
Initial Development of ”Infection Defender”: A Children’s Educational
Game for Pandemic Prevention Measurements
Ivan Nikolov and Claus Madsen
Department of Architecture, Design and Media Technology, Aalborg University, Rendsburggade 14, Aalborg, Denmark
Keywords:
Health, Education, Pandemic, COVID-19, Web Application, Serious Games.
Abstract:
Using serious games to communicate and teach complex topics to children and adolescence has gained a lot of
popularity, especially in the medical fields. The spread of COVID-19 and the need to change everyday habits
has opened up the need to teach children the required precautions for limiting the spread of potential pan-
demics. In this paper we present the initial development of the game Infection Defender, promoting children’s
awareness of closing schools, social distancing, testing and hospitalization for fighting the spread of infectious
diseases in Denmark. These activities are given in the hands of children, between 10 and 13 years old, and
the goal of the game is achieving a balanced response to a possible infectious decease outbreak. We present
the game, its design considerations and how the learning objectives are integrated into it. An analysis of the
game by pedagogical workers is made and a pilot test is carried out assessing children’s reactions to it. Initial
positive feedback shows that the game sparks interest and discussion in children and can be used as part of the
study curriculum to help children understand the need for certain measurements. The game code is available
online - https://github.com/IvanNik17/InfectionGame.
1 INTRODUCTION
Serious games and gamified experiences are becom-
ing more and more widely used for teaching com-
plex topics to both children and adults, especially in
the field of health education (Lu and Kharrazi, 2018).
The tendency of developing such games has shown
a steady increase starting from the early to mid two
thousands and their target audiences have expanded
from professionals, to children and adolescents. The
topics of such games have also expanded to cover a
wide array of health concerns, problems and good
practices. Such topics range from oral health edu-
cation games (Malik et al., 2017), to mental health
education games (Lau et al., 2017) and improving
eating habits (Chow et al., 2020). Serious games
have proven especially important, with communicat-
ing best practices and behaviours for prevention of the
spread of diseases. These serious games can be build
as e-learning packages (Eley et al., 2019), that can
be implemented as part of the curriculum of students,
as a package of educational experiences (Hale et al.,
2017) or as mobile (Molnar and Kostkova, 2018) or
as virtual (Clack et al., 2018) and augmented real-
ity (Kang and Chang, 2019) experiences. Games that
address directly infection and disease understanding
and prevention are being researched (Castro-S
´
anchez
et al., 2016), especially with the rise of education
needs in the face of pandemics like the COVID-19
one. In this paper we present the initial development
and testing of an educational infection prevention se-
rious game ”Infection Defender”. The game is di-
rected towards 10 to 12 year old children and aims
to introduce the concepts of social distancing, infras-
tructure lockdown and the problems with hospital ca-
pacity. We go through the process of designing the
game experience, as well as the initial evaluations,
both from teachers, as well as from students.
Figure 1: A view from the developed game ”Infection De-
fender” presented in the paper.
Nikolov, I. and Madsen, C.
Initial Development of ”Infection Defender”: A Children’s Educational Game for Pandemic Prevention Measurements.
DOI: 10.5220/0010284102530260
In Proceedings of the 16th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2021) - Volume 1: GRAPP, pages
253-260
ISBN: 978-989-758-488-6
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
253

2 STATE OF THE ART
It has been shown that serious games can improve stu-
dent engagement, help with topic understanding and
influence learning outcomes, when introduced as part
of the learning curriculum (Huizenga et al., 2017).
Even with these benefits, the introduction of serious
and educational games in classes is still very lim-
ited. For health education, serious games are used as
tools to help with getting a better understanding about
vaccinations (Ohannessian et al., 2016), food hygiene
(Young et al., 2019), antibiotic resistance in bacteria
(Molnar, 2017; Govindan, 2018).
With the increased need for proper information
dissemination to both adults, children and adoles-
cences with the spread of the COVID-19 pandemic,
a number of educational games have been developed.
These serious games tend to tackle ideas such as
social distancing, infection spread, the importance
of testing and good hygiene practices. Some of
these gamified experiences are directed at instructing
personal on proper containment procedures (Suppan
et al., 2020) and takes the form of e-learning ma-
terials containing a mix of interactive experiences,
videos and tests. Other experiences use the pandemic
data present online, to create simulation like environ-
ments to visualizing how infections spread on a lo-
cal (Observable, 2020) and global (Tuovinen, 2020)
scale. These experiences put the power of choice in
the hands of players and use these choices to achieve
different ending. Through these endings, users can
see how following best practices can help not only
themselves, but the people around them. These games
adapt a more serious tone and clean design, which
can be deemed not appealing to younger children.
