
Handling Comparison between a Human and a Patient Simulator for
Nursing Care Related Physical Human-robot Interaction
Christian Kowalski
1
, Pascal Gliesche
1
, Conrad Fifelski-von Böhlen
2
, Anna Brinkmann
2
and Andreas Hein
1,2
1
OFFIS Institute for Information Technology, 26121 Oldenburg, Germany
2
Carl von Ossietzky University, 26129 Oldenburg, Germany
Keywords:
Human-robot Interaction, Nursing Care, Physical Relief.
Abstract:
The occurrence of musculoskeletal diseases among nursing staff leads to an early withdrawal from the profes-
sion, which reinforces the already existing lack of caregivers. To counteract this problem, we would like to
provide physical relief through robotic assistance at the bedside. However, the problem arises that for safety
reasons robotic assistance concepts should not be tested on humans at first. In this case, patient simulators
with an average person’s weight can function as a substitute. For the best results, both cases should behave
very similarly when evaluating robot assistance concepts so that the transfer from patient simulator to human
is small and therefore no major adjustments need to be made. To measure this potential difference, we have
compared the handling properties of both cases in this paper. We examined force measuring platform data
while a nurse mobilized an 80 kg human and a patient simulator from the back to the side. The experimental
results show that moving a patient simulator is more physically demanding compared to moving a human
with similar weight and that conventional collaborative lightweight robots are able to push and move a patient
simulator that is weighing far higher than the robot’s actual payload suggests.
1 INTRODUCTION
Nursing shortage is an already existing problem in
many countries. Demographic change means that
more and more people of advanced age have to be
cared for. In Germany in particular, the number
of nursing staff is also tending to decline (Schulz-
Nieswandt, 2018). The rising number of people in
need of care is being offset by a decreasing number
of qualified nursing staff, so that according to fore-
casts there will be a shortage of more than 450.000
caregivers by 2050 (Ehrentraut et al., 2015). One of
the reasons for the decrease in workforce size is the
early withdrawal from work due to musculoskeletal
disorders (Trinkoff et al., 2003). Especially nursing
activities at the bed have an enormous influence on
the load acting on the caregivers’ spines (Jäger et al.,
2013).
Common physical support tools are only of lim-
ited help in this regard. For instance, the time con-
suming usage of patient lifters is usually limited to the
transfer to or into the bed and thus does not actively
promote the patient’s mobility. A further possibil-
ity of relief is the augmentation of the nursing staff’s
Figure 1: Setup for the support of nursing care bed activities
using a bedside mounted KUKA LBR iiwa 7 R800 (a), an
AMTI AccuPower portable force measuring platform (b),
a rescue dummy functioning as a patient simulator with a
weight of 80 kg (c) and a multi depth camera system (d).
strength by exoskeletons worn on the body (Liu et al.,
2016; Taal and Sankai, 2011). However, an ex-
oskeleton has the disadvantages that it must be put
on before use and it is not able to replace the help of
a second nurse, who is often called in for physically
Kowalski, C., Gliesche, P., Böhlen, C., Brinkmann, A. and Hein, A.
Handling Comparison between a Human and a Patient Simulator for Nursing Care Related Physical Human-robot Interaction.
DOI: 10.5220/0010322006050612
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 605-612
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
605

demanding activities. As mentioned before, calling
a second person for help is often no longer possible
due to lack of personnel. Therefore, we envision to
develop a robotic assistance system that acts as a sub-
stitute for the otherwise missing second caregiver. For
this goal, we designed a setup in previous work where
a KUKA LBR iiwa 7 R800 was mounted to an actu-
ated care bed which is surrounded by a multi depth
camera arrangement (Fifelski et al., 2018) consisting
of Microsoft Azure Kinect 3D cameras and a force
measuring platform (Kowalski et al., 2020). Addi-
tionally, as the system is not certified according to
the Medical Device Directive (MDD of the European
Community), a rescue dummy with the weight of an
average person functions as a patient simulator in this
context (see Fig. 1). In our opinion, three key aspects
need to be researched in order to develop a support
concept for the relief of bedside nursing staff in car-
rying out nursing activities:
1. Force transmission concepts to a potentially vul-
nerable patient, serving a multitude of manipula-
tions and body anatomies.
2. Detection of suitable spots to interact with the pa-
tient.
3. Operation of the robot in orchestration with the
caregiver for an optimal interaction during task
execution.
In this work, we mainly want to discuss boundary
conditions that can lead us to the solution of the three
aforementioned key aspects. An extremely relevant
point is the testing of robotic support concepts in
real life. However, from an ethical and safety point
of view, it is more advantageous to initially test the
robot’s performance on patient simulators with hu-
man weight instead of real humans. The question
whether and to what extent the handling of such a
simulator differs from a real human being has to be
answered, which will be examined in more detail in
this work. Subsequently, we want to take a closer look
at the potential of a conventional light weight robot
manipulator such as the KUKA LBR iiwa 7 R800 to
move a patient simulator on its own. These robots are
not necessarily built to withstand the weight of people
during nursing activities.
