
A Survey of Possibilities and Challenges with AR/VR/MR and
Gamification Usage in Healthcare
Yu Fu
1 a
, Yan Hu
1 b
, Veronica Sundstedt
1 c
and Cecilia Fagerstr
¨
om
2 d
1
Department of Computer Science, Blekinge Institute of Technology, Karlskrona, Sweden
2
Department of Health and Caring Sciences, Linnaeus University, Kalmar, Sweden
Keywords:
Virtual Reality, Augmented Reality, Mixed Reality, Healthcare, Game, Gamification.
Abstract:
Software and applications of augmented reality (AR), virtual reality (VR), and mixed reality (MR) technol-
ogy combined with game/gamification techniques in healthcare have increasingly been studied in academia.
However, there is a need to explore the usage, challenges and opportunities of AR/VR/MR game/gamification
software/applications in the healthcare system. To explore this, we present an online survey conducted in the
healthcare-relevant system (including hospital-based system, homecare-based system, institute and university,
and industry). Based on the answers, we found examples of digital games and AR/VR/MR applications used
in healthcare, as well as some general information (name and feature, purpose, target user, and use occasion),
usage situation, and user experience. This presented survey is beneficial for both researchers and developers
in computer science and medical science. It can familiarise them with existing products and their current
use, advantages and potential issues of AR/VR/MR and game applications in healthcare. In future work,
the survey would be extended to obtain other user experiences and feedback of AR/VR/MR techniques and
game/gamification technology applied to healthcare, as well as to study how to overcome the challenges, and
develop the opportunities further.
1 INTRODUCTION
Recent research has started to focus on combining
augmented, virtual and mixed reality (AR/VR/MR)
technology with game techniques in healthcare ap-
plications. These applications have been developed
to match the requirements of healthcare issues or to
enhance traditional solutions in healthcare. This pa-
per presents a user survey with relevant staff, students,
and professionals related to the healthcare area, with
the aim to explore the possibilities and challenges
with AR/VR/MR and game/gamification applied in
healthcare. The research objectives focused on the
use, opportunities, and challenges, with AR/VR/MR
techniques and game/gamification technology.
The rest of the paper is organised as follows. Sec-
tion 1.1 describes the relevant background concepts
including VR/AR/MR and game/gamification. Then,
Section 2 illustrates the related work in both medi-
a
https://orcid.org/0000-0003-3520-3302
b
https://orcid.org/0000-0002-3283-2819
c
https://orcid.org/0000-0003-3639-9327
d
https://orcid.org/0000-0002-4257-282x
cal science and computer science. Next, Section 3
explains the aim and objectives, research questions,
and the research method, including the ethics descrip-
tion of this research, questionnaire structure and logic,
questions topic content, and pilot study. Section 4
shows the result based on 30 questionnaire answers,
including the perspective of application purpose and
target user, use time and frequency, advantages and
disadvantages, obstacles to mass adoption, and re-
quirements and concerns. Based on the results pre-
sented in Section 4, Section 5 tries to explore the
possible reasons behind the results. Finally, Section6
gives a summary of the study and highlights some rel-
evant future work.
1.1 Background
Games are not a concept only in the field of computer
science, but they are increasingly familiar and used
in other areas because they are often combined with
computer technology. A game is a system based on a
rule, which has a variable and quantifiable outcome,
with assigned different values (Lima et al., 2017). The
effort of the player will influence the result (Lima
Fu, Y., Hu, Y., Sundstedt, V. and Fagerström, C.
A Survey of Possibilities and Challenges with AR/VR/MR and Gamification Usage in Healthcare.
DOI: 10.5220/0010386207330740
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 733-740
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
733

et al., 2017). The challenge and fun in the game are
the primary motivations for people to play it. Gami-
fication is using game-design elements and principles
in non-game contexts (Deterding et al., 2011), and it
aims to bring the benefits of games to non-game con-
texts. AR systems add or remove virtual (computer-
generated) objects, which coexist in the same space
as the real world (Blusi, 2014). VR systems are dif-
ferent. They generate 3D objects by the computer,
which simulates a virtual world, and cut off users’
perception of the real world by using peripherals such
as immersion glasses and interaction devices (Okeil,
2010). MR is sometimes referred to as ’hybrid re-
ality’, and is the merging of real worlds and virtual
environments. MR provides new environments and
visualisations, where physical and digital objects can
coexist and interact in real-time (de Lima et al., 2016).
According to the immersion level, Li et al. clas-
sified AR/VR techniques into seven categories: (1)
least-immersive VR, (2) semi-immersive VR, (3) im-
mersive VR, (4) tangible AR, (5) collaborative AR,
(6) distributed VR/AR, and (7) other VR/AR (Li et al.,
2018). They claimed that technology selection leads
to different immersion and interaction and should
adapt to the application requirements (Li et al., 2018).