Other educational games rely more on the simplified
representation of a pandemic and use more simple
and easy to grasp game mechanics and visuals (Jacob
and Wiseman, 2020; LuluLab, 2020), more suited for
younger children. These games simplify the ideas of
social distancing, treatment, wearing mask.
For developing our proposed solution we try to
strike a balance, between a simplified approach to rep-
resentation of the many different problems associated
with dealing with pandemics and developing a game
that can be used for self-reflection and evaluation of
the players choices. To do this we develop a simple
gameplay concept, inspired by the approach presented
by (Molnar and Kostkova, 2018) and combine it with
a system that takes into account the different player
choices, which can be later viewed and accessed in
easily to understand and clean graphical form.
3 METHODOLOGY
The game development will be discussed in this sec-
tion, going from the initial idea inception, through the
choice of the main topics of the game - closing in-
frastructures, social distancing, testing and hospital-
ization to limit infection spread. We will also look
at how each of these topics has been introduced in
the game and how the idea of achieving balance be-
tween lowering the infection rates and keeping peo-
ple safe and dealing with the consequences of pro-
longed lockdown measurements. Finally, we will dis-
cuss the tools used for visualizing the consequences
of the players’ actions and how they can be used as a
positive teaching feedback loop.
The application is built in the Unity game engine,
utilizing a simple one screen style, which is easy to
port to different platforms like mobile and tablet or
web-based. The visual style relies on a 2.5D combina-
tion of polygonal objects and sprites, which is aimed
at a younger audience and emphasises lightweight vi-
suals, which should run on a wide array of hardware.
3.1 Initial Idea
The driving force for developing the game is creating
a engaging, easy to understand and educational appli-
cation, which can be used as a supervised tool, part of
a study curriculum. Pandemic and COVID-19 spread
visualization materials currently present are directed
more to the general public (Observable, 2020; Tuovi-
nen, 2020) and lack an easy to comprehend interface
and engaging gameplay, that would make them ap-
peal to younger children. On the other hand, there are
the children oriented education games like (Jacob and
Wiseman, 2020; LuluLab, 2020), which try to teach
good habits to children, but lack a more serious look
on how, the players’ choices have affected the game’s
outcome, which is proven to be a strong learning tool
(Taub et al., 2020).
The main topics we look at are social distancing,
closing of infrastructures, hospitalization and the ef-
fect of the pandemic and social precautions on peo-
ple’s mental health. The most important topic is social
distancing, as this is an idea that has become prevalent
in lowering the transmission rates of infections. It can
also be seen as a new concept for younger children,
which changes the way they interact with one another,
their family, teachers and random people in their ev-
eryday life. The second topic is the closing of infras-
tructures like schools, parks, shops and others, which
help limit the spread of infections, but also drastically
changes the day to day lives of children. The testing
and hospitalization are also topics, which can prove
GRAPP 2021 - 16th International Conference on Computer Graphics Theory and Applications
254

hard to explain to younger children. Finally, the topic
of the consequences of all these measurements on the
mental state of everyone that experiences them.
Next a design philosophy for the developed game
needs to be selected. We choose to build the game
around the idea of balancing between four main fac-
tors - amount of people sick in society, the maxi-
mum possible hospital capacity, the possibility to en-
force stronger or lighter social distancing measure-
ments and the mental health strain that these can have
on people. The game should have multiple levels, as
this has shown to produce more engagement (Wehbe
et al., 2017; Korchi et al., 2020) and each level should
last for a set time limit, shown to the players as days.
This would again mimic the real world problems of
prolonged social distancing. A view from the main
screen of ”Infection Defender”, can be seen in Figure
1.
3.2 Designing the Gameplay
The main factors of the game can be extremely
complicated to visualize and communicated, even to
adults. This is why special care needs to be taken for
expressing them in a way that children can understand
and relate to. It is shown that children respond better
to visual cues and explanations (Javora et al., 2019),
even though these visual do not help with learning,
they help with directing and keeping the attention of
children. The majority of the game design concerning
pandemic topics is thus developed as visual concepts.
