
Mathematical Model for Estimating Nutritional Status of the Population
with Poor Data Quality in Developing Countries: The Case of Chile
Denisse
´
Avalos
1
, Crist
´
obal Cuadrado
2,3 a
, Jocelyn Dunstan
4,5 b
, Javier Moraga-Correa
1,6
,
Luis Rojo-Gonz
´
alez
1,7 c
, Nelson Troncoso
1
and
´
Oscar C. V
´
asquez
1 d
1
Department of Industrial Engineering, Universidad de Santiago, Santiago, Chile
2
School of Public Health, Universidad de Chile, Santiago, Chile
3
Centre for Health Economics, University of York, York, U.K.
4
Center for Mathematical Modeling - CNRS UMI2807, Universidad de Chile, Santiago, Chile
5
Center for Medical Informatics and Telemedicine, Universidad de Chile, Santiago, Chile
6
Business School, University of Nottingham, Nottingham, U.K.
7
Facultat de Matem
`
atiques i Estad
´
ıstica, Universitat Polit
`
ecnica de Catalunya, Barcelona, Spain
Keywords:
Transition Probabilities, Obesity, Developing Countries, Non-linear Programming, Poor Data Quality.
Abstract:
Obesity is one of the most important risk factors for non-communicable diseases. Nutritional status is gen-
erally measured by the body mass index (BMI) and its estimation is especially relevant to analyse long-term
trends of overweight and obesity at the population level. Nevertheless, in most context nationally represen-
tative data on BMI is scarce and the probability of individuals to progress to obese status is not observed
longitudinally. In the literature, several authors have addressed the problem to obtain this estimation us-
ing mathematical/computational models under a scenario where the parameters and transition probabilities
between nutritional states are possible to compute from regular official data. In contrast, the developing coun-
tries exhibit poor data quality and then, the approaches provided from the literature could not be extended to
them. In this paper, we deal with the problem of estimating nutritional status transition probabilities in settings
with scarce data such as most developing countries, formulating a non-linear programming (NLP) model for
a disaggregated characterization of population assuming the transition probabilities depend on sex and age.
In particular, we study the case of Chile, one of the countries with the highest prevalence of malnutrition in
Latin America, using three available National Health Surveys between the years 2003 and 2017. The obtained
results show a total absolute error equal to 5.11% and 10.27% for sex male and female, respectively. Finally,
other model applications and extensions are discussed and future works are proposed.
1 INTRODUCTION
The nutritional status of the population is generally
measured using the body mass index (BMI). This
metric is defined as the weight divided by height
squared, kg/m
2
(Okorodudu et al., 2010; Apovian,
2016). In contrast to other technical metrics such
as dual-energy x-ray absorptiometry, BMI is easy-
to-implement in clinical practice and population sur-
veys and provides a similar discriminatory capability
a
https://orcid.org/0000-0002-0174-5958
b
https://orcid.org/0000-0001-6726-7242
c
https://orcid.org/0000-0003-4894-2470
d
https://orcid.org/0000-0002-1393-4692
(Huxley et al., 2010; NCD Risk Factor Collaboration
(NCD-RisC), 2016; NCD Risk Factor Collaboration
(NCD-RisC), 2017). In practice, this metric allows to
classify the nutritional status for individuals aged 18
years and older according to its BMI into four groups
proposed by the World Heath Organization (WHO): i)
Underweight, BMI < 18.4; ii) Normal, 18.5 ≤ BMI
≤ 24.9; iii) Overweight, 25.0 ≤ BMI ≤ 29.9; and iv)
Obese, BMI ≥ 30.
Unfortunately, obesity represents one of the most
important risk factors for non-communicable dis-
eases. It was declared an epidemic in 1990 by the
World Health Organization, reaching the first position
in the 21st century. Between the years 1995 and 2000,
408
Ávalos, D., Cuadrado, C., Dunstan, J., Moraga-Correa, J., Rojo-González, L., Troncoso, N. and Vásquez, Ó.
Mathematical Model for Estimating Nutritional Status of the Population with Poor Data Quality in Developing Countries: The Case of Chile.
DOI: 10.5220/0010262404080415
In Proceedings of the 10th International Conference on Operations Research and Enterprise Systems (ICORES 2021), pages 408-415
ISBN: 978-989-758-485-5
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

adult population with obesity increased in 100 mil-
lion people, reaching 300 million worldwide, whereas
18 million under-five year children have overweight
(World Health Organization, 2003). In addition, more
than 1.9 billion adults aged 18 years and older were
overweight, being 650 million adults were obese in
2016 (World Health Organization, 2016).
Consequently, the estimation of the prevalence of
different nutritional status categories is especially rel-
evant for the development of future health policies
due to at least two reasons:
• Obesity is associated with the leading causes of
death worldwide since the management of its re-
lated factors has proven to be tremendously com-
plex presenting a sustained upward trend. In par-
ticular, obesity is related to serious health risks
(National Institutes of Health, 1998). For in-
stance, every 5-unit increases in BMI above 25,
the overall mortality increases by 29%, cardiovas-
cular mortality by 41%, and diabetes-related mor-
tality by 210% (Apovian, 2016).
• In terms of the associated costs, a person who
has obesity incurs an annual healthcare cost of
36% greater than a normal weight person and a
77% higher in the medication costs (Sturm, 2002).
