
Custom FHIR Resources Definition of Detailed Radiation Information
for Dose Management Systems
Abderrazek Boufahja
a
, Steven Nichols
b
and Vincent Pangon
c
GE Healthcare, Strasbourg, France
Keywords:
FHIR
R
, DICOM
R
, Dose, Radiation, RDSR.
Abstract:
Medical diagnostic imaging dose management systems aggregate and calculate irradiation dose generated
by acquisition modalities, collected through standardized methods such as DICOM
R
, HL7
R
or proprietary
interfaces. Irradiation dose information is valuable to multiple stakeholders, such as, general practitioners
(GP), nationalized dose registries, patient facing applications, and information systems, such as, the Radiology
Information System (RIS) or Electronic Health Record (EHR). For Medical Physicists, the radiation data is
used to perform patient cohort and statistical analysis as part of a dose management program. However, there is
no standardized, lightweight method to exchange the collected dose information with third party applications,
through RESTful APIs. In this paper, we define a methodology to expose the content of the Radiation Dose
DICOM
R
SR data models as custom HL7
R
FHIR
R
resources. This methodology leverages the strength of
FHIR
R
in defining and exchanging resources, and the strength of the DICOM
R
SR data models, as their
structure is implemented, maintained, and tested by dozens of modality providers.
1 INTRODUCTION
In recent years, dose management systems have
played an increasingly important role within the fleet
of applications inside hospitals, assisting in compli-
ance with regional and national regulations, and im-
proving the safety of irradiated patients (R. Loose,
2020). Dose management systems gather technical
information from modalities and demographic and
clinical observation data from other various facility
applications. Some dose management systems pro-
vide functionalities for the enhancement of dose in-
formation through calculations and analyzes, such as
effective dose calculation, organ dose, size specific
dose estimation (SSDE), etc. Where IHE profiles
and DICOM
R
specifications have been established
to normalize the exchange between modalities and
dose management systems (IHE, 2020b) (IHE, 2016),
there has been no standardization exposing the dose
information from the dose management systems to
third party applications through RESTful APIs. Such
exposure should include both the collected and en-
hanced data. In this paper, we first describe the prob-
lem and the need for ”API-zation” of dose informa-
a
https://orcid.org/0000-0002-6481-2185
b
https://orcid.org/0000-0002-4873-1676
c
https://orcid.org/0000-0001-5031-8525
tion exposure. Then, we detail the methodology for
taking advantage of the rising HL7
R
FHIR
R
standard
(Fast Healthcare Interoperability Resources) (HL7,
2019). Finally, we perform a comparison between the
described methodology and another possible solution.
2 PROBLEM
The dose irradiation information is collected from
multiple sources. The most standardized structure
is the DICOM
R
Radiation Dose Structured Report
(RDSR) based structures. There are four RDSR struc-
tures allowing to expose the dose information and de-
fined in PS3.16 of the DICOM
R
standard (DICOM,
2020c):
• X-Ray Radiation Dose SR
• CT Radiation Dose SR
• Radiopharmaceutical Radiation Dose SR
• Cone-beam CT Radiation Dose SR (WIP)
Each of these structures define a complete struc-
tured report of irradiation events. Radiation expo-
sure information can be collected from other kinds
of messages, as well. For instance, some modalities
share the dose information through MPPS messages.
Boufahja, A., Nichols, S. and Pangon, V.
Custom FHIR Resources Definition of Detailed Radiation Information for Dose Management Systems.
DOI: 10.5220/0010251104670474
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 467-474
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
467

Also, some DICOM
R
images contain relevant dose
information, like nuclear medicine images (R. Loose,
2020). The most structured definition of radiation ex-
posure information are RDSR DICOM
R
objects.
The IHE Radiology domain defined two IHE inte-
gration profiles: REM (Radiation Exposure Monitor-
ing) (IHE, 2020b), and REM-NM (Radiation Expo-
sure Monitoring for Nuclear Medicine) (IHE, 2016).
The aim of these profiles is to define the actors in-
tervening in patient radiation exposure process, their
roles and the different transactions performed be-
tween them. REM profiles the X-Ray Radiation Dose
SR and the CT Radiation Dose SR; and REM-NM
profiles the Radiopharmaceutical Radiation Dose SR.
The aim of both integration profiles is to describe how
the dose information transits between modalities or
radiopharmaceutical activity suppliers and the dose
registry actors. During the process of sharing the dose
information with the dose registry, the dose consum-
ing actors may enhance the dose content with calcu-
lated information, like the effective dose, the organ
dose, or the size specific dose estimation methods.