The core playability of the designed game re-
volves around the formula of catching and dodging.
These types of fast passed gameplay are shown to
have a positive influence in the possibility of chil-
dren learning and understanding the information, be-
ing given through the gameplay experience. Hav-
ing chosen the main gameplay loop, each of its parts
needs to be connected to one of the four main factors.
The three parts of the catching and dodging loop are:
• Obstacles and rewards are spawned at one part of
the game field
• A player-controlled character dodges obstacles
and collects rewards at the center of the game field
• A end zone collects the missed obstacles and re-
wards, changing a player score
The first part of the gameplay loop, is where
healthy and infected people can spawn. A cartoon 3D
model of a person is created for this (Figure 2a), for
easier association, where healthy people are spawned
with blue shirts and infected people with red shirts.
This is done for easier color differentiation. To make
the visual representation of this easier to understand,
these people are spawned from houses, which are
shown as part of society (Figure 2b). They can then
go into one of four possible infrastructures - a super-
market, a school, a park with a pool and an amuse-
ment park (Figure 2e). This represents what a person
could do in a normal everyday life context, without
any social distancing restrictions in play. Here the
first interaction possibility is given to users - they can
choose to open or close these infrastructures, effec-
tively limiting the number of people that can spread a
possible infection. Once a infrastructure is closed, an-
other of the main factors comes into play - the gradual
decrease in people’s happiness. This happiness is de-
creased every day, while the infrastructure is closed,
until it’s reopening, when it starts to increase.
The second part of the gameplay loop is repre-
sented a player controlled character that can catch in-
fected people and send them to the hospital. For the
character we have chosen a representation of an am-
bulance, where sick people can be intercepted (Figure
2c). Here another of the chosen factors is developed
- the player can try to catch every infected and send
them to the hospital, but that would take up all of the
hospital’s capacity (Figure 2d). The third part of the
loop is the end zone, where the healthy people and
the infected ones, missed by the player would end up.
This is represented with houses, which represent peo-
ple visiting their friends, family or relatives and if in-
fected, unknowingly spreading the infection (Figure
2f).
Four endings are possible for each level, repre-
senting problems faced by people and governments
at times of epidemics spread:
• The player lets too many infected people pass and
the infection spreads too much
• The player hospitalizes too many infected people,
resulting a shortage of hospital beds
• The player leaves the infrastructures closed for