After the presentation of the related work, we will first
present the results of the aforementioned nursing ac-
tivity analysis. Then, the two different experiments
including the comparison between a human and a pa-
tient simulator and the force transmission to move a
patient are conducted and discussed.
2 RELATED WORK
The intentional contact between robot and human
with additionally controlled force transmission is a
rather unusual topic, which is why the number of
publications for this particular subject is quite sparse,
even in the field of physical Human-Robot Interaction
(pHRI). In the health care domain, Erickson et al. pre-
sented a work on washing patients using a PR2 robot
with the help of capacitive sensing instead of vision
or force feedback (Erickson et al., 2019a). The robot
was able to follow and clean a human arm by follow-
ing its contour while maintaining a force under a cer-
tain threshold. The capacitive sensing neural network
model was trained to estimate the relative position of
the closest point on a person’s limb surface. For mo-
tion control, a high level Cartesian controller was used
to provide joint values to the low-level proportional-
integral-derivative (PID) controllers of the robot ac-
tuators. Only a few researchers have worked towards
the goal of washing a patient and in most cases the
they did not tackle the washing problem directly but
rather developed exoskeletons (Satoh et al., 2009) or
bath water control systems. King et al. again devel-
oped a robot that wipes off debris of a human’s up-
per arm, forearm, thigh or shank lying in a bed using
a compliant force-controlled wiping motion without
tracking but with the help of an operator (King et al.,
2010).
Another group of works deals with the aspect
of developing robots for the purpose of massaging.
Here, the contact between robot and human with si-
multaneous application of a predefined force is in-
tended, whereby the contact forces with the soft tis-
sue of the human are particularly difficult to assess.
Except for the bones in the human body, everything
else is defined as soft tissue and can be distinguished
by their different characteristics. The Young’s Modu-
lus of typical soft tissue is relatively low with a value
of around 1 MPa (Akhtar et al., 2011) and its model
can be described as a multilayered, anisotropic, vis-
coelastic, inertial, plastic and non-stationary environ-
ment (Golovin et al., 2014). In contrary, the Young’s
Modulus of skin can range from 5 kPa to 140 MPa
(Akhtar et al., 2011). This shows, that it is difficult
to grasp the properties in advance to a contact and
that they also most likely vary from person to person
based on the body composition, muscle contraction
and many other factors, once again showing the com-
plexity of soft tissue contact scenarios. Nevertheless,
Golovin et al. incorporated a control method includ-
ing position and force to perform the task of massag-
ing (Golovin et al., 2014). In most pHRI use cases,
a compliant robotic behaviour is desirable, which is
why impedance control is often the first choice in this
HEALTHINF 2021 - 14th International Conference on Health Informatics
606

area (Hogan, 1985; De Santis et al., 2008; Haddadin
et al., 2008).
In the context of medicine and surgery, the appli-
cation of force directly on humans by robotic assis-
tance systems is not a novelty, but the forces applied
are relatively small compared to the forces occurring
during the execution of nursing tasks (Peirs et al.,
2004; Ho et al., 1995). Another fitting area of work
in robotics is the manipulation of objects in the envi-
ronment by pushing, which is usually the method of
choice when the target object is too big or too heavy to
grasp. Just like in the aforementioned literature, ma-
nipulation by pushing is not trivial due to the many
geometrical and physical properties associated with
the robot’s surroundings. In general, for planning and
control either a forward model or an inverse model is
used to predict the next state based on an action of
the current state or to compute the action that changes
the current state to a desirable target state (Stüber
et al., 2020). There are many different approaches to
this topic, ranging from deep (reinforcement) learning
(Peng et al., 2018; Byravan and Fox, 2017; Ehrhardt
et al., 2017), data-driven (Stüber et al., 2018; Ridge
et al., 2015), analytical (Lee et al., 2015; Dogar and
Srinivasa, 2011) to physics engine (Zhu et al., 2017)
based methods. Although the pushing methods pre-
sented so far cover a broad field, to our knowledge
they have not yet been applied in the context of nurs-
ing, which adds a whole new layer of complexity due
to safety reasons.
3 APPROACH
3.1 Nursing Activity Investigation and
Physical Load Limits
In the beginning, a small focus group meeting was
held with four people attending who had a nursing
background. The reason for the meeting was, on the
one hand, to identify the everyday nursing activities
at the bed, which require physical effort and on the
other hand, to explore cooperative activities, since
in some cases the activity cannot be easily managed
alone. The activities were also carried out in an ex-
emplary fashion and recorded using the Azure Kinect
3D depth cameras for later analysis. The activities
determined were then compared with the literature to
obtain a complete representation. Then, the activi-
ties were compared with the ones used in a study by
Jäger et al. to determine the loads on the lumbar spine
with the help of a biomechanical model (Jäger et al.,
2013). In Table 1 these values are compared with the
maximum recommended lumbar load for healthy and
back-friendly working (Jäger, 2019). It is noticeable
that the execution of most nursing care bed activities
exceeds the load limits and therefore has a negative
impact on the musculoskeletal system. Another
aspect, which is of great relevance in this context, is
the consideration of the maximum forces that can be
applied to the human body. Due to the fact that the
intended transmission of force using robots is rarely
carried out, no values have yet been determined for
this application. However, it is possible to fall back
on safety values for collisions with robots for the
time being. Table 2 shows the maximum permissible
forces in Newtons per body region, which are derived
from DIN ISO/TS 15066 (ISO, 2017).
