A Cone Beam Computed Tomography Annotation Tool for Automatic
Detection of the Inferior Alveolar Nerve Canal
Cristian Mercadante
1
, Marco Cipriano
1
, Federico Bolelli
1
, Federico Pollastri
1
,
Mattia Di Bartolomeo
2
, Alexandre Anesi
3
and Costantino Grana
1
1
Department of Engineering “Enzo Ferrari”,
University of Modena and Reggio Emilia, Via P. Vivarelli 10, 41125 Modena, Italy
2
Surgery, Dentistry, Maternity and Infant Department, Unit of Dentistry and Maxillo-Facial Surgery,
University of Verona, P.le L.A. Scuro 10, 37134 Verona, Italy
3
Department of Medical and Surgical Sciences for Children & Adults, Cranio-Maxillo-Facial Surgery,
University of Modena and Reggio Emilia, Largo del Pozzo 71, 41124 Modena, Italy
crimerca96@gmail.com, mattiadiba@hotmail.it
Keywords:
CBCT, IAC, IAN, Annotation Tool, Segmentation.
Abstract:
In recent years, deep learning has been employed in several medical fields, achieving impressive results. Un-
fortunately, these algorithms require a huge amount of annotated data to ensure the correct learning process.
When dealing with medical imaging, collecting and annotating data can be cumbersome and expensive. This
is mainly related to the nature of data, often three-dimensional, and to the need for well-trained expert tech-
nicians. In maxillofacial imagery, recent works have been focused on the detection of the Inferior Alveolar
Nerve (IAN), since its position is of great relevance for avoiding severe injuries during surgery operations
such as third molar extraction or implant installation. In this work, we introduce a novel tool for analyzing
and labeling the alveolar nerve from Cone Beam Computed Tomography (CBCT) 3D volumes.
1 INTRODUCTION
Maxillofacial surgery is a medical-surgical field that
concerns the diagnosis and treatment of a wide vari-
ety of head and neck pathologies, including functional
and aesthetic problems. Maxillofacial surgical inter-
ventions comprise oral and dental operations. Among
the cited surgical interventions, the extraction of im-
pacted teeth (especially third molars) and the implant-
prosthetic rehabilitation are two of the most common
procedures. This kind of surgical interventions are
routinely executed and may become very tricky due
to the risk of damaging the Inferior Alveolar Nerve
(IAN).
This sensory nerve supplies the omolateral sensi-
bility to part of the lower third of the face and of the
inferior dental arch. In order to preserve this noble
structure during the surgery, an accurate preoperative
planning must be done and has to include the local-
ization of the IAN. Its position might be indirectly de-
duced via the individuation of the mandibular canal,
also known as Inferior Alveolar Canal (IAC), which
runs inside the mandibular bone. The nerve might be
in close relation to the roots of impacted teeth (es-
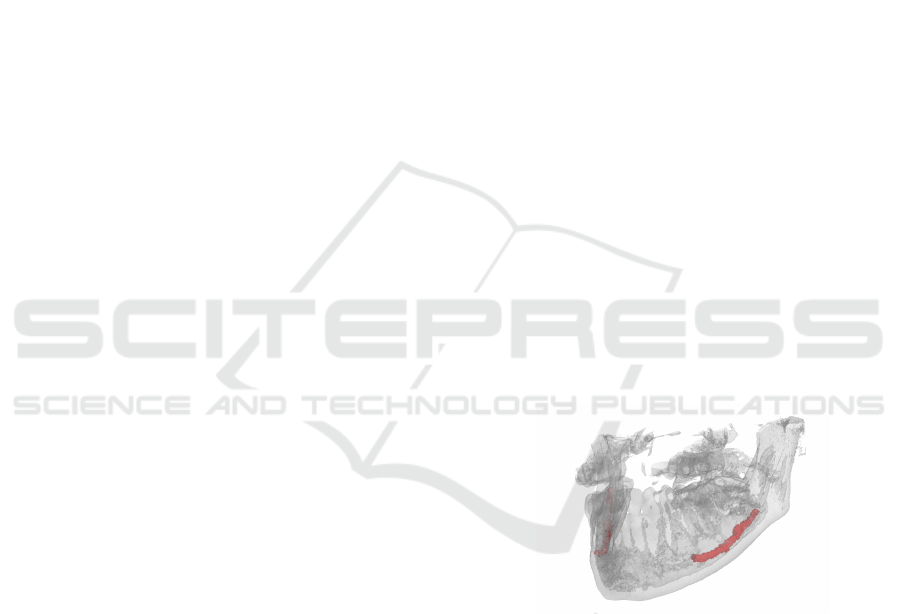
Figure 1: 3D view of a jawbone (gray) underlying the lo-
cation of the IAC (red). The original volume has been ac-
quired with Cone Beam Computed Tomography.
pecially the molars) and a detailed 3D description
of their positions must be comprehended before the
surgery. A dental implant consists in the surgical in-
sertion of an artificial root into the jawbone to provide
anchorage for a dental prosthesis replacing the miss-
ing tooth (implant-prosthetic rehabilitation). To this
purpose, to plan and place accurately a dental implant
it is mandatory to know the linear distance from the
midpoint of the alveolar crest to the IAC.
In order to facilitate the identification of the IAN,
many computer-based techniques have been proposed
in the past. Most of the approaches available in the
724
Mercadante, C., Cipriano, M., Bolelli, F., Pollastri, F., Di Bartolomeo, M., Anesi, A. and Grana, C.
A Cone Beam Computed Tomography Annotation Tool for Automatic Detection of the Inferior Alveolar Nerve Canal.
