
Investigating the Impediments to Accessing Reliable, Timely and
Integrated Electronic Patient Data in Healthcare Sites in Uganda
Andrew Egwar Alunyu
1,2 a
, Joseph Wamema
2b
, Achilles Kiwanuka
2c
, Bagyendera Moses
2
,
Mercy Amiyo
2d
, Andrew Kambugu
3e
and Josephine Nabukenya
2f
1
Department of Computer Engineering, Busitema University, Tororo, Uganda
2
Department of Information Systems, Makerere University, Kampala, Uganda
3
Infectious Disease Institute, Makerere University, Kampala, Uganda
Keywords: Data Accessibility and Reliability, Electronic Health Information Systems, Integrated Patient Data.
Abstract: The purpose of collecting patient data is to support their care and wellbeing. Patient-centred care is attained
by securely availing all records about the patient whenever it's necessary to the right persons and at the right
time. However, healthcare providers have often failed to share integrated patient data on time due to
limitations in accessing reliable patient data required to inform care/treatment decisions. This study aimed to
investigate impediments to accessing reliable, timely and integrated patient data through investigating the
processes for collection, analysis, and presentation of data across various healthcare sites in Uganda. A cross-
sectional study design was followed, and data was collected from purposively selected National level
(policymakers) and Sub-national level (health facilities). The field findings indicate various impediments to
accessing patient data including but not limited to inadequate mechanisms for electronic health data collection,
storage and access, non-standardised health data sharing mechanisms, inadequate Health Information System
(HIS) and Information and Communication Technology (ICT) infrastructure, and inadequate skills,
knowledge and training. Other impediments included; insufficient security and privacy measures, weak
eHealth governance, and inadequate management support. Accordingly, these have negatively impacted on
patient data use and quality of patient care in Uganda.
1 INTRODUCTION
Governments in lower-middle and low-income
countries like Uganda have adopted the use of ICT to
improve the delivery of services including healthcare
to all its citizens. Uganda’s eHealth Policy and
Strategy documents have identified unique pillars
necessary to support the successful adoption of ICT
to support healthcare (Ministry of Health, Uganda,
2016). However, reaping the benefits of ICT in
healthcare have continued to face a lot of challenges
including; lack of specific standards on electronic
data collection, storage and sharing, non-
interoperable ICT systems and technologies,
resistance to using ICT to support healthcare, limited
a
https://orcid.org/0000-0003-2957-8423
b
https://orcid.org/0000-0001-6328-7801
c
https://orcid.org/0000-0003-3352-0312
d
https://orcid.org/0000-0002-8172-5382
e
https://orcid.org/0000-0002-3075-0211
f
https://orcid.org/0000-0002-4731-2496
ICT skills and knowledge as well as weak governance
structures ( Ministry of Health, Uganda, 2016; Ross
et al., 2016; Sara, 2016).
These ICT challenges often impact the collection,
sharing, storage, and use of patient data. Patient data
is collected “to create holistic views of patients,
personalize treatments, advance treatment methods,
improve communication between doctors and
patients, and enhance health outcomes”(Sakovich,
2019). To have a complete history of a patient, there
is a need for all medical records/ data to be availed in
an integrated and reliable manner. However,
healthcare providers have often failed to access
patient data on time, even though patient-centred care
requires that all data about a patient is made available
522
Alunyu, A., Wamema, J., Kiwanuka, A., Moses, B., Amiyo, M., Kambugu, A. and Nabukenya, J.
Investigating the Impediments to Accessing Reliable, Timely and Integrated Electronic Patient Data in Healthcare Sites in Uganda.
DOI: 10.5220/0010266705220532
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 522-532
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

on time (Kuipers et al., 2019). Any delay to access a
patient’s data resulting from technology, access rights
or even lack of integration may lead to loss of life.
Besides, patient data may be captured/stored on
different geographically placed eHealth systems. Any
lack of integration of patient data fetched from such
systems may negatively impact healthcare.
Patient care involves the participation of various
stakeholders including healthcare practitioners who
provide care, healthcare organisations who
participate in patient care, decision-makers in
government, the patient’s caretakers and the patients
themselves. Patient data is required by any of them,
anywhere, anytime; thus, the need for integration and
timely access as any delay or lack of integration
would hamper proper care of the patient.
To gain an insight into impediments to accessing
reliable, timely and integrated electronic patient data
in lower-middle and low-income countries. This
study investigated Uganda’s healthcare sites with a
specific focus on the processes for collection,
analysis, and presentation of patient data.
2 METHODS
The study followed a cross-sectional design. The
cross-sectional design provides a snapshot of the
prevalence of the study subjects in a single time point
(Awaisu, et al., 2019).
Sampling Method: Purposive sampling was used
to select both study sites and participants of this
study. The decision to use purposive sampling was
motivated by its ability to support the identification
of all cases that meet a predetermined criterion of
importance (Palinkas et al., 2015) as described below:
Inclusion Criteria for Study Sites: This study
mainly focused on the HIV/TB disease domain of
Uganda’s healthcare system. The HIV/TB disease
domain was adopted because of the heavy reliance on
eHealth systems (i.e Integrated Clinic Enterprise
Application (ICEA) and OpenMRS/UgandaEMR) to
deliver services to clients (Castelnuovo et al., 2012).