In this sense, some authors have been reported
that an obese patient has annual medical spending
between 25% (Detournay et al., 2000) and 42%
(Finkelstein et al., 2003) higher than who is of
normal weight. This account for direct costs of,
at least, 5%, of the total health expenditures of
developed countries (Levy et al., 1995; Manson
et al., 2004). In practice, if the number of indi-
viduals aged 16 and 17 who have overweight or
obesity could be reduced by 1%, this would re-
sult in a decrease in lifetime medical costs of $586
million (Wang et al., 2010). In addition, it might
be expected that at low-income levels of the coun-
try the underweight prevalence should dominate
the landscape, but the projected average annual
growth of obesity indicates that, across 147 coun-
tries, it will increase 2.47% respect to the Gross
Domestic Product per capita during 2019-2024
(Talukdar et al., 2020).
The problem of estimation of long-term trends of obe-
sity prevalence is mainly addressed by using mathe-
matical models that aim to capture the relationships
among environment, biological, social and cultural
aspect from a system point of view under a scenario
where regular official data is available (Mitchell et al.,
2011; Frerichs et al., 2013). However, these ap-
proaches could not be easily extended to other settings
where the data is not collected regularly or not exten-
sively enough. For instance, the developing countries
such as Argentina (Secretar
´
ıa de Gobierno de Salud,
Argentina, 2019), Brazil (Instituto Brasileiro de Ge-
ograf
´
ıa e Estad
´
ıstica, Brasil, 2020), Colombia (Min-
isterio de Salud, Colombia, 2015) and Chile (Ministe-
rio de Salud, Chile, 2017) only provide two and three
national health survey into two decades.
1.1 Literature Review
In the literature, the importance of estimating obesity
prevalence over time and how to use National Health
Surveys in each country as main data source, is em-
phasized from different modeling perspectives (see
(Olariu et al., 2017) for a recent survey in Markov
cohort models and (Xue et al., 2018) for a recent sur-
vey in system dynamic (SDM) and agent-based mod-
eling (ABM)). In particular, the researchers mention a
special key input called transition probabilities in the
chronic disease modeling context. They are defined as
the probability or rate to move from one state of a cat-
egorical risk factor (e.g. nutritional status) to another
(Van de Kassteele et al., 2012); being transition rates
and transference rates sometimes used as synonyms.
In the last decades, several authors have addressed
the estimation of the nutritional status for the pop-
ulation from developed countries. For instance, a
multi-stage Markov model is decribed in (Van de
Kassteele et al., 2012), which is used on the “Perma-
nent Onderzoek Leef Situatie” data for the Nether-
lands collected between 2006 and 2007, that is to
say, a cross-sectional study, considering the individ-
uals of 85 years old tops. To compute the transi-
tion probabilities the authors consider a transportation
problem (well-known in Linear Programming), where
the results show that the prevalence of being normal
weight during the last year and have obesity the next
year, and vice versa, is null at any age. A suscep-
tible–infected–recovered model for the United States
(US) and the United Kingdom (UK) is proposed in
(Ward et al., 2017), using the information between
1988 and 1998 (Ogden et al., 2006), and the Health
Survey for England between 1993 and 1997 (Thomas
et al., 2014), respectively; indicating that, via a for-
ward simulation, the obesity prevalence will plateau
independent of current prevention strategies at 32%
(US) and 39.6% (UK) by about 2030. A longitudinal
study, from an ABM simulation point of view, was
carried out using the National Health and Nutrition
Examination Survey from 1976 through 2014 to pre-
dict risk factors for the nutritional statuses for indi-
viduals aged 35 years. The results project that a ma-
jority of children (57.3%) will be obese at the age of
35 years, and roughly half of the projected prevalence
will occur during childhood.
Mathematical Model for Estimating Nutritional Status of the Population with Poor Data Quality in Developing Countries: The Case of Chile
409

Recently, several authors have tackled the prob-
lem of estimating the nutritional status of the popu-
lation with poor data quality. A time-homogeneous
continuous-time Markov model is proposed in (Lartey
et al., 2020) to compute the transition probabilities
between nutritional statuses, using the Ghana Who
SAGE in 2007/2008 and 2014/2015. The obtained re-
sults show that, for obese individuals, the probability
of remaining obese, decrease to overweight and nor-
mal weight was 90.2%, 9.2%, and 0.6%, respectively.
Complementary to the previous works in this field,
our research acknowledges the reality of the so-called
developing countries, where the data is not collected
regularly or not very extensively.
1.2 Our Contribution
This research deals with the problem of estimating
the nutritional status of the population with poor data
quality in developing countries. In particular, we
study the case of Chile, which ranks third in Latin
America in child overweight prevalence with a pres-
ence of 9.3% (Food and Agriculture Organization,
2018) and second among the countries of the Orga-
nization for Economic Cooperation and Development
in overweight prevalence for the population over 15
years old. Chile represents an example where the data
is not collected regularly or not very extensively, as it
is often the case in other regions of the ’developing’
world. Formally, we formulate a non-linear program-
ming (NLP) model, which allows us to determine the
transition probabilities considering a set of disaggre-
gated variables by BMI and age ranges and assum-
ing the transition probabilities depend on sex and age
range. The parameters are obtained from the analysis
of the official reports and the three available national
health surveys between the years 2003 and 2017. To
test the performance of our NLP model, we carry out
computational experiments and compute the total ab-
solute error of our estimation in different scenarios.
Finally, other applications for the model are discussed
and future works are proposed.
2 NON-LINEAR PROGRAMMING
(NLP) MODEL
2.1 Dynamic Conceptualization
In order to define our model, we introduce the dy-
namic conceptualization for the population’s nutri-
tional status during a given period. Let I , J and K
be the sets of discretized BMI, age ranges, and sexes,
respectively. For convenience, we denote T the set of
the years within the given period and the state of the
population is defined by BMI i, age range j, and sex k.