According to equipment, Okeil grouped VR by
two immersive levels: (1) immersive VR (using HMD
or CAVE) and (2) non-immersive VR (using screen
including laptop, computer, mobile, tablet PC, TV,
and large screen) (Okeil, 2010). Desktop-based VR
was defined as operating on a simple computer moni-
tor, controlled by mouse and keyboard, and without
tracking equipment (Wang et al., 2018). Although
desktop-based VR provided lower-level immersion,
compared with other kinds of VR techniques, the
device also has a lower cost. Immersive VR relies
on specialised hardware such as HMDs and sensor
gloves (Wang et al., 2018).
Adding sensors into the hardware made them pro-
vide real-time feedback. Because of the real-time
capabilities, Sacks and Pikas believed that immer-
sive VR is better than non-immersive VR (Sacks and
Pikas, 2013). Additionally, Wang et al. highlight that
by integrating visual and interactive multi-user oper-
ation technologies, VR training games could reduce
the complexity of task processes, thereby enhancing
user interactions (Wang et al., 2018).
2 RELATED WORK
Ma et al. summarised three keywords to the fu-
ture trends of VR/AR and game in healthcare: the
location-based exergaming, mobile apps, and social
media gaming for public health (Ma et al., 2014).
They claimed that the approach of healthcare and
medical education might be changed by the research
and development of mobile devices combined with
wearable devices over the next decade (Ma et al.,
2014). A social media effect on games in health-
care will be growing due to social games’ popular-
ity and social interactions’ effectiveness (Ma et al.,
2014). AR/VR techniques were proven effective to
some healthcare issues, as a new solution or to en-
hance the conventional solutions. Jorge et al. re-
viewed the approaches and challenges to the VR/AR
technique in healthcare and rehabilitation (Jorge et al.,
2019). In the review, they illustrated several exciting
VR/AR systems, such as VR for radiologists in the
reading room, and in the operations room, augmented
surgery, and laparoscopic, as well as exergames for
locomotion rehabilitation by VR (Jorge et al., 2019).
Perkins Coie LLP and the XR Association have
surveyed AR/VR yearly, since 2017. They inter-
viewed 200 startup founders in 2019, executives with
established technology companies, investors and con-
sultants in the AR/VR/MR related area, in the past
four years. In their new survey report in 2019 (LLP
and the XR Association, 2019), they pointed out that
90% of the respondents believed immersive technolo-
gies including AR/VR/MR would be ubiquitous like
mobile devices, by 2025.
They also claimed that the quality of user expe-
riences, available content offerings, and the pace of
adoption were the concerns and similar to the past sur-
veys’ result. For AR technology to be mass adopted,
the largest obstacle was the lower user experience,
including bulky hardware or technical glitches. The
second one was the content offerings, including the
quantity and quality of content. Similarly with the
survey results of AR technology, user experience and
offering content were the two most considerable ob-
stacles to getting VR technology to be mass adopted.
Respondents also pointed out that the most common
concern was the slow adoption among consumers.
Some respondents believed hardware should be
more user-friendly, and the cost, comfort and utility
should be addressed. However, they have still strong
confidence with them when it comes to the future
of the AR/VR/MR technologies. One of the respon-
dents said that immersive technologies could connect
further to people in an organisation, such as in doc-
tors’ offices or schools, instead of only facing indi-
vidual consumers. In their report, the game technique
again, as in their previous surveys, led the combina-
tion with AR/VR/MR applications. Not far behind
was the healthcare and medical devices.
HEALTHINF 2021 - 14th International Conference on Health Informatics
734
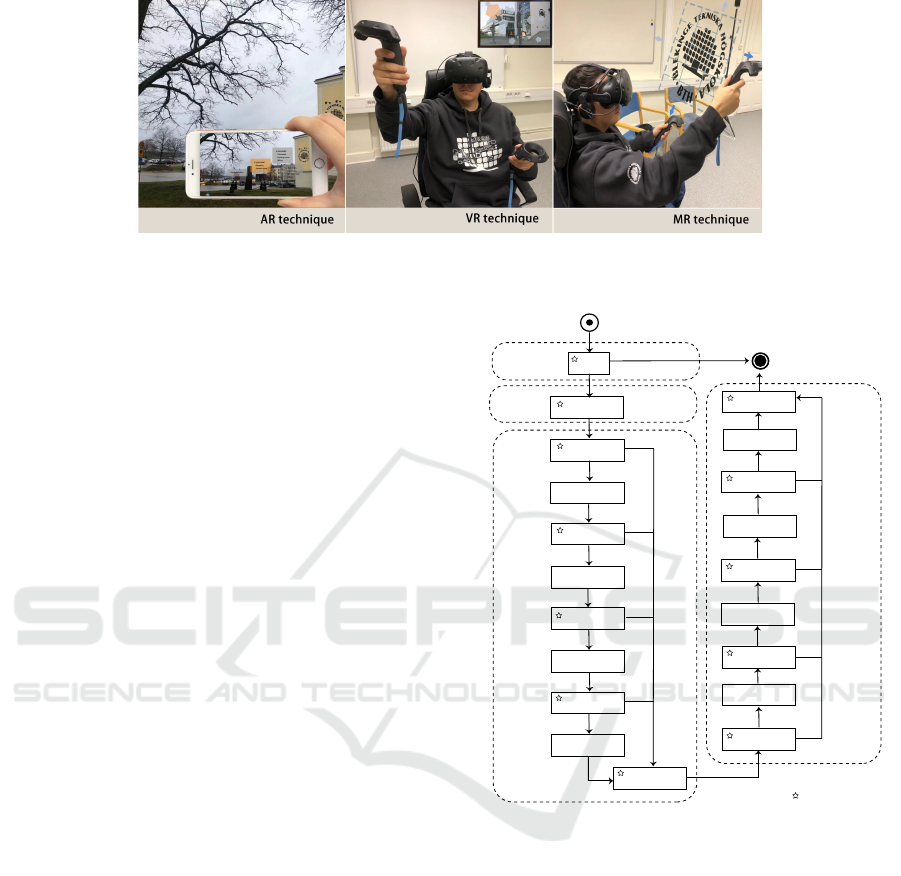
Figure 1: Example of AR/VR/MR technology.
