adapt to the needs of the
participants. Moreover, providing a safe environment
and additional training could help participants to gain
the confidence they need, which confirms the work by
(Harrington et al., 2018).
To balance all these conflicting demands, having
multiple researchers present in order to provide assis-
tance is not a luxury, but rather mandatory.
5.1 Recommendations
Based on the findings of this study and related work
analysed, we end this paper with a set of recommen-
dations to guide a HCD process of SMHS involv-
ing older adults, structured according to the different
Human-centred Design of Self-management Health Systems with and for Older Adults: Challenges and Practical Guidelines
99

phases and activities of a HCD process.
5.1.1 General Recommendations
Every research study starts with the recruitment of
participants. It is essential to (1) find a balanced com-
position of participants with different backgrounds
and (2) align expectations between participants and
researchers. By (3) reaching out to local contact
points or organisations a varied sample of partici-
pants can be reached, and this can lower their thresh-
old for participation. It is also beneficial to (4) organ-
ise sessions nearby participants, ideally in their home
environment so they do not need to move. However,
when organising group sessions, one should (5) take
care of transport in order to make sure that all inter-
ested participants can join.
Given that participants often take part in research
studies as a networking event or to help out the re-
searchers, it is important to listen to the participant,
(6) leaving room and time for social interludes.
5.1.2 Inspiration Phase Recommendations
Interviews and Focus Group Discussions. During
conversations, it is important to (7) talk loud enough,
and (8) provide a clear structure in the session. It can
help to make things specific and (9) provide tangible
examples, as it is hard for participants to hypothesise
due to their lack of experiences.
Particularly focus group discussions need multiple
moderators and researchers, both for providing gen-
eral and practical assistance. The moderator should
make sure to (10) get everyone on board and thus
(11) paraphrase regularly what was discussed, but
should also (12) provide practical assistance and help
participants to write, bring coffee, etc.
Given that there should be room for small talk, but
also due to the attention span of older adults, every-
thing proceeds slower. Therefore, it is suggested to
(13) limit the topics that need to be discussed. A rule
of thumb could be to multiply the estimated timing
by two. Furthermore, by providing sufficient breaks,
participants also have the (14) possibility to stand up
in between. To ensure that everyone has had enough
time to voice their concerns, it could also help to
(15) limit the number of participants to a maximum
of 6.
5.1.3 Ideation Phase Recommendations
Low-Fidelity Prototypes. Although low-fidelity
prototypes are interesting to test internally with
proxies, it was hard for participants to understand the
interactions based on such a prototype. Participants
often had little ICT experience, thus lacking a mental
model. Therefore, we suggest to (16) avoid testing
paper-prototypes with older adults.
High-Fidelity/Interactive Prototypes. When present-
ing information to participants, it was important to
avoid English terms and (17) translate all words into
their native language, even if these terms are official
mongrel words.
5.1.4 Evaluation Phase Recommendations
Formative/Summative Usability Test. When con-
ducting user-tests, it is important to start with (18) re-
assuring participants that they cannot do anything
wrong. At all cost, it should be (19) avoided that
participants feel that they are tested, instead of the
application. For participants without any ICT experi-
ence, it can be hard to understand what to do. There-
fore (20) providing alternatives for participants who
have no mental model on using a technology can help
them. Especially for user-tests with multiple partici-
pants, it is beneficial to have (21) one moderator or
researcher for every 3 to 4 participants. These are
necessary when participants are stuck or have practi-
cal questions.
Adoption Study. Before starting the experiment it is
important to (22) comfort participants and (23) try out
all features together so participants can first experi-
ment in a safe environment.
Questionnaires. First of all, it is important to
(24) avoid questionnaires that are too long, as par-
ticipants’ attention will decrease, resulting in incom-
plete or incorrectly filled out questionnaires. Further-
more, (25) avoid negative phrased questions as these
can be harder to interpret. In addition, when possible,
(26) ask questions orally.
6 LIMITATIONS AND FUTURE
WORK
For the participants’ recruitment, we aimed for a het-
erogeneous sample in which we also included the old-
est old. However, given that participants chose them-
selves whether to participate or not, self-selection was
inevitable. This could also introduce bias in the find-
ings by favouring those who were cognitively or phys-
ically stronger. However, given the transitional qual-
ity of ageing (Durick et al., 2013), it is hard to dis-
tinguish participants based on only age or ability, as
this would simplify the ageing process without hav-
ing a sound theory (Vines et al., 2015). Moreover,
we acknowledge that this research study has come to
ICT4AWE 2021 - 7th International Conference on Information and Communication Technologies for Ageing Well and e-Health
100

life by studying our own practicalities and that it is
limited to these experiences on what did or did not
work. Therefore, future work is necessary to validate
our recommendations.