too long, resulting in in a deterioration of people’s
mental health and happiness
• The player manages to navigate the epidemic for
a set number of days, without any of the first three
endings happening
This combination of endings creates a sense of un-
certainty and the possibility of experimentation with
different play strategies, which have been shown to
help with engagement and interest (Nugroho et al.,
2018; Tancred et al., 2018). This ties to the post-level
experience, where the consequences of the players ac-
tions are visualized.
Initial Development of ”Infection Defender”: A Children’s Educational Game for Pandemic Prevention Measurements
255
(a) (b) (c) (d)
(e) (f)
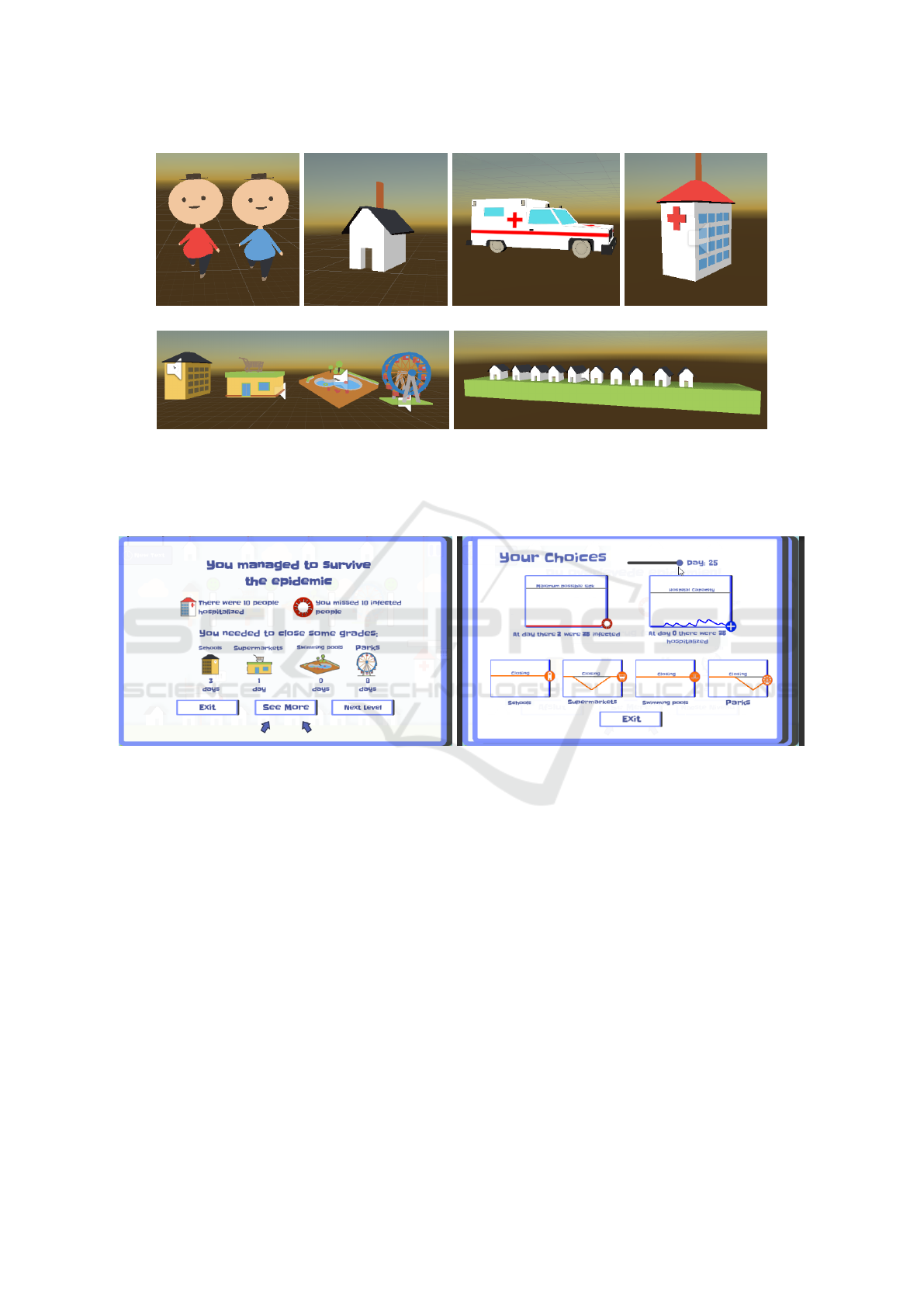
Figure 2: Parts of the gameplay loop - infected and healthy people (Figure 2a), houses which spawn new people (Figure 2b),
ambulance used by the player to catch infected people (Figure 2c), hospital building, where infected people go and which
has maximum possible capacity (Figure 2d), different infrastructures, which can be closed to slow down the infection spread
(Figure 2e) and houses representing society (Figure 2f).
(a) (b)
Figure 3: Two of the end screens of the game giving information to the player. Figure 3a is the end of level visualization,
showing what were the end results from the decisions of the player. The results are separated into - how many people were
hospitalized, how many people have spread the infection and how many days was each of the infrastructures closed. From
this screen users can either go directly to the next level with higher challenge or go and see the more detail results Figure 3b.
Details screen, shows the day by day choices and progress of the player, for how many people were hospitalized, how many
left the hospital, how many were missed and how the happiness and mental health changed depending on the opening and
closing of infrastructures.
3.3 Post-level Statistics
Once a level is finished, no matter the achieved end-
ing, the post-level statistics are visualized. These are
separated in two screens. The first one (Figure 3a)
represents a more easily approachable overview of the
consequences from the level, where everything is pre-
sented in the form of a combination of images and
snippets of text. In this screen the overview of how
much infected people have been hospitalized, how
many have been missed and how many days have the
different infrastructures been closed is given. The sec-
ond screen is given as a optional experience, which is
designed to be used, as part of a class discussion or
together with an teacher or parent. In this screen the
day by day changes in the overall infected and hospi-
talized people, as well as the decrease in happiness for
each closed place, through the played level are given
(Figure 3b). Here users can freely move through the
different days and see how their choices have influ-
enced the different parts of the game and where po-
tential problems have started to arise.