3 METHOD
The survey used an online questionnaire to eval-
uate the usage of AR/VR/MR applications and
game/gamification technology in healthcare. The re-
search questions are shown below:
• RQ1: How can digital game/gamification and
AR/VR/MR technology be applied in healthcare?
• RQ2: What are the opportunities and challenges
of game/gamification and AR/VR/MR applica-
tions in healthcare?
The link to the questionnaire was either emailed to
target organisations, or posted on social media such
as LinkedIn and Twitter. Based on the principles of
Singer and Vinson’s practical guideline for ethical is-
sues on the conduct of empirical studies (Singer and
Vinson, 2002), and the General Data Protection Reg-
ulation (GDPR) (Voigt and Von dem Bussche, 2017),
we created a detailed ethics description of our survey
in the informed consent, and illustrated it in the invita-
tion letter, the consent form, and the beginning of the
online questionnaire. Here it was highlighted that no
sensitive data was gathered and it was all confidential.
In the questionnaire, there were three sections
with 85 questions. Out of these, 17 were required
and mandatory marked with a star. The structure
and logic of the questionnaire are shown in Fig. 2,
Except for the informed consent, the other ques-
tions included two aspects: (1) general information
and (2) topic-related questions. Before the topic-
related questions, there was an introduction to the
survey, informed consent, background concepts intro-
duced, and data collection of the respondents’ gen-
eral information (including the location, and occu-
pation and the work content of the participant). In
the topic-related questions, we tried to obtain in-
formation about the game/gamification application(s)
and AR/VR/MR application(s) in healthcare. To ad-
dress RQ1, the application(s) information questions
Yes
Yes
Yes
Yes
No
No
No
No
Yes
No
Yes
No
Yes
Yes
Yes
No
No
No
Q1
Q2-Q5
Q6
Q7-Q14
Q15
Q42-Q43
Q44
Q84-Q85
Q45-Q53
Q54
Q16-Q23
Q24
Q25-Q32
Q33
Q34-Q41
Q55-Q63
Q64
Q65-Q73
Q74
Q75-Q83
Required question
Repeat 1
Repeat 2
Repeat 3
Repeat 3
Repeat 2
Repeat 1
Part 2. Game/ gamication in general healthcare
software/applications
Part 3. Healthcare software/applications
with AR/VR/MR technology
Part 1.
Consent form
Start
End
Figure 2: The questionnaire structure and logic.
(Game/gamification part: Q7-Q14; AR/VR/MR part:
Q45 to Q53) covered application name and feature,
purpose, target user, use environment, use frequency,
use time, advantages and disadvantages, and whether
it was using a game/gamification technique (only in
Part 3). To answer RQ2, we generated questions
(Game/gamification part: Q42-Q43; AR/VR/MR
part: Q84-Q85) to better know the requirements and
obstacles to mass adoption of AR/VR/MR techniques
and game technology.