From each state, the movements within and between
the BMI and age ranges are modeled according to the
transition probabilities. We distinguish the transition
probabilities to decrease, to remain or to increase the
current BMI as follow: i) α
j,k
, is the transition proba-
bility to increase the BMI of the people of sex k from
the year t to the year (t + 1); ii) β
j,k
, is the transition
probability to decrease the BMI of the population of
sex k from one year t to the year (t + 1) and iii) φ
j,k
,
is the transition probability to remain the BMI of the
population of sex k from one year t to the year (t +1).
In addition, we consider the population growth
κ
t
i, j,k
and the population proportion γ
t
j,k
of sex k in the
upper bound of the age range j at year t (i.e., the pop-
ulation proportion that would change their age range
from year t to year (t + 1)). Note that this proportion
is assumed equal to 0% in the last age range. Thus, the
transition probabilities for the above population pro-
portion can be separated into two sub-categories as
follow: i) η
α,t
j,k
:= γ
t
j,k
α
j,k
, η
β,t
j,k
:= γ
t
j,k
β
j,k
and η
φ,t
j,k
:=
γ
t
j,k
φ
j,k
as the transition probabilities to increase, to
decrease or to remain the BMI from year t to the year
(t +1) but, at the same time, changing their age range;
and ii) ψ
α,t
j,k
:= (1−γ
t
j,k
)α
j,k
, ψ
β,t
j,k
:= (1−γ
t
j,k
)β
j,k
and
ψ
φ,t
j,k
:= (1 − γ
t
j,k
)φ
j,k
as the transition probabilities to
increase, to decrease or to remain the BMI from year
t to the next one (t +1) but, at the same time, remain-
ing their age range. An illustration of the dynamic
conceptualization is shown in Figure 1.
Figure 1: Illustration of the dynamic conceptualization.
Two consecutive years, t and t + 1 are depicted in order to
show the transitions of some defined population.
ICORES 2021 - 10th International Conference on Operations Research and Enterprise Systems
410

2.2 Formulation
We denote I
t
i, j,k
the continuous positive variable that
represents the population of BMI i ∈ I , age range j ∈
J and sex k ∈ K at year t ∈ T . Let T and T be the
bounds on the years in the model. The model aims
to minimize the weighted mean squared error in the
fitting of the population during the period in [T ;T ].
We define w
T
j,k
as the population proportion of sex k ∈
K in age range j ∈ J at the end of the year T . Let
U
T
i, j,k
be the real population at the end year T . Given
a sex k ∈ K , the NLP model is defined as follows:
[MIN]
∑
i∈I
∑
j∈J
(I
T
i, j,k
−U
T
i, j,k
)
2
w
T
j,k
(1)
subject to (for each year t ∈ {T ...T − 1})
I
t+1
i, j,k
1 − κ
t
i, j,k
=ψ
α,t
j,k
I
t
i−1, j,k
+ +η
α,t
j−1,k
I
t
i−1, j−1,k
+ ψ
φ,t
j,k
I
t
i, j,k
+ η
φ,t
j−1,k
I
t
i, j−1,k
+ ψ
β,t
j,k
I
t
i+1, j,k
+ η
β,t
j−1,k
I
t
i+1, j−1,k
∀ j ∈ J \ {1}, ∀i ∈ I \ {1,|I |} (2)
γ
t
j,k
=η
α,t
j,k
+ η
β,t
j,k
+ η
φ,t
j,k
∀ j ∈ J (3)
(1 − γ
t
j,k
) =ψ
α,t
j,k
+ ψ
β,t
j,k
+ ψ
φ,t
j,k
∀ j ∈ J (4)
α
min
j,k
≤ η
α,t
j,k
+ ψ
α,t
j,k
≤ α
max
j,k
∀ j ∈ J (5)
β
min
j,k
≤ η
β,t
j,k
+ ψ
β,t
j,k
≤ β
max
j,k
∀ j ∈ J (6)
φ
min
j,k
≤ η
ψ,t
j,k
+ ψ
ψ,t
j,k
≤ φ
max
j,k
∀ j ∈ J (7)
I
t
i, j,k
,η
α,t
j,k
,η
β,t
j,k
,η
φ,t
j,k
,ψ
α,t
j,k
,ψ
β,t
j,k
,ψ
φ,t
j,k
≥ 0 ∀i ∈ I , j ∈ J (8)
Expression (1) states the objective function of the
model. The possible transition is defined by the set
of constraints (2). These transitions are constrained
to the proportion to change of age range given by the
set of constraints (3)–(4), the bounds on these tran-
sitions are imposed by the set of constraints (5)–(7)
and the domain of the variables is defined in the set of
constraints (8).
2.3 Discretization and Data Wrangling
To compute the required parameters, we consider
official reports such as the three collected National
Health Surveys (ENS) into 15 years provided by the
Ministry of Health of Chile (MINSAL) (Ministerio
de Salud, Chile, 2017), the governmental documents
from the Department of Statistics and Health Infor-
mation (DEIS) (Departamento de Estad
´
ıstica e Infor-
maci
´
on de Salud, 2018) and the National Institute
of Statistics (INE) (Instituto Nacional de Estad
´
ıstica,
2017). Since the proposal required a discretization of
the variables, we should do it to achieve the desired
shape of the input. Thus, we consider the BMI as the
integer value of the recorded value and to group the
age by ranges of 10 years starting from 15 years old
such as a population grid is obtained.
However, as the survey is only a sample of the
entire population, there would likely be some com-
binations of the grid that have zero-counting. There-
fore, we should avoid this first issue by redistribut-
ing the population. So, the discussion now turns into
which model to pick and how to set its parameters.