DOI: 10.5220/0010392307240731
In Proceedings of the 16th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2021) - Volume 4: VISAPP, pages
724-731
ISBN: 978-989-758-488-6
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
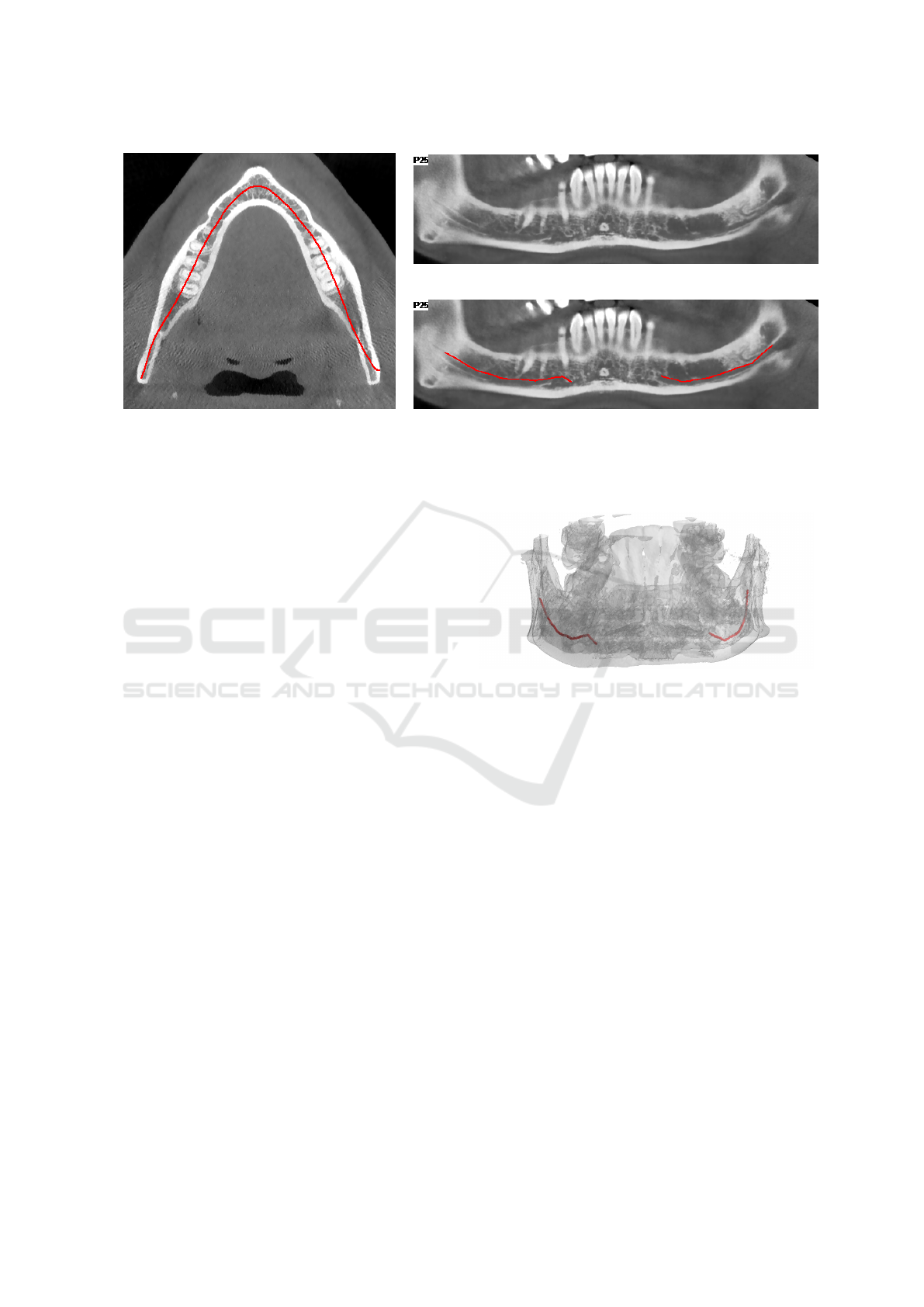
(a) Axial Slice
(b) Original Panoramic View
(c) Annotated Panoramic View
Figure 2: Example of CT annotation based on 2D panoramic views. (a) is an axial slice of the CT where a panoramic base
curve is highlighted in red. (b) is the panoramic view obtained from the CT-volume displaying voxels of the curved plane
generated by the base curve and orthogonal to the axial view. (c) is the same view of (b) showing a manual annotation of the
IAC performed by an expert technician. A 3D view of the CT scan with the same annotation as (c) is reported in Figure 3.
literature focus on the identification of the IAC. As
a matter of fact, the canal is clearly identifiable in
both 2D panoramic radiography —also named Or-
thoPantomoGram (OPG)— and Computed Tomogra-
phy (CT) (Sotthivirat and Narkbuakaew, 2006).
Algorithms based on panoramic radiography re-
ported higher accuracy (Vinayahalingam et al., 2019).
However, OPG images just show the IAN from a sin-
gle point of view, masking the real complexity of the
3D canal structure. Moreover, such a kind of images
usually provide geometrical distorted data (Abra-
hams, 2001) and no information about depth (Sot-
thivirat and Narkbuakaew, 2006). This is why state-
of-the-art approaches tackle the task considering the
entire 3D volume obtained with CT scanners (Kondo
et al., 2004; Kwak et al., 2020). These three-
dimensional data can be reformatted into panoramic
reconstructions (panoramic views) thus being able to
apply 2D strategies also on 3D data. With respect to
OPG, panoramic reconstructions are not affected by
distortion, superimposition of other tissues or magni-
fication errors, permitting a more accurate assessment
of CT data.
In recent years, deep learning algorithms have re-
vealed to be extremely effective solutions to tackle
multiple image processing and computer vision tasks.
In particular, Convolutional Neural Networks (CNNs)
are currently the cornerstone of medical image anal-
ysis (Ronneberger et al., 2015; Esteva et al., 2017;
Canalini et al., 2019; Pollastri et al., 2019; Ligabue
et al., 2020; Pollastri et al., 2021). These techniques
have been recently applied also to the segmentation of
the IAC (Vinayahalingam et al., 2019; Hwang et al.,
2019; Kwak et al., 2020). Unfortunately, they require
Figure 3: 3D view of the manual annotation performed by
an expert technician on the panoramic of Figure 2c.
huge amounts of data, which are hard to obtain and
particularly expensive to annotate, especially in med-
ical fields. However, simple elements like lines and
colors are learned from the first convolutional layers
of CNNs models. For this reason, neural networks
pre-trained with existing collections of natural im-
ages can mitigate the need for large annotated medical
datasets (Deng et al., 2009; Li et al., 2015).
