
Using Data Analytics to Strengthen Monitoring and Surveillance of
Routine Immunization Coverage for Children under One Year in
Uganda
Bartha Alexandra Nantongo, Josephine Nabukenya and Peter Nabende
Department of Information System, College of Computing and Information Systems, Makerere University,
P.O. Box 7062 Kampala, Uganda
Keywords: Data Analytics, Monitoring, Routine Immunization, Coverage, Performance.
Abstract: Immunization coverage is a traditional key performance indicator that enables stakeholders to monitor child
health, investigate gaps, and take remedial actions. It is continuously challenged by validity due to the neglect
of unstructured data and process indicators that track small changes/milestones. While empirical evidence
indicates digitalized immunization systems establish coverage from structured data, renowned administrative
and household survey estimates are often inaccurate/untimely. Government instituted awareness,
accessibility, and results-based performance approaches, but stakeholders are challenged by accurate
monitoring of performance against Global Vaccination Action Plan coverage targets. This heightens
inappropriate strategy implementation leading to persistent low coverage and declining trends. There is scanty
literature substantiating the essence of comprehensive immunization indicators in monitoring evidence-based
and timely interventions. For this reason, health workers failed to appreciate immunization process indicators
and monitoring role. The study aims at developing a real-time immunization coverage monitoring framework
that supports evidence-based strategy implementation using prescriptive analytics. The envisaged artifact
analyzes a variety of data and monitors immunization performance against comprehensive indicators. It is a
less resource-demanding strategy that prompts accurate and real-time insights to support intervention
implementation decisions. This study will follow an explanatory research approach by first collecting
quantitative data and later qualitative for in-depth analysis.
1 INTRODUCTION
Strong evidence indicates that big data analytics have
a positive impact on organization performance
(Bogdan and Borza, 2019), decision enhancing, and
agility gains (Ghasemaghaei, et al., 2017). In
healthcare, big data refers to structured, semi-
structured, and unstructured electronic health data
sets that are complex and difficult to manage with
classical software, data management tools, or
internet-based platforms. (Raghupathi and
Raghupathi, 2014; Dash et al., 2019). The healthcare
industry generates enormous data, scaling from
clinical decisions, patient-care, compliance, and
regulatory requirements (SoleimaniRoozbahani, et
al., 2019; Liang and Kelemen, 2016). The United
States health system alone by 2011 had generated 150
exabytes soon reaching yottabyte (Raghupathi and
Raghupathi, 2014; SoleimaniRoozbahani et al.,
2019). A substantial amount of data in the health
industry are stored in hard copy form, however, rapid
data digitization trend, for example, Digital Health
Management System (DHIS2) in Uganda, Electronic
Immunization Registries (EIR) piloted in Zambia,
Tanzania (Dolan, et al., 2020; Villagereach, 2020),
Immunization Information Systems (IIS) in Mexico
(Derrough, et al,, 2017), and Online Real-Time
Immunization System (OTRIS) among others,
generate volumes of data that can facilitate extracting
useful insights to support decision making for
efficient operations. Big data in healthcare is
overwhelming not only because of its volume but also
because of the diversity of data types and speed at
which it must be managed (Dash et al., 2019;
Palanisamy and Thirunavukarasu, 2017).
In public health, big data encompasses patient
information gathered from electronic health records
and participatory surveillance systems, as well as
mining of digital traces like social media and internet
Nantongo, B., Nabukenya, J. and Nabende, P.
Using Data Analytics to Strengthen Monitoring and Surveillance of Routine Immunization Coverage for Children under One Year in Uganda.
DOI: 10.5220/0010301805490556
In Proceedings of the 14th Inter national Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 549-556
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
549
searches (Bansal et al., 2016). Driven by the potential
to improve quality of healthcare delivery while
reducing costs, these massive quantities of data hold
the promise of supporting a wide range of healthcare
functions such as clinical decisions, gaining valuable
insights in monitoring and surveillance of disease
prevention strategies like immunization.
(SoleimaniRoozbahani et al., 2019).
Immunization is a cost-effective public health
intervention guaranteeing the safety of children
against preventable diseases and a right for every
child (Karami et al., 2019; Wariri et al., 2019). It has
numerous activities grouped into service delivery,
programme management, surveillance and
monitoring, advocacy and communication, vaccine
supply, quality and logistics components
(WHO/IVB/08.05, 2008). Immunization deters 2–3
million deaths yearly and an additional 1.5 million
could be avoided if immunization coverage is
improved worldwide (Bhatti, et al., 2017).