To validate the physical relief, in our case a force
measuring platform is placed in front of the bed in the
nurse’s work area. This does not allow a direct com-
parison with the results of the biomechanical model
of Jäger et al. (Jäger et al., 2013), but it is possible to
have a look at the measured ground reaction forces of
the nurse to draw conclusions from these data. Fur-
thermore, a good picture of the overall force distribu-
tion can be generated with the torque data from each
individual robot joint so that physical relief becomes
quantifiable.
4 EXPERIMENTS AND RESULTS
4.1 Handling Comparison between a
Human and a Patient Simulator
The creation of a realistic test scenario is an impor-
tant factor for many areas of robotics. While many
scientific papers deal with the generalization of robot
behavior and try to represent the real world in simula-
tions, real data remain irreplaceable for testing pur-
poses for the time being. Especially manipulation
tasks are very difficult to reproduce in simulations
due to the complexity caused by the direct contact
with all associated physical parameters (Peng et al.,
2018). This makes testing and data collection in the
real world all the more important. In the case of pHRI,
however, this turns out to be problematic, since dur-
ing development of a robot’s behaviour the collec-
tion of data directly on humans should be circum-
vented for reasons of safety and ethics. This problem
has been recently recognized for assistance robotics
and there exist approaches to collect data directly on
human models from robots in simulation (Erickson
et al., 2019b). In addition to simulation, data collec-
tion in the nursing context in the real world would
Handling Comparison between a Human and a Patient Simulator for Nursing Care Related Physical Human-robot Interaction
607

Table 1: Mean values and ranges of compressive force on the lumbosacral disc for three different execution modes of nine
nursing activities based on the results of Jäger et al. (Jäger et al., 2013). The appropriate force limit starts at 4.1 kN for 20
year old women and decreases down to 1.8 kN for 60+ year old women. For men the limits range from 5.4 kN to 2.2 kN
(Jäger, 2019).
Nursing activity Conventional Optimized Small aids)
a. Raising from a lying to a sitting position 3.4 (1.8 - 5.4) 2.3 (1.9 - 2.9) n.a
b. Elevating to a sitting position at the bed’s edge 5.0 (3.3 - 6.2) 2.7 (2.0 - 3.6) n.a.
c. Moving to the bed headboard with nurse at bed’s side 6.7 (5.6 - 8.0) 5.4 (3.7 - 6.5) 2.8 (2.3 - 3.2)
d. Moving to the bed headboard with nurse at bed’s head 5.7 ( 2.8 - 8.9) 2.5 (2.0 - 3.0) 2.4 (2.2 - 2.8)
e. Moving sidewards 4.9 (3.3 - 5.8) 2.6 (2.0 - 3.4) 1.9 (1.6 - 2.2)
f. Raising the bedhead 4.3 (3.8 - 5.4) 4.1 (3.5 - 5.2) n.a.
g. Assisting with a bed-pan 4.2 (2.6 - 6.5) 2.6 (1.6 - 3.3) n.a.
h. Moving from the bed into a chair 5.1 (3.8 - 6.5) 3.7 (2.3 - 4.4) 3.1 (1.6 - 5.3)
i. Raising from sitting to an upright position 4.9 (3.8 - 6.4) 2.5 (1.9 - 3.1) n.a.
Table 2: Body contact force limits based on (ISO, 2017).
Maximum permissible
Body region contact force [N]
Head 130
Face 65
Neck 150
Back 210
Shoulders 210
Chest 140
Abdomen 110
Pelvis 180
Upper arms 150
Forearms 160
Hands 140
Thighs 220
Calves 210
Figure 2: Process of the experiment to determine the dif-
ferences between handling either a patient simulator or a
human. A nurse is standing on a force measuring platform
(a) while turning the patient to each side (b-c) during the
process of moving towards the bed’s headboard.
also be conceivable with patient simulators. Since no
other work has yet made a comparison with regard to
the forces acting between patient simulators and hu-
mans, we will conduct the research for this particu-
lar topic with the infrastructure described before. For
the purpose of this comparison, the strenuous activ-
ity of moving the patient to the bed’s headboard when
standing at the bed’s side was performed by a care-
giver while standing on a force measuring platform
(see activity c in Table 1 and Fig 2). The activity was
performed five times with a 80.5 kg person and a 80
kg patient simulator. The process is divided into two
steps: The lying person or the lying patient simulator
is first turned to the side in the direction of the nurse
and is moved slightly towards the headboard when the
person is put back on his back. Then the same move-
ment is repeated but this time away from the nurse.