Both national and sub-national level health
institutions were used in this study. At subnational
level, 28 health facilities were chosen to participate in
the study. A health facility was chosen as a study site
if it was among the top four health system levels in
Uganda, i.e., National Referral Hospital (NRH),
Regional Referral Hospital (RRH), District Hospital
(DH), and Health Center Fours (HC IVs); and also, if
it was in the Northern, North-Western, Western or
Central regions of Uganda. These regions were
chosen on grounds that they have a high prevalence
of HIV/TB (Ministry of Health, Uganda, 2017)
characterised by high mobility, slum-dwelling, and
limited social support (Central Uganda), urban/rural
populations undergoing significant socio-economic
transformation with an influx of high-risk groups for
HIV transmission (Mid-Western Uganda), low-
prevalence, sparsely populated area but prone to the
influx of refugees .and or internal displacement (West
Nile and Northern regions of Uganda) Additionally,
the sites were chosen if they had adopted and
implemented eHealth systems of some nature. Lastly,
if the site was an Infectious Disease Institute (IDI)
site. Makerere University IDI is a major partner in the
implementation of HIV in Uganda and possess
experience in transitioning from paper-based to
eHealth systems (Castelnuovo et al., 2012). Also, 11
government Ministries, Departments, and Agencies
(MDAs), healthcare organisations, and eHealth
stakeholders like academia, developers and
implementers were included in the study. These were
chosen on the basis that they participated in the
development of the national eHealth strategy/policy
for Uganda, undertaken research in eHealth,
developed/invested in electronic health systems,
implemented electronic health systems among others.
Overall, the study sample size of this study was 196
possible responses from subnational level and 34
respondents from national level.
Inclusion Criteria for Participants: Participants
at health facility level were chosen if they were
officers-in-charge of a health facility,
ICT/Data/Records/M&E Officers, or users of eHealth
in the categories of Clinical Officers, Nurses,
Pharmacist, and Laboratory Technologist.
Participants at the national level were chosen if they
were eHealth Policy Makers, standard/guideline
developers, Health Implementation Partners, Health
Systems and Health Informatics researchers. Only
potential participants who consented to participate in
the study were finally interviewed.
Ethical Consideration: The researchers obtained
consent to assess the study sites from the Ministry of
Health. Ethical clearance was also obtained from the
Institutional Review Board (IRB) of the School of
Public Health, Makerere University.
Data Collection Tools: To obtain representative
views from facility-level and national-level
participants, the study used both interviews and
questionnaires to collect data. Whereas the
questionnaires helped to discover what the eHealth
stakeholders (the masses) think about timely, reliable
and integrated access to patient data; follow-up
interviews were conducted to further authenticate
and/or corroborate their responses (Cohen, 2013).
Investigating the Impediments to Accessing Reliable, Timely and Integrated Electronic Patient Data in Healthcare Sites in Uganda
523

Data Analysis: To analyse quantitative data (i.e.
data collected at the facility level), the researchers
used MS Excel software. Quantitative analysis was
performed to explore the relationships in the collected
data. The results of the quantitative analysis are
presented either statistically or graphically to show
the status quo regarding impediments to accessing
reliable, timely and integrated patient data. The
qualitative data (i.e. majorly collected at national
level) was analysed following the framework method
(Gale et al., 2013). The framework method allowed
the researchers to develop codes, use and categorise
the codes into themes. NVivo 12 was used to assist
and aid the researchers to code and organise the
qualitative data into themes and evidence on
impediments to accessing reliable, timely and
integrated patient data in Uganda.
3 RESULTS
Results of this study are based on 201 responses from
obtained from sub-national and national levels. The
sub-national level response was highest among nurses
(26%) who are the majority users of the ICT,
followed by medical officers (15%), laboratory
(14%), pharmacy (13%), officers-in-charge of health
facilities (11%). Response at the national level is
represented by 6% being health systems and health
informatics researchers, 4% were policymakers from
Ministries, Departments and Agencies (MDAs), and
3% being the Healthcare Development Partners
(HDPs) in Uganda.
Subsequent subsections present the findings
categorized under the three broad themes of
technology-related impediments, inadequate user
skills, knowledge and training on eHealth, and
healthcare organizational environment.
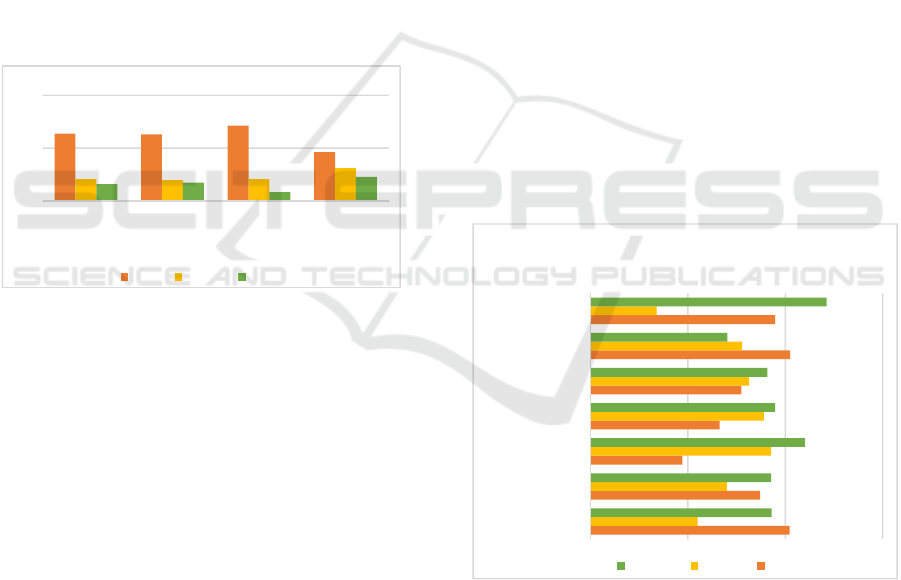
3.1 Technology-related Impediments
a) Mechanisms for Data Handling
Figure 1 shows the views of respondents regarding
the handling (i.e., collection, storage and access) of
patient data at various health facilities across the four
regions that were studied. The responses relate to how
patient data handling processes at health facilities
affect its timely access, reliability and integration.