Even although we should deal with a bi-variate distri-
bution over the BMI and the age range, there is not
evidence of this, but it does by considering the BMI
itself. For instance, it is common to assume a Gaus-
sian distribution, but it would be true if and only if
the related multi-factorial processes have additive ef-
fects; nonetheless, for biologic variables, the knowl-
edge suggests that these processes have a multiplica-
tive effect, e.g., an obesogenic environment, which is
more likely to follow a skewed, possibly log-normal,
distribution (Penman and Johnson, 2006).
A particular analysis is carried out on the popula-
tion growth, κ
t
i, j,k
. The population growth is the dif-
ference between the birth rate and the mortality rate
and, as we are considering people older than 15 years
old, it is necessary to get this rate in a time-lagged
sense, i.e., we need the birth rate of the people that
were born 15 years ago. Besides, a requirement is that
this rate should be distributed by BMI and age ranges.
Addressing this latter issue, from a separable point of
view, we have that: i) the lagged birth rate only in-
fluences on the first age range whereas the mortality
rate is in the whole set of age ranges; ii) to get the
distributed population growth, we use a study related
to survival analysis which works on the Hazard ratios
(Berrington de Gonz
´
alez et al., 2010) to get them by
BMI.
Even although the transition probabilities are the
core of the study itself, we must provide the feasible
bounds for the estimation. Several authors have been
reported evidence on the transition probabilities for a
specific nutritional status (Power et al., 1997; Orpana
et al., 2006; Laitinen et al., 2001; Booth et al., 2012;
Fildes et al., 2015; Srinivasan et al., 1996). However,
the obtained results reported by them are not neces-
sarily the BMI and age range considered. To address
this problem, we propose to work with multiple sce-
narios approach from the literature data. Thus, the
bounds of the transition probabilities, X, and its mean
value, Ave(X ), are assumed to be normal distributed
such that the confidence bounds of the transition prob-
ability, say Ave(X ) as the lower bound, and Ave(X) as
the upper bound, at a confidence level δ% can be ob-
tained from Pr(Ave(X) ≤ X ≤ Ave(X)) = δ.
Mathematical Model for Estimating Nutritional Status of the Population with Poor Data Quality in Developing Countries: The Case of Chile
411

3 RESULTS
The computational experiments are carried out split-
ting up the data into a fitting period (2003-2010) and
a validation period (2010-2017) as a forward simula-
tion to set out the performance of the model.
3.1 Implementation
The mathematical model is implemented in AMPL
programming language with Minos as the solver and
executed on a MacBook Air Intel i5, 1.6 GHz, 8GB
RAM, with no stopping time, 2500 iterations tops
considering five random seeds given the non-linearity
of the model. The obtained results are such that we
use to make a discrete grid at confidence levels in
[0.01;0.995] such as 256 and 254 scenarios are given
with solving time of 38.96 minutes and 41.90 minutes
for males and females, respectively.
3.2 Transition Probabilities
The obtained results show that there are some differ-
ences between the sexes. In particular, such as Table 1
shows, we can see that the standard deviation for each
fitted parameter is quite similar between sexes and the
comparison between them shows a remarkable differ-
ence over the age ranges but not at all. For instance,
while the transition probability to remain the current
BMI is the highest one, the transition probability to
increase the BMI is greater than to decrease until the
65 years old for both sexes but between 65 and 74
years old, the sex female reverses this trend, i.e., the
transition probability to increase the BMI is greater
than to decrease, then this relation gets reverse and
then goes back to the same.
A second important remark concerns the density
of the results (see Figure 2). In fact, the transition
probabilities are ever in the same order; in decreasing
order, they are to remain, to increase, and to decrease.
So, in general, although the transition probability to
remain the current BMI dominates the others, this ef-
fect does not make the difference due to remain a sta-
tus is possible at any level and if we compare from one
year to another it means that the population has a sta-
ble BMI, but when we make the period wider, e.g., 2
years, if the person increases its BMI in the first place
and then remains it, the overall effect is that the per-
son increases its BMI from the beginning of the study.
Therefore, it is clear that the population, in the long-
term sense, has a trend to increase their BMI, but im-
portant differences especially exist for sex male and
some age ranges, including ones where the transition
probabilities to decrease or to increase are almost the
same.
For both sexes there is an age range that changes
with respect to the others, for sex male, it is 55-64
years old and for sex female, it is 15-24 years old.
These age ranges have completely different shapes of
the distribution; in fact, they are, from a biological
point of view, interesting phases of hormonal changes
in the body, so they should be carefully analyzed. On
the other hand, for both sexes, a useful remark is re-
lated to the variability and the shape of the transition
probabilities. The distributions are wide enough to
cover the half of the probabilities, at least, whereas
there are not bi-modal ones except the distributions
for the first age range. However, the entire previous
comments are just true if the fitting is well. Using
the total absolute error as a metric to compare the
forecasting population against the real population in
2017, it reaches a 5.11% and 10.27% for sex male and
female, respectively. Even when the numbers seem
quite well, it is necessary to see the behavior of the
estimation. Figure 3 depicts, by sex, the real popu-
lation at each BMI (points) and the fitted curve ob-
tained from the model (lines) including their respec-
tively 95% confidence intervals at the end of the fit-
ting period (2010) and at the end of the validation
period (2017). The comparison shows quite similar
behavior and, with low total absolute error for both
sexes, and the fact that the real data belongs to the
confidence intervals (which are not too wide), the fit-
ting might be understood as a good one but taking into
account that both periods differ from each other.