The entire process is also recorded by a depth cam-
era, so that the times of the two turning processes can
be tracked exactly for a precise analysis. The result-
ing forces of one pass can be seen in Fig. 3. In all
five passes, the two body turning activities were anal-
ysed both individually and together for every axis,
which can be seen in Table 3. In particular, the arith-
metic mean value, standard deviation, minimum and
maximum values were calculated for further inspec-
tion. If one compares the two turn activities with each
other, it becomes clear that the second turning event
of the patient requires less effort in the case of the
human and more effort in the case of the patient sim-
ulator. This becomes particularly obvious by looking
at the forces in the direction of the z-axis which is
5.27 times higher. Also, the overall standard devia-
tion is slightly larger during the first turn activity. Fur-
thermore, the minimum values when moving a human
are approximately the same during both turns with a
small difference of 8.8, the values while moving the
patient simulator are much further apart where the av-
erage value for the first turn is -130 while the second
turn has a value of only -24.1. In both scenarios, the
first turn activity has a higher value for the maximum
values, but the difference is greater for the human with
a value of 65 at the first turn while the difference for
the patient simulator is only 18.37. As expected, the
maximum values also show the highest peak load of
310.8 on average for the human and 388.7 for the pa-
tient simulator in the direction of the x-axis of the
force measuring platform, which is most likely due to
HEALTHINF 2021 - 14th International Conference on Health Informatics
608
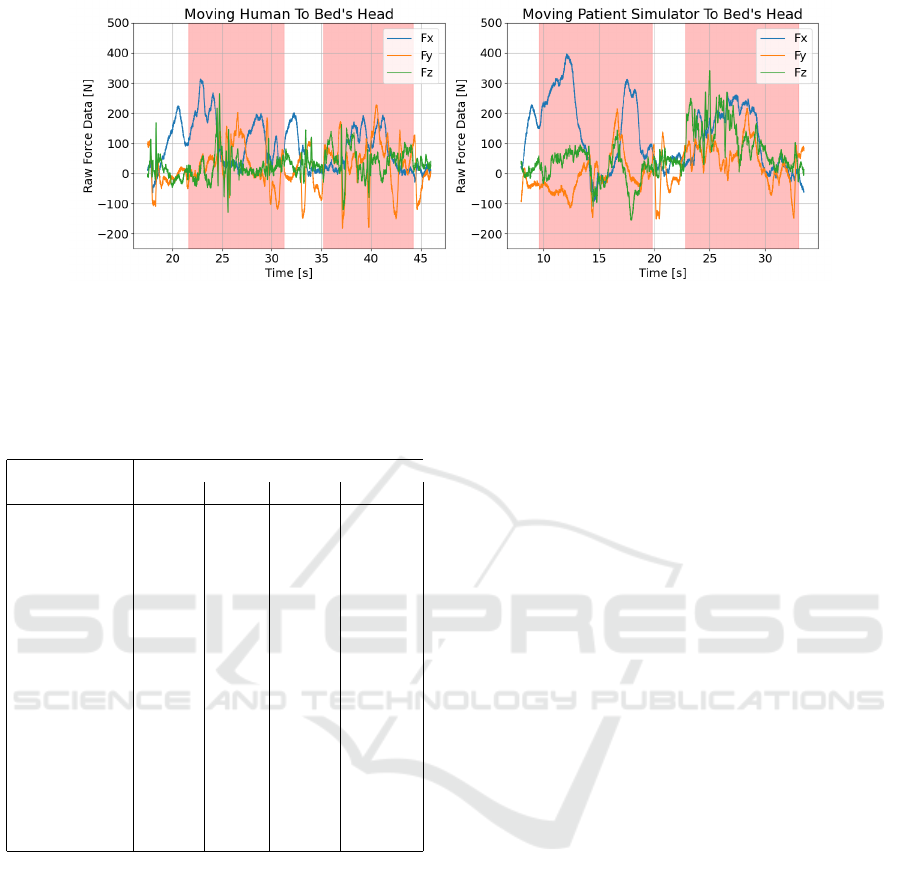
Figure 3: Raw force data (x, y and z axis) recorded while a nurse moves a human or a patient simulator towards the bed’s
headboard. The activity mainly consists of two turn movements (areas marked in red) which have been annotated using the
data of a depth camera recording.
Table 3: Results of the comparison between the handling of
a patient simulator and a human during the nursing activ-
ity of moving a patient towards the bed’s headboard in two
individual steps.