7 CONCLUSION
In this study, we report findings based on a four-year
HCD process conducted with 81 older adults (median
age=83). Based on a thematic analysis, four themes
emerged: ‘a life course marked by grand experi-
ences’, ‘a discomfort with unknown digital technolo-
gies’, ‘impact of age-related impairments’, and ‘relat-
edness as core to research participation’. Moreover,
each theme presents insights and guidelines, which
are summarised in section 5.1. This study contributes
by offering lessons learned in the different phases of
an HCD process. Our aim is that these guidelines
can help future researchers to undertake more effec-
tive and useful study designs.
ACKNOWLEDGEMENTS
We would like to thank InnovAge, Zorg Leuven, and
Triamant for their participation, as well as all partici-
pants for helping out during one or multiple phases in
this research study.
REFERENCES
Amaro, A. C., Rodrigues, R., and Oliveira, L. (2020).
Engaging older adults in participatory and intergen-
erational design teams and processes: a systematic
review of the current investigation. ESSACHESS–
Journal for Communication Studies, 13(2 (26)):157–
181.
Association for Computing Machinery (2021). Acm digital
library.
Brown, T. et al. (2008). Design thinking. Harvard business
review, 86(6):84.
Chaudhry, B., Duarte, M., Chawla, N. V., and Dasgupta,
D. (2016). Developing health technologies for older
adults: methodological and ethical considerations. In
Proceedings of the 10th EAI International Conference
on Pervasive Computing Technologies for Healthcare,
pages 330–332.
Clarke, V. and Braun, V. (2014). Thematic analysis. In En-
cyclopedia of critical psychology, pages 1947–1952.
Springer.
Cooley, M. (1996). On human-machine symbiosis. In Hu-
man Machine Symbiosis, pages 69–100. Springer.
Cooper, A., Reimann, R., and Cronin, D. (2007). About face
3: the essentials of interaction design. John Wiley &
Sons.
Cornet, V. P., Toscos, T., Bolchini, D., Ghahari, R. R.,
Ahmed, R., Daley, C., Mirro, M. J., and Holden, R. J.
(2020). Untold stories in user-centered design of mo-
bile health: practical challenges and strategies learned
from the design and evaluation of an app for older
adults with heart failure. JMIR mHealth and uHealth,
8(7):e17703.
Crumlish, C. and Malone, E. (2009). Designing social in-
terfaces: Principles, patterns, and practices for im-
proving the user experience. O’Reilly Media, Inc.
Czaja, S. J., Boot, W. R., Charness, N., and Rogers, W. A.
(2019). Designing for older adults: Principles and
creative human factors approaches. CRC press.
Davidson, J. L. and Jensen, C. (2013a). Participatory design
with older adults: an analysis of creativity in the de-
sign of mobile healthcare applications. In Proceedings
of the 9th ACM Conference on Creativity & Cognition,
pages 114–123.
Davidson, J. L. and Jensen, C. (2013b). What health top-
ics older adults want to track: a participatory design
study. In Proceedings of the 15th International ACM
SIGACCESS Conference on Computers and Accessi-
bility, pages 1–8.
De Witte, N. and Van Daele, T. (2017). Vlaamse UTAUT-
vragenlijst.
D’Haeseleer, I., Gerling, K., Schreurs, D., Vanrumste, B.,
and Vanden Abeele, V. (2019). Ageing is not a dis-
ease: Pitfalls for the acceptance of self-management
health systems supporting healthy ageing. In The 21st
International ACM SIGACCESS Conference on Com-
puters and Accessibility, pages 286–298.
Duh, E. S., Guna, J., Poga
ˇ
cnik, M., and Sodnik, J. (2016).
Applications of paper and interactive prototypes in de-
signing telecare services for older adults. Journal of
medical systems, 40(4):92.
Duque, E., Fonseca, G., Vieira, H., Gontijo, G., and Ishitani,
L. (2019). A systematic literature review on user cen-
tered design and participatory design with older peo-
ple.
Durick, J., Robertson, T., Brereton, M., Vetere, F., and
Nansen, B. (2013). Dispelling ageing myths in tech-
nology design. In Proceedings of the 25th Australian
Computer-Human Interaction Conference: Augmen-
tation, Application, Innovation, Collaboration, pages
467–476.