Once the original and the enhanced dose informa-
tion are stored in the dose registry, which could be
a hospital based registry or a regional/national based
registry (IHE, 2020a), there is a need to expose the
radiation information to third parties in a lightweight
manner. Exposing the complete RDSR is useless for
most of the use cases:
• Most of the display applications need only few
parts of the RDSR
• Many third party applications are specialized in
specific dose information like the effective dose,
the organ dose, or the size specific dose estima-
tion. However, these applications cannot access
such specific dose information without retrieving
the entire RDSR.
• Backend applications performing cohort search
and measures need efficient data structures to
query information within the RDSR
Partial exposure of the RDSR contents is needed.
However, there is no lightweight methodology facil-
itating access to the dose information content within
the RDSR from the dose management system to the
third party applications.
Many healthcare systems can benefit from the
exposure of dose details from the dose reg-
istry/repository actors:
• Mobile applications: new dose related mobile
applications may benefit from the exposure of
the information in the dose management systems.
Such applications could follow accumulated pa-
tient dose exposure in a multi-facility enterprise.
Figure 1: IHE REM/REM-NM profiles description.
• RIS: Radiology Information Systems may bene-
fit by retrieving dose data for inclusion in the fi-
nal imaging report, as mandated by multiple na-
tional/regional regulations promoting the sharing
of dose information (IHE, 2020a).
• EHR: Electronic Health Record systems can ben-
efit from sharing dose information, as some utilize
manual entry of dose, and many do not support
the ingestion and analysis of DICOM
R
objects,
especially SR objects. A REST based API allows
simple integration of dose information within the
EHR system. Dose information can be provided
to practitioners for appropriate procedure selec-
tion during a diagnostic encounter.
• CQMS: Clinical Quality Management Systems
can benefit from lightweight exposure of dose in-
formation, in order to provide different metrics for
a multitude of stakeholders. These metrics can
be used to compare facilities, patient cohorts, or
even, regional practices as part of a comprehen-
sive quality control program.
• Third party application backends: some third
party applications may use the exposed dose in-
formation for other uses. For example, technical
exposure factors of previously performed exams
for a specific patient can be used by the modality
operator to set parameters of the current exam.
• Third party dose registries: API based exposure
can facilitate reconciliation between multiple dose
registries implementing the same API.
The most widely used standard for exposing APIs
and resources in healthcare domain is FHIR
R
, which
fits our problem well.
HEALTHINF 2021 - 14th International Conference on Health Informatics
468

3 STATE OF THE ART
3.1 Dose Summary on FHIR
An ongoing work item within the DICOM
R
WG-
20 and the HL7
R
O&O (Orders and Observations)
group analyses the specification and the profiling of
the Dose Summary on FHIR
R
(DICOM, 2020a). The
aim of this working item is to describe the minimal re-
quired dose information within a normative resource
(likely the Observation resource), allowing commu-
nication of the accumulated dose information from
the performed procedure step, to provide a summary
overview of the patient dose exposure. This working
item will involve several activities, like the identifica-
tion of the minimal dose information from various na-
tional regulations and recommendations, and the pro-
filing of the Observation resource in order to integrate
the minimal dose information. The scope of the Dose
Summary on FHIR
R
is to share a summary of dose in-
formation by exam through FHIR
R
, which is different
than the scope of this analysis: sharing details of the
radiation administration, and sharing of the enhanced
data like SSDE and effective dose to third party appli-
cations.
3.2 DICOM SR to FHIR Mapping
Another ongoing work item is a mapping be-
tween DICOM
R
SR and FHIR
R
resources (DICOM,
2020b). The scope of this work item is to map key
SR templates and content into FHIR
R
resources. At
the time of this paper, the work item was concentrated
in the mapping of measurement TIDs (Template IDs:
TID1410, TID1411, and TID1420). There are two
explored solutions: Observation based solution, and a
CDA
R
based solution. The first solution is describing
all elements inside the TIDs using the ”hasMember”
and ”component” attributes. The second solution is
to translate the SR into CDA
R
, following DICOM
R
PS3.20 (DICOM, 2020d). After CDA
R
mapping, a
translation between CDA
R
and FHIR
R
can be per-
formed using custom resources, following the project
Clinical Document Architecture V2.1 (HL7, 2020a).
The methodology is very interesting, as it allows the
direct mapping from SR templates to custom FHIR
R
resources. However, this is less relevant for DICOM
R
Radiation SR templates. In fact, in PS3.20, there is
only one CDA
R
section defined, summarizing the pa-
tient dose exposure. This section is useful for the
Dose Summary on FHIR
R
work item; however, it is
not useful for a detailed mapping between DICOM
R
RDSRs and FHIR
R
resources.