Human Patient Simulator
Turn: 1st 2nd 1st 2nd
∅ F [N] 51.7 39.2 66.6 107.6
∅ F_x [N] 112.9 52 156.4 135.3
∅ F_y [N] 21.5 30.7 19.4 60.2
∅ F_z [N] 20.6 35 24.1 127.2
∅ SD [N] 62.2 55.7 87.6 57
∅ SD_x [N] 85.8 49.2 124 43.6
∅ SD_y [N] 66 80.7 68.8 61.2
∅ SD_z [N] 34.8 37.2 70 66.1
∅ Min [N] -93.8 -85.0 -130 -24.1
∅ Min_x [N] -21.8 -24 -59.4 35.1
∅ Min_y [N] -174.4 170.2 -162.8 -83.6
∅ Min_z [N] -85.3 -60.9 -167.8 -24.7
∅ Max [N] 221.6 156.6 265 246.63
∅ Max_x [N] 310.8 155.9 388.7 214
∅ Max_y [N] 188.4 178.9 220.7 218.8
∅ Max_z [N] 165.7 134.9 185.4 307.2
the leverage when pulling the patient during the first
turn. This high value can also be found in the over-
all force, especially in the x-axis component. This is
also where the two most important statements regard-
ing the validity of the data can be found: first, the
x-axis component of the force data has very high val-
ues during the execution of the task. Second, turning
towards the nurse - i.e. the first part of the activity -
is more strenuous in both scenarios. Third, moving
the patient simulator is more strenuous than moving
the human being of an almost identical weight. On
average, turning towards the nurse is 1.28 times more
difficult using the patient simulator according to the
measurement and even 2.74 times more difficult when
during the turn away activity. Interesting at this point
is the difference in the load peaks, which are given
by the maximum values. During the first turn activ-
ity we measured a 1.2 times higher maximum force
when handling the patient simulator, during the sec-
ond turn activity it is even 1.57 times higher. It can
be concluded from the results that in the process of
placing the patient on his side, the patient simulator
with an almost identical weight cannot reproduce the
kinematics, material characteristics or loads of a real
human being. This experiment suggests that for a
test environment similar to that of a real human be-
ing, the patient simulators either need to be equipped
with better mobility or they need a lower weight in or-
der to map the potential load forces of a person with
more weight. It must be said, however, that the ex-
periment is limited to the performance of one specific
nursing activity and the results may vary significantly
for other activities.
4.2 Maximum Robot Load for Physical
Human-robot Interaction
Another important aspect, which is necessary for the
investigation of pHRI in the field of physical assis-
tance in care, is the payload or the potential of the
robots to move larger masses. It is well known that
robots are capable of moving large masses. However,
the potential maximum payload depends on the de-
sign, the configuration in respect to the patient and
the maximum torques at the relevant joints of the
robot. In nursing, however, it is also necessary to
have enough space for the collaborating caregiver.
The keyword "collaborating" is particularly impor-
tant here, since most collaboration robots are built
smaller and have lower payloads than common indus-
trial robots. In our example setup, an iiwa manipula-
tor with a maximum payload of 7 kg is used. How-
ever, for health care support, the robot has to cope
with the patients’ weight to provide physical relief.
Handling Comparison between a Human and a Patient Simulator for Nursing Care Related Physical Human-robot Interaction
609
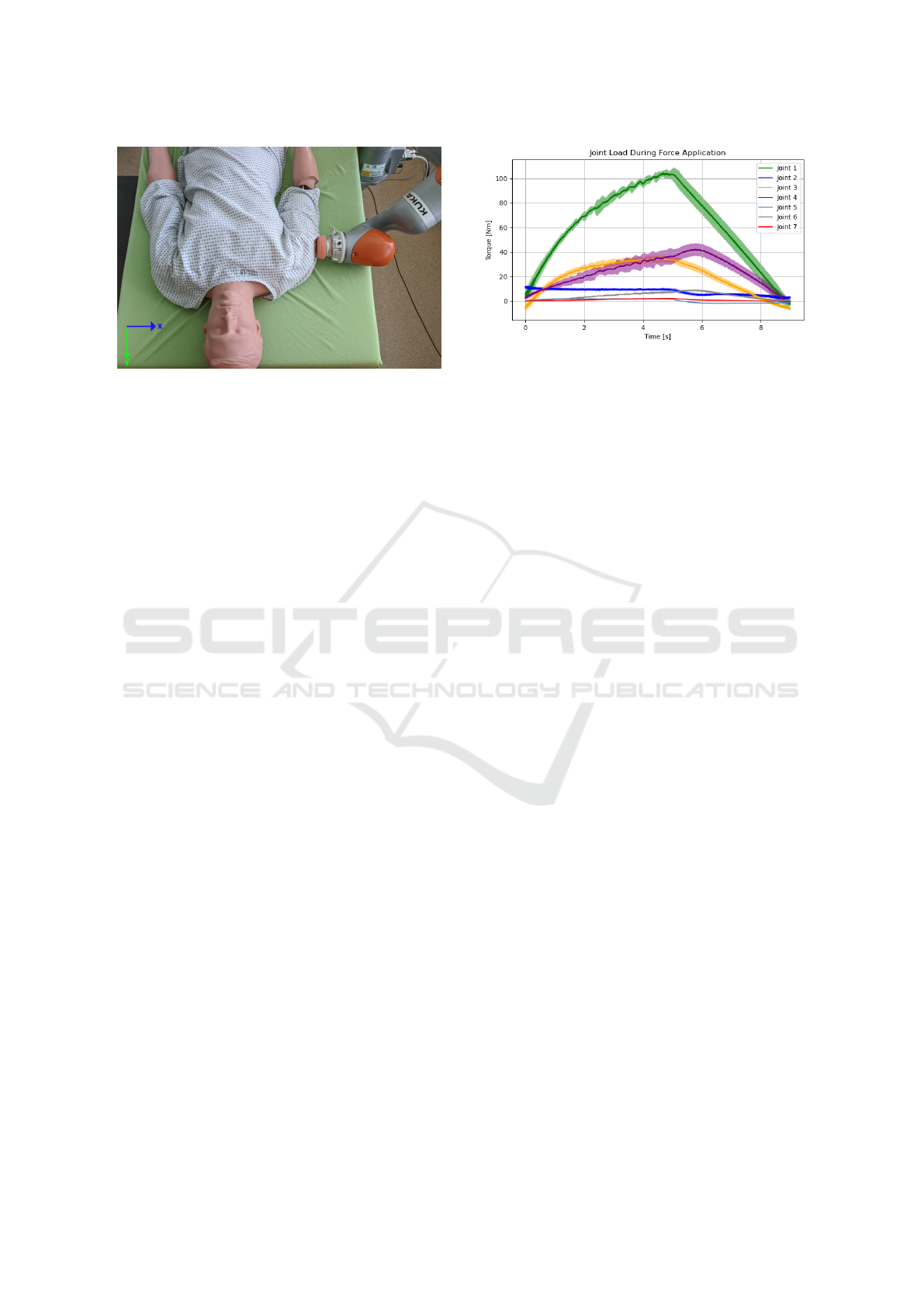
Figure 4: The setup of the robotic load experiment where
the robot tries to push the 80 kg weighing patient simulator
without any external help. The pushing starts at about 2.4
seconds and ends after 12.2 seconds. The torque for every
joint during the execution is measured.
For this case we have carried out a joint load test ex-