Gould, J. D. and Lewis, C. (1985). Designing for usability:
key principles and what designers think. Communica-
tions of the ACM, 28(3):300–311.
Harrington, C. N., Wilcox, L., Connelly, K., Rogers, W.,
and Sanford, J. (2018). Designing health and fit-
ness apps with older adults: Examining the value of
experience-based co-design.
Heart, T. and Kalderon, E. (2013). Older adults: Are they
ready to adopt health-related ICT? International Jour-
nal of Medical Informatics, 82(11):e209–e231.
InnovAge (2016). Innovage.
ISO, I. O. f. S. (2019). Iso 9241–210: 2019 (en) er-
Human-centred Design of Self-management Health Systems with and for Older Adults: Challenges and Practical Guidelines
101

gonomics of human-system interaction—part 210:
Human-centred design for interactive systems.
Kononova, A., Li, L., Kamp, K., Bowen, M., Rikard, R.,
Cotten, S., and Peng, W. (2019). The use of wear-
able activity trackers among older adults: Focus group
study of tracker perceptions, motivators, and barriers
in the maintenance stage of behavior change. JMIR
mHealth and uHealth, 7(4):e9832.
Lindsay, S., Jackson, D., Schofield, G., and Olivier, P.
(2012). Engaging older people using participatory de-
sign. In Proceedings of the SIGCHI conference on hu-
man factors in computing systems, pages 1199–1208.
Martin-Hammond, A., Vemireddy, S., and Rao, K. (2018).
Engaging older adults in the participatory design of
intelligent health search tools. In Proceedings of the
12th EAI International Conference on Pervasive Com-
puting Technologies for Healthcare, pages 280–284.
Mehrotra, S., Motti, V. G., Frijns, H., Akkoc, T., Yengec¸,
S. B., Calik, O., Peeters, M. M., and Neerincx, M. A.
(2016). Embodied conversational interfaces for the
elderly user. In Proceedings of the 8th Indian Confer-
ence on Human Computer Interaction, pages 90–95.
Muller, M. J. and Kuhn, S. (1993). Participatory design.
Communications of the ACM, 36(6):24–28.
Nunes, F., Verdezoto, N., Fitzpatrick, G., Kyng, M.,
Gr
¨
onvall, E., and Storni, C. (2015). Self-care tech-
nologies in hci: Trends, tensions, and opportunities.
ACM Transactions on Computer-Human Interaction
(TOCHI), 22(6):1–45.
Peek, S. T., Luijkx, K. G., Rijnaard, M. D., Nieboer, M. E.,
van der Voort, C. S., Aarts, S., van Hoof, J., Vrijhoef,
H. J., and Wouters, E. J. (2016). Older adults’ reasons
for using technology while aging in place. Gerontol-
ogy, 62(2):226–237.
Sanders, E. B. (2002). From user-centered to participatory
design approaches. Design and the social sciences:
Making connections, 1(8):1.
Sengpiel, M., Volkmann, T., and Jochems, N. (2019).
Considering older adults throughout the development
process–the hcd+ approach. Proceedings of the Hu-
man Factors and Ergonomics Society Europe, pages
5–15.
Sintonen, S. and Immonen, M. (2013). Telecare services
for aging people: Assessment of critical factors influ-
encing the adoption intention. Computers in Human
Behavior, 29(4):1307–1317.
Triamant (2020). Triamant group.
Vines, J., Pritchard, G., Wright, P., Olivier, P., and Brit-
tain, K. (2015). An Age-Old Problem: Examining the
Discourses of Ageing in HCI and Strategies for Fu-
ture Research. ACM Trans. Comput.-Hum. Interact.,
22(1):2:1–2:27.
Volkmann, T., Sengpiel, M., and Jochems, N. (2016). Histo-
rytelling: a website for the elderly a human-centered
design approach. In Proceedings of the 9th Nordic
Conference on Human-Computer Interaction, pages
1–6.
von Humboldt, S. and Leal, I. (2015). The old and the
oldest-old: Do they have different perspectives on ad-
justment to aging? International Journal of Gerontol-
ogy, 9(3):156–160.
Xie, B., Yeh, T., Walsh, G., Watkins, I., and Huang, M.
(2012). Co-designing an e-health tutorial for older
adults. In Proceedings of the 2012 iConference, pages
240–247.
Zorg Leuven (2020). Zorg leuven. (Accessed on
03/12/2020).
ICT4AWE 2021 - 7th International Conference on Information and Communication Technologies for Ageing Well and e-Health
102