Limited Training in Electronic Health Data
Classification: On the classification of health data,
81.1% of the respondents agreed that they do classify
the health data during its collection. Much as the
majority of the respondents agreed to classifying
health data during collection, only 40.9% reported
that they had been trained on health data
classification, an indication that they had limited
training in health data classification as expressed by
respondent HSL4-25 … “For me, I was not trained in
coding but I had to learn from a colleague who was
trained by ministry officials.” Lack of proper training
in the classification of health data can affect its
reliability and integration since data collectors are
likely to use different classification codes. When
respondents were asked what challenges were faced
in classifying the health data during its collection,
changing of indicator definitions was mentioned as
the key challenge. In an interview, a respondent said:
“The challenge that we have is that the indicators are
usually changing. You find even the indicators that
are national keep on changing. For example, the
HMIS tools have been revised. We have to be so
adaptive to all the new changes and train people
again. When the staff have just learnt how to capture
the data, new indicators are put in place and so more
training is needed on the new indicators” - HSL2-06.
While another respondent felt the impact of changing
indicators’ definitions as expressed: “Since many of
the tools we use are routinely revised. You find that
the data that was stored five years ago is different
from the data that is currently stored because of the
new indicators. If they add new indictors, they bring
along new registers. Therefore, I am asked to train
the staff on the new registers”- HSL3-01.
Figure 1: Views on Health Data Handling.
Use of Paper-based Data Storage Mechanisms:
To gain an insight into how health data was stored at
respective health facilities, majority of the
respondents (84.8%) reported that this was done. Our
findings indicate that most of the health data was
stored manually (paper-based files), and most times
were incomplete as reported by one respondent:
“Most of our data is in manual files so we keep the
files in the records office that you see there. Some are
incomplete, others are misplaced. They always
81.1
40.9
84.8
78.8
9.8
19.7
10.6
12.1
9.1
39.4
4.5
9.1
Health data is
classified
Adequate
training on
health data
classification
Health data
from the health
facility is
archived
I access
patient’s data
in a timely
manner
Percentage of Respondents (%)
Health data Collection, Storage and Access
(Data Management)
Agree Neutral Disagree
HEALTHINF 2021 - 14th International Conference on Health Informatics
524

present it to us as senior management on every
Thursday but you see a lot of gaps in them when they
are presenting”- HSL2-02.
On how to access the data stored in manual files,
a respondent indicated that it was a tedious exercise
requiring one to go through all the shelves to locate a
file that had a record of interest. A respondent had this
to say: “Filing is one of the trick works. Sometimes,
once in a while someone can interchange the position
of the file and you want to retrieve and you cannot see
it. Maybe by mistake it has been twisted and it has
missed its position. That can make the file a little bit
difficult to be traced.”-HSL4-25. Such a response
evidenced use of poor mechanisms to store health
data, impacting its timely access as well as reliability.
Untimely Access to Health Data: To understand
how well health data is managed at the health
facilities, respondents were asked whether they had
timely access to patients’ data. 78.8% agreed they do.
However, some complained about delay in accessing
patient data as commented by this respondent: “The
only challenge to data access is the workload of the
person who has the data that you need. You may find
that that person has too much work and cannot give
you the data at the time that you need it. You go and
find someone doing other things and may postpone
the time you may access data” – HSL2-04.
b) Non-standardised Health Data Sharing
Mechanisms
To gain an insight into the data-sharing challenges,
this study investigated issues on the guidelines/SOPs
for sharing health data, and how this data was shared
both within and with other health facilities (Figure 2).
Figure 2: Mechanisms for Health Data Sharing.
Existence of Guidelines/SOPs for Sharing
Electronic Health Data: On the existence of
guidelines and/or Standard Operating Procedures
(SOPs) for sharing health data, 64.4% agreed to
existence of guidelines/SOPs for data sharing. The
majority of the respondents who agreed to the
existence of guidelines/SOPs for sharing health data
might not have referred specifically to the use of ICT
to share data, rather to the general guidelines for
health data sharing and exchange such as the data
protection policy, as evidenced by some respondents
who said; as an institution, we have a data protection
policy that guides all staff that are accessing data and
other records” – IP06; “what I know is that data is
confidential and if you are sharing you need to share
with only health workers” – HSL4-26; “There is no
comprehensive SOP” – HSL3-02. However, some
respondents indicated that though their facilities had
SOPs for data sharing, these were not comprehensive
enough and that some had been locally made as
reported by respondents: “There is no comprehensive
SOP” - HSL3-02; “the health sector is sensitive and
you cannot come up with your own SOP and yet
“some of them are locally made”- HSL2-06.
On the issue of guidelines for accessing EMRs,
the respondents had mixed opinions. While 31.8% of
the respondents agreed to the existence of guidelines
for EMR, 42.4% were neutral and 25.8% disagreed.
The respondents who agreed to the existence of the
standards to access EMRs could not provide copies of
such standards as we observed: “It’s not documented
but we know about them”-HSL4-26.
On data sharing within a health facility, 84.8%
agreed that health data was shared. The respondents
who agreed to share data intra-facility referred to the
paper-based mechanism to share health records. For
example, when asked whether they used ICTs to share
health data with another ward or physician within the
health facility, a respondent said: “currently we have
not been using ICT, but we are hoping that it will be
there” – HSL3-06.
On data sharing with other health facilities, 56.1%
of respondents agreed that they do. However, from
the interviews, it was noted that the current nature of
shared data mainly constituted national, monthly and
quarterly reports as evidenced by one respondent who
said: “The information we generate from here is
entered into the District Health Information System
and from there it is transmitted to the ministry. The
partners also use the same system to get their share,
their part of the information. But, at the same time
like for the partners, they come up to the primary
source of the data, they pick it also and then they
compare with what the facility has sent” – HSL4-11.
As much as patient data was shared both within
and outside the health facility, there seemed to be no
agreed mechanism for sharing this health data as
indicated by a respondent in an interview: “We have
to use other things. So, you have to use like WhatsApp
and Facebook, those others, not the government
systems, not the Uganda health system” – HSL4-20.