4 DISCUSSION AND FUTURE
WORK
This work addressed the problem of estimating nutri-
tional status with poor data quality. A non-linear pro-
gramming model is formulated to obtain the transition
probabilities that are key elements in the modeling of
this epidemic and the designing of malnutrition public
policy options and the computation of the associated
costs of a specific population. Our proposal provides
a novel methodology to estimate them with a few data
available and a disaggregated characterization of the
population by sex, BMI and age ranges, in contrast to
other similar work works.
In particular, the research was focused on the
case of Chile, one of the countries with the highest
malnutrition in Latin America. The obtained results
show the fitted transition probabilities are fair via a
straight comparison against the last known informa-
tion. Nonetheless, it is important to say that, despite
ICORES 2021 - 10th International Conference on Operations Research and Enterprise Systems
412
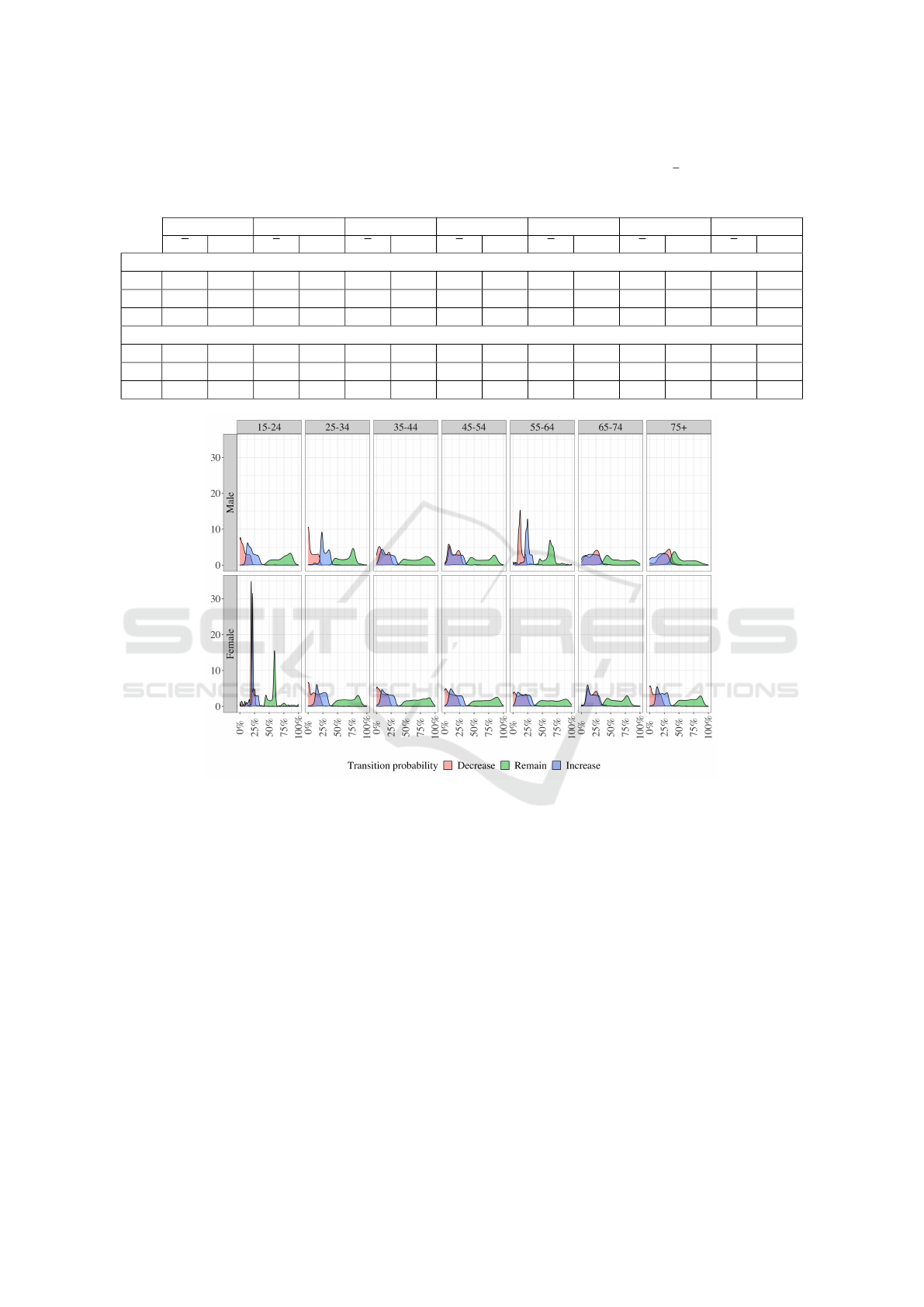
Table 1: Summary of the transition probabilities by sex and age ranges considering the whole fitting period (2003-2010). The
standard deviation (Sd) for each fitted value is similar between sexes. The comparison, in mean (x) terms, shows that the
transition probability to increase the BMI is greater than to decrease until the 65 years old for both sexes but between 65 and
74 years old, the female sex reverses this trend.
15-24 25-34 35-44 45-54 55-64 65-74 75+
x Sd x Sd x Sd x Sd x Sd x Sd x Sd
Male
β
j,.
7.5 7.6 6.7 7.3 11.9 9.3 15.8 9.4 13.8 8.0 19.8 10.6 26.4 10.3
φ
j,.
71.5 15.7 65.2 15.2 69.7 18.4 65.3 18.6 62.1 12.4 62.1 19.5 54.8 17.2
α
j,.
20.6 8.3 27.8 8.0 17.8 9.9 18.0 9.9 24.5 8.2 17.7 11.0 18.6 10.4
Female
β
j,.
19.9 8.4 9.1 8.6 9.8 8.7 11.0 10.7 13.3 11.4 20.4 11.3 10.2 9.6
φ
j,.