Immunization coverage (IC) is a cornerstone of
Primary Health Care and a key immunization
programme performance indicator that shows how far
a country is from preventable disease outbreaks
(Roux, et al., 2017; Derrough, et al., 2017). Coverage
is calculated as the percentage of persons in the target
age group who received a particular vaccine dose by
a specified age and is globally the most closely
followed indicator annually tracked (Sodha & Dietz,
2015). Indicators like the third dose of diphtheria-
tetanus-pertussis (DTP3) coverage is used to measure
the strength & reach of routine immunization (RI)
(Mihigo et al., 2016). RI ensures that children below
one year receive recommended vaccination on time,
at the right age, in accordance to the recommended
schedule by age, gender and with ease of access to the
point of vaccination (MOH-UG, 2017).
It is important to note that, the 194 GVAP
member states including Uganda have instituted
accessibility and awareness strategies like free
immunization, outreaches, traditional leader
engagement, mass campaigns among others to
increase IC (Bhatti, et al., 2017; Malande, et al.,
2019). Additionally, development partners like
GAVI, global fund, master card, Orange, have
subsidized vaccine costs and supported private health
facilities to ease community service accessibility
(Villagereach, 2020). Similarly, technological
strategies like IIS monitor vaccine coverage and
effectiveness (Derrough, et al., 2017); EIR are
capable of child enrolment at birth, unique
identifition, structured data aggregation, among
others (Dolan, et al., 2020; Villagereach, 2020).
However, an estimated 19.7 million children
under the age of one year never received basic
vaccines according to the global immunization
coverage 2019. Correspondingly, Uganda at 73%
DPT3, 88% BCG (WHO/UNICEF, 2020) and 55% of
fully immunized children coverage (MOH-UG, 2017)
lag below the GVAP 90% national coverage target by
2020 (Mihigo et al., 2016). Awareness/accessibility
strategies target caretakers while digital interventions
known to reduce health worker data burden are a
replicate of the current paper-based system (Dolan, et
al., 2020; Villagereach, 2020) aggregating structured
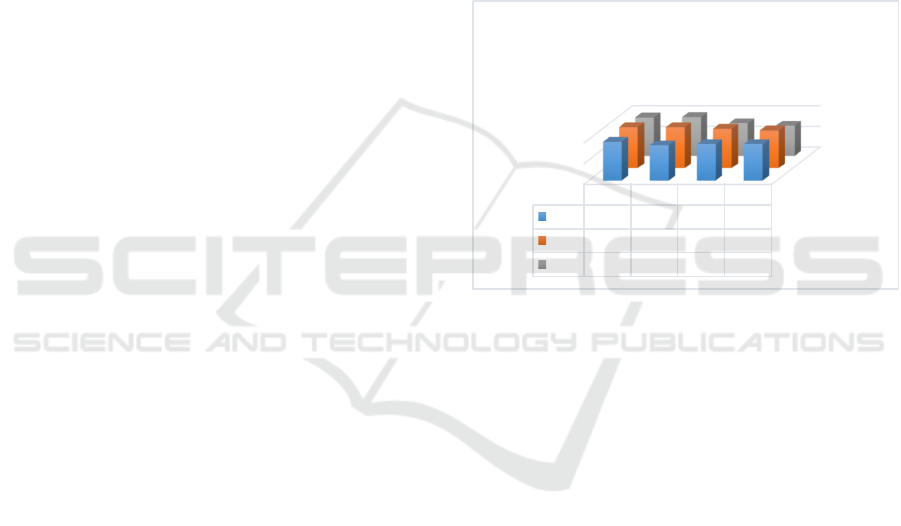
data only. Currently, government and development
partners are concerned about Uganda’s immunization
declining trends (WHO/UNICEF, 2020) as illustrated.
Figure 1: Current immunization coverage estimates.
The achieved IC gains were reversed due to reported
high infant mortality rate attributed to Vaccine-
Preventable Diseases -VPD (MOH-UG, 2017) and
sporadic measles and rubella 2018 outbreaks in 55
and 13 districts respectively (Opendi, 2018). In fact,
100% IC is still the target to avoid further mortality
(Bhatti, et al., 2017) which is hard to achieve without
constant monitoring.
Monitoring is a systematic and continuous
process of examining data, procedures and practices
to measure progress, identify problems, develop
solutions, and guide policies. It is an important tool
for mid-level managers to improve the quality of the
immunization programme by ensuring that: (1) all
infants are immunized; (2) vaccines and safe injection
equipment are delivered in correct quantities and on
time; (3) staff are well trained and adequately
supervised; (4) information on disease incidence and
adverse events following immunization (AEFI) are
collected and analyzed, (5) community has
confidence in the vaccines delivered and
immunization service they receive (WHO/IVB/08.05,
2008).
