
Epidemiological and Prognostic Factors Related to COVID-19 in
Primary Care in a Municipality in Southern Brazil
Luís Rafaeli Coutinho
1 a
, Lecian Cardoso Lopes
2 b
, Henrique Pereira Oliveira d’Eça Neves
3 c
,
Hidelbrando Rodrigues
4 d
, Sibele Holsbach Costa
5 e
and Fábio Sensever
6 f
1
Family Health Support Center of the Municipal Health Department, Porto Belo, Brazil
2
Universidade Regional de Blumenau, Blumenau, Brazil
3
Centro Universitário Municipal de São José, São José, Brazil
4
Universidade Federal do Amazonas Itacoatiara, Brazil
5
Family Health Support Center of the Municipal Health Department, Florianópolis, Brazil
6
Family Health Strategy of the Municipal Health Department, Porto Belo, Brazil
Keywords: COVID-19, SARS-COV-2, Telehealth.
Abstract: The COVID-19 pandemic crisis led to a reflection on health systems in general, addressing the importance
not only of equitable, but also universal, care to populations in a global context. Numerous ways to identify
and propose alternatives to COVID-19 issues are enabled by technological advances, specifically those
applied to health. This study aimed to investigate COVID-19-related epidemiological and prognostic factors
remotely in primary care in the Brazilian public health system. The sample consisted of 77 users of primary
care who had records of respiratory symptoms during the pandemic, aged between 5 and 83 years. The
study was carried out in 07 Health Centers in Porto Belo (SC), Brazil. Data analysis and subsequent
evaluation found a possible demand with symptoms and sequelae of COVID-19 that was shown mainly by
users who reported difficulty or
“tiredness” in basic Activities of Daily Living (ADLs) and Instrumental
Activities of Daily Living (IADLs), which may result in patients with chronic muscle fatigue and dyspnea
as a future demand in the municipality.
a
https://orcid.org/0000-0003-0367-8637
b
https://orcid.org/0000-0003-4439-6193
c
https://orcid.org/0000-0003-0000-5197
d
https://orcid.org/0000-0003-1266-0957
e
https://orcid.org/0000-0001-9358-2094
f
https://orcid.org/0000-0003-1632-8134
1 INTRODUCTION
Since December 2019, a new coronavirus-infected
pneumonia (SARS-CoV-2) (COVID-19) has
emerged in Wuhan and has spread rapidly
throughout China (MO, 2020). The coronavirus
disease 2019 (COVID-19) is caused by SARS-COV-
2 and refers to the causative agent of a potentially
fatal disease that has resulted in a major concern for
global public health (Rothan; Byrareddy, 2020).
The epidemic then expanded to an increasing
number of countries, some of which have reported
progressive transmission. There is an urgent need to
expand activities in public health to clarify the
epidemiology of the new virus and characterize its
potential impact (Lipsitch; Swerdlow; Finelli, 2020).
Broad measures have been implemented to reduce
COVID-19 person-to-person transmission and
control the current outbreak. Special attention and
efforts are required to protect or reduce transmission
in susceptible populations, including children,
healthcare professionals and the elderly (Rothan;
Byrareddy, 2020).
Scientists from around the world work tirelessly
while information on transmission, the mechanisms,
clinical spectrum of the disease, new diagnoses and
prevention and therapeutic strategies are being
developed. Preventive strategies are focused on
patient isolation and careful infection control,
Coutinho, L., Lopes, L., Neves, H., Rodrigues, H., Costa, S. and Sensever, F.
Epidemiological and Prognostic Factors Related to COVID-19 in Primary Care in a Municipality in Southern Brazil.
DOI: 10.5220/0010265705150521
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 515-521
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
515

including measures to be taken during diagnosis and
provision of clinical care to the infected patient
(Cascella et al, 2020).
In response to COVID-19, many countries are
using a combination of containment and mitigation
activities in order to delay large outbreaks of
patients. Response strategies include various levels
of tracking and self-isolation or quarantine, in
addition to promoting public health measures. Some
countries should consider a combination of response
measures, and monitoring of cases and contacts.