In part two and three, the questions for collect-
ing application information were repeated three times
(Game/gamification part: Q16-Q23, Q25-Q32, Q34-
41; AR/VR/MR part: Q55-Q63, Q65-73, Q75-83),
to obtain further data if the interviewee used more
than one software/application. Before each repetition,
there was a required question (Game/gamification
A Survey of Possibilities and Challenges with AR/VR/MR and Gamification Usage in Healthcare
735

25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance to
embrace game/gamifica�on technique
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance to…
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance to…
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
24
17
15
17
19
7
1
25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
24
17
15
17
19
7
1
25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
24
17
15
17
19
7
1
25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
24
17
15
17
19
7
1
25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer/business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer/business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer/business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer/business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversight
Other
Game/Gamifica�on AR/VR/MR
6
4
5
2
1
3
2
1
1
8
7
3
0 1 2 3 4 5 6 7 8 9
Doctor
Nurse
Assistant nurse
Pharmacise
Den�st
Psychologist
Physiotherapist
Therapist
Anaesthe�st
Researcher and developer
Research student
Others
6
4
5
2
1
3
2
1
1
8
7
2
0 1 2 3 4 5 6 7 8 9
Doctor
Nurse
Assistant nurse
Pharmacise
Den�st
Psychologist
Physiotherapist
Therapist
Anaesthe�st
Researcher and developer
Research student
Others
6
4
5
2
1
3
2
1
1
8
7
2
0 1 2 3 4 5 6 7 8 9
Doctor
Nurse
Assistant nurse
Pharmacist
Den�st
Psychologist
Physiotherapist
Therapist
Anaesthe�st
Researcher and developer
Research student
Others
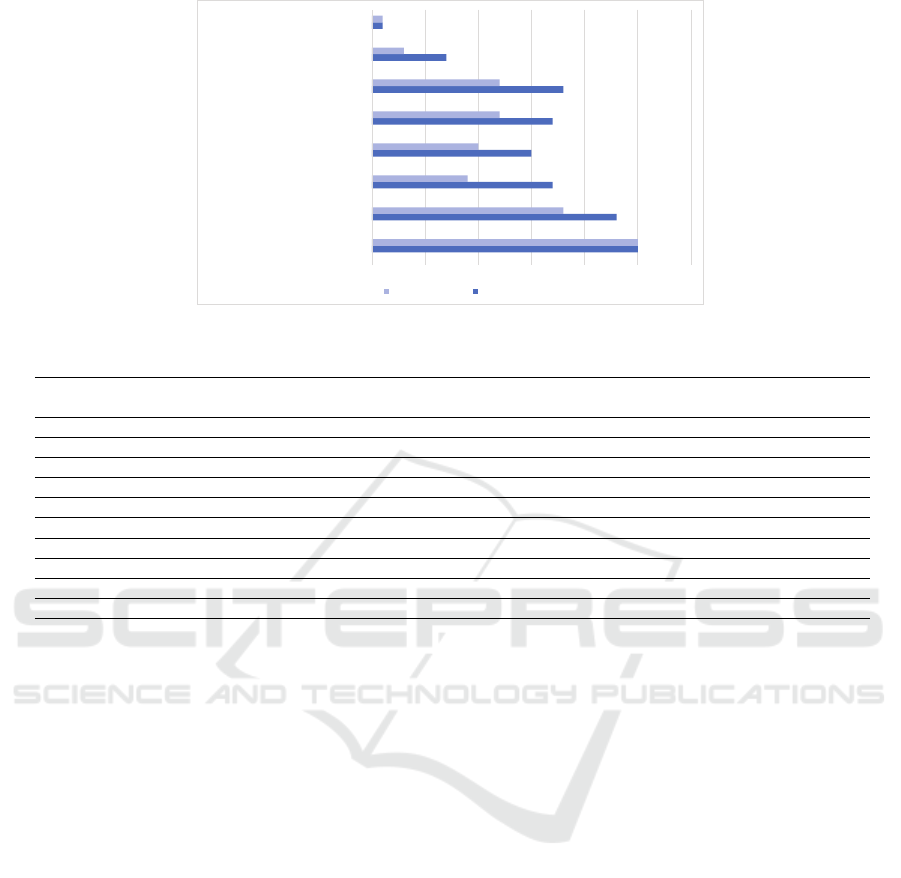
Figure 3: Participant’s position.
part: Q15, Q24, Q33; AR/VR/MR part: Q54, Q64,
Q74) to determine whether to enter the follow-up re-
peat questions at this stage or directly jump to the next
section. If the respondents did not have the user ex-
perience of another software/application, they could
skip these questions. There were instructions at the
beginning of each part, and after the questions, to re-
duce any misunderstanding.
The questions were designed as a single choice,
multiple-choice, and open questions. For the single-
choice or multiple-choice questions, we quantified the
options and performed descriptive tables to analyse
them. Before the main questionnaire survey was car-
ried out, five researchers from the internal organisa-
tion were invited to participate in a brief pilot study
to estimate the answering time, test the validity of the
questionnaire, and obtain any potential comments or
feedback on the main questionnaire.
4 RESULTS
By mid-November (2020-11-15), there were 31 an-
swers from ten countries (Sweden, Australia, China,
USA, Netherlands, Thailand, the United Kingdom,
Spain, Japan, and Germany). One answer was
excluded due to the participant position being a
babysitter (not necessarily related to the medical
background requirement). In this work, healthcare-
relevant knowledge and skill are not mandatory, de-
spite useful. Hence, this was classified to belong to
non-healthcare relevant work in the analysis. Thus,
the following analysis and results were based on 30
individual participants.
The interviewees mainly came from academia (ten
people), hospital (eight people), and primary health
care organisations (six people). As shown in Fig. 3,
the participants were working more as research stu-
dents, researchers, and developers in their organisa-
tion. Their main tasks were research and studying
in their fields, such as eHealth, information systems,
telecommunication systems, palliative care, dental
hygienists, psychological counselling, and nursing.
Classification of the doctors and nurses in the partici-
pants were various, such as being an orthopedist, pae-
diatrician, pharmacist, family doctor, as well as mid-
wife, or in elderly home care.