BCG
DPT3
0
50
100
2016 2017 2018 2019
BCG
94 85 88 88
DPT1
99 99 95 91
DPT3
93 94 79 73
Coverage
Ugandaimmunisationcoverageestimates
2016‐ 2019byWHO/UNICEFasper1stJuly
2020
HEALTHINF 2021 - 14th International Conference on Health Informatics
550

African ministers collectively and individually
committed themselves to monitor progress towards
achieving the goal of the global and regional
immunization plans having recognized that Africa
despite the progress, was largely off track compared
to the 2020 90% target (Desalegn, 2016). At national
and subnational levels, monitoring and assessment of
coverage rates are critical for countries to prioritize
and customize strategies or operation plans to address
immunization gaps and reach life-saving vaccine to
every child (Dicko, 2020; Derrough, et al., 2017).
However, IC validity is continuously questionable
as different tools report differing coverage for the
same population and time (Liu, et al., 2017; Murray,
et al., 2018). Known coverage determination methods
of administrative overestimate or underestimate
coverage while surveys are costly and provide
untimely information to guide programmes (Sodha &
Dietz, 2015. This is attributed to low-quality data.
Surveillance and monitoring data is largely captured
passively from structured DHMIS2. These traditional
passive monthly reports do not capture much
information on the advocacy and communication, and
programme-management components of the
immunization system (WHO/IVB/08.05, 2008.
Active supervision like physical supportive visits is
the instituted way to collect uncaptured data. It is
known to increase reporting of measles, rubella, and
hepatitis in demonstration projects but is generally
too expensive to be performed routinely (Roush,
2017), notorious for severe time lags and challenged
when aggregating variety of data (Bansal et al., 2016).
WHO asserts that monitoring requires a combination
of passive and active data collection measured against
indicators.
“Additional indicators that describe immunization
system functioning in real-time can provide managers
with essential information to guide their actions for
improving IC. Process indicators like a micro plan,
supervision, outreach conducted among others have
long been proposed but not highly valued by health
personnel or promoted as useful tools for
management” (USAID_MCSP, 2018). As the need
for evidence-based policies grows, big data hold the
key to rapid improvements to promote health/prevent
disease (Gall and Suzuki, 2019).
A new era is dawning where
monitoring/surveillance systems are strengthened by
big-data streams, from legacy systems and non-
traditional digital data sources, like social media
(Bansal, et al., 2017). Big data analytics technologies
and techniques can analyze large, diverse and
dynamic data sets intended to enhance firm decision
making/performance (Al-Shiakhli, 2019). They
discover associations, understand patterns and trends
within the data to improve care, save lives and lower
costs (Raghupathi and Raghupathi, 2014). “The
impact of big data in healthcare lies in identifying
new data sources such as wearable devices in addition
to the data in legacy sources”. Coupling analytics and
all data sources provide valuable insights for
researchers to attain novel health care solutions
(Palanisamy and Thirunavukarasu, 2017). Big data
analytics is beneficial to public health by turning
large amounts of data into actionable information that
can be used to identify needs, provide services,
predict and prevent crises especially for the benefit of
populations (Raghupathi and Raghupathi, 2014). Big
data analytics has been mainly used to predict (Heart
Attack, Disease Outcome/Outbreak), on fewer
occasions diagnosis and vaccine development. (Das
et al., 2018). Using prescriptive analytics,
Performance of public health intervention can be
monitored in real-time.
“Prescriptive analytics includes functions as a
decision support tool that explores a set of possible
actions and suggests decision based on descriptive
and predictive analysis of complex data” (Liang &
Kelemen, 2016). Using tools like optimization,
simulation, business rules, algorithms, and machine
learning (Al-Shiakhli, 2019), prescriptive analysis
conducts real-time analytics using point-of-care data
to present immediate and actionable information to
providers (Liang and Kelemen, 2016).
1.1 General Research Question
How can data analytics strengthen monitoring and
surveillance of routine immunization coverage?
1.2 Research Questions
1.
To what extent does data analytics influence
immunization coverage validity?
2.
How can big data analytics enhance
comprehensive indicators monitoring?
3.
What components must the immunization
coverage monitoring framework have to support
evidence strategy implementation?
4.
How will the developed coverage monitoring
framework be evaluated?
Using Data Analytics to Strengthen Monitoring and Surveillance of Routine Immunization Coverage for Children under One Year in Uganda
551

1.3 General Objective
To develop a real-time routine immunization
coverage monitoring framework that supports
evidence-based strategy implementation to improve
coverage, uptake and completion of routine
immunization.
1.4 Research Objectives
1. To establish the extent to which data analytics
can influence immunization coverage validity.
2.
To determine how big data analytics can enhance
comprehensive indicators monitoring.
3.
To design a real-time immunization coverage
monitoring framework.
4.
To evaluate the designed framework.
2 LITERATURE REVIEW
2.1 Immunization Data Quality
Immunisation programme performance management
must be built on a foundation of accurate and
complete data collection. Data checks and
management are crucial to improving performance
management, evaluation and form the basis of
evidence-based advocacy to politicians and donors.