These measures should include public awareness,
promotion of personal hygiene and protection,
preparation of health systems for a wave of critically
ill patients, stronger infection prevention and control
in health facilities, nursing homes and long-term
care facilities, and postponement or large-scale
cancellation of public meetings (Bedford et al,
2020).
COVID-19 changed the practice of palliative
care and clinical medicine as we know it. In this
context, telehealth emerged as a technology capable
of providing medical care to patients at a critical
moment, as a way of trying to reduce the
transmission of COVID-19 between patients,
families and healthcare professionals. However,
ensuring equitable access and accessible means of
telemedicine technology for vulnerable populations,
through creative solutions, has become a necessary
challenge in preserving scarce resources, especially
in developing countries (Calton; Albedini; Fratkin,
2020).
Integrated mobile health programs allow patients
to be treated at home, with virtual top-level medical
support. Other health professionals (e.g. as nurses,
physiotherapists, and medical assistants) also
contribute to telehealth, allowing continuous care for
patients during the pandemic (Hollander; Carr,
2020).
The prevention and control of COVID-19 is
extremely important due to the rapid increase in
confirmed cases (Zheng et al, 2020). Therefore,
some measures are recommended, such as the close
monitoring of changes in local epidemiology and the
effectiveness of public health with strategies and
their social adherence. As well as contact tracking
and health monitoring, in addition to specific
guidelines in health facilities and support for
individual preventive measures. In addition to health
control with continued surveillance activities and
restrictions imposed on the population. Monitoring
the health of symptomatic individuals is also
suggested through remote health consultation by
phone or online and providing essential vital support
for emergency services, if required (Heymann;
Shindo, 2020).
Healthcare professionals must be protected from
SARS-CoV-2 infection during clinical care. In this
context, telehealth has become necessary and
reduces the number of health professionals who
interact with infected patients (Gandhi; Lynch; del
Rio; 2020). This study aimed to investigate COVID-
19-related epidemiological and prognostic factors
remotely in public primary care.
2 METHODS
The sample consisted of 77 users of primary care
who had records of respiratory symptoms during the
pandemic, aged between 5 and 83 years. The study
was carried out in 07 Health Centers in Porto Belo-
SC (Brazil), which are among the 08 Primary Health
Units (UBS) in the municipality. Data were
collected between September 22 and 30, 2020.
A form was developed on Google Forms in order
to identify epidemiological and prognostic factors
related to COVID-19 infection. The questionnaire
included questions on demographic, epidemio-
logical, clinical and laboratory aspects for COVID-
19 and was developed for each UBS. An initial
telephone contact was made to explain the
procedures that would be performed and the form of
access, then a link was provided to answer the
questions. The link included information on the
work, its relevance and how it would be conducted,
following the completion of the study form provided
via WhatsApp. Data was collected through Google
Forms and then introduced in Excel spreadsheets for
further analysis.
This study was approved by the Research Ethics
Committee of the UDESC – Universidade do Estado
de Santa Catarina, based on the Resolution 466/12,
which defines the Guidelines and Regulatory
Standards for Research involving Human Beings
under no. 4,268,895.
3 RESULTS
Telemedicine is a proven and consolidated way to
provide care to the most vulnerable people. Now,
caring for people and their families requires strict
social distancing measures to protect patients and all
health staff. Therefore, creative ways are required to
ensure that all patients have equal access to this
valuable resource, including the poorest and most
HEALTHINF 2021 - 14th International Conference on Health Informatics
516
vulnerable individuals. Even though through
outdated technology, people who do not have access
to the most advanced technologies need access to
health care (Calton; Albedini; Fratkin, 2020).
The study collected information from 77
individuals in 7 (seven) Primary Health Units in
Porto Belo (SC). Porto Belo is located in the
southern region of Brazil, in the state of Santa
Catarina, with a territorial area of 93,673 km², an
estimated population of 21,932, demographic
density of 171.77 inhabitants/km² and MHDI
(Municipal Human Development Index) of 0.760
(IBGE, 2019).