57.7 14.1 67.9 16.9 70.5 17.1 69.8 18.8 67.8 19.9 60.8 17.9 68.9 16.9
α
j,.
23.4 8.5 22.4 9.3 18.6 9.3 18.7 10.2 18.8 10.5 19.1 9.4 21.0 8.7
Figure 2: Distribution of the transition probabilities obtained for the fitting period (2003-2010) by age range and sex. The
transition probabilities are ever in the same order; in decreasing order, they are Remain, Increase, Decrease; but via look-up
analysis, we can suspect that this particular population tends to increase their BMI due to remaining a status just implies
non-changes when the study is at short-term.
the low error in the fitting period, the variability of
the transition probabilities distribution can make them
noisy and their interpretation might be carefully done.
However, the level of disaggregation of the variables
plays an important role in it. Thus, on the assumption
that the transition probabilities are constant within a
particular period and that they do depend on the age
and sex of the person, we get that the population un-
der study has a clear trend, in the long-term sense,
to increase their BMI, but it seems to be some vari-
ables that are not included yet. Besides, note that
the non-linearity of the mathematical model plays an
important role since the non-integer variables cannot
be solved. Also, the lack of information, especially
the time windows for collecting the data, is an im-
portant problem that adds noise to the model when
non-stationary variables are considered. Also, an im-
portant discussion must be done about the obtained
results, where it is known that any long-term forecast-
ing or extrapolation may be wrong when the period
gets longer. In this case, we can see an excellent esti-
mation at first glance in the fitting period, but the fore-
casting suffers a change of trend, especially for sex
female, in the validation period. Anyway, the tran-
sition probabilities distribution shows that there are
differences not just between sexes, but between age
ranges as well. In general terms, two age ranges that
have a remarkable change of shape, at 55-64 years
Mathematical Model for Estimating Nutritional Status of the Population with Poor Data Quality in Developing Countries: The Case of Chile
413
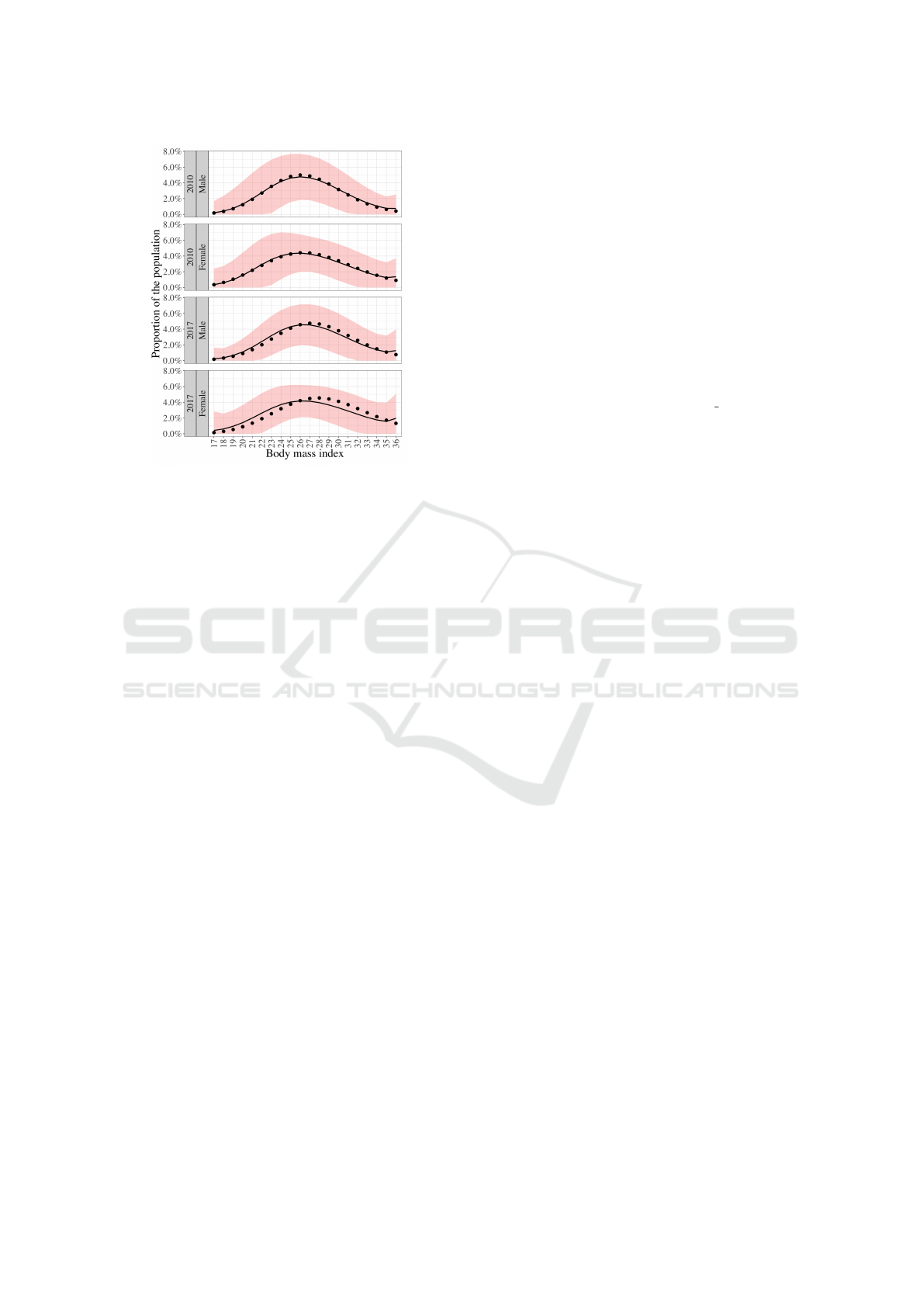
Figure 3: Comparison of the population obtained at the end
of the fitting period (2010) with a 5.11% of total absolute
error, and that one obtained from the forward simulation at
the end of the validation period (2017) with a 10.27% total
absolute error, by sex. The figure shows the known data
as points and the fitted values are shown as lines, whereas
the shaded area around them represents the 95% confidence
interval.
old for sex men and at 15-24 years old for sex female.