The two post-level statistical screens are designed,
with the idea to provoke discussion and a sense of cu-
GRAPP 2021 - 16th International Conference on Computer Graphics Theory and Applications
256

riosity. Users should be able to easily see, how their
interactions and choices have invoked a certain level
ending sequence. And more importantly these parts
of the game are designed to provide a sense of reflec-
tion and the desire to understand and try again.
4 TESTING
The main concepts of the game and the gameplay loop
are initially tested through a series of internal collabo-
rator testing. Once the overall feel of the game and its
components, menus and basic visuals are selected, the
second part of the evaluation is done through a collab-
oration with an external primary school teacher. The
teacher evaluated the application and the possibility of
using it as part of a curriculum or self-study sessions
on the topic of decease and infection prevention. Fi-
nally, an unstructured playtesting session is arranged
with a class of 11 to 12 year old children. After the
play session, kids are asked question about what they
liked and disliked about the game, as well as what
they learned and what was hard to understand.
4.1 Internal Testing
Through the process of developing the educational
game, an internal collaborator testing was set up,
where participants could test the developed game
parts and provide feedback about the usability of the
menus, the level of difficulty, the gameplay elements
and feeling of the game. For this early a set of strict
guidelines are set up. As the participants are older
people the main concern at this stage are - the diffi-
culty of the game, the overall clearness of the message
and evaluation of the different game parts. The par-
ticipants were given the game and left to test it out at
their pace. They were given an online questionnaire
containing both open ended questions evaluating the
experience, as well as questions regarding their play
setup - using a computer, table, phone, as well as the
maximum reached level.
The main point that participant feedback focused
on was a balance between challenge and user interest
and to facilitate that a gradual increase in difficulty
is introduced for each successfully passed level. This
increase is tied to the basic ideas present in the simpli-
fied mathematical modeling of infection diseases, as
presented in the Susceptible, Exposed, Infectious, or
Recovered (SEIR) model (Li and Muldowney, 1995).
These types of models are used for predicting the
possible spread, total number of infections, the time
needed for the disease to die down, etc. Taking inspi-
ration of these types of models, we base the increase
in difficulty of the game to a number of factors:
• The chance of spreading the infection - repre-
sented by the stochastic chance of spawning an
infected person. This chance becomes higher with
each successful level and is capped after a certain
values
• Time to recover - represented by the time spawned
people taken to the hospital would become
healthy, lowering the number of infected in it
• Number of hospital beds and number of possible
infected in society, before the spread becomes too
much. This is represented in the game as lowering
values, making it harder for the player to achieve
the a positive level outcome
The amount by which these values increase or de-
scries, as well as the caps to how much they can
change are set, after a number of testing sessions, end-
ing with participant feedback and discussions.
Another important factor of this initial internal
testing is providing a easy to learn and use controls
and menus for the game. Early on it was chosen that
the game needs to be playable in a web browser, with
an additional version for mobile and touch screen de-
vices. This influenced the design of the interactions
with the game, which mostly consist of swipes and
presses. Both the mechanic of catching the infected
people and opening and closing infrastructures are de-
signed to be used with just presses and swipes. All
menus are also designed to be easily navigated, with
only button presses and dragging motions.
4.2 Teacher Feedback
Once a stable internal prototype is created, the next
step is an evaluation by a primary school teacher. This
evaluation is done so feedback can be given on any
possible problems or places where children might find
context hard to understand or navigate. In addition,
parts of the game that need to be added or changed
can be identified, to make the game better suited as
a possible part of a study curriculum. The evaluation
guidelines given to the teacher were more relaxed -
they could test the prototype and use a think-aloud
method for asking questions and giving feedback to
their experience.
The teacher is experienced in teaching students
between 10 and 13 years old and is used to imple-
menting activities, games and participation experi-
ences in the day to day curriculum. After analysing
the game a number of points were given about the us-
ability, ease of understanding and lessons that can be
learned from it. A number of concerns are given for
Initial Development of ”Infection Defender”: A Children’s Educational Game for Pandemic Prevention Measurements
257

the possibility that students can get incorrect under-
standing of the spread of infections or how the differ-
ent measures would change the spread. In addition, it
is pointed out that the reliance of images and smaller
amount of text, could make understanding and get-
ting into the game’s flow a problem. Finally, some of
the visualizations in the game are pointed out as ei-
ther being too hard to understand or posing a risk of
stressing out the students. To address these concerns
a number of improvement are made to the experience,
to contextualize and refine its visuals and messages.