64.4
31.8
84.8
56.1
19.7
42.4
8.3
13.6
15.9
25.8
6.8
30.3
There is SOP for
moving data
Facility has
guidelines for
accessing EMRs
Intra-Facility
HIE
Inter-Facility
HIE
Percentage of Respondents
(%)
Health Data Sharing
Agree Neutral Disagree
Investigating the Impediments to Accessing Reliable, Timely and Integrated Electronic Patient Data in Healthcare Sites in Uganda
525
c) Insufficient Electronic Health Data Security
and Privacy Measures
The study also investigated the existence of measures
for security and privacy of health data at the health
facilities (that is, safeguards to health data as well as
personally identifiable data as seen in Figure 3). On
the issue of safeguards to health data, 63.6% of
respondents agreed that security measures/controls
had been implemented at the health facilities. This
high percentage could have referred to physical
access to health data storage facilities including ICTs.
In an interview, respondents had this to say: “Physical
security is key, the server environment is secured,
locked with only fingerprint access” - IP03. “specific
people who are using this machine. It’s not everybody
who accesses it and even we lock also the computers
and even as I told you we have the security guards we
have two that makes our information safe” – HSL4-
18. “Not everyone enters the records room. All the
cabinets are lockable” – HSL4-22.
Figure 3: Data Security and Privacy Measures.
On whether security controls had been
implemented in the ICTs that are used at the health
facilities, 62.9% agreed that this had been done.
Respondents could have interpreted security to mean
the presence of passwords that are used to access
computers as evidenced by the interview responses:
“There is a password in this EMR. A person who is
logging in is given account so you log in using their
account. And the account is not given to all. And the
access right is not given to all the people”-HSL4-13;
“Here like on my computer, we have password that
not everyone has access to”-HSL3-03; and “In
softcopies there is passwords which I normally put
there and people cannot access the data”-HSF4-18.
However, only 46.2% agreed that information
security controls were sufficient. Those who
disagreed (22.7%) or were neutral (31.1%) could
have represented respondents from health facilities
where security breaches had been experienced. From
the interviews, respondents said; “we have
experienced theft of computers like regional referral
in October they lost about ten computers.” - HSL4-
25; “Yes, some thieves have ever broken in the
facility, although the computers were recovered. if
his place can be faced maybe the issue of security
would be solved and also we might need more
security guards to guard the facility”-HSL4-30.
Concerning personally identifiable data, 71.2% of
respondents agreed that this data is hidden which is
an indication that measures to ensure the privacy of
personally identifiable data had been implemented.
This high percentage of respondents who agreed
could be attributed to the need to protect information
as confirmed by 80.3% of respondents who said that
the health data they collect is valuable.
d) Inadequate HIS and ICT Infrastructure
Respondents were asked to give their views on the
suitability of existing HISs and supporting
infrastructure in Uganda’s top four health system
levels to deliver access to quality and timely health
data. The questions asked related to the relevance of
the applications to support healthcare work routines,
use of eHealth applications and/or technologies,
characteristics that make the application suitable, and
technology infrastructure to support access to
patients’ data in a reliable, timely, and integrated
manner (Figure 4).
Figure 4: Characteristics of eHealth applications/
technologies used in healthcare facilities.
Apprehension to using ICT in Healthcare:
Results show that although a majority of the
respondents agreed on the compatibility of existing
technologies with work routines (40.9%) and ability
of eHealth applications to enhance productivity
(41%); they disagreed or remained neutral on the rest
63.6
62.9
71.2
46.2
20.5
19.7
20.5
31.1
15.9
17.4
8.4
22.7
Security
controls are
implemented
Existing ICTs
are secure and
privy
Personal
identifiable
data is hidden
Security
controls are
sufficient
Percentage of Respondents
(%)
Data Security and Privacy
Agree Neutral Disagree
40.9
34.8
18.9
26.5
31
41
37.9
22
28
37.1
35.6
32.6
31.1
13.6
37.2
37.1
44
37.9
36.3
28.1
48.5
Compartibility with
work routines
Easy to Learn
Erro Free
App is Intergratble
App provides
Relevant Data
App enhances
Productivity
Adequate ICT
Infrastacture
Percentage of Respondents (%)
Characteristics of eHealth
Applications/Technologies currently used to
support healthcare services in Uganda
Disagree Neutral Agree
HEALTHINF 2021 - 14th International Conference on Health Informatics
526

of the characteristics indicative of existing
apprehension/challenges to using ICT in healthcare.
Insufficient Training in the use of eHealth
Applications/Technologies: On the question of
whether the eHealth applications that they used were
easy to learn, respondents had mixed reactions with
34.8% in agreement, 28% neutral and 37.1%
disagreed. The negative responses concerning the
ease of use of the eHealth applications could have
been a result of the varied training capacities, that is,
while some were trained by the funders/investors,
others did not receive any training as evidenced from
the interview responses; “We are given the system
with the database and they are national. We are
trained on how to use it” – HSL4-24; on the contrary,
a respondent said: “No I just trained myself” – HSL4-
08; while another respondent said: “All those who
work on these computers struggle with some few days
of training, say like in Uganda EMR” – HSL3-05.
Characteristics of the HIS Applications that are
used: Respondents were asked to give their opinions
on the characteristics of the eHealth applications that
they use. On whether the applications were error-free,
only 18.8% agreed. This meant that the reliability of
the applications' data could be queried. This could be
the reason 37.1% disagreed with the relevancy of data
provided by these eHealth / HIS applications.