Those age ranges might be associated with hormonal
changes in the body for the respective sex, such as
the andropause for sex male (Tan and Pu, 2002) and
the menstrual cycle for sex female (Van Hooff et al.,
2004). Finally, we propose to explore the transition
probabilities estimation by relaxing the assumption
on the constant behavior according to the current BMI
and to consider non-constant variables based on a dif-
ferent point of view as the Bayesian analysis.
ACKNOWLEDGEMENTS
The authors are grateful for partial support from
the following sources: ANID Beca Mag
´
ıster en
el Extranjero, Becas Chile, Folio 73190041 (Javier
Moraga-Correa) and Folio 73201112 (Luis Rojo-
Gonz
´
alez), CONICYT-FONIS SA14ID0176 and
RCUK-CONICYT Newton-Picarte MR /N026640/1
(Crist
´
obal Cuadrado), CMM-ANID AFB 170001 and
CIMT-CORFO Cost Center 570111 (Jocelyn Dun-
stan), Universidad de Santiago de Chile, Proyecto DI-
CYT 061817VP (
´
Oscar C. V
´
asquez).
REFERENCES
Apovian, C. (2016). Obesity: definition, comorbidities,
causes, and burden. The American Journal of Man-
aged Care, 22(7 Suppl):s176–85.
Berrington de Gonz
´
alez, A., Hartge, P., Cerhan, J., et al.
(2010). Body-mass index and mortality among 1.46
million white adults. The New England Journal of
Medicine, 363(23):2211–2219.
Booth, H., Prevost, A., and Gulliford, M. (2012). Epi-
demiology of clinical body mass index recording in
an obese population in primary care: a cohort study.
Journal of Public Health, 35(1):67–74.
Departamento de Estad
´
ıstica e Informaci
´
on de Salud
(2018). Defunciones. https://public.tableau.com/
profile/deis4231#!/vizhome/Anuario Defunciones/
Defunciones. Online; accessed 3 oct 2020.
Detournay, B., Fagnani, F., Phillippo, M., et al. (2000).
Obesity morbidity and health care costs in France: an
analysis of the 1991-1992 medical care household sur-
vey. International Journal of Obesity, 24(2):151–155.
Fildes, A., Charlton, J., Rudisill, C., et al. (2015). Probabil-
ity of an obese person attaining normal body weight:
cohort study using electronic health records. Ameri-
can Journal of Public Health, 105(9):e54–e59.
Finkelstein, E., Fiebelkorn, I., and Wang, G. (2003). Na-
tional medical spending attributable to overweight and
obesity: How much, and who’s paying? further evi-
dence that overweight and obesity are contributing to
the nation’s health care bill at a growing rate. Health
Affairs, 22(Suppl1):219–226.
Food and Agriculture Organization (2018). Panorama de la
seguridad alimentaria y nutricional en am
´
erica latina
y el caribe.
Frerichs, L., Araz, O., and Huang, T. (2013). Modeling
social transmission dynamics of unhealthy behaviors
for evaluating prevention and treatment interventions
on childhood obesity. PloS One, 8(12):e82887.
Huxley, R., Mendis, S., Zheleznyakov, E., et al. (2010).
Body mass index, waist circumference and waist: hip
ratio as predictors of cardiovascular risk—a review of
the literature. European Journal of Clinical Nutrition,
64(1):16–22.
Instituto Brasileiro de Geograf
´
ıa e Estad
´
ıstica, Brasil
(2020). Pesquisa Nacional de Sa
´
ude - PNS.
https://www.ibge.gov.br/estatisticas/sociais/
justica-e-seguranca/9160-pesquisa-nacional-de-
saude.html?edicao=9177&t=o-que-e. Online;
accessed 3 oct 2020.
Instituto Nacional de Estad
´
ıstica (2017). Proyecciones de
Poblaci
´
on. https://www.ine.cl/estadisticas/sociales/
demografia-y-vitales/proyecciones-de-poblacion.
Online; accessed 3 oct 2020.
Laitinen, J., Power, C., and J
¨
arvelin, M. (2001). Family so-
cial class, maternal body mass index, childhood body
mass index, and age at menarche as predictors of adult
obesity. The American Journal of Clinical Nutrition,
74(3):287–294.
Lartey, S., Lei, S., Otahal, P., et al. (2020). Annual tran-
sition probabilities of overweight and obesity in older
ICORES 2021 - 10th International Conference on Operations Research and Enterprise Systems
414

adults: Evidence from world health organization study
on global ageing and adult health. Social Science &
Medicine, 247:112821.
Levy, E., L
´
evy, P., Le, C., et al. (1995). The economic cost
of obesity: the French situation. International Journal
of Obesity and Related Metabolic Disorders: Journal
of the International Association for the Study of Obe-
sity, 19(11):788–792.
Manson, J., Skerrett, P., Greenland, P., et al. (2004). The es-
calating pandemics of obesity and sedentary lifestyle:
a call to action for clinicians. Archives of Internal
Medicine, 164(3):249–258.
