
WoundArch: A Hybrid Architecture System for Segmentation and
Classification of Chronic Wounds
Carlos Diego F. da Rocha
1a
Bruno M. Carvalho
1b
, Vítor G. Marques
2c
and Bruno S. Silva
3d
1
Informatics and Applied Mathematics Dept., Fed. Univ. of Rio Grande do Norte, Natal, Brazil
2
Informatics Institute, Fed. Univ. of Rio Grande do Sul, Porto Alegre, Brazil
3
Digital Metropolis Institute, Fed. Univ. of Rio Grande do Norte, Natal, Brazil
Keywords: Chronic Wounds, Devices Furniture, Watershed, Image Processing.
Abstract: Every year, millions of people are affected by wounds worldwide. The wound treatment process is costly and
requires the nurse to perform activities during patient care: tissue classification and calculation of the wound
area. Thus, this work proposes to build a hybrid computer system with two configurations to support wound
care. The first configuration uses a smartphone to perform the capture, segmentation and classification of the
wound images. The other configuration has a client-server architecture, the images are captured and segmented
in the application and sent, via the internet, to the web server, which is responsible for classifying the tissue
of the wounds. The proposed methodology is the segmentation of images using the watershed algorithm and
classification of tissues in Necrosis, Granulation or Crushing. fulfilled. To evaluate the application,
experiments were performed with 20 images of wounds and the system was evaluated in two architectures:
client and client-server. The results show that the client-server reached accelerations of up to 3.2 times in
relation to the client-only architecture. The client-server architecture also saves energy and space in the client
units, increasing the uptime of smartphones, in addition to reducing the storage load of the same.
1 INTRODUCTION
A wound is an interruption in the continuity of tis- sues
by external mechanical force by physical force, but
also damage by heat, cold, chemicals, electricity and
radiation (Pounder, 1969). Wounds can be clas- sified,
according to tissue repair time, in acute and chronic
(Whitney, 2005). Acute wounds are those that heal in
a timely manner and without complications, while
chronic wounds take longer to heal due to their
extension and severity, and usually present
inflammation in the wound tissues (Clark, 2014). The
causes for their existence are usually associated with
pre- existing diseases (comorbidities), such as
diabetes and venous insufficiency, for example, and
complications such as infections that hinder the
healing process. Wound is a worldwide health
problem and affects a large number of people,
compromising their quality of life. According to Sen
a
https://orcid.org/0000-0003-4018-664X
b
https://orcid.org/0000-0002-9122-0257
c
https://orcid.org/0000-0000-0000-0000
d
https://orcid.org/0000-0002-7689-8000
et al. (Sen et al., 2009), annually, in the United States
alone, as chronic wounds affect 6.5 million patients,
generating an estimated expenditure of U$ 25 billion
annually in the treatment of chronic wounds; In the
Netherlands, annual costs for pressure ulcer
treatments range from U$ 362 mil- lion to U$ 2.8
billion, representing 1% of the Nether- lands budget
(Brem and Lyder, 2004). These figures indicate the
magnitude of the problem with significant
socioeconomic repercussions. Chronic wound
treatment incur into high costs for health services and
the patient, especially when referring to chronic
wounds due to increased prolongation of treatment
(Nussbaum et al., 2018).
The nursing process (Garcia and Nóbrega, 2009)
guides the performance of these health professionals
through steps that should be developed during patient
care, namely: collection of nursing data, nursing
diagnosis, nursing planning, implementation and
F. da Rocha, C., Carvalho, B., Marques, V. and Silva, B.
WoundArch: A Hybrid Architecture System for Segmentation and Classification of Chronic Wounds.
DOI: 10.5220/0010341406510658
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 651-658
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
651
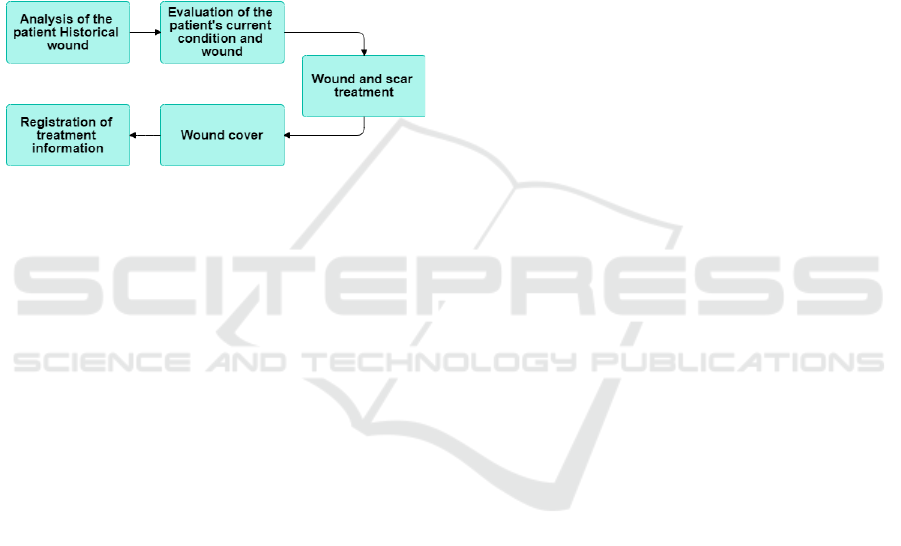
evaluation. In the context of wound treatment
(Kordestani, 2019), this process can be specialized as
follows: the professional begins analyzing the
patient’s health history, wound history and previously
performed treatments; then it analyzes the current
state of patient health conditions and wound
conditions (tissue types, size, location, etc.) to make a
diagnosis. Subsequently, the professional performs
wound and scar treatment, possibly with debridement,
cleaning, med- ication (or equivalent intervention) and
maintenance of moist tissue. Finally, the nurse
performs the procedure of the coverage necessary for
the wound and records the information about the
treatment (Figure 1).