Choices are required during the epidemic on the
interventions to be carried out and under what
circumstances. The early start of surveillance
activities will allow to select the most efficient ways
to fight the epidemic and avoid interventions that
may be unnecessarily expensive or overly restrictive
(Lipsitch; Swerdlow; Finelli, 2020).
A tool with a standard screening questionnaire
recommended by the Ministry of Health of Brazil
(202a and 2020b) was developed in Google Forms
to assist in the telemonitoring of symptomatic
respiratory patients, including questions about
influenza-like illness, comorbidities and questions
about COVID-19 (appendix). The links of the
referred medical record were submitted by the teams
to the patients of each Primary Health Unit
according to their territory. The monitoring
instrument was provided via WhatsApp, thus
providing an effective and easy tool for family
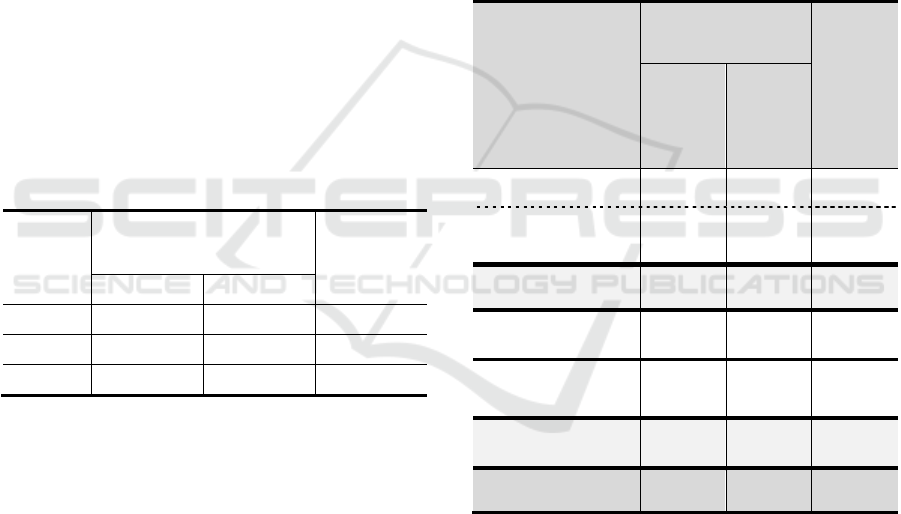
health teams and simple handling by patients. Chart
1 shows the amount of data collected, by UBS.
Chart 1: Distribution of Data Collection by UBS, Porto
Belo (SC), 2020.
Source: Prepared by the authors (2020)
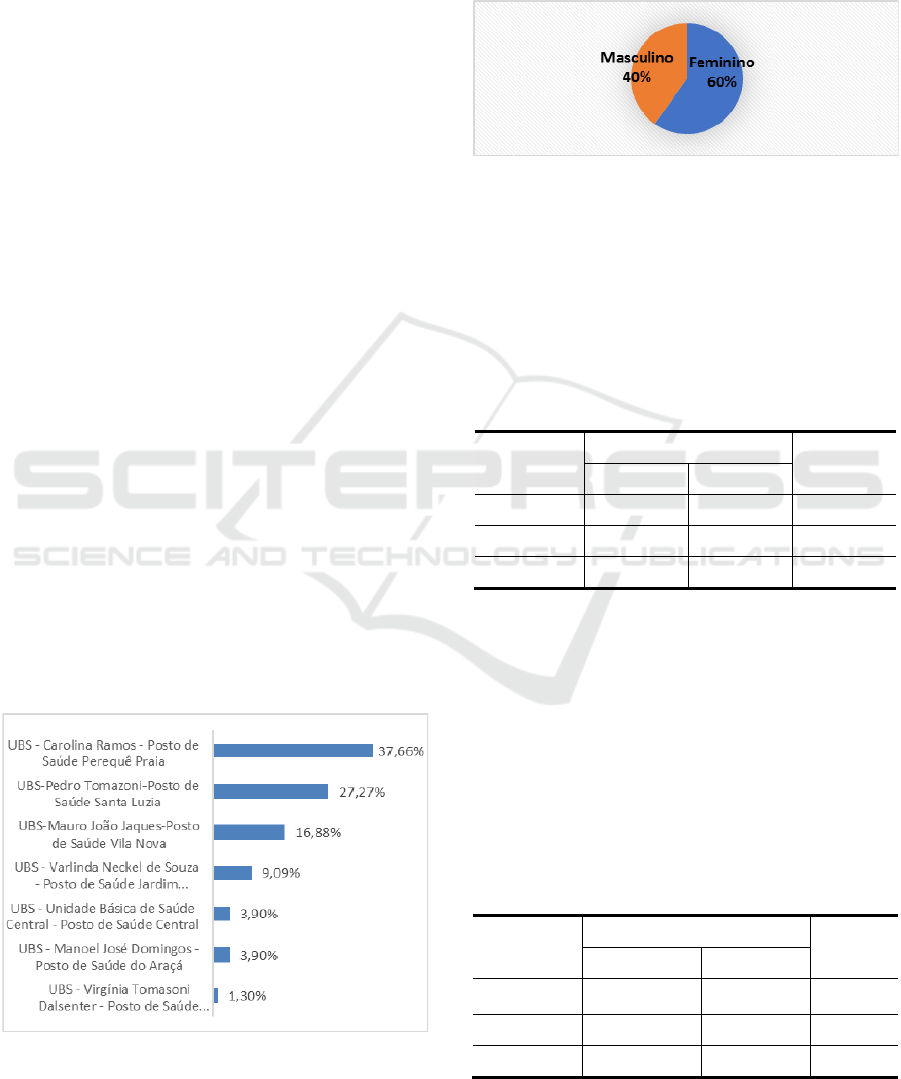
As shown by the distribution of patients by
Gender in Chart 2, 60% of the participants are
female.
Chart 2: Percentage of Patients by Gender, in Porto Belo
(SC), 2020.
Source: Prepared by the authors (2020)
Users were asked if they were tested to COVID-
19 and to report their results. Table 1 shows the
results of the question about testing for COVID-19,
including the 5 (five) participants who preferred not
to answer. Among the respondents, 51.4% had
already taken the test, 30.6% being female and
20.8% male.
Table 1: Contingency Table of Total People who took the