From the 30 answers, we found six people
having experience of game/gamification soft-
ware/applications, and 16 people had experience
with AR/VR/MR software/applications, which
involved six games, and nine AR/VR/MR soft-
ware/applications amongst them. Based on the
used techniques, these software/applications were
classified into three groups: (1) game/gamification
(without AR/VR/MR), (2) game/gamification
and AR/VR/MR, and (3) AR/VR/MR (non-
game/gamification). Table 1 shows the general
information (name and feature, purpose, target user,
and use occasion) of the software/applications.
4.1 Application Purpose and Target
User
Game/gamification and AR/VR/MR applications in
healthcare were shown to aim to deal with a variety of
health issues. Applications’ purpose were classified
as three groups with eight subgroups, for prevention
(including disease prevention, health behaviour train-
ing/health knowledge teaching, and encouraging ex-
ercise), for treatment (including mental treatment, ad-
juvant therapy, physiotherapy and rehabilitation), and
for medical education and training.
As shown in Table 1, there were 15 soft-
ware/applications mentioned in the survey answers.
The game/gamification techniques were mainly used
HEALTHINF 2021 - 14th International Conference on Health Informatics
736
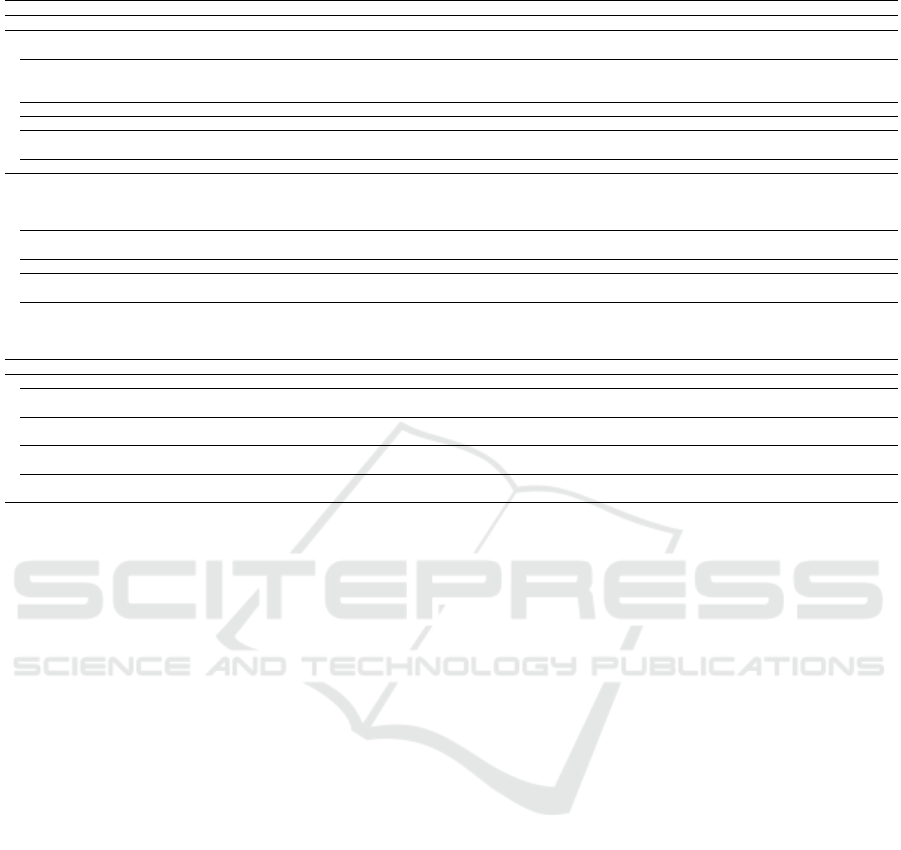
Table 1: The general information of the software/applications.
Name/feature Purpose User Occasion
Game/gamification
Digital patient meeting
Mental treatment,
Disease prevention
Hospital-based care provider,
Patient
Hospital
Null
Medical education and training,
Health behaviour training/ Health knowledge teaching,
Adjuvant therapy
Hospital-based care provider,
Home-based care provider,
Medical student
Hospital, Home,
School/University/Institute,
Outdoors
Treatment for autistic children Mental treatment, Adjuvant therapy Patient Hospital
Word puzzle Disease prevention Patient, High-risk group of certain diseases Home
HUAWEI health wrist ring
Health behaviour training/ Health knowledge teaching,
Encouraging exercise
Hospital-based care provider,
Home-based care provider
Hospital, Home, Outdoors,
School/University/Institute
Game/gamification + AR/VR/MR
”Deep”
Mental treatment,
Health behaviour training/ Health knowledge teaching
High-risk group of certain diseases,
Patient, Home-based care provider,
Hospital-based care provider,
Lecturer and Researcher, Patient
Hospital, Home,
School/University/Institute
”Stress jam”
Mental treatment,
Health behaviour training/ Health knowledge teaching
High-risk group of certain diseases,
Patient
Home,
Hospital
VR technique in simulation CPR Medical education and training Medical student School/University/Institute
VR exercise game
Encouraging exercise,
Health behaviour training/ Health knowledge teaching
High-risk group of certain diseases,
Patient
Home
The model video of operation
Mental, treatment,
Medical education and training,
Health behaviour training/ Health knowledge teaching,
Adjuvant therapy, Disease prevention
Home-based care provider,
Hospital-based care provider,
Lecturer and Researcher, Patient
Hospital, Home,
School/University/Institute
AR/VR/MR
For autism spectrum disorder treatment Mental treatment Patient Hospital
3D body map,
3D human body anatomy
Medical education and training Medical student
Home, Hospital,
School/University/Institute
Training software for X-ray imaging Medical education and training Hospital-based care provider
Hospital,
School/University/Institute
Virtual surgery,
Surgical simulation
Medical education and training Medical student
Hospital,
School/University/Institute
”MindMaze”
(stroke rehabilitation training)
Rehabilitation, Encouraging exercise
Hospital-based care provider,
Home-based care provider, Patient
Home, Hospital
Note: The ”Null” means the information was not mentioned in the participant’s answer.