The main changes made from this feedback is the
addition of ”How To Play” (Figure 4a) section to the
start menu of the game, as well as an extended vi-
sual tutorial (Figure 4b), which runs users through
the main parts of the game and explains how they
function and what is required. In addition, the main
playable character is changed to a bed, where in-
fected people can be cough and send to the hospital.
This is made to make it less stressful to children and
lower the association to ambulances and emergency
situations. The interface is also made more reactive,
with the implementation of additional visual cues and
sound effects to signal to children that there are prob-
lems.
4.3 Student Feedback
As part of the evaluation a number of students from
third, fourth and fifth grade were shown the prototype
and could try it out. For the evaluation the teacher
first would show the game to the students and ex-
plain the overall structure and goal. The students then
play the game, initially with the teacher as a facilita-
tor and later by themselves. Once they felt that they
had played enough the teacher asked the whole class
what were their thoughts and questions.
The third grade students are shown to be receptive
to the overall message of the application with com-
ments like - ”If you close schools not many people
will be infected. It fits that it got better in Denmark
when we closed the schools” and ”You lose, if you
close things for too long”. It is also shown that there
is still some confusion, about the rate at which the
infection spreads - ”It’s a strange game because it’s
mega easy to get infected in that game. It doesn’t go
that fast in reality”. The game needs to communi-
cate better the generalization of the infection spread
from real life to game form and what simplifications
are used.
Students from fourth and fifth grade were testing
the application, from a point of view of using it as
a source to spread awareness. Students had observa-
tions on the messages communicated by the prototype
- ”You get isolated at home. It is only if things have
gone awry that you get to the hospital”, as well as the
need to position the game as part of a larger contex-
tual explanation of infection spread - ”It shows nicely
enough how it develops, but if you had not been told
in advance that it was a model of infection spread,
and have just played the game, you probably would
not have caught it. It requires that you have been told
the meaning of the game from the start”. An interest-
ing insight in the students’ understanding of infection
spread, many comments were made about the need
for differentiating between different groups of peo-
ple - older, younger or ones with pre-existing condi-
tions and how some are more susceptible, than others.
Comments like ”It does not show at all how bad it
can be for other people. It does not show that people
are different” and ”It’s weird if they come down from
their home, then to school and then down to another
home. Is it their grandparents’ home - so they can
infect them?”, show that a better separation between
the visualized people and houses needs to be done, so
the idea of not going out and staying home to lower
infection rates can be more easily communicated.
Overall the even it this early prototype stage, the
game has been shown to produce a lot of discussion
on the topic of infection spreading and how to prevent
it in a sustainable way. By seeing the consequences of
their decisions in each level, students could get a bet-
ter understanding of what was shown and try to do
better. A number of problems and possible optimiza-
tions are extracted from the students feedback. The
most important take always can be summarized as:
• The simplification of the real world infection
spread, to a simple game form needs to be ex-
plained in bigger detail - what are the houses rep-
resenting, what are the closed and open facilities
representing, why it’s important to have some in-
fected going to the hospital, which it’s important
to not let the infection spread too much.
• There needs to be a separation between different
groups of people - the ones more vulnerable to the
effects of a possible infection and the ones less
vulnerable. Different measurements can be em-
ployed to address different people.
• Make the experience more personal - children
want to see familiar things so they can empathise,
with what’s unfolding on the screen.
• A larger study context needs to be provided for
the game experience. It can be used as a part of a
infection prevention study, with other similar ex-
periences.
GRAPP 2021 - 16th International Conference on Computer Graphics Theory and Applications
258

(a) (b)
Figure 4: Screens added after the initial testing by the teacher - a ”How to Play” screen (Figure 4a), which can be easily access
from the start menu and would give a starting understanding of what is the main idea of the game. The second screen is an
interactive tutorial (Figure 4b), which gives a deeper look on the different system. The tutorial cannot be skipped the first time
the game is started.