COVID-19 test, by Gender, Porto Belo (SC), 2020.
Gender
Tested for COVID-19
Total
No Yes
Female 26.4% 30.6% 57.0%
Male 22.2% 20.8% 43.0%
Total 48.6% 51.4% 100.0%
Source: Prepared by the authors (2020)
Table 2 shows the percentage of responses
obtained between positive and negative cases in
performed tests. Although 8 (eight) participants
decided not to answer, most of the 69 (sixty-nine)
participants who answered had not taken the test
(73.9%). Thus showing a trend of denial to the
diagnosis of COVID-19, even without performing
the test to confirm the result. Among the people who
tested positive for COVID-19, 17.4% were female,
Table 2: Contingency Table of the Test Result for
COVID-19, by Gender, Porto Belo (SC), 2020.
Gender
COVID-19 Test Result
Total
Negative Positive
Female 37.7% 17.4% 55.1%
Male 36.2% 8.7% 44.9%
Overall 73.9% 26.1% 100.0%
Source: Prepared by the authors (2020)
Epidemiological and Prognostic Factors Related to COVID-19 in Primary Care in a Municipality in Southern Brazil
517
while 8.7%, were male. Overall, the number of
females who tested positive for COVID-19 (12
cases) is exactly twice as many cases reported
among males (6 cases).
In turn, this data is not in line with a study
carried out in Italy comparing the number of cases
by gender, which reported a greater number of cases
of COVID-19 in males (59.8%) when compared to
females (40.2%) (Livingston; Bucher, 2020). Public
health policies and efforts have barely addressed the
possible impacts of gender on COVID-19 outbreaks,
so there is little knowledge of any gender analysis
related to the outbreak by global health institutions
or governments in affected countries or in the
preparation stages (Wenham; Smith; Morgan, 2020).