Figure 1: Steps of the nursing process.
In the context of wound treatment, one of the
fundamental steps to arrive at a diagnosis is the
identification of characteristics of the lesions, such as:
the causal agent, the depth, the shape, the size, the
amount of exudate, the location, the appearance and
treatment environment (Dealey, 2008). Also
according to the author, the objective of the
evaluation is to extract information about the stage of
the wound and, consequently, its follow-up based on
the organism’s response to the treatment being
performed. The correct identification of these
variables is highly dependent on the professional’s
expertise. In this way, it is based on the individual
ability to visually assess how injuries have been
shown to be susceptible to errors.
In this context, in order to reduce human
limitations, computer systems have received great
attention as a work tool in the health area, mainly for
the power of information processing, for the ability to
work with a large volume of information and for the
convergence between media and devices. This type of
sup- port provides greater precision and agility at
work, helps, personalizes and expands the activities to
be performed by health professionals (Tibes et al.,
2015). In the literature, it is possible to find some
studies that present proposals for informational
systems that sup- port wound care.
Different scientific studies have been developed
focusing on the use of smartphone-web server plat-
forms in nursing diagnoses in patients with wounds.
Wallis et al. (Wallis et al., 2016) shows the use of a
mobile application that captures images of wounds
due to burns and sends them to the server so that
doctors can evaluate and make the diagnosis. Sir-
azitdinova and Deserno (Sirazitdinova and Deserno,
2017) describe a wound assessment system that uses
a smartphone device to capture images and a server
that processes, stores and reconstructs wounds in 3D
models.
In this work, we propose the use of a client-server
application to perform a necessary need for chronic
wounds, a classification of their tissues in splinter-
ing, granulation and necrosis. The construction app
will allow not only to support wound assessment, but
also offer a tool that will help prevent complications
that can result in early amputations. In addition to
facilitating the work of nurses in the classification of
wound tissues and presenting the data regarding the
injury in an appropriate way. Nursing professionals
increasingly have mobile devices that allow them to
capture images of wounds. Thus, knowing and im-
proving the efficiency of processing wound images on
mobile devices is essential for scientific knowl- edge
to reach the market and make sense in the reality of
nursing professionals. The literature still lacks re-
search that evaluates the execution time and battery
consumption of wound segmentation and classifica-
tion systems on mobile devices.
2 RELATED WORK
During the development of this project, several
systems that have similar objectives to those proposed
in the work were studied. At this stage, some of the
systems found in the literature will be described,
pointing their practical motivations and their respec-
tive limitations. In particular, we consider the works
of (Cohen and Bard, 2015), (DigitalMedLab, 2019),
(Ciancio et al., 2016) and (Friesen et al., 2016). We
also searched the literature for studies that evalu- ated
the efficiency of computer systems in supporting
wound treatment. Three nursing studies were found
that assessed efficiency and other aspects of quality of
systems aimed at end users: (Sperandio, 2008), (Tibes
et al., 2015) and (Oliveira and Peres, 2015).
Cohen and Bard (Cohen and Bard, 2015) describe
a mobile application developed at the Worcester Poly-
technic Institute, called Sugar, to help people with
diabetes manage their blood sugar level and the state
of chronic foot ulcers. The app is available only for
Android smartphones and communicates via wire- less
internet to the patient’s glucose meter in order to track
blood sugar levels and weight. The app uses the
device’s camera to capture and analyze images of
HEALTHINF 2021 - 14th International Conference on Health Informatics
652

chronic foot injuries. It tracks the wound area and
healing state and then reports the information in an
easy format for patients. The app can be used only to
analyze injuries in the foot region.
DigitalMediaLab developed WoundDesk
(DigitalMedLab, 2019), a mobile solution for wound
management, which, according to them, saves 60% of
documentation time, medical errors and increased
wound healing improvement. The application has
wound evaluation features, automated analysis, semi-
automatic and sterile wound measurement, and
documents patient information. The app is available
for both Android and IOs for free. The calculation of
the area is semi-automatic, as you need to place a ruler
next to the wound so that the processing algorithm
can calculate a coarse estimation of the PU area. This
can lead to risks of wound contamination.