periment, where the robot manipulator should inde-
pendently move the patient simulator by pushing it
within the bed. To be more precise, the robot’s start
position q
q
q
start
(t) and goal position q
q
q
goal
(t) in joint
space have already been defined in advance so that
we only have to deal with the Cartesian movement
between these positions. In addition, we are only
considering the translational component of the move-
ment, breaking it down to a one dimensional motion
along the Y-axis relative to the robot’s base frame. For
the experiment, the end effector presses on the upper
arm of the patient simulator and thus moves it side-
ways by an amount of about 10 cm without additional
help (see Fig. 4). The resulting external torques at the
individual joints were observed over time (see Fig. 5).
The experiment was repeated 8 times and in all ex-
periments it was possible to move the 80 kg patient
simulator by about 10 cm without external help. The
experiment carried out reveals two important points:
first, the robot’s payload is not decisive for the max-
imum applicable force to move masses and second,
it is necessary to optimize both the configuration to
support without disturbing the caregiver and the joint
loads of the robot for maximum exploitation of the
push potential to maintain τ
τ
τ
min
(t) ≤ τ
τ
τ ≤ τ
τ
τ
max
(t) due
to the robot’s maximum allowed joint torques in New-
ton meters, being 176, 176, 110, 110, 110, 40 and
40 for the used robot manipulator beginning from the
robot’s first joint (base) to the last joint (end effec-
tor). This is very important because in the context
of nursing care, any robotic support movement will
have to deal with the problem of applying a prede-
fined force on one or more body parts of the patient
to cooperate with the nurse during the task execution
to finally provide physical relief. The complexity of
the trajectories while applying the forces can arbitrar-
Figure 5: Visualization of the joint torques during the
robotic load experiment where the robot applies a force to
move the 80 kg weighing patient simulator. Mean torques
of every joint and lower and upper error are visualized.
ily increase or decrease and is not dependent on the
actual force transmission itself, except in relation to
the force limit values, which must be adjusted regard-
ing the selected body part as shown in Table 2. As
already stated before, our system uses the FRI in or-
der to achieve a control loop frequency of up to 1
kHz. However, this also limits the obtainable robot
information so that only the individual external joint
torques can be acquired. For nursing care, it would
be best to make assumptions about the Cartesian end
effector forces without using any additional sensors.
For this particular case, it is possible to predict the
forces by using the relationship between applied end
effector wrenches and applied forces and torques to
the joints as in (Siciliano and Khatib, 2016)
τ
τ
τ = J
J
J(
(
(q
q
q)
)
)
>
f
f
f , (1)
where τ
τ
τ is the forces and torques vector for a robotic
manipulator of n degrees of freedom (DOF), J
J
J
>
is the
transposed Jacobian matrix and f
f
f is the end effector
force vector. To get the actual Cartesian end effector
forces it is possible to make use of the Moore-Penrose
inverse to finally get
f
f
f = (J
J
J(
(
(q
q
q)
)
)
>
)
−1
τ
τ
τ. (2)
Multiplying this result with the Jacobian gives us the
Cartesian end effector forces in its local frame. In
real care scenarios using a robot, the support move-
ment should make use of the force measurements to
constantly update the position along a predefined tra-
jectory to maintain the applied force below a desired
threshold depending on the individual body part, the
values for each can be found in Tab. 2 (ISO, 2017).