As for the contact with people who tested
positive for COVID-19, Table 3 shows that most
participants reported not having had contact with
people who tested positive (54.7%), while 45.3%
reported that they had. Regarding those who
reported that have been in contact with people
infected with COVID-19, 28.0% were female, while
17.3% were male.
Table 3: Contingency Table of Total People Who Have
Been in Contact With People Infected With COVID-19,
by Gender, Porto Belo (SC), 2020.
Gender
Have been in contact with
people who tested positive
for COVID-19
Total
No Yes
Female 32.0% 28.0% 60.0%
Male 22.7% 17.3% 40.0%
Total 54.7% 45.3% 100.0%
Source: Prepared by the authors (2020)
Tables 1, 2 and 3 show that the gender should be
considered when analyzing the data during the
COVID-19 pandemic. On the one hand, the
percentage of females who answered the questions
in this research (60%) should be highlighted, which
is much higher than that of males (40%). At least in
part, this imbalance may explain the percentage of
females who tested positive for COVID-19 to be
twice (17.4%) the percentage of males (8.7%) who
tested positive. On the other hand, females
performed more COVID-19 tests (30.6%) than
males (20.8%). However, Table 3 shows a greater
exposure of females with positive results in tests, as
28.0% of them reported that they have been in
contact with people who had tested positive for
COVID-19, while 17.3% of males have been in
contact with confirmed cases.
Table 4 summarizes the crossing of three
variables: close contact with any confirmed case of
COVID-19 or an unwell family member, whether
the participant tested positive or not, and whether or
not the participant had difficulty or “tiredness” in
basic Activities of Daily Living (ADLs) (e.g. self-
care, hygiene and dressing). Of the 58 (fifty-eight)
participants who answered the three questions, 6.9%
reported having difficulty in basic ADLs. Of these,
1.7% has been in close contact with a confirmed
case of COVID-19 or an unwell family member, and
1.7% also tested positive for COVID-19.
Table 4: Percentage of participants who have been in
contact with people who tested positive for COVID-19 or
a suspected family member, and who also tested positive,
and if they reported difficulties or “tiredness” in basic
ADLs, Porto Belo (SC), 2020.
Have been in
contact with people
who tested positive
for COVID-19 or a
suspected family
member / Tested
positive for COVID-
19
Had difficulty or
“tiredness” in basic
ADLs
Total
No Yes
Tested negative for
COVID-19
34.6% 0.0% 34.6%
Yes and tested
positive for COVID-
19
17.2% 5.2% 22.4%
Subtotal 1 - No
contact
51.8% 5.2% 57.0%
Tested negative for
COVID-19
17.2% 0.0% 17.2%
Yes, have been in
contact with people
who tested positive
24.1% 1.7% 25.8%
Subtotal 2 - Yes,
have been in contact
41.3% 1.7% 43.0%
Total 93.1% 6.9% 100.0%
Source: Prepared by the authors (2020)
Table 5 summarizes the crossing of three
variables: close contact with any confirmed case of
COVID-19 or an unwell family member, whether
the participant tested positive or not, and whether
or not the participant had difficulty or “tiredness”
in Instrumental Activities of Daily Living (IADLs),
such as work, leisure and physical activities. Of the
55 (fifty-five) participants who answered the three
questions, 5.5% reported having difficulty in
IADLs. Of these, 1.8% have been in close contact
with a confirmed case of COVID-19 or an unwell
HEALTHINF 2021 - 14th International Conference on Health Informatics
518
family member, and 1.8% also tested positive for
COVID-19.
Although Tables 4 and 5 show a higher
percentage of people who did not report difficulty or
“tiredness” in ADLs or IADLs (93.1% and 94.5%,
respectively), 22.4% of the first group and 18.2% of
the second group, tested positive for COVID-19.
The percentage of those who tested positive for
COVID-19 and also had dyspnea in basic ADLs was
higher compared to those who had dyspnea in
IADLs (5.2% and 3.6%, respectively), thus
suggesting a smaller number of people with more
serious sequelae and confirming the high
transmission rates of the virus when compared with
the contact of these individuals with confirmed cases
of COVID-19 or suspected family member (also
1.7% and 1.8%, respectively).