In Friesen (Friesen et al., 2016), the development
of the SmartWoundCare app is described, designed to
document and evaluate chronic wounds through An-
droid and iOS smartphones and tablets. The
application uses the Braden scale to predict the risks
of wounds, evaluates and stores all patient
information on the device in a standalone mode,
without the patient’s registration function. In
addition, the application does not analyze the area of
the lesion and does not generate a report of the data
collected from patients.
Ciancio et al. (Ciancio et al., 2016) describes the
MOWA - Mobile Wound Analyzer app. The applica-
tion performs the identification of the existing tissues
in a wound from the capture of an image of the site.
With this, it provides a list of care suggestions. Like
WoundDesk, MOWA calculates the area of the lesion
with the aid of a ruler, making the procedure
vulnerable to contamination of the region and it can
produce bad estimations. Because it is an app without
new up- dates its interface is to be desired and is
probably no longer compatible with some versions of
Android and IOs systems.
In Oliveira (Oliveira and Peres, 2015), the study
aims to evaluate the functional performance and tech-
nical quality of the Electronic Documentation System
of the Nursing Process at the University Hospital of
the University of São Paulo, called PROCEnf-USP.
The evaluation was based on the Quality Model of the
standard 25010 and the Evaluation Process de- fined
in standard 25040 and used the following parameters:
functional suitability, reliability, usability,
performance efficiency, compatibility, security,
maintainability and portability.
In Sperandio (Sperandio, 2008), the research
sought to assess the functional performance and
technical quality of the prototype software developed
for nursing assistants. The software developed for
mobile devices with integrated wireless network
interface, al- lows nurses to access information and
document data about patients at the bedside. Said
author used the Evaluation Process Model provided in
the ISO / 9126
standard, which deals with the external and
internal quality of the software. This model uses six
quality evaluation parameters, namely: functionality,
reliability, usability, efficiency, maintainability and
portability. However, in his study, the evaluation of
the quality attributes of the prototype software was
based on usability and efficiency.
In Tibes (Tibes et al., 2015), the UpCare applica-
tion was evaluated by a committee of computer spe-
cialists and nursing specialists. The evaluation was
based on aspects of functionality, reliability, usabil-
ity, efficiency, maintainability and portability. For
this, two questionnaires were developed, based on the
study by (SPERANDIO, 2008), which evaluate these
aspects.
Although it is possible to find studies that have
evaluated the efficiency of in supporting the treatment
of wounds, there is a lack in the literature regarding
regarding works that address battery consumption and
run time of image segmentation and classification al-
gorithms in classification systems of wounds. The pa-
pers did not address wound segmentation and classi-
fication algorithms, and did not analyze consumption
battery life of the proposed systems.
3 WoundArch ARCHITECTURE
The present system follows the client-server ar-
chitecture shown in Figure 2, where the client uses its
mobile device to capture and segment the image of the
wound, while the server is responsible for the
classification of the tissues and the computation of the
tissues’ areas.
In this work, we built on the work proposed by
Godeiro et al. (Godeiro et al., 2018), which per- forms
the segmentation and classification of chronic
wounds. Figure 3 describes the steps performed for
the execution of the segmentation and classification
steps, which we will describe shortly.
3.1 Image Acquisition
At this stage, a specific protocol is defined for captur-
ing the images by using the mobile device, in order to
avoid the presence of noise as well as the presence of
other parts of the human body that may interfere with
the image preprocessing process. In addition, the
WoundArch: A Hybrid Architecture System for Segmentation and Classification of Chronic Wounds
653
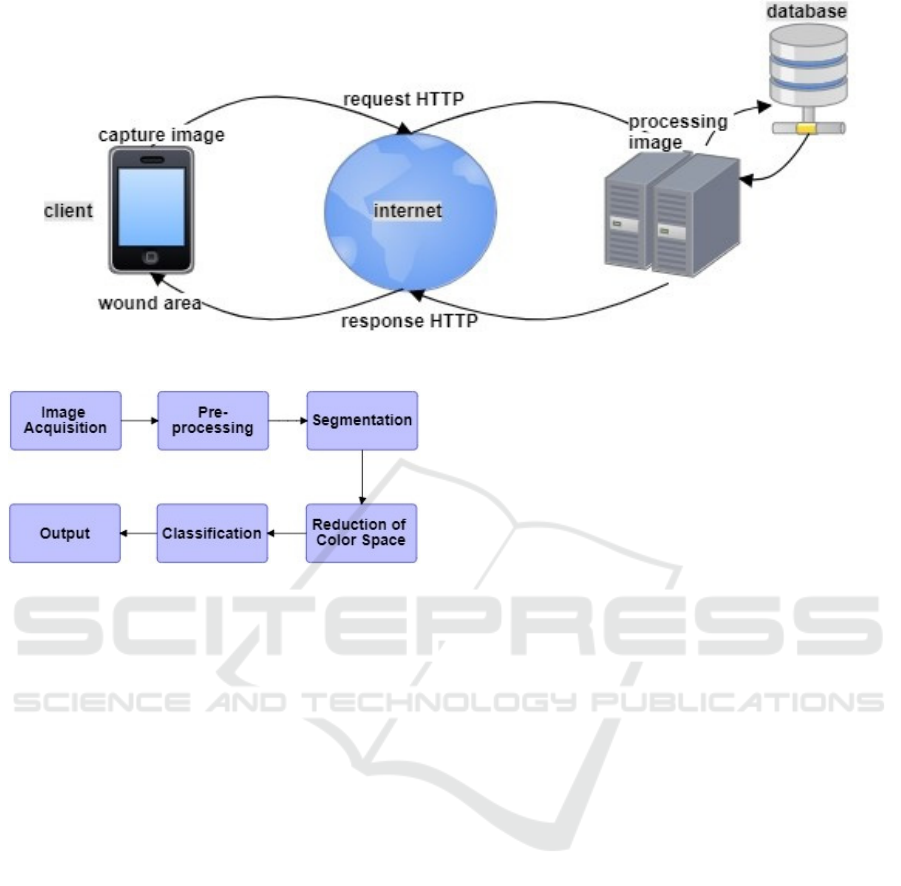
Figure 2: Client-server architecture.