Ministerio de Salud, Chile (2017). Base de datos. http://
epi.minsal.cl/bases-de-datos/. Online; accessed 3 oct
2020.
Ministerio de Salud, Colombia (2015). Gesti
´
on
del conocimiento y fuentes de informaci
´
on.
https://www.minsalud.gov.co/salud/publica/
epidemiologia/Paginas/gestion-del-conocimiento-y-
fuentes-de-informacion.aspx. Online; accessed 3 oct
2020.
Mitchell, N., Catenacci, V., Wyatt, H., et al. (2011). Obe-
sity: overview of an epidemic. Psychiatric Clinics,
34(4):717–732.
National Institutes of Health (1998). Clinical guidelines for
the identification, evaluation, and treatment of over-
weight and obesity in adults - the evidence report.
Obesity Reviews, 6(2):51S–209S.
NCD Risk Factor Collaboration (NCD-RisC) (2016).
Trends in adult body-mass index in 200 countries from
1975 to 2014: a pooled analysis of 1698 population-
based measurement studies with 19.2 million partici-
pants. The Lancet, 387(10026):1377–1396.
NCD Risk Factor Collaboration (NCD-RisC) (2017).
Worldwide trends in body-mass index, underweight,
overweight, and obesity from 1975 to 2016: a pooled
analysis of 2416 population-based measurement stud-
ies in 128.9 million children, adolescents, and adults.
The Lancet, 390(10113):2627–2642.
Ogden, C., Carroll, M., Curtin, L., et al. (2006). Prevalence
of overweight and obesity in the United States, 1999-
2004. JAMA, 295(13):1549–55.
Okorodudu, D., Jumean, M., Montori, V., et al. (2010). Di-
agnostic performance of body mass index to identify
obesity as defined by body adiposity: a systematic re-
view and meta-analysis. International Journal of Obe-
sity, 34(5):791–799.
Olariu, E., Cadwell, K., Hancock, E., et al. (2017). Current
recommendations on the estimation of transition prob-
abilities in markov cohort models for use in health
care decision-making: a targeted literature review.
ClinicoEconomics and Outcomes Research: CEOR,
9:537–546.
Orpana, H., Tremblay, M., and Fin
`
es, P. (2006). Trends
in Weight Change Among Canadian Adults: Evidence
from 1996/1997 to 2004/2005 National Population
Health Survey. Citeseer.
Penman, A. and Johnson, W. (2006). The changing shape
of the body mass index distribution curve in the popu-
lation: implications for public health policy to reduce
the prevalence of adult obesity. Preventing Chronic
Disease, 3(3).
Power, C., Lake, J., and Cole, T. (1997). Body mass index
and height from childhood to adulthood in the 1958
british born cohort. The American Journal of Clinical
Nutrition, 66(5):1094–1101.
Secretar
´
ıa de Gobierno de Salud, Argentina
(2019). 2° Encuesta Nacional de Nutrici
´
on
y Salud ENNYS 2. Resumen ejecutivo.
https://cesni-biblioteca.org/2-encuesta-nacional-
de-nutricion-y-salud-ennys-2-resumen-ejecutivo/.
Online; accessed 3 oct 2020.
Srinivasan, S., Bao, W., Wattigney, W., et al. (1996). Ado-
lescent overweight is associated with adult overweight
and related multiple cardiovascular risk factors: the
bogalusa heart study. Metabolism, 45(2):235–240.
Sturm, R. (2002). The effects of obesity, smoking, and
drinking on medical problems and costs. Health Af-
fairs, 21(2):245–254.
Talukdar, D., Seenivasan, S., Cameron, A., et al. (2020).
The association between national income and adult
obesity prevalence: Empirical insights into tempo-
ral patterns and moderators of the association using
40 years of data across 147 countries. PloS One,
15(5):e0232236.
Tan, R. and Pu, S. (2002). Impact of obesity on hypogo-
nadism in the andropause. International Journal of
Andrology, 25(4):195–201.
Thomas, D., Weedermann, M., Fuemmeler, B., et al.
(2014). Dynamic model predicting overweight, obe-
sity, and extreme obesity prevalence trends. Obesity,
22(2):590–597.
Van de Kassteele, J., Hoogenveen, R., Engelfriet, P., et al.
(2012). Estimating net transition probabilities from
cross-sectional data with application to risk factors
in chronic disease modeling. Statistics in Medicine,
31(6):533–543.
Van Hooff, M., Voorhorst, F., Kaptein, M., et al. (2004).
Predictive value of menstrual cycle pattern, body mass
index, hormone levels and polycystic ovaries at age 15
years for oligo-amenorrhoea at age 18 years. Human
Reproduction, 19(2):383–392.
Wang, L., Denniston, M., Lee, S., et al. (2010). Long-term
health and economic impact of preventing and reduc-
ing overweight and obesity in adolescence. Journal of
Adolescent Health, 46(5):467–473.
Ward, Z. J., Long, M. W., Resch, S. C., et al. (2017). Simu-
lation of growth trajectories of childhood obesity into
adulthood. The New England Journal of Medicine,
377:2145–2153.
World Health Organization (2003). Controlling the global
obesity epidemic. https://www.who.int/nutrition/
topics/obesity/en/. Online; accessed 9 sep 2020.
World Health Organization (2016). Obesity and over-
weight. https://www.who.int/news-room/fact-sheets/
detail/obesity-and-overweight. Online; accessed 9 sep
2020.
Xue, H., Slivka, L., Igusa, T., et al. (2018). Applications
of systems modelling in obesity research. Obesity Re-
views, 19(9):1293–1308.
Mathematical Model for Estimating Nutritional Status of the Population with Poor Data Quality in Developing Countries: The Case of Chile
415