Table 5: Percentage of participants who have been in
contact with people who tested positive for COVID-19 or
a suspected family member, and who also tested positive,
and if they reported difficulties or
“tiredness” in IADLs,
Porto Belo (SC), 2020.
Have been in contact with
people who tested positive
for COVID-19 or a
suspected family member
/ Tested positive for
COVID-19
Had difficulty or
“tiredness” in
IADLs
Total
No Yes
Tested negative for
COVID-19
36.4% 0.0% 36.4%
Yes and tested positive for
COVID-19
14.5% 3.6% 18.2%
Subtotal 1 - No contact 50.9% 3.6% 54.5%
Tested negative for
COVID-19
18.2% 0.0% 18.2%
Yes and tested positive for
COVID-19
25.5% 1.8% 27.3%
Subtotal 2 - Yes, have
been in contact
43.6% 1.8% 45.5%
Total 94.5% 5.5% 100.0%
Source: Prepared by the authors (2020)
Outbreaks of new and reemerging diseases, such
as the current COVID-19 epidemic, can potentially
overwhelm health systems at the expense of primary
health care requirements in low-income countries
(Velavan; Meyer, 2020). These outbreaks can have
huge potential implications for planning and
decision-making in confirmed cases of COVID-19,
especially in high-risk areas (Petropoulos;
Makridakis 2020). Each outbreak also provides an
opportunity to obtain relevant information, some of
which are associated with a limited window of
opportunity (Fauci; Lane; Redfield, 2020).
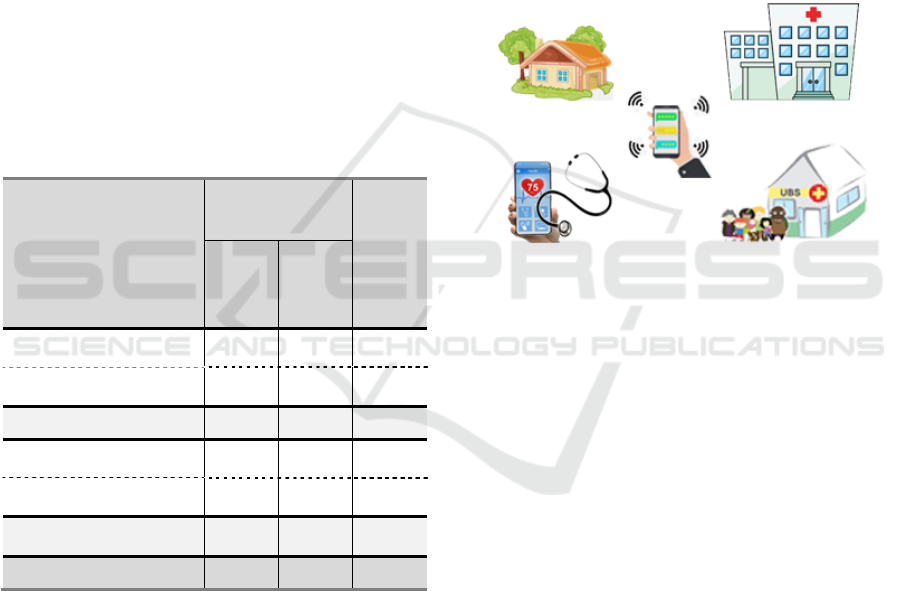
In this context, telemonitoring contributed to the
planning of health actions within the scope of each
of the Primary Health Units in the municipality, in
addition to generating data for epidemiological
surveillance regarding the prevalence of symptoms
and prognostic factors for COVID-19 in the
population of each territory. Therefore, it contributes
to the performance of diagnostic tests and to assist
team decision making in the UBS according to the
Operational Structure of the Primary Health Care
Network, as proposed in Figure 1. The results were
analyzed in order to generate data focused on health
planning and assisting team decision making within
the health field.
Source: Prepared by the authors (2020)
Figure 1: Operational Structure of the Primary Health Care
Network, Porto Belo (SC), 2020.