Figure 3: System flow chart.
following protocol aims to ensure equal lighting
conditions for all photos taken. Godeiro (Godeiro,
2018) defined the following acquisition protocol:
1.
Take the photo at a distance between 30cm and
40cm from the wound;
2.
Take the photo with a white or blue background
to avoid adding unwanted objects in the
background (e.g. parts of the human body or
other object other than the wound);
3.
Take the photo without flash to avoid adding
extra brightness to the image;
4.
When taking the photo, place an object with a
known size in the image, at the same depth of the
wound, to retrieve the scale of the pixels;
5.
When taking the photo, use white lighting to
avoid variations in image colors;
6.
When taking the photo, make sure that the entire
wound is equally illuminated to avoid shadows
in the image.
3.2 Preprocessing
With the photo of the wound acquired, the applica-
tion performs a color conversion of the RGB image
to the HSV color system. The HSV model is used
when it is necessary to identify colors very similar to
other colors (Cardani, 2001). Unlike the RGB color
system, whose color determinants are all parameters
(red, green and blue), in the HSV model the color
determinant is the hue. In our tool, the H and S
components are used to detect skin color and remove
the parts of the image that do not contain skin or
wound. Then, the result obtained is converted from
the HSV to the RGB color system.
3.3 Segmentation
At this stage, the objective is to identify the region
of interest of the image so that the algorithm can
eliminate the regency where there is no presence of
lessions on the skin. For this, the Watershed
segmentation method (Meyer, 1992) is used in the
application. This region-based segmentation method
delivers results with closed and well-defined
contours, which is great importance to the image
segmentation process.
This is a semi-automatic process, that receives
user markings on the smartphone screen as an in- put
to the segmentation method. This process is also
used so the user can isolate a wound for processing,
in the cases where more than one wound is present
in the same picture.
3.4 Spatial Color Reduction
In the last step on the client side, a color reduction of
the image is performed. First, each RGB color com-
ponent of each pixel is quantized using 6 bits by divid-
ing its value by 4. With this reduction, the histogram
size changes from 256
3
possible colors to 64
3
possible
colors. After this, the image in the RGB format is
converted to the CIELab color space because it was
designed to approximate the human vision, as a
perceptually uniform model, i.e., the distance between
colors in this space are approximately proportional to
the color distances perceived by humans. Then, the
HEALTHINF 2021 - 14th International Conference on Health Informatics
654

frequency of colors in the histogram is computed and
those with at least 0.05% instances are stored in a list
of representative colors. The colors of the image are
analyzed and those that were not saved in the list, i.e.,
not labeled as representatives, will be mapped into the
closest color based on the Euclidean distance in the
CIELab space.
After this color space reduction, the image is ready
for the classification step, that can be performed
locally or remotely by a server through HTTP re-
quests that manage and forward the image data so that
it can be processed. The choice of the model used for
processing, being processed completely on the client
side, or divided between the client and server depends
on smartphone capabilities such as processing power
and available storage, as well as network bandwidth
and also security issues related to the available wire-
less networks.
3.5 Classification
Upon receiving the image, the server is responsible for
classifying the tissues present in the wound as
Necrosis, Granulation, or Slough. For this, a
clustering is carried out by computing the Earth
Mover’s Distance (EMD) (Rubner et al., 2000). This
distance measures the difference between signatures
that are compact distribution representations by
comparing two histograms and verifying how
different these histograms are.
In order to do that, a set of 30 wound images was
used to serve as a training base. During the training
phase, we used patches 11 × 11, a size determined
empirically (Godeiro et al., 2018), and used the EMD
to retain only patches which were at a reasonable
distance from the other retained patches. We also use
an heuristic to reduce the number of patches per class
that are used for comparisons in the classification, by
keeping only the patches which have larger sum of
distances from the other patches of the class. By
doing this, we select only the more external elements
of the cluster representing a class, i.e., the patches the
define the external borders of the clusters.
Each patch of the analyzed image is compared by
EMD with the entire set of patches retained in the
training step. The tissue label associated with a pixel
is defined by the smaller distance, computed using the
EMD, between the patch centered at it and the
training set patches.