When asked whether the eHealth applications
used within the health facilities can integrate with
other eHealth applications outside of the health
facilities, there were mixed responses; 37.9% of
respondents disagreed, 35.6% remained neutral, and
26.5%agreed. Those who remained neutral and
disagreed may represent respondents that had a
limited understanding of the functionalities of the
eHealth applications that were being used at the
health facilities. Generally, the respondents did not
commit to the suitability of the eHealth applications
that they used to access health data on time. In one of
the respondents’ own words he said: “I would
actually recommend that if there is need to introduce
any other system, it should be a system that is safe,
effective, fast which can help us access what we need
in a timely manner. If we can at least get a system
which is quick, effective and convenient with no
interruptions, it would be better” – HSL2-04.
Poor eHealth Infrastructure: On whether the
health facilities had adequate eHealth infrastructure
to support timely access to patient data, 48.5% of
respondents reported that hardware and application
technologies that support eHealth were not sufficient
to support healthcare processes that relate to
collection and analysis of health data. The
respondents’ views ranged from inadequate ICT
devices e.g. “lack of enough systems in place like the
workstations. You find you may have like 3 computers
to serve all this large number of 12000 clients.” –
HSL2-04); poor electric power e.g. “we have power
challenges. we find that at times there is power
fluctuation and our backups at times are not so
reliable. We have a backup generator but at times
there is no fuel.” – HSL2-06); poor maintenance e.g.
“The few gadgets around have a challenge of
maintenance costs and so maintenance being a
problem” -HSL4-32); and intermittent network
connectivity and/or lack of mobile data e.g., “The
challenge I have experienced for a while has been
internet connectivity. Sometimes you are supposed to
send reports when there is no data on the modem” –
HSL2-01) among others.
3.2 Inadequate Skills, Knowledge and
Training on eHealth
This study also sought for respondents’ views on the
expertise, confidence and training on using eHealth
(Figure 5). On confidence and control when using
eHealth, only 31.1% of respondents agreed that they
were confident when using eHealth applications. The
low percentage of respondents who agreed to be
confident when using eHealth may be attributed to
limited experience and expertise in eHealth usage.
Less than half (42.4%) of respondents agreed that
they had experience and expertise in using eHealth.
The low percentage of those who agreed that they had
experience and expertise in the use of eHealth may
also be attributed to insufficient training (52.3%), as
evidenced by some respondents: “… challenge is the
human resource. They are yet to train our people to
know how to use it” – HSL2-02; “it is a new system
which has come up. You know it comes with some
challenges if one is having a knowledge gap” –
HSL2-05; and “ICT skills are inadequate/lacking
among healthcare workers”– RI01.
Figure 5: Capacity in using eHealth Applications/
Technologies in Healthcare Processes.
42.4
31.1
28
23.5
25.8
19.7
34.1
43.2
52.3
Adequate expertise in
eHealth
Confidence & control
using eHealth
application
Trained to use the
eHealth application
Percentage of Respondents
(%)
Use skills and knowledge
Agree Neutral Disagree
Investigating the Impediments to Accessing Reliable, Timely and Integrated Electronic Patient Data in Healthcare Sites in Uganda
527

The limitations of user skills and knowledge by
health practitioners may be a result of failure to
incorporate ICT skills in most of the curriculum of
healthcare professionals as mentioned by some
respondents who said: “inadequate integration of
eHealth skills into existing health professional
training curricula”-IP04; and “Not everyone in the
ART clinic is computer literate. It is only the health
information assistant who is well trained in computer
skills” – HSL4-15. Some universities and tertiary
institutions have however started training healthcare
professionals in ICTs skills as mentioned by a
respondent: “ICT skills related to eHealth are
inadequate, both in terms of the numbers and skills
mix/set. However, situation though is much better
now than it was 5 years or more ago. Some training
institutions has trained healthcare professionals who
understand ICT” - IP04.
3.3 Healthcare Organizational
Environment
To further understand how the healthcare
environment can impact on access to reliable, timely,
and integrated data, this study also investigated the
governance factors including governance of ICT for
healthcare and management support for the
implementation and operation of eHealth (Figure 6).
Figure 6: eHealth governance factors that affect eHealth
data management.
Weak eHealth Governance - On the governance
of eHealth, this study mainly focused on planning for
eHealth, coordination of eHealth implementation and
compliance monitoring. The majority of the
respondents (52.3%) reported that management is
involved in the preparation of eHealth
implementation plans and that there is coordination
with implementation agencies (60.6%). These
findings indicate that there is some kind of framework
that is followed to govern the implementation of
eHealth in Uganda. However, our findings indicate
that the framework has not yet been documented as
evidenced by one respondent: “let’s say there is a
framework but at the time we developed ICEA, it
wasn’t necessarily written down. It’s just that we all
knew that the system we wanted to develop would
address the institutions need, the funders need, and
the MOH requirement. So that was the framework,
but that framework was in our mind, I don’t think it
was explicitly laid down somewhere at that time”-
IP05. Lack of a well-documented implementation
framework was further echoed by respondents:
“There are insufficient governance structures to
guide the development of eHealth across the health
sector” –R101; and that “There is insufficient
coordination and participation of partners in public-
private-partnerships in promoting ICT in the health
sector”-PM04.
On the existence of monitoring structures, 34.8%
agreed, 37.1% remained neutral and 28% disagreed.
Also, on monitoring compliance with ICT guidelines,
30.3% agreed that this is done, 35.6% remained
neutral, while 34.1% disagreed. These results show
that a higher number of respondents remained neutral
on the existence of monitoring structures as well as
compliance with ICT guidelines. This may signify the
lack of awareness of eHealth governance structures at
the health facilities level. It is evident by the fact that
despite more respondents agreeing on the existence of
monitoring structure (34.8%), a significant number
said it is not monitored (34.1%). Most users of
eHealth comply because it is mandatory; however,
with “limited/lack of a monitoring system in place” –
RI01, the compliance is compromised.