Nevertheless, this approach can not be the panacea
since it may introduce biases towards certain charac-
teristics and features. As an example, CNNs trained
using ImageNet are strongly biased in recognizing
textures rather than shapes (Geirhos et al., 2018).
Several proprietary tools for annotating the infe-
rior alveolar canal from computed tomography scans
are available in the literature. Such tools are usually
supplied together with CT scanners and not other-
wise accessible. Moreover, most of them only pro-
vide two dimensional annotation mechanisms based
on panoramic reconstructions from CT data (an ex-
planatory example is reported in Figure 2).
A Cone Beam Computed Tomography Annotation Tool for Automatic Detection of the Inferior Alveolar Nerve Canal
725

This paper proposes a novel IAC Annotation Tool
(IACAT in short) that aims to overcome the aforemen-
tioned limitations, guaranteeing a more accurate an-
notation while speeding up and simplifying the man-
ual effort of expert technicians.
In Section 2, imaging techniques for maxillofacial
surgery and deep learning approaches for the auto-
matic detection of the inferior alveolar nerve are de-
tailed, focusing on the employed data. Section 3 de-
scribes the annotation tool released with this paper.
Finally, some conclusions are drawn in Section 4.
2 RELATED WORK
2.1 Imaging for Maxillofacial Surgery
Many imaging techniques have been used in the past
for implant dentistry. Among them, OrthoPantomo-
Gram (OPG), Computed Tomography (CT), and Cone
Beam Computed Tomography (CBCT) are certainly
the most widespread. In clinical research, CBCT is
increasingly being used for 3D assessment of bone
and soft tissue (Benic et al., 2015).
The term orthopantomogram, orthopantomogra-
phy, panoramic tomography or OPG in short, refers to
panoramic single image radiography of the mandible,
maxilla and teeth. This technique is based on X-ray
and the OPG unit is designed to rotate around the head
of the patient during the scan. It represents an inex-
pensive and rapid way to evaluate the gross anatomy
of the jaws and related structures, but its limits are
bidimensionality and structure distortion.
Computed Tomography, instead, refers to a com-
puterized X-ray imaging procedure that provides
more complete and detailed information than OPG.
CT employs a narrow beam of X-rays and the ma-
chine emitting this beam quickly rotated around the
body, producing signals that are then processed by a
computer. The output of the CT scanner are cross-
sectional images (slices) of the analyzed body section.
Sequential slices can be digitally stacked to form a 3D
volume, allowing for easier identification and location
of basic structures.
Cone Beam Computed Tomography is a variation
of the traditional Computed Tomography and rep-
resents the most commonly employed 3D imaging
modality in dentistry, both for treatment planning and
postoperative evaluation (Jaju and Jaju, 2014).
A CBCT scanner employs a cone beam radiating
from an X-ray source in the shape of a cone. The
use of this particular shape allows to cover large vol-
umes while performing a single rotation around the
patient. CBCT imaging is powerful and presents a de-
creased effective radiation dose exposure to patients
compared to traditional multi-slice CT (Silva et al.,
2008; Ludlow and Ivanovic, 2008; Loubele et al.,
2009; Carrafiello et al., 2010)
The entire 3D volume is then reconstructed pro-
cessing acquired data with specific algorithms. A
sample view of CBCT-acquired 3D volume is re-
ported in Figure 1.
2.2 IAC Automatic Detection
Given the relevance of the task, many efforts have
been given to employ computer vision for IAC au-
tomatic detection. The first approach (Kondo et al.,
2004) consisted in reformatting the original CT im-
ages to obtain panoramic reconstructions from CT
data (panoramic views), which are a series of cross-
sectional images along the mandible (lower jawbone).
Voxel intensities and 3D gradients are then exploited
to identify empty canals in the panoramic views. The
axis of the IAC is then traced out by a 3D line-tracking
technique, effectively extracting the IAC despite the
open structure of the surrounding bone.
In the same year, Hanssen et al. presented a
method for 3D segmentation of the same nerve chan-
nels in the human mandible. Their technique utilizes
geodesic active surfaces, implemented with level sets,
and consists of two steps. For the first step, two points
are defined to denote the entry and exit of the nerve
channel, and a connecting path of minimal action in-
side the channel is calculated. This calculation is
driven by the gray values in proximity to the two de-
fined points inside the channel. For the next step, the
authors exploit this path as an initial configuration,
and let an active surface evolve until the inner borders
of the channel are reached (Hanssen et al., 2004).
Two years later a new technique was introduced
to automatically detect the alveolar nerve canals on
panoramic reconstructions from CT data (Sotthivirat
and Narkbuakaew, 2006). By using a set of axial
CT images acquired from the CT scanner, a series
of panoramic images are generated along the dental
curve. Generated images are then processed by means
of contrast enhancement and Gaussian smoothing fil-
tering before being fed to a detection algorithms
based on the distance transform of the edge image,
morphological operations, and an approximation of
the nerve canals shape.