Given the above, there is still much to be
developed despite the experience and robustness of
the surveillance system and public policies (Turci;
Holliday; de Oliveira, 2020). Continuous
surveillance of the various countries facing the
pandemic is required to better understand the global
epidemiology of COVID-19, including transparent
and accurate reporting of patient characteristics and
symptoms (Onder; Rezza; Brusaferro, 2020).
4 CONCLUSIONS
A longer period of monitoring in Health Centers is
required to reach broader conclusions among
suspected and confirmed cases of COVID-19 in the
primary care facilities in Porto Belo.
Data analysis and subsequent evaluation found a
possible demand with symptoms and sequelae of
COVID-19. This was shown mainly by users who
reported difficulty or “tiredness” in basic ADLs and
IADLs, which may result in patients with chronic
Epidemiological and Prognostic Factors Related to COVID-19 in Primary Care in a Municipality in Southern Brazil
519

muscle fatigue and dyspnea as a future demand in
the municipality.
These data are essential for the health decision-
making process of managers, through the
formulation of public policies and the rational
application of resources in the most sensitive
segments in care, as in promotion and prevention.
The COVID-19 pandemic led to a reflection on
public health systems and strategies, as well as the
importance of care that is not only equitable, but
also universal to populations in a global context.
REFERENCES
Bedford, Juliet et al. COVID-19: towards controlling of a
pandemic. The Lancet, v. 395, n. 10229, p. 1015-1018,
2020.
Cascella, Marco et al. Features, evaluation and treatment
coronavirus (COVID-19). In: Statpearls [internet].
StatPearls Publishing, 2020.
Calton, Brook; Abedini, Nauzley; Fratkin, Michael.
Telemedicine in the time of coronavirus. Journal of
Pain and Symptom Management, 2020.
Fauci, Anthony S.; Lane, H. Clifford; Redfield, Robert R.
Covid-19
—navigating the uncharted. 2020.
Gandhi, R. T.; Lynch, J. B.; Del Rio, C. Mild or Moderate
Covid-19. The New England Journal of Medicine,
2020.
Heymann, David L.; Shindo, Nahoko. COVID-19: what is
next for public health?. The Lancet, v. 395, n. 10224,
p. 542-545, 2020.
Hollander, Judd E.; Carr, Brendan G. Virtually perfect?
Telemedicine for COVID-19. New England Journal of
Medicine, v. 382, n. 18, p. 1679-1681, 2020.
IBGE, Panorama de Porto Belo (SC), disponível em:
https://cidades.ibge.gov.br/brasil/sc/porto-
belo/panorama. Acessado em 28 de setembro de 2020.
Lipsitch, Marc; Swerdlow, David L.; Finelli, Lyn.
Defining the epidemiology of Covid-19
—studies
needed. New England journal of medicine, v. 382, n.
13, p. 1194-1196, 2020.
Livingston, Edward; Bucher, Karen. Coronavirus disease
2019 (COVID-19) in Italy. Jama, v. 323, n. 14, p.
1335-1335, 2020.
Ministério da Saúde (BR). Fast-Track para a atenção
primária em locais com transmissão comunitária: fluxo
rápido [Internet]. Brasília: Ministério da Saúde; 2020a
[Last access April 15, 2020]. Available from:
http://189.28.128.100/dab/docs/portaldab/
documentos/20200407_BOLSO_ver07.pdf
Ministério da Saúde (BR). Protocolo de manejo clínico do
coronavírus (Covid-19) na Atenção Primária à Saúde
[Internet]. Brasília: Ministério da Saúde; 2020b [Last
access April 15, 2020]. 32 p. Available from:
https://www.saude.gov.br/images/pdf/2020/
marco/20/20200318-ProtocoloManejo-ver002.pd
Mo, Pingzheng et al. Clinical characteristics of refractory
COVID-19 pneumonia in Wuhan, China. Clinical
Infectious Diseases, 2020.
Onder, Graziano; Rezza, Giovanni; Brusaferro, Silvio.
Case-fatality rate and characteristics of patients dying
in relation to COVID-19 in Italy. Jama, v. 323, n. 18,
p. 1775-1776, 2020.