(Stokes-Prindle et al., 2012). Poor quality and
underuse of data remain a persistent problem,
affecting the ability of countries and partners to
monitor progress against the GVAP goals as well as
supporting optimal changes to immunization
programmes (SAGE, 2019). The lack of adequate
skills in data collection, analysis, interpretation and
use among health workers are key factors limiting the
quality and use of data (SAGE, 2019).
In Uganda, vaccine dose administration data are
often not available or low-quality to optimally plan,
monitor, evaluate program performance (Ward, et al.,
2017) and target missed populations (Carnahan,
2020). Optimal immunization coverage relies on
high-quality immunization data, which are a
prerequisite for effective and efficient public health
action to improved population immunity against
VPDs (Ward, et al., 2017; Nzaji, et al., 2019).
Administrative IC estimates enable programme
managers to monitor, investigate gaps and take
remedial action. However, population denominator
used in the computation is often inaccurate (Ward, et
al., 2017).
In-accurate IC estimates are evident in many
countries like; inflation in administrative coverage
data in 2013 according to national data quality self-
assessment (DQS) in Uganda attributed to sub-
optimal data quality. Similarly, in Nigeria,
administrative data were indicated as unreliable to
accurately represent RI coverage levels hence
difficulty to evaluate programme performance
(Stokes-Prindle, et al., 2012). Overestimation and
underestimation occur in rural and near urban areas
districts respectively, therefore national coverage
estimates may not accurately reflect the true situation
(Wetherill, et al., 2017). In Democratic Republic of
Congo over-reporting on the administration of third-
dose of the pentavalent vaccine was identified in
Tshiaba, Mukeba and Ditalala and measles antigen in
Tshiaba and Tshibombo health facilities, while under-
reporting was evident in Ditalala and Mukeba (Nzaji,
et al., 2019). Surveys that never depend on census
population as dominator are known to be more
reliable. However, they are costly and provide
untimely (after 3-4 years) information to guide
programmes (Sodha and Dietz, 2015; Cutts et al.,
2016). Unreliable estimates undermine national and
international investments, prevents accurate
monitoring of global immunization initiatives, and
can increase the risk of VPDs outbreaks. (Wetherill,
et al., 2017).
2.2 Performance Indicators Monitoring
Strategies
2.2.1 Results-based Approaches
Results-based Approaches (RBA) and Results-based
financing and incentives (RBF) are government tools
to disburse a portion of its health budget in cash or
goods conditional on measurable actions taken or
performance target achieved by health workers
(Naimoli and Brenzel, 2009; Pearson, et al., 2010).
For example, GAVI funded programs receive results-
based funds after two years of an initial investment
(Stokes-Prindle, et al., 2012). RBF implemented in
Rwanda, Zambia and Ghana, between 2009-2014
indicated improved health services (Naimoli and
Brenzel, 2009; Stokes-Prindle, et al., 2012).
Conditional Cash transfer programs targeting
users of services began in Latin America/Caribbean
region in the 1990s; where a cash transfer to
household conditional on completing certain actions
statistically indicated significant IC increment in
Mexico and Nicaragua (Naimoli and Brenzel, 2009).
HEALTHINF 2021 - 14th International Conference on Health Informatics
552

These strategies, however, have unintended
pitfalls like non-remunerated services neglect, falsify
reporting, propagating a culture of monetization
among health workers, sustainability and cost-
effectiveness challenges (Stokes-Prindle, et al.,
2012). Pearson asserts that there is a risk of these
schemes to focus on results that are measurable
instead of important (Pearson, et al., 2010).
2.2.2 Other Approaches
The Reach Every District (RED) approach
implemented since 2002, emerged from WHO and
partners in an attempt to devise an innovative strategy
to improve stagnating immunization coverage in
Africa. It offers planning for better management of
resources, supportive supervision, link communities
with service delivery and ensures monitoring for
action (Mahigo, 2009). RED’s passive monitoring
tools like drop out chart, timeliness and completeness
reports, and data analysis increased IC. However,
RED is challenged by funding, lack of qualified staff
and immunization declining trends.
2.3 Comprehensive (Process and Basic)
Indicators’ Role
The capacity to attain and sustain recommended IC is
a great challenge facing expanded programs on
immunization (EPI). Bicaba et al. indicated that full
immunization coverage (FIC) is sufficient neither to
evaluate EPI performance nor to help identify the
broad strategies that must be implemented to improve
performance. The study asserts that FIC is a
restrictive process that only accounts for several
vaccines received, but not the age of the child at the
time of vaccination and adherence to schedule. They
recommended a tripartite performance view
including FIC, the adherence to vaccination schedule
and status of children not completely vaccinated. It
yields better-targeted interventions, inequity
reduction and vaccination accessibility. Conversely,
the study never investigated the reasons underlying
performance deficiencies (Bicaba, et al., 2009).