in mental health treatment, and health behaviour
training/health knowledge teaching, especially com-
bined with the AR/VR/MR technology. Those two
kinds of software/applications purposes involved the
treatment of mental health problems such as autism,
stress (”Stressjam”), and anxiety (”Deep”); as well as
physical training.
Except for being used in the mental health treat-
ment and health behaviour training/health knowledge
teaching, the AR/VR/MR techniques were widely
used in medical education and training, such as in
cardiopulmonary resuscitation (CPR), surgery, and
3D body map (for medical students to study the
knowledge of human anatomy). It is worth noting
that AR/VR/MR in medical education and training
was commonly used without game/gamification tech-
niques.
Based on the purpose and features, the primary
target user of the software/applications were hospital-
based care provider and patient. They were generally
used in the hospital and home. Furthermore, the soft-
ware/applications for medical students were mainly
used in a school, university, or institute.
4.2 Use Time and Frequency
Just four participants mentioned the soft-
ware/applications use time, and two refer to the
frequency. There were four years for the HUAWEI
health wrist ring used in the interviewee’s organi-
sation and two years for the Deep and Stressjam,
as well as one year for the CPR simulation. The
HUAWEI health wrist ring used in the interviewee’s
organisation was reported to be used two hours per
week, and for Deep, it was about five hours. The
other 27 participants claimed they did not know the
use time and frequency of the software/applications
in their organisations.
4.3 Advantages and Disadvantages
From the view of advantages in game/gamification
software/applications, some participants believed
they were helpful, such as the HUAWEI health wrist
ring for users’ health, as well as autism spectrum
disorder (ASD) treatment software for ASD patients,
their families, and doctors. Moreover, an intervie-
wee said, ”game is more in line with children’s cogni-
tion and acceptance”. Another person thought game
applications provide stronger motivation than non-
game activities. On the other hand, the interviewees
mentioned the disadvantages of game/gamification
techniques as well. One of them pointed out the
cost of suitable equipment and software support be-
ing quite expensive. Two others said problems of
game/gamification could be that they might not be ap-
propriate and could be addictive.
A Survey of Possibilities and Challenges with AR/VR/MR and Gamification Usage in Healthcare
737

From the view of advantages of AR/VR/MR tech-
niques in healthcare software/applications, the partic-
ipant who mentioned the application for the model
video operation believed it is more precise, more use-
ful for the end of the operation and to get a better re-
sult. Using a CPR simulation application, one inter-
viewee claimed the application provided the ability to
change the setting for the patient/student. Moreover,
the user of the 3D body map said, it is intuitive, clear,
and easier to perceive the spatial position and rela-
tionship of various organs, bone, and blood vessels
than in books. Furthermore, interviewees mentioned
the advantage of simulation surgery was beneficial for
being able to repeat several times. For Deep, safety
was mentioned, for VR exercise game, it was the bet-
ter gaming experience, and for X-ray imaging train-
ing applications, it was also safe and infinitely repeat-
able. The disadvantages of AR/VR/MR techniques
in healthcare software/applications mainly focused on
high cost and equipment. Especially the high cost
of costumers led by over-reliance on high-tech elec-
tronic equipment, as well as problems with fluency
and low quality presented caused by data transmis-
sion delays.
4.4 Obstacles to Mass Adoption
As shown in Fig. 4, the largest obstacle of
game/gamification techniques to mass adoption was
the user experience (25), and the following three were
the main challenges: content offering (18), the cost
to consumers (12) and the financing and investment
(12) were tied for third. The first two obstacles of
the AR/VR/MR techniques to mass adoption were the
same as the game/gamification techniques: user expe-
rience (25) and content offering (23). However, the
following were different. For the AR/VR/MR tech-
niques, the cost to consumers (18) was the third ob-
stacle, and the financing and investment (17) and the
consumer and business reluctance (17) were tied as
the fourth obstacle.