4 EXPERIMENTS
All the experiments performed here were developed
on a notebook equipped with an Intel Core i5
Processor (6th Generation) Model 6200U with 2
cores running at 2.3GHz, with 3MB of cache, 12GB
DDR3L 1600 MHz RAM and running Linux Mint
19.3.
For the development of the server, the PHP
language Version 7.2 was used, along with the web
text editor PHPStorm 2019.3.4. The Laravel
Framework for Web Artisans 6.0 was used in
conjunction with the dependency manager Composer
1.10.1. For the computer vision stage, the OpenCV
4.1 library with C++ was used. For the development
and emulation of the client, we used the Kotlin
Language 1.3. The client used to perform the tests was
the Redmi Note 8 Smartphone equipped with a
Qualcomm SDM665 Snapdragon 665, an Octa-core
(4 ×2.0 GHz Kryo 260 Gold & 4x 1.8 GHz Kryo 260
Silver) CPU, an Adreno 610 GPU, and 64GB of
storage and 4GB RAM. This smartphone has a
Quadruple Camera: 48 MP, f/1.8, (wide), 1/2”, 0.8µm,
PDAF + 8 MP, f/2.2, 13mm (ultrawide), 1/4”, 1.12µm
+ 2 MP, f/2.4, 1/5”, 1.75µm (dedicated macro camera)
+ 2 MP, f/2.4, 1/5”, 1.75µm, depth sensor; 6.3 inches;
with a maximum resolution of 1080 × 2340 pixels.
In this section, the prototype of the application is
described (see Figure 4). The application interface is
very lean and objective so that the nurse can ob- tain
the wound information with a few touches on the
screen. When opening the app, the nurse attaches the
image of the wound, either by a photo captured at that
moment or by an image from the gallery of the smart-
phone. The patient’s name is then filled in and then
the image is uploaded to the server or processed
locally.
5 RESULTS AND DISCUSSION
For the purpose of validation of the client-server
system, a base with 20 images of wounds was used.
Table 1 presents the results obtained by the system
divided into two scenarios: segmentation and
classification in the client architecture; and
segmentation on the client with classification of the
wound on the server. In order to verify the efficiency
between client and client-server, the execution times
measured in sec- onds were compared. Each image
was executed five times for each scenario. The
Segmentation, Classification, and Total columns
show the average times and standard deviation
obtained. Even though the images are ordered by their
total number of pixels, we can see that the second
smallest image, 650 × 375, has the third highest
execution average, 9.718 seconds, a circumstance that
is related to the size of the wound area being analyzed.
WoundArch: A Hybrid Architecture System for Segmentation and Classification of Chronic Wounds
655
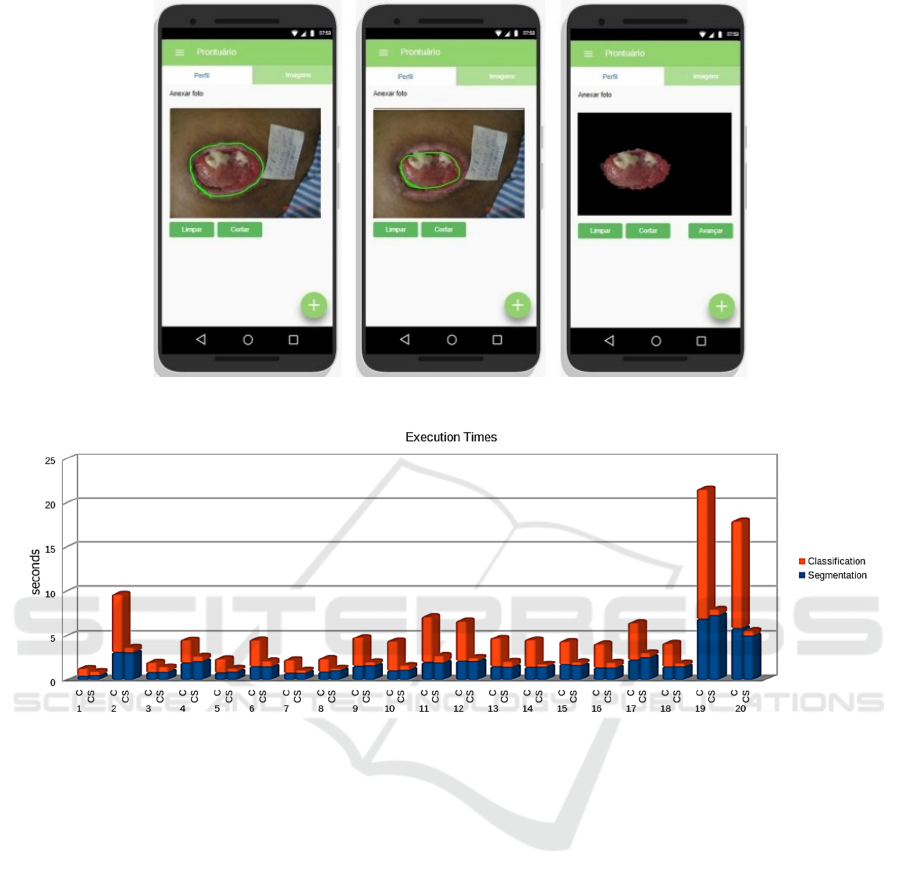
Figure 4: Example of the mobile application screen: processing seen on the client’s App.