Inadequate Management Support - Results
from this study (Figure 7) show that management at
the health facilities provides resources and support for
use of the eHealth (50.7%). This may be attributed to
the management’s awareness of the benefits of
eHealth (69.7%). Support for eHealth by
management was echoed by some respondents as
evidenced in their own words: “Management, their
level has done best to ensure that possible request has
been met in terms of the ICT tools. The computers and
these all come through them” – HSL2-01;
“Management has always been supportive in the use
of electronic systems, electronic data. How are they
supportive? Right now, if you can see there is a lot of
investment being done in purchase of these electronic
systems” – HSL3-01; and “The management has
helped us in funding our trainings, when we have
been called for training because the training focus on
the use of the software system or the software we have
been using for the medical management”-HSL2-01.
52.3
60.6
34.8
30.3
28.8
20.5
37.1
35.6
18.9
18.9
28
34.1
Mgt prepares
eHealth
implemention
plan
Coordination by
implementing
agencies
A monitoring
structure exists
Compliance
with ICT
guidelines is
monitored
Percentage of Respondents
(%)
eHealth Governance
Agree Neutral Disagree
HEALTHINF 2021 - 14th International Conference on Health Informatics
528

Figure 7: Role of Management to Support Implementation
and Use of eHealth Applications.
These responses could mean that there is suitable
eHealth implementation and its use; however, gaps
remain as only 42.4% agreed that management
effectively address eHealth applications challenges.
Although 60.6% of respondents agreed that there
were good communication and coordination among
eHealth implementing agencies, 18.9% disagreed.
The few who disagreed argued that there is still
“insufficient coordination and participation of
partners in public-private-partnerships in promoting
ICT in the health sector”-PM04. The limitation in
communication and or coordination may be attributed
to governance factors including structures to oversee
implementation and compliance to standards as
reported by some respondents: “Insufficient
governance structures to guide the development of
eHealth across the health sector” – PM04;
“Limited/lack of monitoring system in place” – RI01;
and “I believe the regulatory framework is still in its
infancy stage and therefore generally still lacking; it
needs to become better developed, coordinated and
enforced” – IP07.
4 DISCUSSION
In Uganda, we observed that numerous EMR-based
electronic Health Information Systems(eHIS)
initiatives including OpenMRS/ UgandaEMR, ICEA,
DHIS2, OptionB+ were being used in the
management of HIV and TB patients (Ministry of
Health, Uganda, 2016). Despite their existence, our
findings evidence various impediments to accessing
reliable, timely and integrated patient data from
existing eHIS as discussed below:
Insufficient Mechanisms for the Collection,
Storage and Access to Electronic Health Data –
Collecting healthcare data generated across a variety
of sources encourages efficient communication
between doctors and patients, and increases the
overall quality of patient care providing deeper
insights into specific conditions. The way health data
is collected and stored has a bearing on its access,
reliability and ability to integrate. For example,
“during the move from a paper record or from one
computerized system to another, records can be
misplaced or incorrectly added to a patient’s record”
(Rodziewicz & Hipskind, 2020) affecting the
reliability of the patient data. The study identified
limited training in electronic health data classification
and use of paper-based data storage mechanisms as
specific impediments to the process of electronic data
handling in Uganda’s health system affecting
integrated and timely access to patient data across
health facilities. Therefore, first-line eHealth
technology users (data collectors) and the
eHISs/applications or technologies need to capture,
process and present accurate data.
Inadequate and Unsuitable HIS and ICT
Infrastructure – eHealth has been recognized to
have tremendous potential for managing patient
health data (Barello et al., 2016). eHIS and/or
applications allow the development of reliable and
integrated patient data and promote effective
exchanges among the actors involved in the
healthcare process (Khubone et al.,2020). However,
existing eHealth applications have errors, lack useful
data, and cannot be easily integrated with data from
other applications. This is a design-reality gap.
eHealth success or failure largely depends on the size
of the gap that exists between current realities and the
design of the application (Anthopoulos et al., 2016;
Ishijima et al., 2015) which user-centred participatory
design can remedy (Williams & Coles-Kemp, 2014).
Also, facilitating infrastructure should be
adequate to support capture, analysis, storage, sharing
and presentation of health data (Aanestad et al.,
2017). However, findings revealed few and poorly
maintained infrastructural resources that may be slow
and unable to support the timely and integrated
sharing of health data. Current modes of health data
communication include the sharing of text, images,
audio, and video (Al-Safadi, 2016) requiring the
supporting eHealth infrastructure to be fast, flexible,
large, reliable and with appropriate security and
privacy measures (Aanestad et al., 2017). The poor
state of the eHealth applications and infrastructure
could have led to apprehension among some of the
target users of eHealth in Uganda to use ICT in
46.3
60.6
50.7
42.4
69.7
25
20.5
25.8
31.1
20.5
28.8
18.9
23.4
26.6
9.8
There is strong eHealth governance at
the health facility
There is good communication and
coordination among eHealth
implementing agencies
Management provides necessary
resources and support for use eHealth
Management effectively address
emerging challenges to eHealth
application
Management is aware of the benefits of
eHealth
Percentage of Respondents (%)
Role of Management
Disagree Neutral Agree
Investigating the Impediments to Accessing Reliable, Timely and Integrated Electronic Patient Data in Healthcare Sites in Uganda
529

support of healthcare processes contributing
additional challenges to timely access to patient data
(Ministry of Health, Uganda, 2016).
Inadequate eHealth Skills and Knowledge –
although eHealth has become an integrated part of
modern healthcare (Bedeley & Palvia, 2014; Gregory
& Tembo, 2017), a range of individuals within
healthcare experience challenges of using and
benefiting from the technology (Furstrand & Kayser,
2015). For eHealth to be valuable in providing timely,
accessible and integrated health data, users must have
the necessary skills and understanding (Standing &
Cripps, 2015). However, this study showed that there
was a lack of sufficient skills and knowledge to use
eHealth applications as represented by 52.3 % who
claimed that they were not trained in the use of
eHealth. Without proper skills and knowledge,
healthcare providers are likely to find difficulty in
accessing healthcare information to make good
medical decisions (Hoque et al., 2014). Availability
of a skilled workforce that understands healthcare and
ICT is a critical success factor (Standing & Cripps,
2015). That can be achieved through training and
demonstrating the benefits of eHealth (Alunyu et al.,
2020; Hoque et al., 2014; Were et al., 2015).