In more recent times this task has been affected,
as the the rest of the medical imaging area, by
the groundbreaking rise of deep learning. In 2019,
Vinayahalingam et al. focus on detecting the IAN and
the third molar in Orthopantomogram Panoramic Ra-
VISAPP 2021 - 16th International Conference on Computer Vision Theory and Applications
726
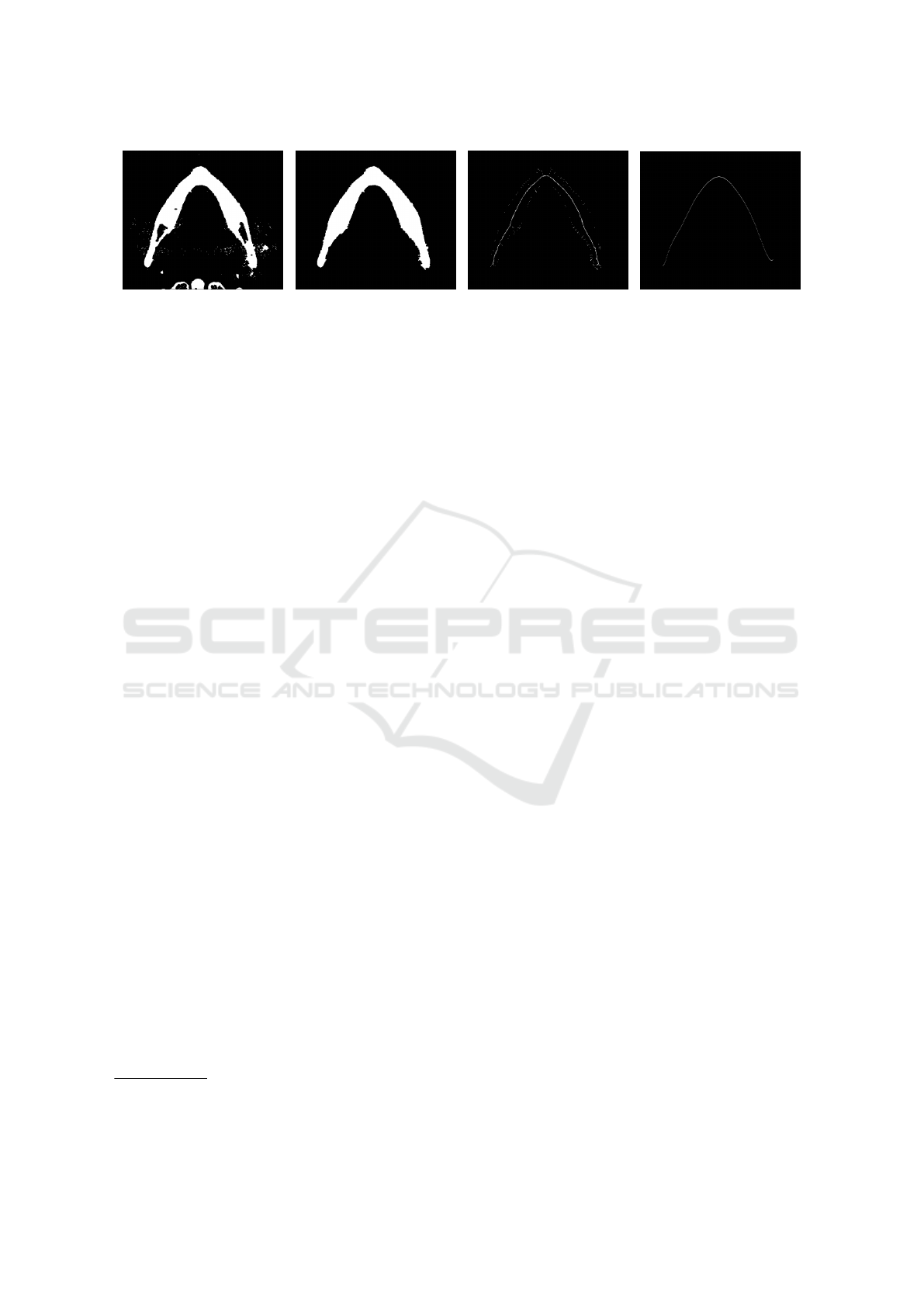
(a) Closing & Thresholding (b) CCL (c) Skeletonization (d) Polynomial Approx.
Figure 4: Automatic arch detection steps.
diographs (OPG) (Vinayahalingam et al., 2019).
The authors claim that specific radiographic fea-
tures on OPGs such as darkening of the root, nar-
rowing of the mandibular canal, interruption of the
white line, are risk factors for IAN injuries. Accord-
ingly, they employ deep learning in the detection of
third molars, mandibular canals, and for the identifi-
cation of certain radiological signs for potential IAN
injuries.
The following year, a preliminary research for a
dental segmentation automation tool on CT scans has
been published (Kwak et al., 2020). In this paper, a set
of experiments were conducted on models based on
2D SegNet (Badrinarayanan et al., 2017), 2D and 3D
U-Net (Ronneberger et al., 2015; C¸ ic¸ek et al., 2016).
3 THE IAC ANNOTATION TOOL
Most of the datasets employed in literature for the au-
tomatic segmentation of the inferior alveolar nerve
have been annotated using proprietary software, e.g.
Photoshop
1
and Invivo
2
. However, working with
3D data can be laborious and time-consuming. This
paper proposes a tool for smoothing the burden of
manual annotation, specifically designed for the IAN
canal. It processes and visualizes CBCT data stored
in DICOM format, driving the user towards the anno-
tation of axial images, panoramic and cross-sectional
views. Annotated data can be easily exported to be
employed in multiple tasks, e.g. the training of deep
learning models.
3.1 Pre-processing
The tool requires a DICOM input, in particular a
DICOMDIR file linked to dcm files, representing single
axial images of the scan. Radiography values repre-
sent attenuation of the X-rays emitted and captured
by a detector. These measures are always considered
1
https://www.photoshop.com
2
https://www.anatomage.com/invivo
on the Hounsfield scale, where higher numbers indi-
cate a high attenuation. After loading the scan vol-
ume, a saturation threshold is applied: bone voxels
have Hounsfield units usually in the range [400, 3000]
(Nysj
¨
o, 2016), but peak values around 14 000 usually
correspond to the tooth crown and enamel (less of 2%
of the volume). Since the IAN canal is not involved in
this operation, it is reasonable to saturate from the top
with the 0.98 percentile value. The values are then
normalized in the range [0, 1] and stored as 32 bits
floating point values without loosing any information.
This pre-processing acts as a contrast stretching of the
original DICOM values.
3.2 Axial Image Annotation
After loading the input data, the arch approximation
that better describes the canal course must be iden-
tified inside one of the axial images. This process
is partially automated and aims to segment the gums
region in order to obtain a skeleton and to approxi-
mate it with a polynomial. A morphological closing
(Gil and Kimmel, 2002) with an elliptical 5 × 5 struc-
turing element is applied in order to close gaps in-
side foreground regions. Then, the image is binarized
by selecting the threshold value so that foreground
pixels are between 12% to 16% of the image. Con-
nected Components Labeling (CCL) (Bolelli et al.,
2019) is employed to keep only the biggest object —
the gums— by removing all the other components.
Inner holes are filled with a second CCL pass, produc-
ing a binary image with the gums region appearing as
a filled arch. Image skeletonization is then performed
using thinning (Bolelli and Grana, 2019). The out-
put is a one pixel thick curve crossing the dental arch,
which is approximated with a polynomial. The entire
process is depicted in Figure 4.