HEALTHINF 2021 - 14th International Conference on Health Informatics
610

5 CONCLUSIONS
In this paper we were able to collect important aspects
for the approach to the topic of pHRI in the care do-
main. There is a general need for physical relief in
care. For this relief through robotic assistance, how-
ever, a force application directly or indirectly on hu-
mans is necessary. Safety standards with values for
force limits depending on the body part do already ex-
ist but these were not created with the intention of pro-
viding relief in care and are currently only means to an
end. It requires a systematic creation of care-related
force limits. When testing care-relevant robotic sup-
port movements, initial experiments using humans is
not desirable and one should switch to patient sim-
ulators for this particular task. In the present paper,
however, it could be shown that there is a mismatch
between patient simulators and humans, which must
either be taken into account or developments in this
field must take place so that simulators become more
similar to humans with a suitable weight, material and
mobility. Finally, we were able to show that even col-
laborative lightweight robots can apply enough force
to independently move an 80 kg patient simulator in
bed and are thus also suitable for nursing activities.
6 FUTURE WORK
The presented work should serve as a basis for the
field of pHRI for nursing care and should also show
that despite existing gaps in the framework condi-
tions, there is a potential for force relief of caregivers
by collaborative robots. In future work, we will fo-
cus on directly supporting caregivers using robots and
on measuring and comparing the degree of potential
physical relief. For this, the three main difficulties in
this complex project mentioned at the beginning have
to be considered more intensively in follow-up work.
On the one hand, an additional assessment of physi-
cal properties may possibly provide an advantage in
the transmission of force. On the other hand, nursing
activities at the bed are such highly complex activi-
ties that this problem should perhaps be handled by a
robot controller learned through reinforcement learn-
ing rather than using a handcrafted controller. Over-
all, there are still many areas where the present system
can be further improved and used for research. We
envision a system which ensures significant physical
relief through human-robot interaction and coopera-
tion while maintaining safety standards with regard
to maximum force limits dependent on the patient’s
condition.
ACKNOWLEDGEMENTS
This work was funded by the German Ministry
for Education and Research (BMBF) within the re-
search project Nursing Care Innovation Center (grant
16SV7819K).
REFERENCES
Akhtar, R., Sherratt, M. J., Cruickshank, J. K., and Derby,
B. (2011). Characterizing the elastic properties of tis-
sues. Materials Today, 14(3):96–105.
Byravan, A. and Fox, D. (2017). Se3-nets: Learning rigid
body motion using deep neural networks. In 2017
IEEE International Conference on Robotics and Au-
tomation (ICRA), pages 173–180. IEEE.
De Santis, A., Siciliano, B., De Luca, A., and Bicchi, A.
(2008). An atlas of physical human–robot interaction.
Mechanism and Machine Theory, 43(3):253–270.
Dogar, M. and Srinivasa, S. (2011). A framework for push-
grasping in clutter. Robotics: Science and systems VII,
1.
Ehrentraut, O., Hackmann, T., Krämer, L., and Schmutz,
S. (2015). Zukunft der Pflegepolitik: Perspek-
tiven, Handlungsoptionen und Politikempfehlungen.
Friedrich-Ebert-Stiftung, Abteilung Wirtschafts-und
Sozialpolitik.
Ehrhardt, S., Monszpart, A., Mitra, N. J., and Vedaldi, A.
(2017). Learning a physical long-term predictor. arXiv
preprint arXiv:1703.00247.
Erickson, Z., Clever, H. M., Gangaram, V., Turk, G.,
Liu, C. K., and Kemp, C. C. (2019a). Multidimen-
sional capacitive sensing for robot-assisted dressing
and bathing. In 2019 IEEE 16th International Confer-
ence on Rehabilitation Robotics (ICORR), pages 224–
231. IEEE.
Erickson, Z., Gangaram, V., Kapusta, A., Liu, C. K., and
Kemp, C. C. (2019b). Assistive gym: A physics simu-
lation framework for assistive robotics. arXiv preprint
arXiv:1910.04700.
Fifelski, C., Brinkmann, A., Ortmann, S. M., Isken, M., and
Hein, A. (2018). Multi depth camera system for 3d
data recording for training and education of nurses. In
2018 International Conference on Computational Sci-
ence and Computational Intelligence (CSCI), pages
679–684. IEEE.
Golovin, V., Arkhipov, M., and Zhuravlev, V. (2014). Force
training for position/force control of massage robots.
In New trends in medical and service robots, pages
95–107. Springer.