5 NEXT STEPS
Because of lack of long term testing and quantita-
tive data the current study presents just a initial ex-
ploration, which will be build upon in consecutive
studies. A number of next steps are suggested for
the development of the application and its position in
a possible educational package. Further work with
teachers would be made to create a study curriculum
comprising of lectures on the topic of infection spread
and prevention. These lectures will be followed by a
number of animated shorts presenting every day sce-
narios where people could stop the spread of a in-
fections disease by following preventive recommen-
dations, such as social distancing, avoiding contact,
washing their hands and limiting traveling. The pre-
sented game prototype will be followed by a num-
ber of additional interactive applications and physical
boardgames around the same ideas. Children would
be able to play these games both together with teach-
ers, as well as alone. After the activities the knowl-
edge of students on the topics will be tested with a
number of assignments and discussions. This edu-
cational package will be available online for use by
teachers.
6 CONCLUSION AND FUTURE
WORK
In this paper, we presented the first steps for creat-
ing a educational game for children between 10 and
13 years old, in the topic of infection spread preven-
tion. We build the application with the main idea of
choices and consequences, where a balance between
preventing infection spreading, shortages of hospital
beds and preserving the population’s morale needs to
be found. To facilitate the idea of choices and conse-
quences, the application contains extensive post-game
statistical summaries, which can be used to reflect on
the choices and how they have affected the outcome
of the game.
Initial testing of the prototype was made as a com-
bination of internal developer testing, teacher evalu-
ation and student feedback. A number of improve-
ments were made to the application as a result of
these tests - mainly an better visual representation of
the game world, an implementation of tutorials, more
reactive user interfaces and menus. The application
has proven to facilitate discussion between students
around infection spread and interest and interest in the
topic.
As a next step a structured user testing is pre-
pared for students, where statistics like amount of
time played, maximum level reached, positive versus
negative outcomes reached, as well as hospital space
used, amount of days each infrastructure is closed,
amount of missed infected people, would be analyzed
to better suit the game to the user group. In addition,
a mobile version of the game would be prepared, as
well as implementing all the feedback from the initial
round of feedback.
ACKNOWLEDGEMENTS
This work was partially funded by the The Novo
Nordisk Foundation, grant no. NNF20SA0063089.
This funding is gratefully acknowledged.
Initial Development of ”Infection Defender”: A Children’s Educational Game for Pandemic Prevention Measurements
259

REFERENCES
Castro-S
´
anchez, E., Kyratsis, Y., Iwami, M., Rawson,
T. M., and Holmes, A. H. (2016). Serious elec-
tronic games as behavioural change interventions in
healthcare-associated infections and infection preven-
tion and control: a scoping review of the literature and
future directions. Antimicrobial Resistance & Infec-
tion Control, 5(1):34.
Chow, C. Y., Riantiningtyas, R. R., Kanstrup, M. B., Pa-
pavasileiou, M., Liem, G. D., and Olsen, A. (2020).
Can games change children’s eating behaviour? a re-
view of gamification and serious games. Food Quality
and Preference, 80:103823.
Clack, L., Hirt, C., Wenger, M., Saleschus, D., Kunz, A.,
and Sax, H. (2018). Virtue-a virtual reality trainer
for hand hygiene. In 2018 9th International Confer-
ence on Information, Intelligence, Systems and Appli-
cations (IISA), pages 1–2. IEEE.
Eley, C. V., Young, V. L., Hayes, C. V., and McNulty, C. A.
(2019). Evaluation of an e-learning platform for edu-
cators to improve education around infection preven-
tion and antibiotics. Technology, Pedagogy and Edu-
cation, 28(5):485–501.
Govindan, B. (2018). Bacterial survivor: an interactive
game that combats misconceptions about antibiotic re-
sistance. Journal of microbiology & biology educa-
tion, 19(3).
Hale, A. R., Young, V. L., Grand, A., and McNulty, C. A. M.
(2017). Can gaming increase antibiotic awareness in
children? a mixed-methods approach. JMIR Serious
Games, 5(1):e5.
Huizenga, J., Ten Dam, G., Voogt, J., and Admiraal, W.
(2017). Teacher perceptions of the value of game-
based learning in secondary education. Computers &
Education, 110:105–115.
Jacob, M. and Wiseman, R. (2020). Can you save the world.
https://martin-jacob.itch.io/can-you-save-the-world.
Accessed: 2020-08-31.