Once the axial image and its arch approxima-
tion are selected, the tool generates a Catmull-Rom
spline (Catmull and Rom, 1974; Barry and Goldman,
1988) by sampling the polynomial to select the con-
trol points of the spline. This curve is the base of
a Curved Planar Reformation (CPR) that produces
A Cone Beam Computed Tomography Annotation Tool for Automatic Detection of the Inferior Alveolar Nerve Canal
727

(a) (b) (c) (d) (e)
(f) (g) (h) (i) (j)
Figure 5: Morphological Geodesic Active Contours evolution on a sequence of cross-sectional images.
a panoramic 2D image. This view is obtained dis-
playing voxels of the curved plane corresponding the
base curve and orthogonal to the axial slice. When
the user moves, creates or removes control points, the
panoramic view changes accordingly. The goal of this
step is to highlight the IAC on the panoramic view, by
finding the best arch curve. The user can also offset
the position of this curve in order to produce an upper
and lower panoramic view, thus ensuring a better edit-
ing of the spline itself (Sotthivirat and Narkbuakaew,
2006).
Two offset curves (outer and inner) are drawn with
distance 50 pixels from the main arch. For each
point of the spline, a perpendicular line called Cross-
Sectional Line (CSL) is computed. Since the points
of the spline are as many as the euclidean distance be-
tween two control points, a different resolution of the
spline would generate more or less CSLs. These lines
are the base of Multi Planar Reformations (MPRs)
called Cross-Sectional Views (CSVs). These are 2D
images obtained interpolating the values of the re-
spective base line across the whole volume height.
3.3 Annotating Cross-sectional Views
For each CSV, the user can draw a closed Catmull-
Rom spline to annotate the position of the IAC.
As usual, control points can be created, deleted, or
moved. To speed-up the annotation phase, an active
contour model (Kass et al., 1988) is used to automat-
ically propagate the annotation to the following im-
age. In particular, Morphological Geodesic Active
Contours have been selected (Caselles et al., 1997;
Alvarez et al., 2010): this technique employs mor-
phological operators to evolve the curve, combined
with the concept of energy minimization in the prob-
lem of geodesic curve computation. In absence of
gradients, this algorithm forces the contour to expand
—the balloon factor— whereas other active contour
approaches shrink object shapes.
In order to propagate the annotation to the fol-
lowing (or previous) cross-sectional view, the Mor-
phological Geodesic Active Contours algorithm re-
quires two inputs: the current annotation as a binary
mask, and the gradients of the following (or previous)
CSV. The output of the algorithm is a new annotation
mask from which the tool generates the spline with
an amount of control points that depends on its length
(the longer it is, the more control points are needed
to approximate the real shape). The model runs for 5
iterations, with a smoothing factor of 1, and a balloon
factor of 1. Figure 5 shows the evolution of the spline
in subsequent images, starting from a manual annota-
tion, up to the ninth following image. The model is
able to create accurate annotations without user inter-
vention for many consecutive images. In this exam-
ple, the first mistake appears in Figure 5i (the top edge
of the spline), and is propagated into Figure 5j.
Any user adjustment can be automatically propa-
gated to the following views.
The splines are saved as the coordinates of their
control points, and a label mask is generated for each
CSV. The labels employed are four (C¸ ic¸ek et al.,
2016): unlabeled, background, contour, interior. Im-
ages that are not annotated inherit unlabeled class by
default. Otherwise, the mask is set to background,
with the spline labeled as contour and internal pixels
labeled as interior.
3.4 Tilted Cross-sectional Views
An important feature introduced in the IACAT tool
is the extraction of CSVs orthogonal to the canal
slope. To achieve this goal, the Cross-Sectional
VISAPP 2021 - 16th International Conference on Computer Vision Theory and Applications
728
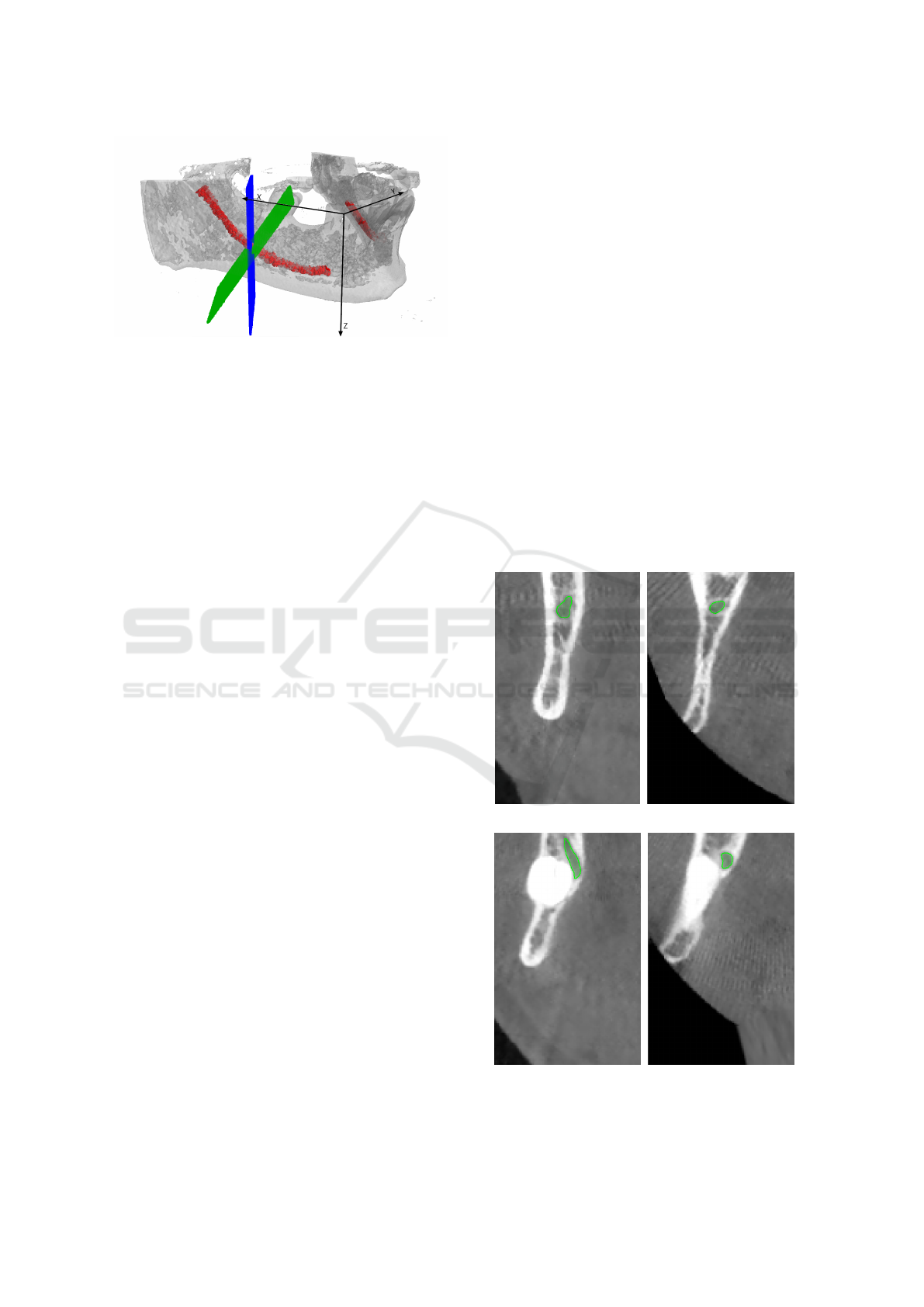
Figure 6: A visualization of the cross-sectional plane ro-
tation around the y axis, as described in Section 3.4. The
original plane is presented in blue, whereas the tilted one is
green. The IAC is red.