Similarly, Naimoli and Brenzel indicated there is
need for a comprehensive approach in monitoring the
immunization programme to draw attention to low
performing areas instead of the classical coverage
indicators (Naimoli and Brenzel, 2009). To
emphasize, Better Immunization Data (BID)
prioritization exercise team arrived at four
challenging areas that could be informed by EIR data
analysis namely: Denominators and population
movement, Missed opportunities, Continuum of Care
and Continuous quality improvement (CQI). CQI is
“an iterative data-driven process of empowering
health care workers to improve health service
delivery by identifying challenges, trends,
consistencies, outliers in coverage and dropout rate”.
BID is meant to share findings with stakeholders
(Carnahan, 2020). This approach, however, lasts for
a period, never informs stakeholders in real-time and
emphasis is put on basic performance indicators.
2.4 Big Data Analytics
The success of public health big data applications
entirely depends on underlying architecture and
utilization of appropriate tools. Data curation plays a
vital role in transforming big data into actionable
knowledge (Palanisamy and Thirunavukarasu, 2017).
Big data generate more revenue while reducing risk
and predicting future outcomes with greater
confidence at low cost. Big data management cycle
includes capture, organize, integrate, analyze and act
(Hadi, et al., 2015). However, validation,
interpretation, and visualization are crucial in
extracting actionable knowledge for decision making
(Liang and Kelemen, 2016). Besides,
real-time big
data analytics is a key requirement in healthcare to
address the lag between data collection and
processing (Raghupathi and Raghupathi, 2014).
Information systems design theory (ISDT)
underpins this study. ISDT’s strength is the
theoretical basis of “vigilance denoting the ability of
an information system to help an executive remain
alertly watchful for weak signals, discontinuities and
opportunities”. (Walls, et al., 1992)
. ISDT indicates
how to design an artifact on principles of function,
methods and justificatory theoretical knowledge.
3 METHODOLOGY
Pragmatism will form the basis of the study. It
integrates both inductive and deductive research and
accepts concepts to be relevant only if they support
action (Ågerfalk et al., 2008). The explanatory
approach will be used because it provides a greater
depth and breadth of information. (Venkatesh et al.,
2013). The research strategy is both qualitative
(useful to provide a detailed description as it occurs
in context) and quantitative methods (searches for
significant relationships, patterns or correlations
between variables) (Nowell and Albrecht, 2018)
following design science.
Using Data Analytics to Strengthen Monitoring and Surveillance of Routine Immunization Coverage for Children under One Year in Uganda
553
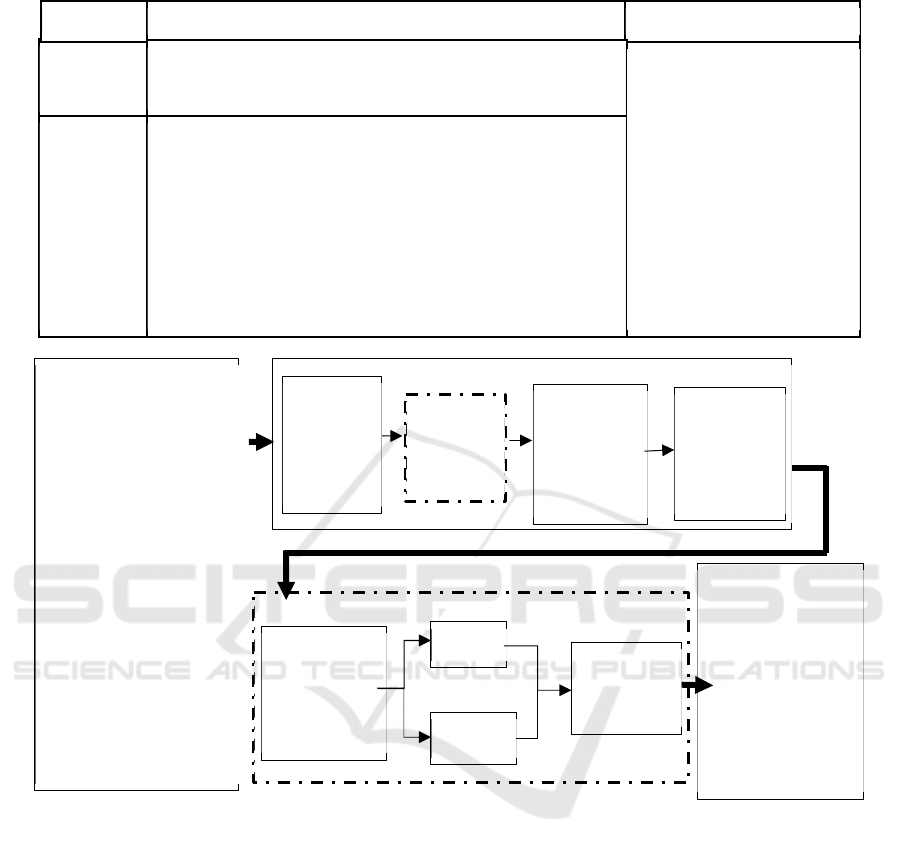
Table 1: Case study population.