3.3 DICOM SR and FHIR
Representations for Imaging
Measurements
An analysis was performed within the 30th Project
Week event, in order to convert the TID 1500 - Mea-
surement Report, to FHIR
R
resources (H. Meine,
2019). The working team concluded that the FHIR
R
resources should be used to store only the most rele-
vant information, and to keep DICOM
R
as main stor-
age format. A python based project is shared in a
GitHub repository to describe the different samples
and code used to generate the FHIR
R
resources. From
the samples provided, the targeted mapping between
TID 1500 and FHIR
R
is based on combination be-
tween the resources DiagnosticReport, Observation
and ImagingStudy.
4 METHODOLOGY
4.1 Apization of DICOM Radiation SR
The best way to expose detailed radiation informa-
tion through an API is to combine the strength of
FHIR
R
(HL7, 2019) (T. Benson, 2016), and the sta-
ble structure of the RDSRs coming from PS3.16
(DICOM, 2020c). HL7
R
FHIR
R
provides a strong
API model and capabilities for searching and ex-
posing resources, like indexing and searching oper-
ations. The FHIR
R
community has published nu-
merous open source tools, simplifying any integration
with a FHIR
R
server, and simplifying the creation
of FHIR
R
servers. FHIR
R
also comes with defined
primitive and complex types, ready for use. Compar-
ing to proprietary APIs, FHIR
R
facilitates conception
of custom resources and the profiling of existing re-
sources, which reduces the time to production. In
fact, many open source applications exist, facilitat-
ing the profiling of FHIR
R
resources. Examples in-
clude FHIR
R
Shorthand / Sushi (HL7, 2020b), SIM-
PLIFIER.NET (K. Gopinathan, 2018), and FHIR
R
IG
publisher tool (HL7, 2020d). For custom resources,
HL7
R
provides FHIR
R
spreadsheet authoring, an Ex-
cel or OpenOffice structure for designing FHIR
R
data
types, resources, and profiles (HL7, 2020c).
DICOM
R
PS3.16 provides a complete definition
of each RDSR type, with a clear definition of con-
tent items, cardinality, data type, format, and con-
straints. The structure of the RDSRs have been de-
fined since 2004 and tested hundreds of times during
testing events like IHE Connectathons, or directly in
production. Their structure has evolved over the years
Custom FHIR Resources Definition of Detailed Radiation Information for Dose Management Systems
469
but can be considered as having a stable structure and
content.
Our methodology takes advantage of both stan-
dards: we defined FHIR
R
resources using the ele-
ments and the structures defined in PS3.16 of the
DICOM
R
standard. For each defined container in the
DICOM
R
RDSR structure, a custom FHIR
R
resource
is defined. For each container, a list of rules is fol-
lowed to create the custom resource. A custom re-
source may also be a subset of a container defining a
node with a considerable number of nested levels.
4.2 Mapping between Dose SR and
FHIR Resources
Each Dose SR can be described as a tree of different
TIDs. Each TID can be a container of elements, or a
tree of containers. Each container is described in the
defined API as a custom FHIR
R
resource. For exam-
ple: TID 10003 (Irradiation Event X-Ray Data) (DI-
COM, 2020c) describes the container with the iden-
tifier EV (113706, DCM, ”Irradiation Event X-Ray
Data”).
For a specific dose container, a custom resource
is created. A container is not always described by a
TID. In fact, a TID can describe multiple containers as
well as a subset of a container. This nuance is impor-
tant for the definition of the FHIR
R
custom resources.