Figure 5: Execution times required for the segmentation (blue) and classification (red) tasks. The bars labelled C correspond
to the execution times when both tasks were performed on the client side, while the label CS indicates that the classification
task was performed on the server side.
In the client-only application, when analyzing the
results of segmentation and classification, we can see
that the classification time is roughly twice as long as
the segmentation time. In classification, the vast ma-
jority of the results were below 10 seconds, only im-
ages 19 and 20 were classified on 21.584 and 17.990
seconds, respectively.
In the client-server application, due to the
segmentation continuing to be performed on the
client, the values showed little variations in relation to
the exe- cution time of the client application, that can
be ex- plained by different computational loads being
exe- cuted on the smartphone. In the classification
column, Images 19 and 20 achieved the largest time
reduction compared to the client application, from
14.69 sec- onds to 0.70 and 12.18 to 0.55, respectively.
Actually, all classifications in the server were
performed in un- der a second, including the
transmission time of the files in both directions.
The graph in Figure 5 shows the execution times
for the two options of the proposed architecture,
where the blue bars represent the segmentation time
and the red bars represent the classification times. An-
alyzing the columns, it can be noted that the longest
execution time was the one for Image 19 performed in
the client application, with more than 21 seconds,
while it took 8.01 seconds for the client-server
architecture, followed by Image 20, with 17.99
seconds for the client application, and 5.57 seconds
for the client- server.
A similar pattern can be observed for Images 2,
11, 12 and 17. The speedups obtained by the usage of
the client-server architecture in relation to the client-
only varied from 1.35 to 3.23 times. Therefore, it can
be easily observed on Table 1 and Figure 5 that the
Client-Server architecture proposed is advantageous
when compared to a standalone, or as it is called here,
client-only architecture for solving this problem.
HEALTHINF 2021 - 14th International Conference on Health Informatics
656
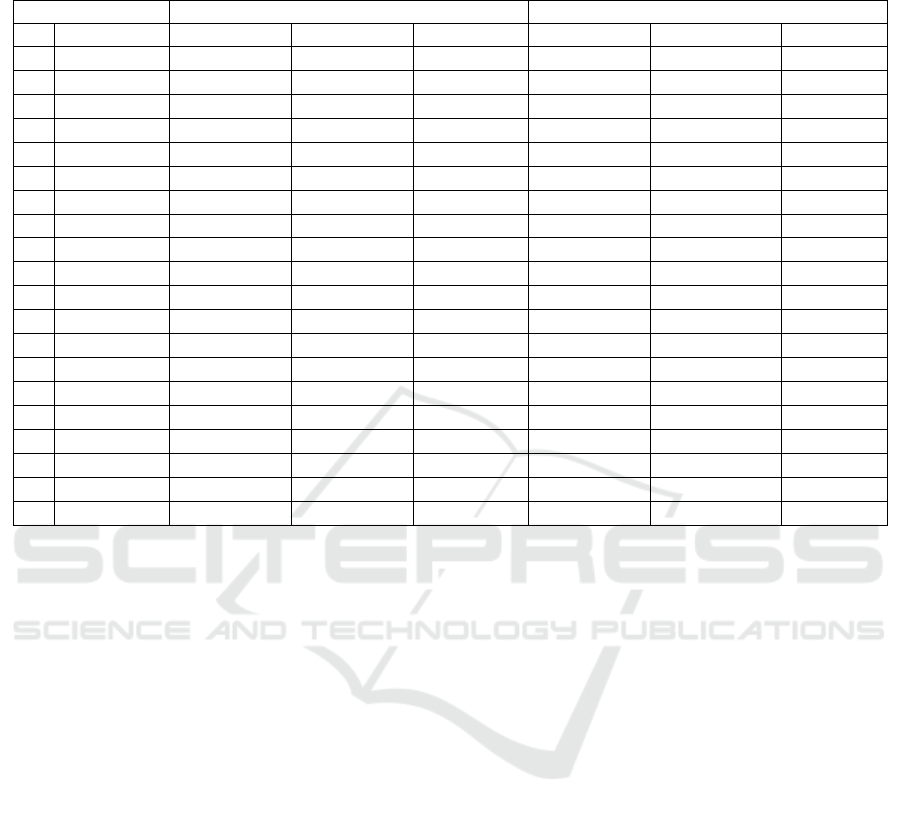
Table 1: Execution times (in seconds) for the segmentation and classification. The Classification* times reported for the
Client-Server system includes the transmission times of the segmented image to the server and the classification map back to
the client.