4.5 Requirements and Concerns
From the 30 answers, there were ten requirements
of game/gamification and AR/VR/MR techniques in
healthcare, as shown in Table 2. The keywords can
be separated into two groups, the aim, purpose, and
target users. We can see the requirements of physi-
cal health issues, such as exercise, rehabilitation, and
muscle relaxation. Furthermore, the requirements put
more attention to psychological and mental health
problems both in treatment and training. Moreover,
medical education and training were also mentioned
in the requirements. The target user was not only or-
dinary and patients; some interviewees pointed out,
especially the requirements facing students, elderly,
children, and babies. However, the interviewees also
expressed concerns about the process of technology
realisation. Someone believed it is difficult to com-
mercialise. Another thought that AR/VR/MR tech-
niques might be too high tech for their patient groups
who are the elderly over 65 years old. Moreover, the
clinical effect could be challenging to verify.
5 DISCUSSION
Although several interviewees coming from academia
may cause many software/applications related to
medical education and training, it was undeniable
the numbers of mature software/applications used in
healthcare. Students and researchers, as their primary
target users, may lead to an easier acceptance of new
techniques. The requirements of the medical edu-
cation and training software/applications were more
straightforward and clear to analyse, such as the 3D
body map for studying the human body anatomy, and
X-ray imaging training for learning how to take X-
ray images. Thus, the design and prototype process
of such software was more comfortable to implement
and evaluate.
A safe, controlled, and a repeatable environment;
multi-angle presentation; and simulation of the real
world were the main reasons for the AR/VR/MR tech-
niques used in healthcare. The AR/VR/MR tech-
niques provided a virtual environment similar to the
real world. It is a safe and controllable environ-
ment for expensive and high-risk teaching or train-
ing. Users can consolidate knowledge and skills in
actual operations and avoid the serious consequences
of incorrect operations. However, for serious pur-
poses, the proportion of using games/gamification
techniques in this kind of software/applications is rel-
atively small. However, there is still space to combine
game/gamification techniques into medical education
and training software/applications.
Training skills in taking care of babies could
look like a ”medical education and training” soft-
ware, but for new parents instead of users with
a medical background. It was mentioned both in
the game/gamification and AR/VR/MR technique re-
quirements in healthcare. In an environment that
maintains social distancing and avoids gatherings for
safety reasons, software/applications have become a
better solution instead of face-to-face instruction.
The topic of treating psychological and mental
health problems is an account for a large proportion
HEALTHINF 2021 - 14th International Conference on Health Informatics
738
6
4
5
2
1
3
2
1
1
8
7
3
0 1 2 3 4 5 6 7 8 9
Doctor
Nurse
Assistant nurse
Pharmacise
Den�st
Psychologist
Physiotherapist
Therapist
Anaesthe�st
Researcher and developer
Research student
Others
6
4
5
2
1
3
2
1
1
8
7
2
0 1 2 3 4 5 6 7 8 9
Doctor
Nurse
Assistant nurse
Pharmacise
Den�st
Psychologist
Physiotherapist
Therapist
Anaesthe�st
Researcher and developer
Research student
Others
25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance to
embrace game/gamifica�on technique
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance to…
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance to…
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
24
17
15
17
19
7
1
25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
24
17
15
17
19
7
1
25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
24
17
15
17
19
7
1
25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
24
17
15
17
19
7
1
25
19
9
10
12
13
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer and business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer/business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer/business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer/business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversigh
Other
Game/Gamifica�on AR/VR/MR
25
23
17
15
17
18
7
1
25
18
9
10
12
12
3
1
0 5 10 15 20 25 30
User experience
Content offerings
Consumer/business reluctance
Regula�on and legal risks
Financing and investment
Cost to consumers
Government oversight
Other
Game/Gamifica�on AR/VR/MR
Figure 4: Obstacles to mass adoption of game/gamification and AR/VR/MR.
Table 2: Requirement of game/gamification and AR/VR/MR technique in healthcare software/applications.
Requirement
Game/
Gamification
AR/VR/MR
Prescribe exercise to clients •
Rehabilitation • •
Treatment of psychological and mental problems, such as phobia, PTSD, and dementia. • •
Game for the elderly health • •
Psychological diagnosis or psychotherapy, especially for the elderly and children. • •
Taking care skills training of baby • •
Memory training •
Mental relaxation and distraction • •
Teaching students •
Muscle relaxation after prolonged sitting •
of the overall, both in the results of existing software
and the requirements designed. This theme has great
demand and space for development. Similar to the
medical education and training software/applications,
the wide application of AR/VR/MR techniques in
such software mainly lies in being safe and control-
lable. Virtual objects provide a safe and controllable
treatment environment for doctors. They can influ-
ence the mental state of users through the tasks they
are designed to provide treatment or relief, such as
Deep and Stressjam. Games or gamification tech-
niques could bring fun and motivation in the treat-
ment, promoting usage time and effect. As mentioned
by one interviewee, the gamification interaction was
more friendly to children’s cognitive level. In gami-
fied tasks, they were easier to understand and accept
in the software/application. This could also apply to
users with cognitive impairments.