Insufficient Electronic Health Data Security
and Privacy Measures – The study findings show
three broad security and privacy concerns, i.e.,
limited understanding of ICT security and privacy
measures, lack of policies specific to security and
privacy of health data, and full implementation and
enforcement of security and privacy measures to
include both physical and electronic security. The
right of individual patients to nondisclosure of their
health information (privacy) and mechanisms in place
to protect privacy (security) may directly or indirectly
contribute to reliable, timely and integrated access to
patient's health data/information (Sahama et al.,
2013). Privacy in healthcare settings refers to
people’s right to control access to their personal
information (Kumar & Wambugu, 2016). Security,
on the other hand, refers to the mechanisms put in
place to safeguard health information and health
information systems from unauthorised access,
modification and denial of service to authorised users
(Kumar & Wambugu, 2016). For providers and
individuals to adopt eHealth, they must trust the
security and privacy of their electronic health
information (Sahama et al., 2013). If patients feel that
the eHealth systems are not secure, they may not use
them to share their health information with healthcare
providers. This has a negative bearing on timely
access to patient information for decision making by
providers.
Non-standardised Health Data Sharing
Mechanisms – Mukasa et al., (2017) recommends
that organisations who intend to share data should
deploy standards as part of their integration efforts.
The purposes of the standards are; to ensure proper
and integratable data formats are captured, those
participating in sharing of health data/information
adhere to a set of rules that govern exchange, only the
right persons have access to a patient’s data, and
security and privacy of patient information are
protected (Adebesin et al., 2013; ITU-T, 2012;
Mukasa et al., 2017). However, our study findings
show that although there are SOPs for sharing of
health information, they are not comprehensive
enough to guide patient data sharing; and procedures
for accessing EMRs are not documented or
documentation is not widely shared. These
shortcomings are a hindrance to timely access or
electronic sharing of patient data. This study suggests
that future development or review of standards for
eHealth should include health facility level users as
part of the stakeholders involved in the development
and/or review of the standards. Furthermore, the
standards for eHealth should be widely provided and
disseminated among all eHealth implementing
agencies and developers.
Organizational Healthcare Environment – in
this study, eHealth governance and leadership, legal
and regulatory frameworks as well as standards have
been reported as key to successful utilization of
eHealth (Hoque et al., 2014; Ishijima et al
., 2015;
Ross et al., 2016). Without an enabling organization
healthcare environment, it may be difficult to
successfully utilize eHealth to realize timely, reliable
and integrated health data (Palabindala et al., 2016).
However, our study findings indicate that there are
insufficient governance structures within Uganda’s
health system to monitor the implementation of
eHealth as well as compliance to standards.
Healthcare is a sensitive domain. If some eHealth
application is going to be used to handle data, proper
governance, as well as procedures and rules, need to
be devised and followed to ensure safe practices of
healthcare services; otherwise, it could lead to serious
consequences. Although the Government of Uganda
has some guidelines and policies in place, the
regulatory and legal framework has not yet been
modernized and or operationalised at health facility
level. This study, therefore, recommends that the
Ministry of Health creates structures at facility level
to oversee the implementation and use of eHealth.
HEALTHINF 2021 - 14th International Conference on Health Informatics
530

5 CONCLUSIONS
This study investigated the impediments to accessing
reliable, timely, and integrated electronic patient data
in healthcare sites in Uganda’s health system.
Findings show the key impediments ranging from
unsuitable mechanisms for electronic health data
collection, storage and access; non-standardised
health data sharing mechanisms; inadequate HIS and
ICT infrastructure; inadequate skills, knowledge and
training; to insufficient security and privacy
measures. Other impediments include weak eHealth
governance and inadequate management support for
eHealth. To mitigate these challenges and attain the
full benefits of eHealth, our future work will generate
requirements that must be met to improve access to
reliable, timely and integrated patient data in the
healthcare sites. The requirements will act as inputs
to the development of contextualised eHealth
standards and an eHealth Enterprise Architecture to
digitally-enable, standardize, implement and use
eHealth in healthcare and service in Uganda.
ACKNOWLEDGEMENTS
We acknowledge the Government of the Republic of
Uganda through Makerere University Research and
Innovation Fund for sponsoring the study; and thank
the study participants at the national and sub-national
levels in Uganda’s health system for participating
effectively in the study.
REFERENCES
Aanestad, M., Grisot, M., Hanseth, O., & Vassilakopoulou,
P. (2017). Strategies for Building eHealth
Infrastructures. In M. Aanestad, M. Grisot, O. Hanseth,
& P. Vassilakopoulou (Eds.), Information
Infrastructures within European Health Care: Working
with the Installed Base (pp. 35–51). Springer
International Publishing. https://doi.org/10.1007/978-
3-319-51020-0_4
Adebesin, F., Kotze, P., Foster, R., & Van Greunen, D.
(2013). A Review of Interoperability Standards in E-
health and Imperatives for their Adoption in Africa.
South African Computer Journal, 50(1), 55–72.
Al-Safadi, L. (2016). The effects of real-time interactive
multimedia teleradiology system. BioMed Research
International, 2016.
Alunyu, A. E., Munene, D., & Nabukenya, J. (2020).
Towards a Digital Health Curriculum for Health
Workforce for the African Region: A Scoping Review.
Journal of Health Informatics in Africa, 7(1), 38–54.
https://doi.org/10.12856/JHIA-2020-v7-i1-265
Anthopoulos, L., Reddick, C. G., Giannakidou, I., &
Mavridis, N. (2016). Why e-government projects fail?