Image Client Client‐Server
N
Size Segmentation Classification Total Segmentation Classification* Total
1
500× 435 0.45± 0.84 0.84± 0.21 1.29± 0.20 0.51± 0.04 0.45± 0.44 0.96± 0.46
2
65× 375 3.10± 0. 22 6.62± 0.03 9.72± 0.21 3.07± 0.19 0.62± 0.30 3.69± 0.35
3
800× 500 0.84± 1.17 1.17± 0.09 2.01± 0.19 0.88± 0.06 0.60± 0.52 1.48± 0.58
4
900× 700 1.95± 0.34 2.58± 0.32 4.53± 0.66 2.10± 0.26 0.57± 0.44 2.67± 0.44
5
1000× 667 0.82± 0.09 1.58± 0.07 2.40± 0.15 0.91± 0.12 0.40± 0.35 1.31± 0.40
6
1000× 669 1.50± 0.18 3.05± 0.04 4.54± 0.21 1.47± 0.04 0.69± 0.40 2.16± 0.43
7
1024× 703 0.78± 0.04 1.50± 0.06 2.28± 0.09 0.80± 0.05 0.29± 0.09 1.10± 0.14
8
1024× 768 0.89± 0.03 1.52± 0.05 2.41± 0.06 1.06± 0.10 0.24± 0.06 1.30± 0.14
9
1102× 575 1.54± 0.18 3.27± 0.40 4.81± 0.57 1.61± 0.02 0.45± 0.27 2.05± 0.28
10
1111× 640 1.03± 0.10 3.38± 0.23 4.41± 0.30 1.10± 0.07 0.54± 0.39 1.64± 0.39
11
999× 1228 2.00± 0.23 5.15± 0.11 7.16± 0.33 1.94± 0.07 0.80± 0.55 2.74± 0.54
12
1280× 960 2.15± 0.28 4.54± 0.21 6.69± 0.34 2.12± 0.10 0.40± 0.07 2.52± 0.07
13
1333× 885 1.49± 0.05 3.24± 0.05 4.73± 0.09 1.43± 0.09 0.69± 0.46 2.13± 0.49
14
1400× 931 1.42± 0.03 3.13± 0.03 4.55± 0.09 1.47± 0.08 0.32± 0.11 1.79± 0.15
15
1460× 980 1.75± 0.13 2.59± 0.02 4.34± 0.14 1.64± 0.05 0.40± 0.23 2.04± 0.26
16
1600× 800 1.35± 0.08 2.73± 0.01 4.08± 0.08 1.35± 0.15 0.65± 0.40 2.00± 0.48
17
1637× 1255 2.26± 0. 13 4.23± 0.03 6.50± 0.16 2.55± 0.14 0.53± 0.40 3.07± 0.40
18
1850× 870 1.46± 0.02 2.69± 0.04 4.15± 0.05 1.48± 0.06 0.44± 0.42 1.92± 0.44
19
1505× 1852 6.90± 0. 50 14.69± 0.29 21.58± 0.23 7.31± 0.28 0.70± 0.13 8.01± 0.22
20
2048× 1536 5.81± 0. 45 12.18± 0.37 17.99± 0.66 5.01± 0.09 0.55± 0.15 5.57± 0.21
Moreover, the usage of the proposed client-server
architecture allows the system to keep synchronized
by saving the processed images and generating and
storing reports about the wound treatment evolution.
One can also point out to the fact that the computer
used as a server is far from being a high end PC, and
so, the usage of a more powerful computer can offer
much higher throughputs.
6 CONCLUSIONS
Mobile apps have proven to be important tools with
great potential for benefits for health activities. In this
work, we propose a mobile application for fol- lowing
the treatment of chronic wounds. This task is achieved
by performed the segmentation and classification of
chronic wound tissues and keeping track of the
treatment evolution. The main objective is to pro- vide
health professionals with a tool capable of accu-rately
classify the areas of these lesions occupied by slough,
granulation and necrosis tissues.
In order to validate the work, we performed exper-
iments with the segmentation and classification tasks
organized into a client-only and a client-server archi-
tectures. The results show the advantage of the client-
server architecture over the client-only, with speedups
of up to 3.2 times being achieved. The client-server
architecture also saves power and space on client
units, thus, increasing the up time of the smartphones
used as clients as well as decreasing the storage
burden on them. This allows for the usage of lower
end smartphone as clients.
The work developed here is part of a proposed
mobile application for wound care. Future work in-
clude incorporating a three-dimensional re-
construction module in order to make the area
measurements more accurate and provide information
about the wounds’ depths. We also plan to develop a
follow-up module that will store the treatment
progress and a diagnostic module that will suggest
potential treatments based on historic data. Finally, it
is necessary to improve the graphical interface to
improve its usability.
ACKNOWLEDGMENTS
The authors would like to thank the financial support
provided by the Coordenação de Aperfeiçoamento de
Pessoal de N´ıvel Superior Brasil (CAPES) Finance
Code 001, during the development of this work. BMC
would also like to thank the CNPq INCT-MACC for
its support.
WoundArch: A Hybrid Architecture System for Segmentation and Classification of Chronic Wounds
657

REFERENCES
Brem, H. and Lyder, C. (2004). Protocol for the successful
treatment of pressure ulcers. The American Journal of
Surgery, 188(1):9–17.