As the problem of population ageing on a
global scale becomes increasingly serious, the health
problems of the elderly are receiving more atten-
tion. This is also confirmed from the results of
the requirements in healthcare. Many interviewees
mentioned game/gamification and AR/VR/MR soft-
ware/applications requirements for elderly healthcare.
Although the sample size of the total intervie-
wees and each job position could be more extensive,
the above results, show some usage and development
trends of game/gamification and AR/VR/MR tech-
niques in healthcare. Similar to the results in the
related work, we can see the software/applications
aimed at location-based exergaming and rehabilita-
tion. It can also be seen that the AR/VR/MR tech-
niques can be effective in some healthcare issues. On
the other hand, the result of obstacles to mass adop-
tion was similar to the related work as well. The
user experience and content should be the most cru-
cial quality indexes to consider. The usefulness of the
software as the solution in healthcare and the accept-
ability of using AR/VR/MR were essential as well.
Including medical experts and target users in the de-
velopment and evaluation may help to solve this issue.
Moreover, the customer cost (hardware and software)
should balance with the user experience and effects.
6 CONCLUSIONS
This paper has presented an online survey, based on
30 participants, exploring the possibilities and chal-
lenges with AR/VR/MR and game/gamification usage
in healthcare. The participants believed these tech-
niques were helpful for some health issues due to the
A Survey of Possibilities and Challenges with AR/VR/MR and Gamification Usage in Healthcare
739

acceptance and motivation in game/gamification; as
well as the safety, repeatability, and potential for an
improved experience in AR/VR/MR. However, the
seen challenges were relating to cost and equipment.
There were some requirements of game/gamification
and AR/VR/MR in healthcare software/applications,
such as in mental and psychological treatment, el-
derly health, and skills training in caretaking. The
interviewees also pointed out the worries of the tech-
niques and obstacles to mass adoption. Although the
sample size was limited, a conclusion was still ob-
tained, that game/gamification and AR/VR/MR have
been accepted and applied in healthcare, as well as
highlighting further development space of software
and hardware. These insights are useful for both re-
searchers and developers to know the state and devel-
opment trends of game/gamification and AR/VR/MR
in healthcare. Future work will extend the survey to
a larger sample size, in several countries, to obtain
more universal results.
REFERENCES
Blusi, M. (2014). E-health and information-and communi-
cation technology (ICT) as support systems for older
family caregivers in rural areas. PhD thesis, Mittuni-
versitetet.
de Lima, R. M., de Medeiros Santos, A., Neto, F. M. M.,
de Sousa Neto, A. F., Le
˜
ao, F. C. P., de Macedo, F. T.,
and de Paula Canuto, A. M. (2016). A 3d serious game
for medical students training in clinical cases. In 2016
ieee international conference on serious games and
applications for health (segah), pages 1–9. IEEE.
Deterding, S., Dixon, D., Khaled, R., and Nacke, L. (2011).
From game design elements to gamefulness: defin-
ing” gamification”. In Proceedings of the 15th inter-
national academic MindTrek conference: Envisioning
future media environments, pages 9–15.
Jorge, J., Campos, P., and Lopes, D. S. (2019). Approaches
and challenges to virtual and augmented reality in
health care and rehabilitation. In SIGGRAPH Asia
2020 Courses, pages 1–90.
Li, X., Yi, W., Chi, H.-L., Wang, X., and Chan, A. P.
(2018). A critical review of virtual and augmented
reality (vr/ar) applications in construction safety. Au-
tomation in Construction, 86:150–162.
Lima, T., Barbosa, B., Niquini, C., Ara
´
ujo, C., and Lana,
R. (2017). Playing against dengue design and devel-
opment of a serious game to help tackling dengue. In
2017 IEEE 5th International Conference on Serious
Games and Applications for Health (SeGAH), pages
1–8. IEEE.
LLP, P. C. and the XR Association (2019). 2019 augmented
and virtual reality survey report.
Ma, M., Jain, L. C., and Anderson, P. (2014). Future trends
of virtual, augmented reality, and games for health.
In Virtual, augmented reality and serious games for
healthcare 1, pages 1–6. Springer.
Okeil, A. (2010). Hybrid design environments: immer-
sive and non-immersive architectural design. Journal
of Information Technology in Construction (ITcon),
15(16):202–216.
Sacks, R. and Pikas, E. (2013). Building information mod-
eling education for construction engineering and man-
agement. i: Industry requirements, state of the art, and
gap analysis. Journal of Construction Engineering
and Management, 139(11):04013016.
Singer, J. and Vinson, N. G. (2002). Ethical issues in em-
pirical studies of software engineering. IEEE Trans-
actions on Software Engineering, 28(12):1171–1180.
Voigt, P. and Von dem Bussche, A. (2017). The eu general
data protection regulation (gdpr). A Practical Guide,
1st Ed., Cham: Springer International Publishing.
Wang, P., Wu, P., Wang, J., Chi, H.-L., and Wang, X.
(2018). A critical review of the use of virtual real-
ity in construction engineering education and training.
International journal of environmental research and
public health, 15(6):1204.
HEALTHINF 2021 - 14th International Conference on Health Informatics
740