Let’s consider for example the CT Radiation Dose SR
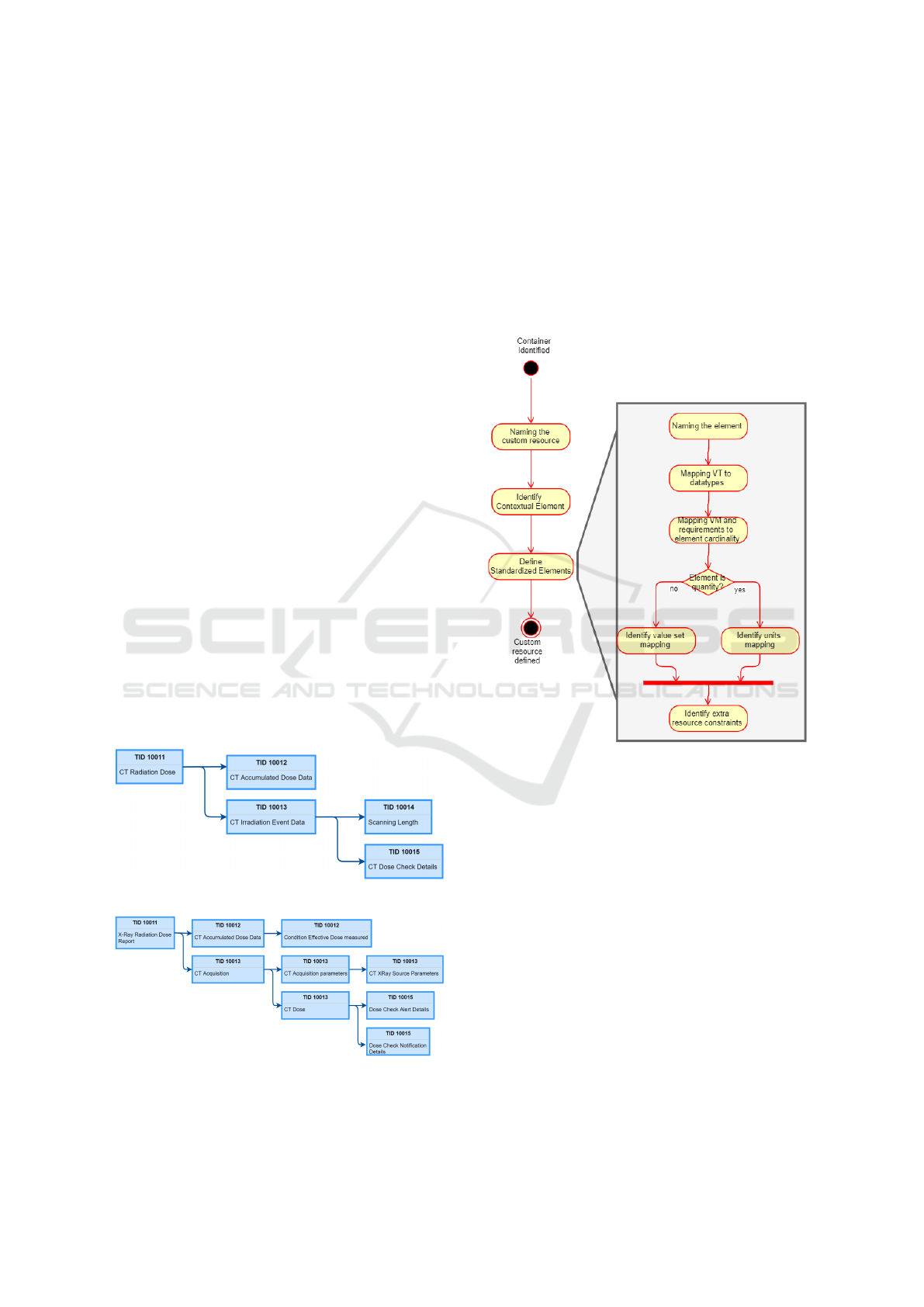
IOD Templates. The figure 2 describes the TIDs re-
lationship, and the figure 3 describes the containers
relationship, within the same IOD.
Figure 2: CT Radiation Dose SR IOD TIDs relationship.
Figure 3: CT Radiation Dose SR IOD containers relation-
ship.
We note that the tree of containment is not the
same. Containers relationship is better suited as unit
for FHIR
R
resources definition than the DICOM
R
TIDs. In fact, the containers have a better granular-
ity than TIDs and can be shared independently from
the rest of the structured report. Example: in TID
10013, CT Acquisition parameters may be shared be-
tween multiple RDSRs generated by the same modal-
ity.
The figure 4 describes the workflow used to define
custom resources based on the identified container.
Figure 4: Workflow to define custom FHIR
R
resources
from Radiation DICOM
R
templates.
The first step is to name the custom resource. The
name is based on the code used to identify the con-
tainer. Each custom resource contains two kinds of
elements: contextual elements and standardized ele-
ments. The second step is to define contextual ele-
ments. They are defined based on the contextual us-
age of the resource. Contextual elements describe the
context of the resource, such as encounter informa-
tion, patient identification, performed exam identifi-
cation, exam description, and exam date.
The third step is to identify the standardized ele-
ments, their cardinalities, datatypes, and constraints.
For each content item in the TIDs, an element or a
sub-element in the FHIR
R
custom resource is created.
We applied the following rules:
• The concept name defines the name of the FHIR
R
element, using the name of the attribute in lower
camel case. Example: the content item with the
HEALTHINF 2021 - 14th International Conference on Health Informatics
470
value EV (113764, DCM, ”Acquisition Plane”) is
transformed into element with the name ”acquisi-
tionPlane”.
• The level of the content item is respected, i.e. the
Nesting Level (NL) in the parent container is the
same as in the custom FHIR
R
resource.
• The relationship with parent is ignored.
• The VT (Value Type) is mapped with its cor-
responding primitive or complex types. Table
1 describes the mapping between VT types and
FHIR
R
datatypes.