An analysis of the Healthcare. gov website.
Government Information Quarterly, 33(1), 161–173.
Awaisu, A., Mukhalalati, B., & Mohamed Ibrahim, M. I.
(2019). Research designs and methodologies related to
pharmacy practice. Encyclopedia of Pharmacy Practice
and Clinical Pharmacy, 7.
Barello, S., Triberti, S., Graffigna, G., Libreri, C., Serino,
S., Hibbard, J., & Riva, G. (2016). eHealth for patient
engagement: A systematic review. Frontiers in
Psychology, 6, 2013.
Bedeley, R., & Palvia, P. (2014). A study of the issues of E-
health care in developing countries: The case of Ghana.
Castelnuovo, B., Kiragga, A., Afayo, V., Ncube, M.,
Orama, R., Magero, S., Okwi, P., Manabe, Y. C., &
Kambugu, A. (2012). Implementation of provider-
based electronic medical records and improvement of
the quality of data in a large HIV program in Sub-
Saharan Africa. PloS One, 7(12), e51631.
Cohen, L. (2013). Research Methods in Education (7th ed.).
Routledge. https://doi.org/10.4324/9780203720967
Furstrand, D., & Kayser, L. (2015). Development of the
eHealth Literacy Assessment Toolkit, eHLA. MedInfo,
971.
Gale, N. K., Heath, G., Cameron, E., Rashid, S., &
Redwood, S. (2013). Using the framework method for
the analysis of qualitative data in multi-disciplinary
health research. BMC Medical Research Methodology,
13(1), 1–8.
Gregory, M., & Tembo, S. (2017). Implementation of e-
health in developing countries challenges and
opportunities: A case of Zambia. Science and
Technology, 7(2), 41–53.
Hoque, M. R., Mazmum, M. F. A., & Bao, Y. (2014). e-
Health in Bangladesh: Current status, challenges, and
future direction. The International Technology
Management Review, 4(2), 87–96.
Ishijima, H., Mapunda, M., Mndeme, M., Sukums, F., &
Mlay, V. S. (2015). Challenges and opportunities for
effective adoption of HRH information systems in
developing countries: National rollout of HRHIS and
TIIS in Tanzania. Human Resources for Health, 13(1),
1–14.
ITU-T. (2012). E-health Standards and Interoperability.
Kuipers, S. J., Cramm, J. M., & Nieboer, A. P. (2019). The
importance of patient-centered care and co-creation of
care for satisfaction with care and physical and social
well-being of patients with multi-morbidity in the
primary care setting. BMC Health Services Research,
19(1), 1–9. https://doi.org/10.1186/s12913-018-3818-y
Kumar, M., & Wambugu, S. (2016). A Primer on the
Privacy, Security, and Confidentiality of Electronic
Health Records A Primer on the Privacy, Security, and
of Electronic Health Records. February.
Ministry of Health, Uganda. (2016). Uganda National
eHealth Strategy 2016/2017—2020/2021.
Investigating the Impediments to Accessing Reliable, Timely and Integrated Electronic Patient Data in Healthcare Sites in Uganda
531

Ministry of Health, Uganda. (2017). Uganda Population-
Based HIV Impact Assessment (UPHIA) 2016–2017.
MOH Uganda.
Mukasa, E., Kimaro, H., Kiwanuka, A., & Igira, F. (2017).
Challenges and strategies for standardizing information
systems for integrated TB/HIV services in Tanzania: A
case study of Kinondoni municipality. The Electronic
Journal of Information Systems in Developing
Countries, 79(1), 1–11.
Palabindala, V., Pamarthy, A., & Jonnalagadda, N. R.
(2016). Adoption of electronic health records and
barriers. Journal of Community Hospital Internal
Medicine Perspectives, 6(5), 32643.
Palinkas, L. A., Horwitz, S. M., Green, C. A., Wisdom, J.
P., Duan, N., & Hoagwood, K. (2015). Purposeful
sampling for qualitative data collection and analysis in
mixed method implementation research. Administra-
tion and Policy in Mental Health and Mental Health
Services Research, 42(5), 533–544.
Rodziewicz, T. L., & Hipskind, J. E. (2020). Medical Error
Prevention. In StatPearls. StatPearls Publishing.
http://www.ncbi.nlm.nih.gov/books/NBK499956/
Ross, J., Stevenson, F., Lau, R., & Murray, E. (2016).
Factors that influence the implementation of e-health:
A systematic review of systematic reviews (an update).
Implementation Science, 11(1), 146. https://doi.org/
10.1186/s13012-016-0510-7
Sahama, T., Simpson, L., & Lane, B. (2013). Security and
Privacy in eHealth: Is it possible? 2013 IEEE 15th
International Conference on E-Health Networking,
Applications and Services (Healthcom 2013), 249–253.
Sakovich, N. (2019, April 9). The Importance of Data
Collection in Healthcare and Its Benefits. https://www.
sam-solutions.com:443/blog/the-importance-of-data-
collection-in-healthcare/
Sara, H. (2016, August 11). Top Three Challenges Limiting
Patient Access to Health Data. PatientEngagementHIT.
https://patientengagementhit.com/news/top-3-
challenges-limiting-patient-access-to-health-data
Standing, C., & Cripps. (2015). Critical success factors in
the implementation of electronic health records: A two‐
case comparison. Systems Research and Behavioral
Science, 32(1), 75–85.
Were, M. C., Siika, A., Ayuo, P. O., Atwoli, L., & Esamai,
F. (2015). Building comprehensive and sustainable
health informatics institutions in developing countries:
Moi University experience.
Williams, P., & Coles-Kemp, L. (2014). The changing face
of ehealth security. Electronic Journal of Health
Informatics, 8(2).
HEALTHINF 2021 - 14th International Conference on Health Informatics
532