Planes (CSPs) used for generating the CSVs are tilted
accordingly.
On the panoramic view, the user can draw two
Catmull-Rom splines which indicate the canal posi-
tion, one for each branch. For each point p of the
spline, the slope can be computed by using the deriva-
tive of a 12
th
order polynomial fit f :
β(p) = −arctan( f
0
(p)) (1)
Given the slope of the canal, the cross-sectional
view orthogonal to the canal is obtained as follows:
• The cross-sectional plane is translated so that its
center is placed at the origin of the reference sys-
tem;
• The plane is rotated around the z axis, until it be-
comes parallel to the y axis. The following Equa-
tion shows the rotation matrix, where u is the unit
vector of the plane:
u
y
−u
x
0
u
x
u
y
0
0 0 1
(2)
• The plane is then rotated around the y axis, by the
angle β obtained with Equation 1, using the fol-
lowing rotation matrix:
cosβ 0 sin β
0 1 0
sinβ 0 cosβ
(3)
• Finally, the plane is rotated back around the z axis
to its original position, using the rotation matrix in
Equation 4, and the initial translation is reversed.
u
y
u
x
0
−u
x
u
y
0
0 0 1
(4)
The CSVs are generated from the rotated planes, us-
ing bilinear interpolation. In most cases, since the
canal has a slight inclination, the tilted cross-sectional
views do not differ much from the straight ones. Fig-
ure 7 shows two examples in which tilted views pro-
vide strong improvements to the IAC localization.
3.5 Annotation Re-projection
The re-projection of the labeled masks in 3D is re-
quired to generate the final segmentation. A plane
corresponds to each cross-sectional image, which
contains the floating point coordinates of the volume
voxels used to interpolate a certain pixel in the image.
For each pixel of the image, its label is re-projected in
the corresponding voxel coordinate. To prevent alias-
ing due to the undersampling of the voxel coordinates
in the volume, each label is copied to the positions
corresponding to the f loor and ceil of each coordi-
nate of the plane. Figure 8 shows the results obtained
re-projecting straight cross-sectional images annota-
tion masks in 3D (considering only contour and inte-
rior labels).
The surface of the reconstructed volume is often
irregular, due to the nature of the 2D annotations.
(a) (b)
(c) (d)
Figure 7: Comparison of straight (a), (c) and tilted (b), (d)
cross-sectional images.
A Cone Beam Computed Tomography Annotation Tool for Automatic Detection of the Inferior Alveolar Nerve Canal
729
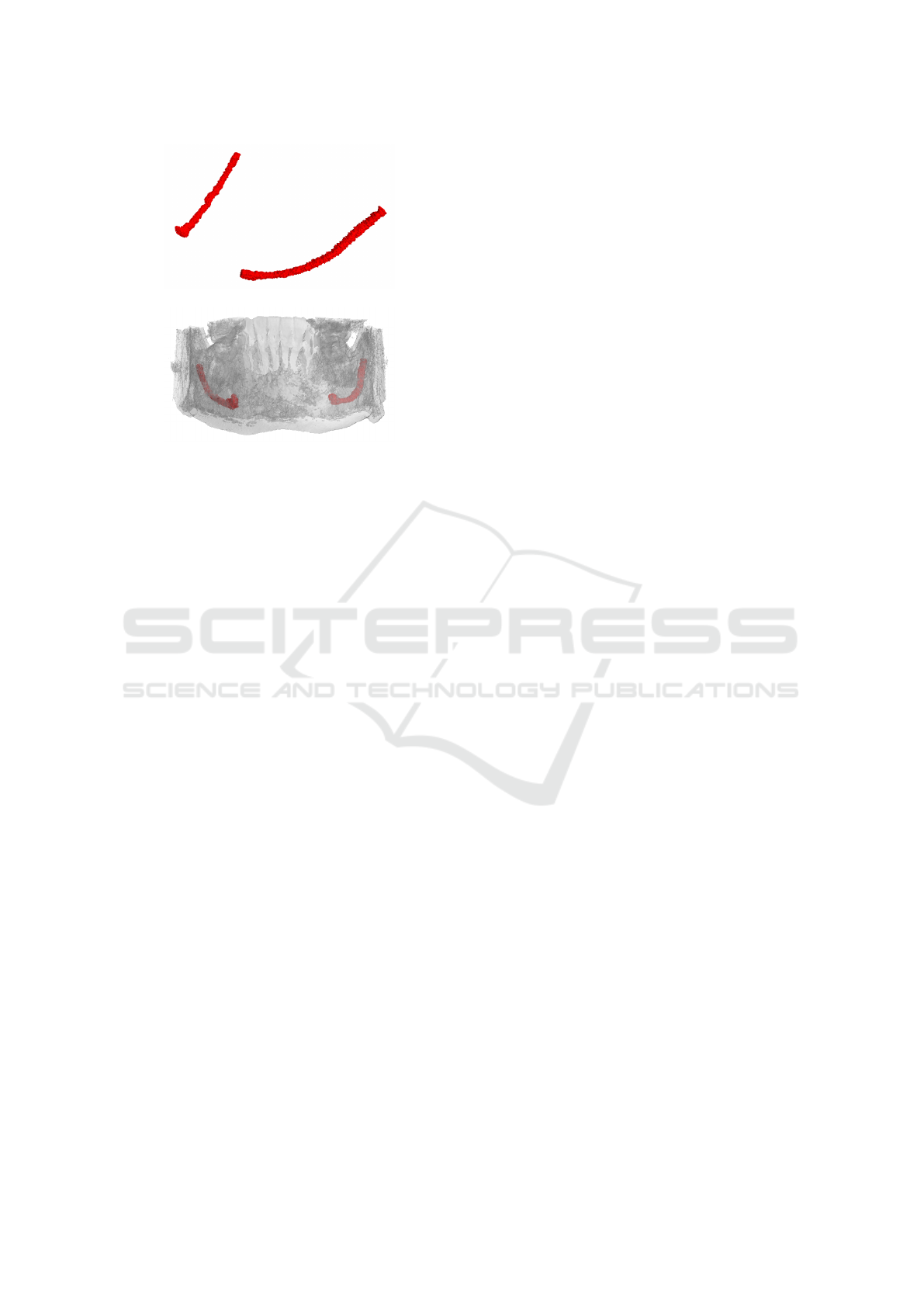
(a)
(b)
Figure 8: (a) 3D view of the canal reconstruction and (b) its
location inside the jawbone.
Therefore, a smoothing process is proposed to pro-
duce a polished contour on the 3D canal shape. A
22 × 22 × 22 kernel is moved with stride 18 along the
reconstructed canal volume. At each step, the convex
hull is evaluated on the current block, obtaining a set
of triangles that composes the convex hull. These tri-
angles are then voxelized and the smoothed canal is
created. The described approach generate a more reg-
ular and uniform segmentation at the expense of the
final accuracy.
3.6 Exports
The annotation can finally be exported as binary npy
files. The two main formats are the concatenation
of cross-sectional image masks and the re-projected
3D annotation. The tool is also able to generate png