• The Value Multiplicity (VM) and Requirement
Type (Req Type) define the cardinality of the el-
ement in the defined custom resource. The cardi-
nality of the FHIR
R
elements is based on the com-
bination of the values of both VM and require-
ment type. The table 2 describes the mapping
to FHIR
R
cardinalities as identified by our anal-
ysis. This table was partially described in PS3.16,
paragraph ”6.1.7 - Requirement Type” (DICOM,
2020c).
• The value set constraints can define:
– The list of supported value sets if the element is
a CodeableConcept
– The unit of the element if it is of type quantity
• The Condition column defines the constraints re-
lated to the custom resource elements
Table 1: Mapping between VT values and FHIR
R
Datatypes.
VT values FHIR
R
Datatypes
CODE CodeableConcept
UIDREF string
TEXT string
DATETIME dateTime
NUM integer k decimal k quantity
IMAGE string
Table 2: Mapping between VM and Req type values, and
FHIR
R
Cardinalities.
VM Req Type FHIR
R
Card
1 M 1..1
1 U 0..1
1 MC 0..1
1-n M 1..*
1-n U 0..*
1-n MC 0..*
This methodology can be used to generate custom
resources for any kind of SR template, not only dose
information templates.
5 RESULTS
5.1 Custom Dose Resources Definition
The described methodology allowed the definition of
custom resources for the different Dose SRs. The
different custom resources are defined using FHIR
R
spreadsheet authoring structure, allowing generating
a Dose Implementation Guide (IG) by leveraging the
FHIR
R
IG publisher tool. The generated IG facili-
tates communication with third parties as it follows
the FHIR
R
IG publisher style. Let’s take the exam-
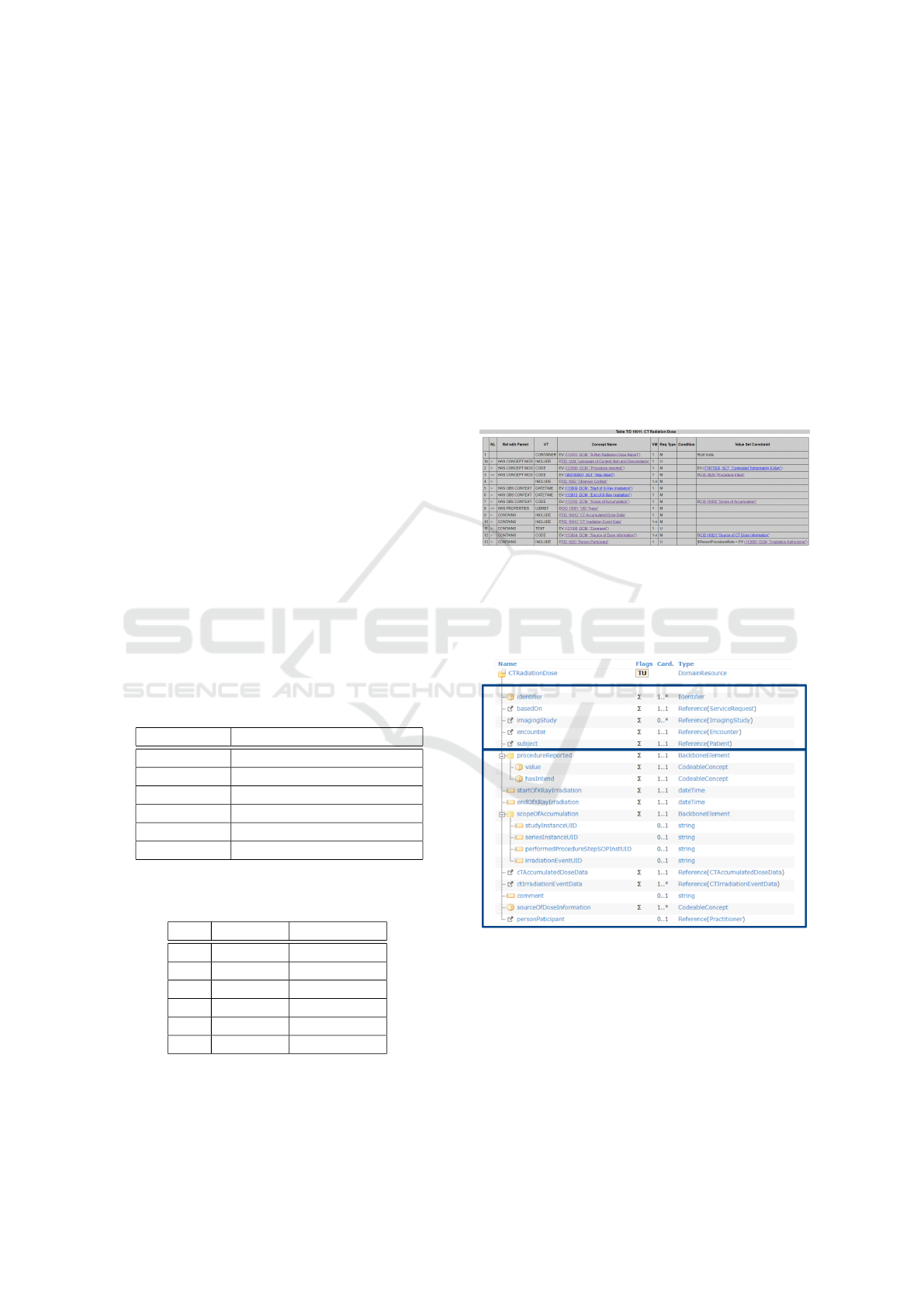
ple of the TID 10011: CT Radiation Dose. Figure 5
describes the structure of this TID as described in the
DICOM
R
standard, PS3.16 (DICOM, 2020c).