Javora, O., Hannemann, T., St
´
arkov
´
a, T., Voln
´
a, K., and
Brom, C. (2019). Children like it more but don’t learn
more: Effects of esthetic visual design in educational
games. British Journal of Educational Technology,
50(4):1942–1960.
Kang, Y.-S. and Chang, Y.-J. (2019). Using a motion-
controlled game to teach four elementary school chil-
dren with intellectual disabilities to improve hand hy-
giene. Journal of Applied Research in Intellectual Dis-
abilities, 32(4):942–951.
Korchi, A., Dardor, M., Messaoudi, F., and Mabrouk, E. H.
(2020). Progression of a serious game difficulty from
a playful and pedagogical point of view: Analyze and
representation. Education and Information Technolo-
gies, pages 1–11.
Lau, H. M., Smit, J. H., Fleming, T. M., and Riper, H.
(2017). Serious games for mental health: are they ac-
cessible, feasible, and effective? a systematic review
and meta-analysis. Frontiers in psychiatry, 7:209.
Li, M. Y. and Muldowney, J. S. (1995). Global stability for
the seir model in epidemiology. Mathematical bio-
sciences, 125(2):155–164.
Lu, A. S. and Kharrazi, H. (2018). A state-of-the-art sys-
tematic content analysis of games for health. Games
for health journal, 7(1):1–15.
LuluLab (2020). Covid-19 educational game. https:
//lululab.org/educationalgames/covid-19-game. Ac-
cessed: 2020-08-31.
Malik, A., Sabharwal, S., Kumar, A., Samant, P. S., Singh,
A., and Pandey, V. K. (2017). Implementation of
game-based oral health education vs conventional
oral health education on children’s oral health-related
knowledge and oral hygiene status. International
Journal of Clinical Pediatric Dentistry, 10(3):257.
Molnar, A. (2017). Children as agents of change in combat-
ting antibiotic resistance. Journal of health services
research & policy, 22(4):258–260.
Molnar, A. and Kostkova, P. (2018). Learning about hy-
giene and antibiotic resistance through mobile games:
Evaluation of learning effectiveness. In Proceed-
ings of the 2018 International Conference on Digital
Health, pages 95–99.
Nugroho, S. M. S., Utama, A. S., Hariadi, M., Yuhana,
U. L., and Purnomo, M. H. (2018). Heirdom: Mul-
tiple ending scenario game for mathematics learning
using rule-based system. In 2018 International Con-
ference on Computer Engineering, Network and Intel-
ligent Multimedia (CENIM), pages 192–197. IEEE.
Observable (2020). People of the pandemic. https://
peopleofthepandemicgame.com/. Accessed: 2020-
08-31.
Ohannessian, R., Yaghobian, S., Verger, P., and Vanhems, P.
(2016). A systematic review of serious video games
used for vaccination. Vaccine, 34(38):4478–4483.
Suppan, M., Gartner, B., Golay, E., Stuby, L., White, M.,
Cottet, P., Abbas, M., Iten, A., Harbarth, S., and Sup-
pan, L. (2020). Teaching adequate prehospital use
of personal protective equipment during the covid-
19 pandemic: Development of a gamified e-learning
module. JMIR Serious Games, 8(2):e20173.
Tancred, N., Vickery, N., Wyeth, P., and Turkay, S. (2018).
Player choices, game endings and the design of moral
dilemmas in games. In Proceedings of the 2018 An-
nual Symposium on Computer-Human Interaction in
Play Companion Extended Abstracts, pages 627–636.
Taub, M., Azevedo, R., Bradbury, A. E., and Mudrick, N. V.
(2020). 9 self-regulation and reflection during game-
based learning. Handbook of Game-Based Learning,
page 239.
Tuovinen, J. (2020). Unusterra. https://github.com/
jarkkotuovinen/UnusTerra/. Accessed: 2020-08-31.
Wehbe, R. R., Mekler, E. D., Schaekermann, M., Lank, E.,
and Nacke, L. E. (2017). Testing incremental diffi-
culty design in platformer games. In Proceedings of
the 2017 CHI Conference on Human Factors in Com-
puting Systems, pages 5109–5113.
Young, V. L., Brown, C. L., Hayes, C., and McNulty, C. A.
(2019). Review of risk communication and education
strategies around food hygiene and safety for children
and young people.
GRAPP 2021 - 16th International Conference on Computer Graphics Theory and Applications
260