Haddadin, S., Albu-Schaffer, A., De Luca, A., and
Hirzinger, G. (2008). Collision detection and reac-
tion: A contribution to safe physical human-robot in-
teraction. In 2008 IEEE/RSJ International Conference
on Intelligent Robots and Systems, pages 3356–3363.
IEEE.
Handling Comparison between a Human and a Patient Simulator for Nursing Care Related Physical Human-robot Interaction
611

Ho, S., Hibberd, R., and Davies, B. (1995). Robot assisted
knee surgery. IEEE Engineering in Medicine and Bi-
ology Magazine, 14(3):292–300.
Hogan, N. (1985). Impedance control: An approach to ma-
nipulation: Part i—theory.
ISO, D. (2017). Ts 15066: 2017-04. Robots and robotic
devices-Collaborative robots (ISO/TS 15066: 2016).
Jäger, M., Jordan, C., Theilmeier, A., Wortmann, N., Kuhn,
S., Nienhaus, A., and Luttmann, A. (2013). Lumbar-
load analysis of manual patient-handling activities for
biomechanical overload prevention among healthcare
workers. Annals of occupational hygiene, 57(4):528–
544.
Jäger, M. (2019). Die revidierten dortmunder richtwerte.
Zentralblatt für Arbeitsmedizin, Arbeitsschutz und Er-
gonomie, 69(5):271–289.
King, C.-H., Chen, T. L., Jain, A., and Kemp, C. C.
(2010). Towards an assistive robot that autonomously
performs bed baths for patient hygiene. In 2010
IEEE/RSJ International Conference on Intelligent
Robots and Systems, pages 319–324. IEEE.
Kowalski, C., Arizpe-Gomez, P., Fifelski, C., Brinkmann,
A., and Hein, A. (2020). Design of a supportive
transfer robot system for caregivers to reduce physi-
cal strain during nursing activities. In Studies in health
technology and informatics, volume 270, pages 1245–
1246.
Lee, G., Lozano-Pérez, T., and Kaelbling, L. P. (2015). Hi-
erarchical planning for multi-contact non-prehensile
manipulation. In 2015 IEEE/RSJ International Con-
ference on Intelligent Robots and Systems (IROS),
pages 264–271. IEEE.
Liu, C., Zhu, C., Liang, H., Yoshioka, M., Murata, Y.,
and Yu, Y. (2016). Development of a light wear-
able exoskeleton for upper extremity augmentation. In
2016 23rd International Conference on Mechatronics
and Machine Vision in Practice (M2VIP), pages 1–6.
IEEE.
Peirs, J., Clijnen, J., Reynaerts, D., Van Brussel, H., Heri-
jgers, P., Corteville, B., and Boone, S. (2004). A micro
optical force sensor for force feedback during mini-
mally invasive robotic surgery. Sensors and Actuators
A: Physical, 115(2-3):447–455.
Peng, X. B., Andrychowicz, M., Zaremba, W., and Abbeel,
P. (2018). Sim-to-real transfer of robotic control with
dynamics randomization. In 2018 IEEE international
conference on robotics and automation (ICRA), pages
1–8. IEEE.
Ridge, B., Leonardis, A., Ude, A., Deniša, M., and Sko
ˇ
caj,
D. (2015). Self-supervised online learning of basic
object push affordances. International Journal of Ad-
vanced Robotic Systems, 12(3):24.
Satoh, H., Kawabata, T., and Sankai, Y. (2009). Bathing
care assistance with robot suit hal. In 2009 IEEE In-
ternational Conference on Robotics and Biomimetics
(ROBIO), pages 498–503. IEEE.
Schulz-Nieswandt, F. (2018). Stationaere Altenpflege und
«Pflegenotstand» in der Bundesrepublik Deutschland.
Peter Lang International Academic Publishers.
Siciliano, B. and Khatib, O. (2016). Springer handbook of
robotics. Springer.
Stüber, J., Kopicki, M., and Zito, C. (2018). Feature-based
transfer learning for robotic push manipulation. In
2018 IEEE International Conference on Robotics and
Automation (ICRA), pages 1–5. IEEE.
Stüber, J., Zito, C., and Stolkin, R. (2020). Let’s push things
forward: A survey on robot pushing. Frontiers in
Robotics and AI, 7:8.
Taal, S. R. and Sankai, Y. (2011). Exoskeletal spine and
shoulders for full body exoskeletons in health care.
Advances in Applied Science Research, 2(6):270–286.
Trinkoff, A. M., Lipscomb, J. A., Geiger-Brown, J., Storr,
C. L., and Brady, B. A. (2003). Perceived physi-
cal demands and reported musculoskeletal problems
in registered nurses. American journal of preventive
medicine, 24(3):270–275.
Zhu, S., Kimmel, A., and Boularias, A. (2017).
Information-theoretic model identification and pol-
icy search using physics engines with applica-
tion to robotic manipulation. arXiv preprint
arXiv:1703.07822.
HEALTHINF 2021 - 14th International Conference on Health Informatics
612