Figure 2: Envisaged Artifact (Adapted from “Applied conceptual architecture of big data analytics” by (Ravikumaran and
Vimala, 2016)).
4 ENVISAGED ARTIFACT:
ROUTINE IMMUNIZATION
COVERAGE MONITOR
FRAMEWORK
The Routine Immunization Coverage Monitor
Framework in Figure 2 is an extension of
Ravikumaran and Vimala, 2016 applied architecture
of big data analytics. The adapted framework initiates
at a big data layer (A) by pulling/integrating
structured data from legacy systems and unstructured
data from immunization generating activities (data
curation) in real-time. These raw data are transformed
and validated at component (B). The transformed data
is subjected to big data tools and platforms like
Hadoop a “NoSQL” open source distributed data
processing technology. MapReduce provides the
interface for the distribution of sub-tasks and tracks
processing of each server/node. Mahout generates
machine learning algorithms while Lucene supports
text search and analytics. Using prescriptive
analytics, data mining and querying will generate
performance reports. The reports are fed into a data
discovery component (C). This component houses
variables like performance indicators. Comparing
immunization performance indicated by insights
Unit of
Analysis
Particular Kampala region details Kampala attributes
Unit of
inquiry
(per
Health
Facility)
Hospitals: 22 General hospitals, 2 National referrals, 3
Regional referrals, 13 Health Centre IV and 48 Health Centre
III. Total : 88
(
MOH U
g
anda
,
2018
)
-Key informants: In charge (health facility), Head of
immunization department, Community personnel (Village
health team), Head immunization outreaches, Records officer,
Nurse/vaccinator; Total study population: 528
-Representative sample size : 226 (Krejcie & Morgan, 1970).
-Sampling techniques: Stratified, simple random, purposive.
-Methods: Interview, questionnaire, focus group and document
review
-Data analysis: Epinfo for quantitative Text for qualitative
-Kampala covers 189.3
square kilo meter.
-Divisions/strata:
Kawempe, Rubaga; Central,
Nakawa, Makidye, -
Parishes 96 and 1285
villages. (UBoS; 2019).
-74,913 births per year.
-6,242 children immunized
(UNICEF-Uganda, 2015)
per month(formula
indicated by
(WHO/IVB/08.05, 2008)).
Knowledge Discovery (C)
Big data sources (A)
Immunization Variety
data
RDMS (DHIS2, IIS,
EIR, ORTIS)
Programme management,
advocacy &
communication
monitoring
TEXT
-SMS, social media
-Community mobilization
-Community meetings
-Supervisory visits
-Session/ outreach reports
-Training sessions
-Staff movement
-Transport schedule
-meetings
recommendation
Big Data techniques (B)
Platforms &
tools
- Hadoop
- Mahout
-MapReduce
-Lucene
Prescriptive
Analytics
-data
mining
-Queries
Comprehensive
Performance
indicators
Process
Basic
Gap
Strength
Appropriate
/
customized
Intervention
Outcome: Real
time performance
monitoring (D)
-Coverage validity
-Timely
interventions
-Increased coverage
-Low child mortality
-Increased hard
immunity, Less costs
-Low dropout rate
-Increased uptake
Data
Validation
Transform
ation
-Extract
Transform
Load
HEALTHINF 2021 - 14th International Conference on Health Informatics
554

from reports against set process and basics indicators,
strength and gaps are easily identified to inform
conclusion and support decisions for appropriate
customized child health intervention. It is this
intervention that is implemented national or
subnational level to attain/sustain recommended
immunization coverage preserving optimal validity.
5 EXPECTED RESEARCH
LIMITATION AND
MITIGATION
The researchers anticipate self-reporting to limit the
study, especially for selected key informants. This
will be mitigated by verifying given information with
doses administered in reports, unique child identifier
from Vital records management systems and National
Identification Regulatory Authority(NIRA) records.
6 CONCLUSION
Monitoring and surveillance of IC rates are critical at
national and subnational levels for countries to
prioritize and customize strategies to address
immunization gaps and reach life-saving vaccine to
every child. The study suggests that the success of the
immunization programme lies in real-time
monitoring of its performance against all set targets.
This study indicates that the envisaged framework
integrates structure and unstructured immunization
data to generate real-time programme performance
actionable knowledge to guide child health
interventions using prescriptive analytics. Monitoring
these insights against comprehensive health facility
indicators like micro-plans, process and national
basic indicators, is important in identifying evidence-
based gaps/strengths that inform conclusion and
support customized remedial action/interventions in
real-time to eliminate VPDs. This artifact also
strengthens monitoring and surveillance of IC with
greater validity confidence. Empirically establishing
the extent to which data analytics influences
immunization coverage validity will be the next step
in our research.