Figure 5: TID 10011 - CT Radiation Dose.
This TID contains a parent container item, which
translated then into a custom FHIR
R
resource. Figure
6 shows the mapping between the TID items and the
FHIR
R
resource elements.
Figure 6: Custom FHIR
R
resource for the TID 10011 - CT
Radiation Dose.
Note there are two parts: the contextual elements
and the standardized elements. In this example, the
contextual elements are: identifiers of the resource,
serviceRequest, imagingStudy, encounter, and pa-
tient. This information defines the context on which
the CT radiation dose was defined, and the different
related stakeholders.
The second part of the resource is the standard-
Custom FHIR Resources Definition of Detailed Radiation Information for Dose Management Systems
471

ized elements as defined in the DICOM
R
standard and
TID 10011. For example, the sourceOfDoseInforma-
tion is taken from the TID 10011, CT Radiation Dose,
under the content item number 12 (DICOM, 2020c),
and identified by EV (113854, DCM, ”Source of Dose
Information”). In the DICOM
R
standard, the related
content item has the Value Multiplicity (VM) of 1-n,
and the Requirement Type to ’M’; this is translated
to a FHIR
R
cardinality of 1..n in the custom resource,
based on the table 2 of mapping of cardinalities. In the
Content Item, VT is ’CODE’ with a defined value set
CID 10021 ”Source of CT Dose Information”, trans-
lated to the CodeableConcept from FHIR
R
datatypes.
Note that the nested levels are respected inside the
defined custom resource and the usage of the sum-
mary marker in the defined custom resource. This al-
lows summary of the resource and a lightweight query
to the dose management system when possible. The
identification of elements that need to be part of the
summary resource depends on the defined resource.
5.2 Comparison between Custom FHIR
Resources and Observation based
Solution
In this paper, we adopted a custom FHIR
R
resources
solution; however, there is another possible solution
to describe the different containers inside the RDSRs,
which is the Observation based solution. This solu-
tion is referenced in the DICOM
R
SR to FHIR
R
map-
ping working item from Imaging Integration WG (DI-
COM, 2020b). To profile dose SR through Observa-
tion resource, here are the steps that can be followed:
• When a content item is describing a container, or
has nested content items, or has the cardinality 1-
n, it shall be described as an independent observa-
tion.
• This observation shall follow these rules:
– Its code element shall follow the code from
DICOM
R
content item definition
– If it does not have nested content items, it shall
have a value element and no components
– If it has nested content items, it may have ”has-
Member” and component elements.
∗ If a nested content item is translated into Ob-
servation, it shall be referenced in the ”has-
Member” element
∗ If the nested content item is not translated
into observation resource, a component ele-
ment needs to be defined, with a slicing using
the code identifier of the content item.
Following these rules, an example of profiling the
Observation resource to cover the CT Radiation Dose
is described in the picture 7. We used FHIR
R
Short-
hand for the profiling process (HL7, 2020b).
Figure 7: CT Radiation Dose profiled through Observation
resources.
This profiling allows description of the CT radi-
ation dose contents inside an Observation resource,
with three additional nested Observation resources.
Even if the same data elements are described in this
structure of resource, the complexity of the structure
is higher in the Observation based solution compared
to the custom resources based solution: four Obser-
vation resources are used instead of one custom re-
source. Also, the use of component instead of custom
elements increases the complexity of searching of the
data inside the resource. For instance, collecting the
endOfXRayIrradiation is less complex in the custom
resource than in the Observation based resources. The
table 3 compares the characteristics of each solution.