images, both for cross-sectional images and their la-
beled masks, and to create a new DICOM file with an-
notations as overlays. An important feature of the
tool is the recording of user actions, in particular of
every interaction with the splines (on axial images,
panoramic views and cross-sectional images). In-
deed, future research directions include the automa-
tion of more steps in the annotation process, by learn-
ing from the actions of an expert. Therefore, cre-
ation, removal and changes in splines control points
are recorded, with contextual information, such as the
current cross-sectional image index. Moreover, the
tool records whether the user is propagating the anno-
tations or resetting the current spline. The history of
actions can be saved on disk in json format.
4 CONCLUSION
In this paper we presented IACAT, a software for the
annotation of CBCT scans. The proposed tool com-
prises and improves the functionality of existing an-
notation tools for the segmentation of Inferior Alve-
olar Nerve, simplifying and improving the work of
expert technicians. The image processing techniques
implemented allow to automatically extend manual
annotations carried out on portions of the volume,
thus speeding up the entire process.
REFERENCES
Abrahams, J. J. (2001). Dental ct imaging: A look at the
jaw. Radiology, 219(2):334–345.
Alvarez, L., Baumela, L., Henriquez, P., and Marquez-
Neila, P. (2010). Morphological snakes. In 2010
IEEE Computer Society Conference on Computer Vi-
sion and Pattern Recognition, pages 2197–2202.
Badrinarayanan, V., Kendall, A., and Cipolla, R. (2017).
SegNet: A Deep Convolutional Encoder-Decoder Ar-
chitecture for Image Segmentation. IEEE Transac-
tions on Pattern Analysis and Machine Intelligence,
39:2481–2495.
Barry, P. and Goldman, R. (1988). A Recursive Evaluation
Algorithm for a Class of Catmull-Rom Splines. ACM
SIGGRAPH Computer Graphics, 22:199–204.
Benic, G. I., Elmasry, M., and H
¨
ammerle, C. H. (2015).
Novel digital imaging techniques to assess the out-
come in oral rehabilitation with dental implants: a
narrative review. Clinical Oral Implants Research,
26:86–96.
Bolelli, F., Allegretti, S., Baraldi, L., and Grana, C. (2019).
Spaghetti Labeling: Directed Acyclic Graphs for
Block-Based Connected Components Labeling. IEEE
Transactions on Image Processing, 29(1):1999–2012.
Bolelli, F. and Grana, C. (2019). Improving the Perfor-
mance of Thinning Algorithms with Directed Rooted
Acyclic Graphs. In Image Analysis and Processing -
ICIAP 2019, volume 11752, pages 148–158. Springer.
Canalini, L., Pollastri, F., Bolelli, F., Cancilla, M., Alle-
gretti, S., and Grana, C. (2019). Skin Lesion Segmen-
tation Ensemble with Diverse Training Strategies. In
Computer Analysis of Images and Patterns, volume
11678, pages 89–101. Springer.
Carrafiello, G., Dizonno, M., Colli, V., Strocchi, S., Taubert,
S. P., Leonardi, A., Giorgianni, A., Barresi, M., Mac-
chi, A., Bracchi, E., et al. (2010). Comparative
study of jaws with multislice computed tomography
and cone-beam computed tomography. La radiologia
medica, 115(4):600–611.
Caselles, V., Kimmel, R., and Sapiro, G. (1997). Geodesic
Active Contours. International Journal of Computer
Vision, 22:61–79.
Catmull, E. and Rom, R. (1974). A Class of Local Interpo-
lating Splines. Computer Aided Geometric Design -
CAGD, 74:317–326.