REFERENCES
Ågerfalk, P. J., Aakhus, M., & Lind, M. (2008).
Introduction to the Inaugural Meeting of the Aisspecial
Interest Group on Pragmatist Isresearch. Twenty Ninth
International Conf. on Information Systems. Paris:
Al-Shiakhli, S. (2019). Big Data Analytics: A Literature
Review. Luleå University of Technology.
Bansal, S., Chowell, G., Simonsen, L., Vespignani, A., &
Viboud, C. (2017, October 29). Big Data for Infectious
Disease Surveillance and Modeling.
Bhatti, U. A., Huang, M., Wang, H.,Zhang,Y., Mehmood,
A., & Di, W. (2017). Recommendation system for
immunization coverage and monitoring.
Bicaba, A., Haddad, S., Kabore, M., Taminy, E., Feletto,
M., & Fournier, P. (2009). Monitoring the performance
of the Expanded Program on Immunization: the case of
Burkina Faso. BMC.
Bloland, P., & MacNeil, A. (2019). Defining & assessing
the quality, usability,and utilization of immunization
data. BMC Public Health.
Bogdan, M., & Borza, A. (2019). Big Data Analytics and
Organizational Performance: A Meta-Analysis.
Carnahan, E. (2020, September 23). Using electronic
immunization registry data to demonstrate the value of
digital systems.
CIA. (2019). Uganda demographic profile 2019. (C. W,)
Cutts, F. T., Claquin, P., Danovaro-Holliday, M. C., &
Rhoda, D. A. (2016). Monitoring vaccination coverage:
defining the role of surveys.
Das, N., Das, L., Rautaray, S. S., & Pandey, M. (2018). Big
Data Analytics for Medical Applications.
Dash, S., Shakyawar, S. K, Sharma, M., Kaushik, S. (2019).
Big data in healthcare: management, analysis
and future prospects.
Derrough, T., Olsson, K., Gianfredi, V., Simondon, F.,
Heijbel, H.,, .Pastore-Celentano, L. (2017, April 27).
Immunisation Information Systems – useful tools for
monitoring vaccination programmes in EU/EEA
countries, 2016.
Desalegn, H. (2016). DECLARATION ON “Universal
Access to Immunization as a Cornerstone for Health
and Development in Africa”. Ministerial Conference on
Immunization in Africa. Addis
Dicko, W. (2020). Global Immunization Coverage 2019.
world health organisation. room/facts-
sheets/detail/immunization-coverage.
Dolan, S. B., Alao, M. E., Mwansa, F. D., Lymo, D. C., . .
. Shearer, J. C. (2020, March 30). Perceptions of factors
influencing the introduction and adoption of electronic
immunisation registries in Tanzania and Zambia.
Gall, C., & Suzuki, E. (2019). Big data: A new dawn for
public Health? In OECD, Health in the 21st Century:
Putting Data to Work for Stronger Health Systems (pp.
146 -167).
Ghasemaghaei, M., Hassanein, K., & Turel, O. (2017).
Increasing firm agility through the use of data analytics:
The role of fit.
Hadi, H. J., Shnain, A. H., Hadi Shaheed, S., & Ahmad, A.
H. (2015). Big Data and Five V’s.
Karami, M., Khazaei, S., Babaei, A., Yaghini, F. A., Gouya,
M. M., & Zahraei, S. M. (2019, June 11). Accuracy and
quality of immunization data in Iran: findings from data
quality self-assessment survey in 2017. BMC.
Using Data Analytics to Strengthen Monitoring and Surveillance of Routine Immunization Coverage for Children under One Year in Uganda
555

Krejcie, R. V., & Morgan, D. W. (1970). Determining
samples size for research activities. educational and
psychological measurement, 607 - 610.
Liang, Y., & Kelemen, A. (2016). Big Data Science and Its
Applications in Health and Medical
Research:Challenges and Opportunities.
Liu, G., Liao, Z., Liang, Y., Xiong, Y., & Ni, J. (2017).
Accuracy of parent-reported measles-containing
vaccination status of children with measles.
Mahigo, R. (2009). Immunisation and vaccination
development. WHO regonal office for Africa.
Malande, O. O., Munube, D., Afaayo, R. N., Annet, K.,
Bodo, . . . Musyoki, A. M. (2019, Febraury 14). Barriers
to effective uptake and provision of immunization in a
rural district in Uganda.
McKay, J., & Marshall, P. (2008). Foundations of Design
Science in Information Systems. Research into
Information Systems in Organisation..
Mihigo, R., Badr, N. A.-A., O’Malley, H., & Chaudhri, I.
(2016). Fulfilling a promise: Ensuring Immunisation
for all in Africa. WHO.