The following metrics describes the improve-
ments between custom resource solution and an ob-
servation based solution. A sample of 500 resources
were selected, 250 custom resources and 250 Obser-
vation resources, describing the same CTRadiation-
Dose data. Four metrics were analyzed:
• The number of characters generated (describing
the network footprint)
• The number of lines generated in pretty format
(describing the complexity of the structure)
• The response time from the hosting server
• The laps of time to perform a marshalling from
JSON to Java
We calculate the average of the metrics for each
solution and we divide the value found for custom re-
sources by the value found for Observation resources.
HEALTHINF 2021 - 14th International Conference on Health Informatics
472
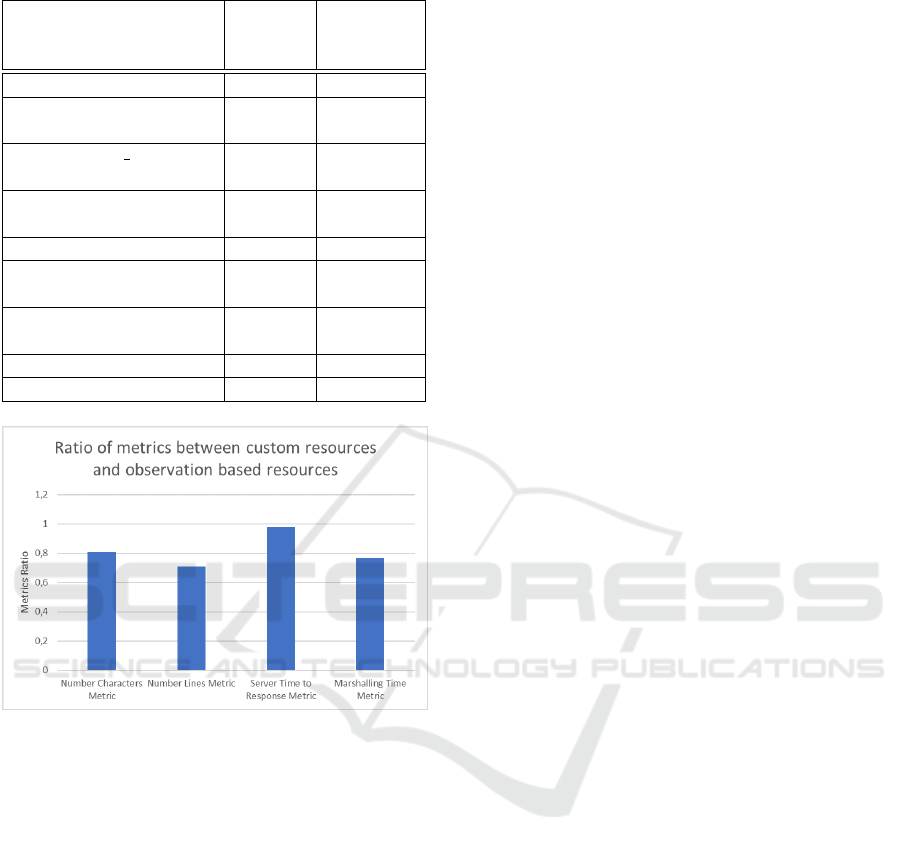
Table 3: Custom resources vs Observation based resources.
Custom
resource
solution
Observation
based so-
lution
Small network footprint X X
Ease of interpretation by
tools
X X
Supports ” summary”
option
X X
Lower processing foot-
print
X X
Human readability X X
Less concepts manage-
ment
X X
Semantic/meaning of the
resource
X X
Ease of EHR integration X X
Ease of specification X X
Figure 8: FHIR
R
custom resources VS Observation based
resources performance.
The metrics analysis demonstrates an average of
20% improvement with custom resources compared
to the Observation resources. The better network
footprint results from a fewer number of exchanged
characters compared to the Observation resources.
The number of lines is also smaller in custom re-
sources versus Observation resources (an improve-
ment of 30%); this explains the better server response
time and marshalling time for custom resources.
Custom resources support the definition of ele-
ments as summary elements, which also allows im-
provement in the network footprint, in some use
cases. In custom resources, there is no need to main-
tain identifying concepts of components and codes of
observations. Also, as radiation information is not a
typical observation, we estimate that the meaning of
the custom resource is more appropriate than in ob-
servation based resources.
A major advantage of using the observation based
solution is the ease of integration with existing EHRs.