VISAPP 2021 - 16th International Conference on Computer Vision Theory and Applications
730

C¸ ic¸ek, O., Abdulkadir, A., Lienkamp, S., Brox, T., and Ron-
neberger, O. (2016). 3D U-Net: Learning Dense Vol-
umetric Segmentation from Sparse Annotation. In In-
ternational Conference on Medical Image Computing
and Computer-Assisted Intervention, pages 424–432.
Deng, J., Dong, W., Socher, R., Li, L.-J., Li, K., and Fei-
Fei, L. (2009). ImageNet: A Large-Scale Hierarchical
Image Database. In 2009 IEEE Conference on Com-
puter Vision and Pattern Recognition, pages 248–255.
IEEE.
Esteva, A., Kuprel, B., Novoa, R. A., Ko, J., Swetter, S. M.,
Blau, H. M., and Thrun, S. (2017). Dermatologist-
level classification of skin cancer with deep neural net-
works. Nature, 542(7639):115–118.
Geirhos, R., Rubisch, P., Michaelis, C., Bethge, M., Wich-
mann, F. A., and Brendel, W. (2018). ImageNet-
trained CNNs are biased towards texture; increasing
shape bias improves accuracy and robustness. arXiv
preprint arXiv:1811.12231.
Gil, J. Y. and Kimmel, R. (2002). Efficient Dilation, Ero-
sion, Opening,and Closing Algorithms. IEEE Trans-
actions on Pattern Analysis and Machine Intelligence,
24(12):1606–1617.
Hanssen, N., Burgielski, Z., Jansen, T., Lievin, M., Ritter,
L., von Rymon-Lipinski, B., and Keeve, E. (2004).
Nerves-level sets for interactive 3d segmentation of
nerve channels. In 2004 2nd IEEE International
Symposium on Biomedical Imaging: Nano to Macro
(IEEE Cat No. 04EX821), volume 1, pages 201–204.
Hwang, J.-J., Jung, Y.-H., Cho, B.-H., and Heo, M.-S.
(2019). An overview of deep learning in the field of
dentistry. Imaging science in dentistry, 49(1):1–7.
Jaju, P. P. and Jaju, S. P. (2014). Clinical utility of dental
cone-beam computed tomography: current perspec-
tives. Clinical, cosmetic and investigational dentistry,
6:29.
Kass, M., Witkin, A., and Terzopoulos, D. (1988). Snakes:
Active contour models. International Journal of Com-
puter Vision, 1(4):321–331.
Kondo, T., Ong, S., and Foong, K. W. (2004). Computer-
based extraction of the inferior alveolar nerve canal
in 3-D space. Computer Methods and Programs in
Biomedicine, 76(3):181–191.
Kwak, H., Kwak, E.-J., Song, J.-M., Park, H., Jung, Y.-H.,
Cho, B.-H., Hui, P., and Hwang, J. (2020). Automatic
mandibular canal detection using a deep convolutional
neural network. Scientific Reports, 10.
Li, Y., Yosinski, J., Clune, J., Lipson, H., and Hopcroft, J. E.
(2015). Convergent Learning: Do different neural net-
works learn the same representations? In Proceed-
ings of the 1st International Workshop on Feature Ex-
traction: Modern Questions and Challenges at NIPS
2015, pages 196–212.
Ligabue, G., Pollastri, F., Fontana, F., Leonelli, M., Furci,
L., Giovanella, S., Alfano, G., Cappelli, G., Testa, F.,
Bolelli, F., Grana, C., and Magistroni, R. (2020). Eval-
uation of the Classification Accuracy of the Kidney
Biopsy Direct Immunofluorescence through Convolu-
tional Neural Networks. Clinical Journal of the Amer-
ican Society of Nephrology, 15(10):1445–1454.
Loubele, M., Bogaerts, R., Van Dijck, E., Pauwels, R., Van-
heusden, S., Suetens, P., Marchal, G., Sanderink, G.,
and Jacobs, R. (2009). Comparison between effec-
tive radiation dose of CBCT and MSCT scanners for
dentomaxillofacial applications. European Journal of
Radiology, 71(3):461–468.
Ludlow, J. B. and Ivanovic, M. (2008). Comparative
dosimetry of dental CBCT devices and 64-slice CT for
oral and maxillofacial radiology. Oral Surgery, Oral
Medicine, Oral Pathology, Oral Radiology, and En-
dodontology, 106(1):106–114.
Nysj
¨
o, J. (2016). Interactive 3D Image Analysis for Cranio-
Maxillofacial Surgery Planning and Orthopedic Ap-
plications. PhD thesis, Uppsala University.
Pollastri, F., Bolelli, F., Paredes, R., and Grana, C. (2019).
Augmenting Data with GANs to Segment Melanoma
Skin Lesions. Multimedia Tools and Applications
Journal, 79(21-22):15575–15592.
Pollastri, F., Maro
˜
nas, J., Bolelli, F., Ligabue, G., Pare-
des, R., Magistroni, R., and Grana, C. (2021). Confi-
dence Calibration for Deep Renal Biopsy Immunoflu-
orescence Image Classification. In 2020 25th Interna-
tional Conference on Pattern Recognition (ICPR).
Ronneberger, O., Fischer, P., and Brox, T. (2015). U-Net:
Convolutional Networks for Biomedical Image Seg-
mentation. LNCS, 9351:234–241.
Silva, M. A. G., Wolf, U., Heinicke, F., Bumann, A., Visser,
H., and Hirsch, E. (2008). Cone-beam computed to-
mography for routine orthodontic treatment planning:
a radiation dose evaluation. American Journal of Or-
thodontics and Dentofacial Orthopedics, 133(5):640–
e1.
Sotthivirat, S. and Narkbuakaew, W. (2006). Automatic De-
tection of Inferior Alveolar Nerve Canals on CT Im-
ages. In 2006 IEEE Biomedical Circuits and Systems
Conference, pages 142–145.
Vinayahalingam, S., Xi, T., Berge, S., Maal, T., and
De Jong, G. (2019). Automated detection of third mo-
lars and mandibular nerve by deep learning. Scientific
Reports, 9.
A Cone Beam Computed Tomography Annotation Tool for Automatic Detection of the Inferior Alveolar Nerve Canal
731