Petropoulos, Fotios; Makridakis, Spyros. Forecasting the
novel coronavirus COVID-19. PloS one, v. 15, n. 3, p.
e0231236, 2020.
Rothan, Hussin A.; Byrareddy, Siddappa N. The
epidemiology and pathogenesis of coronavirus disease
(COVID-19) outbreak. Journal of autoimmunity, p.
102433, 2020.
Turci, Maria Aparecida; Holliday, Julia Braga; De
Oliveira, Nerice Cristina Ventura Costa. A Vigilância
Epidemiológica diante do Sars-Cov-2: desafios para o
SUS e a Atenção Primária à Saúde. APS EM
REVISTA, v. 2, n. 1, p. 44-55, 2020.
Velavan, Thirumalaisamy P.; MeyeR, Christian G. The
COVID
‐19 epidemic. Tropical medicine &
international health, v. 25, n. 3, p. 278, 2020.
Wenham, Clare; Smith, Julia; Morgan, Rosemary.
COVID-19: the gendered impacts of the outbreak. The
Lancet, v. 395, n. 10227, p. 846-848, 2020.
Zheng, Ying-Ying et al. COVID-19 and the cardiovascular
system. Nature Reviews Cardiology, v. 17, n. 5, p.
259-260, 2020.
APPENDIX
Questionnaire used for telemonitoring of patients
with respiratory symptoms:
Name:
Date of birth:
Gender:
( ) Male
( ) Female
Questionnaire on Influenza-like illness and
Comorbidities
Do you have or had any of the following factors?
( ) Cough
( ) Temperature between 35.7ºC and 38ºC
( ) Temperature greater than 38ºC
( ) Fatigue
( ) Mucus
( ) Shortness of breath
( ) Muscle pain
( ) Sore throat / Difficulty swallowing
( ) Headache
( ) Chills
( ) Nasal congestion / runny nose
HEALTHINF 2021 - 14th International Conference on Health Informatics
520

( ) Diarrhea
( ) Nausea or vomiting
Do you have any of the following comorbidities?
( ) Heart diseases
( ) Asthma, emphysema, bronchitis or other lung
disease
( ) Hypertension
( ) Depression
( ) Chronic kidney or liver disease
( ) Previous transplant
( ) Immunosuppression due to disease or
chemotherapy/radiotherapy (other medicines).
( ) Diabetes mellitus
( ) Smoking
Questionnaire on COVID‐19
Do you have or had any of the following factors
since the start of the pandemic?
( ) Severe shortness of breath at rest
( ) Difficulty breathing
( ) Chest pain or pressure
( ) Cold, moist or pale and stained skin
( ) Sudden confusion
( ) Difficulty awakening
( ) Bluish lips or face
( ) Little or no urine production
( ) Coughing up blood
Other conditions, such as:
( ) Neck stiffness
( ) Rash
Do you have or had any of the following factors
before the emergence of the pandemic in Brazil?
( ) yes ( ) no
Have you been in close contact with someone who
has tested positive for COVID‐19 or an unwell
family member?
( ) yes ( ) no
Have you been tested for COVID-19?
( ) yes ( ) no
If so, was it positive?
( ) yes ( ) no
Do you have tiredness or difficulties in performing
basic activities of daily living (e.g. self-care, hygiene
and dressing) after the diagnosis of COVID‐19?
( ) yes ( ) no
Do you have tiredness or difficulties in performing
instrumental activities of daily living (e.g. work,
leisure and physical activities) after the diagnosis of
COVID‐19?
( ) yes ( ) no
Assistance in team decision making:
- Refer for immediate medical care if the subject has
severe symptoms and report the case to the Family
Health Strategy;
- In cases of relevant comorbidities, provide
proactive and complete assistance to the patient;
- Refer for testing and reporting in Epidemiological
Surveillance;
- Specific referral to the Support Center for Family
Health, if required;
- Arrange video conference follow-up and monitor
closely if pneumonia is suspected.
Epidemiological and Prognostic Factors Related to COVID-19 in Primary Care in a Municipality in Southern Brazil
521