In fact, most EHRs supporting FHIR
R
already include
FHIR
R
server, and integrating a profiled observation
resource is much easier than integrating a custom re-
source, which may need additional effort by the EHR
providers. For instance, US Core (HL7, 2020e) is us-
ing the Observation resource to profile many health-
care data like patient BMI, heart rate, body temper-
ature, etc.; this profiling simplifies the adoption by
EHRs. From specification perspective, FHIR
R
re-
sources profiling is easier than defining custom re-
sources, as there are many tools allowing to pro-
file FHIR
R
resources like FHIR
R
Shorthand (HL7,
2020b) or SIMPLIFIER.NET (K. Gopinathan, 2018).
6 CONCLUSION
In this paper, we described our methodology for de-
tailing dose information through custom FHIR
R
re-
sources. This methodology takes advantages of both
the FHIR
R
and DICOM
R
standards: from one, it
takes advantage of the normalization of resources ex-
change, basic datatypes, and existing tooling; from
the other, it takes advantage of the stability of struc-
tures defined within the RDSR templates. This
methodology brings added value to dose management
systems, especially through third party applications.
The defined methodology opens new perspectives for
dose management systems to integrate with hospital
ecosystem, as a provider of enhanced dose data, and
not simply as a consumer of dose information from
modalities. This methodology proves its strengthen
in multiple aspects compared to an Observation based
solution. The exposition of the dose resources im-
proves the communication by normalizing data ex-
change between applications, and simplifying the in-
tegration with patient facing applications, or business
intelligence programs. Although the methodology
proved its strengthen and its multiple possible appli-
cations, an effort to normalize the different custom re-
sources needs to be performed with a greater level of
FHIR
R
community participation, for standardization
and adoption.
ACKNOWLEDGEMENTS
We acknowledge strong GE Healthcare support dur-
ing this study from Performance Intelligence Analyt-
ics and DoseWatch engineering team.
Custom FHIR Resources Definition of Detailed Radiation Information for Dose Management Systems
473

REFERENCES
DICOM, I. I. (2020a). Dose Summary on FHIR.
https://confluence.hl7.org/display/IMIN/Dose+
Summary+on+FHIR. Accessed: 2020-11-22.
DICOM, I. I. (2020b). Mapping of DICOM SR
to FHIR. https://confluence.hl7.org/display/IMIN/
Mapping+of+DICOM+SR+to+FHIR. Accessed:
2020-09-28.
DICOM, S. C. (2020c). DICOM Standard PS3.16 2020c -
Content Mapping Resource. NEMA.
DICOM, S. C. (2020d). DICOM Standard PS3.20 2020c,
Imaging Reports using HL7 Clinical Document Archi-
tecture. NEMA.
H. Meine, Oppermann P., e. a. (2019). ProjectWeek:
Roundtrip conversion between DICOM SR and FHIR
representations for imaging measurements. https:
//projectweek.na-mic.org/PW30 2019 GranCanaria/
Projects/DICOMSRTID1500-FHIR/. Accessed:
2020-09-28.
HL7 (2019). FHIR (Fast Healthcare Interoperability Re-
sources) Specification. HL7, release 4 edition.
HL7 (2020a). Clinical Document Architecture V2.1.
https://build.fhir.org/ig/HL7/cda-core-2.0/. Accessed:
2020-09-28 - continuous build for version 2.1.0.
HL7 (2020b). FHIR Shorthand. https://build.fhir.org/ig/
HL7/fhir-shorthand/. Accessed: 2020-09-28 - contin-
uous build for version 1.0.0.
HL7 (2020c). FHIR Spreadsheet Authoring.
https://confluence.hl7.org/display/FHIR/FHIR+
Spreadsheet+Authoring. Accessed: 2020-09-28.
HL7 (2020d). IG Publisher documentation.
https://confluence.hl7.org/display/FHIR/IG+
Publisher+Documentation. Accessed: 2020-09-
28.
HL7 (2020e). US Core Implementation Guide STU3, v3.1.1
edition.
IHE, R. (2016). Technical Framework Supplement, Ra-
diation Exposure Monitoring for Nuclear Medicine
(REM-NM). IHE, rev. 1.1 edition.
IHE, R. (2020a). Appendices to Integration Profiles, Ap-
pendix I: Deployment of Dose Registries. IHE, rev. 19
edition.
IHE, R. (2020b). Technical Framework Volume 1, Radiation
Exposure Monitoring (REM). IHE, rev. 19 edition.
K. Gopinathan, NA. Kaloumenos, e. a. (2018). FHIR FLI:
An Open Source Platform for Storing, Sharing and
Analysing Lifestyle Data. ICT4AWE.
R. Loose, E. Vano, e. a. (2020). Radiation dose manage-
ment systems - requirements and recommendations
for users from the ESR EuroSafe Imaging initiative.
European Radiology.
T. Benson, G. G. (2016). Principles of Health Interoper-
ability. Springer, Cham.
HEALTHINF 2021 - 14th International Conference on Health Informatics
474