Cardani, D. (2001). Adventures in HSV space. Labora-
torio de Robo´tica, Instituto Tecnolo´gico Auto´nomo
de Mexico.
Ciancio, F., Portincasa, A., Parsi, D., and Innocenti, A.
(2016). Mowa®: A simple and economic way of mon-
itoring chronic wounds outcome with your mobile de-
vices. Annali Italiani di Chirurgia, 88(1):88–94.
Clark, R. A. (2014). Chapter 76 - Wound repair: Basic bi-
ology to tissue engineering. In Lanza, R., Langer, R.,
and Vacanti, J., editors, Principles of Tissue Engineer-
ing (Fourth Edition), pages 1595 – 1617. Academic
Press, Boston, fourth edition.
Cohen, M. and Bard, M. (2015). Pilot clinical study at
UMMS to test ‘sugar’ diabetes app. Available at
https://www.umassmed.edu/news/news-
archives/2015/04/pilot-clinical-study-at-umms-to- test-
sugar-diabetes-app/.
Dealey, C. (2008). The Care of Wounds: A Guide for
Nurses. Wiley-Blackwell.
DigitalMedLab (2019). Wounddesk: The mobile solution
for wound care. Available at https://wounddesk.com/.
Friesen, M. R., Gigliotti, B., and Poon, T. W. K. (2016).
An mHealth technology for chronic wound
management. Mobile Health Technologies: Theories
and Applica- tions, page 115.
Garcia, T. R. and No´brega, M. M. L. d. (2009). Proceso de
enfermer´ıa: De la teor´ıa a la pra´ctica asistencial y de
investigacio´n. Escola Anna Nery, 13(1):816–818.
Godeiro, V. (2018). Ulcer segmentation and tissue classi-
fication using color texture clustering. B.S. Thesis,
Universidade Federal do Rio Grande do Norte.
Godeiro, V., Neto, J. S., Carvalho, B., Santana, B., Ferraz,
J., and Gama, R. (2018). Chronic wound tissue classi-
fication using convolutional networks and color space
reduction. In 2018 IEEE 28th International Workshop
on Machine Learning for Signal Processing (MLSP),
pages 1–6.
Kordestani, S. S. (2019). Atlas of Wound Healing E-Book:
A Tissue Regeneration Approach. Elsevier.
Meyer, F. (1992). Color image segmentation. In 1992 In-
ternational Conference on Image Processing and its
Applications, pages 303–306. IET.
Nussbaum, S. R., Carter, M. J., Fife, C. E., DaVanzo, J.,
Haught, R., Nusgart, M., and Cartwright, D. (2018). An
economic evaluation of the impact, cost, and medicare
policy implications of chronic nonhealing wounds.
Value in Health, 21(1):27–32.
Oliveira, N. B. d. and Peres, H.H.C. (2015). Avaliação do
desempenho funcional e qualidade te´cnica de um
sistema de documentação eletronica do processo de
enfermagem. Revista Latino-Americana de Enfer-
magem, 23(2):242–249.
Pounder, D. (1969). Lecture notes on forensic medicine.
Annals of Internal Medicine, 71(4):886.
Rubner, Y., Tomasi, C., and Guibas, L. J. (2000). The Earth
mover’s distance as a metric for image retrieval. Inter-
national Journal of Computer Vision, 40(2):99–121.
Sen, C. K., Gordillo, G. M., Roy, S., Kirsner, R., Lambert,
L., Hunt, T. K., Gottrup, F., Gurtner, G. C., and Lon- gaker,
M. T. (2009). Human skin wounds: A major and
snowballing threat to public health and the econ- omy.
Wound Repair and Regeneration, 17(6):763– 771.
Sirazitdinova, E. and Deserno, T. M. (2017). System de-
sign for 3D wound imaging using low-cost mobile de-
vices. In Medical Imaging 2017: Imaging Informatics
for Healthcare, Research, and Applications, volume
10138, page 1013810. International Society for Op- tics
and Photonics.
Sperandio, D. J. (2008). A tecnologia computacional
mo´vel na sistematizac¸a˜o da assisteˆncia de
enfermagem: avaliac¸a˜o de um software-proto´tipo.
PhD thesis, Uni- versidade de Sa˜o Paulo.
Tibes, C. M. S., Cherman, E., Souza, V., Westin, U., Zem-
Mascarenhas, S., and Evora, Y. D. M. (2015).
Avaliac¸a˜o de um aplicativo para apoio a` decisa˜o
no cuidado de u´lceras por pressa˜o. In Anais do
Congresso Internacional de Informa´tica Educativa
(TISE), pages 191–199.
Wallis, L. A., Fleming, J., Hasselberg, M., Laflamme, L.,
and Lundin, J. (2016). A smartphone app and cloud-
based consultation system for burn injury emergency
care. PLoS One, 11(2):e0147253.
Whitney, J. D. (2005). Overview: Acute and chronic
wounds. Nursing Clinics, 40(2):191–205.
HEALTHINF 2021 - 14th International Conference on Health Informatics
658