MOH_Uganda. (2018). National Health Facility Master
List 2018. Kampala: Ministry of health and Makerere
University school of public health.
MOH-UG. (2017). Aguide for National and District
Leaders to Promote Routine Immunisation in Uganda.
Kampala:
Murray, C. J., Shengelia, B., Gupta, N., Moussav, S.,
Tandon, & Thieren, M. (2018). Validity of reported
vaccination coverage in 45 countries.
Naimoli, J. F., & Brenzel, L. (2009). Results-
basedFinancing (RBF) for Healthand Immunization.
Nowell, B., & Albrecht, K. (2018). A reviewer's guide to
qualitative rigor. Journal of public administration
research and theory.
NPC. (2019). The state of Uganda Population report.
Kampala: National population council.
Nzaji, M. K., Lungayo, C. L., Kalala, M. N., Ngoie, C. K.,
Makala, J. P., Mwimba, B. L., . . . Mwamba, G. N.
(2019, March). Assessment of the Routine
Immunization Data Quality in Tshishimbi Health Zone,
Democratic Republic Of Congo.
Opendi, S. (2018). Statement to Parliament on
intervervation by the ministry of Health in combating
measles outbreak in Kiryandogo..
Oryema, P., Babirye, J. N., Baguma, C., Wasswa, P., &
Guwatudde, D. (2017, December). Utilization of
outreach immunization services among children in
Hoima District, Uganda: survey.
Palanisamy, V., & Thirunavukarasu, R. (2017).
Implications of big data analytics in developing
healthcare frameworks –A review.
Pearson, M., Johnson, M., & Ellison, R. (2010). Review of
major Results-based Aid (RBA) and Results-based
Financing.
Raghupathi, W., & Raghupathi, V. (2014). Big data
analytics in healthcare: promise and potential. Health
Information Science and Systems.
Ravikumaran P, Vimala D. K. (2016). A review: big data
and analytics in health care. Indian Journal of
Engineering, 2016, 13(31).
Roush, S. W. (2017). Surveillance Indicators. In CDC, &
N. C. Diseases, VPD Surveillance manual.
Roux, e., Akin-Olugbade, O., Katzen, L. S., Laurenzi, C.,
..., Rotheram-Borus, M. J. (2017). Immunisation
coverage in the rural Eastern Cape –are we getting the
basics of primary care right? Results from a
longitudinal prospective cohort study.
SAGE. (2019). Quality and Use of Immunization and
Surveillance Data. SAGE group.
Sodha, S. V., & Dietz, V. (2015, February 3). Strengthening
routine immunization systems to improve global
vaccination coverage.
SoleimaniRoozbahani, F., Ghatari, A. R., & Radfar, R.
(2019). Knowledge discovery from a more
than a decade studies on healthcare Big Data systems:
a scientometrics study.
Stokes-Prindle, C., Wonodi, C., Aina, M., Oni, G.,
Olukowi, T., Pate, M. A., Levine, O. (2012). Landscape
Analysis of Routine Immunization in Nigeria:
Identifying Barriers and Prioritizing Interventions.
UBoS (2019). Statistical Abstract for Kampala City.
Kampala Capital City Authority.
UNICEF_Uganda. (2015). Situation analysis of children in
Uganda. Kampala: UNICEF UGANDA.
USAID_MCSP. (2018). Indicators that describe the
strength of routine immunisation system.
Venkatesh, V., Brown, A. S., Bala, H (2013) Bridging the
Qualitative–Quantitative Divide: Guidelines for
Conducting Mixed Methods Research in Information
Systems.
Villagereach. (2020). Landscape analysis of electronic
immunization registries. Mozambique.
Walls, J. G., Widmeyer, G. R., & Sawy, O. A. (1992).
Building an information system design theory for
vigilant EIS.
Ward, K., Mugenyi, K., Benke, A., Luzze, H., Kyozira, C.,
Immaculate, A., MacN, A. (2017, December).
Enhancing Workforce Capacity to Improve
Vaccination Data Quality, Uganda.
Wariri, O., Edem, B., Nkereuwem, E., Nkereuwem, O. O.,
Umeh, G., Clark, E., Kampmann, B. (2019, September
23). Tracking coverage, dropout and multidimensional
equity gaps in immunisation systems in West Africa,
2000-2017.
Wetherill, O., Lee, C.-w., & Dietz, V. (2017). Root Causes
of Poor Immunisation Data Quality and Proven
Interventions: A Systematic Review.
WHO/IVB/08.05. (2008). Monitoring the immunisation
system. Module 5. In WHO, Training for mid-level
managers (MLM).
WHO/UNICEF. (2020). WHO/UNICEF coverage
estimates for 1980 -2019, as of 1 July 2020.
HEALTHINF 2021 - 14th International Conference on Health Informatics
556
