
Challenges in Developing Software for the Swedish Healthcare Sector
Bilal Maqbool
a
and Sebastian Herold
b
Department of Mathematics and Computer Science, Faculty of Health, Science and Technology, Karlstad University,
Karlstad, Sweden
Keywords:
eHealth, Software Development, Exploratory Study, Empirical Study, Interview Study.
Abstract:
Context: High-quality software is essential to the progressing digitalisation of the Swedish healthcare sector.
Developing software with the desired high quality is far from trivial due to the sophisticated requirements of
the domain. Problem: Studies on healthcare digitalisation challenges in Sweden and other countries, however,
largely focus on the perceptions of healthcare professionals and patients and less on opinions of IT profession-
als. Method: In this exploratory study, we conducted semi-structured interviews with nine IT professionals
about observed challenges in developing software for the Swedish healthcare sector. A qualitative analysis
was performed to identify common themes. Results: We identified the prevalent challenges to be related to
data integrity, privacy and security, rules and regulations, engineering usability, and software testing. Con-
clusion: The results suggest that further research is required regarding agile methods, efficient requirement
engineering, and testing in eHealth as well as in privacy and usability engineering.
1 INTRODUCTION
Since the late 1990s (Della Mea, 2001), modern in-
formation and communication technology has been
used around the world in healthcare (Bhavnani et al.,
2016). Electronic health records (EHR), patient por-
tals, and mobile applications are just some exam-
ples of tools applied to manage and monitor patients’
health (Ventola, 2014). Among the promises of the
progressing digitalisation of the healthcare sector are
increased efficiency, reduced administrative burden,
better insights for patients into their health, and over-
all reduced costs for the public healthcare (Ventola,
2014). Studies also suggest that eHealth is likely to
have a positive effect on the quality life both physi-
cally and psychologically (Wiklund Axelsson et al.,
2013).
eHealth solutions have become an integral part of
Sweden’s healthcare sector, too (Bjorkman, 2019).
For example, 95% of the documentation in the pri-
mary care is stored in EHR and 99% of pharmaceuti-
cal prescriptions are issued electronically (Bjorkman,
2019). Sweden spends approximately USD 1.2 bil-
lion annually for eHealth and has the strategic vision
to become a “Health Tech Leader” by 2025 (Bjork-
man, 2019).
The development of eHealth systems involves
great responsibility as the patient’s health and life
a
https://orcid.org/0000-0002-1309-2413
b
https://orcid.org/0000-0002-3180-9182
may depend on them (PwC, 2016). This particu-
larly applies to software, which is an essential part
of almost every eHealth system (PwC, 2016). Devel-
oping software for the healthcare sector is very de-
manding due to diverse requirements that software
solutions have to fulfill (Magrabi et al., 2019). The
need to meet high demands regarding safety (Holl-
mark et al., 2015; Rydenf
¨
alt et al., 2019; Frennert
and Baudin, 2019), security (Jung and Loria, 2010;
Hollmark et al., 2015;
¨
Ostlund, 2017; Barkman and
Weinehall, 2017), compliance with regulations (Holl-
mark et al., 2015;
¨
Ostlund, 2017; Svanborg-Sj
¨
ovall,
2014) and others require adequate methods and pro-
cesses to deliver high-quality eHealth solutions (Holl-
mark et al., 2015). Failing to maintain software qual-
ity can result in severe danger to patients’ health and
life (Galin, 2005) as well as to the credibility of the
software provider. For example, in a recent inci-
dent, recordings of patients seeking medical advice
via telephone were openly accessible because they
had been stored without proper encryption or authen-
tication mechanisms (BBC, 2019). This incident did
not only raise privacy and security concerns but also
damaged the credibility of the organizations involved.
While the digitalisation of the sector progresses,
investigating the challenges at hand as perceived by
the relevant stakeholders may provide valuable in-
sights in order to address open research gaps. Ex-
isting studies have mainly focused on the perceptions
of healthcare professionals and patients as the main
user groups of software in the domain. Studies that
take into account the complementing view of software
system and system providers are very scarce though.
In this study, we therefore describe the results of
analyzing semi-structured interviews with IT profes-
sionals about their perceptions regarding challenges
in developing software for the Swedish healthcare
sector. The objective is to identify potential short-
comings and research gaps in software development
methods applied for the healthcare domain.
The outline of the paper is as follows: In Sec. 2,
we will discuss related work. In Sec. 3, we explain
the chosen research methodology. Sec. 4 reports on
the findings of the study which are then discussed in
Sec. 5. The article ends with concluding remarks and
an outline of future work in Sec. 6.
2 RELATED WORK
For this section, published studies on the challenges
of using, developing and implementing Swedish
eHealth solutions/services were considered relevant.
In 2007, a qualitative study was conducted among
Swedish tele-nurses who were interviewed to explore
reasons for decision aid software not being used as in-
tended (Holmstrom, 2007). It was found that among
the most important reasons were usage for assessment
only due to insufficient decision making support, in-
consistencies with clinical practices, and difficulties
in learning how to use the system. As a consequence,
participants reported to often discard recommenda-
tions provided by the system and using self-care ad-
vice to a large extent.
Jung and Loria conducted interviews to identify
barriers and intentions in the acceptance of Swedish
eHealth services by the elderly (Jung and Loria,
2010). They concluded that ease of use, trust in ser-
vice, and compatibility with citizen’s needs were the
main acceptance factors. It was added that better in-
formation about eHealth services are needed to in-
crease awareness for these services such that elderly
people can optimally utilize them.
In 2015, a study reviewed the literature to dis-
cuss challenges for implementing eHealth in Swe-
den and efforts done to overcome them (Hollmark
et al., 2015). General problems were identified simi-
lar to those that other researchers reported around the
world, such as interoperability, reimbursement, reg-
ulatory, and usability issues. The authors concluded
that interoperability efforts and standardization, better
communication between developers and stakeholder,
and developer expertise in safety, security and privacy
would be crucial for success.
In 2016, PwC conducted a survey involving doc-
tors and nurses from Sweden to understand their will-
ingness, needs, and perspectives regarding the trans-
formation of traditional healthcare to digital health-
care (PwC, 2016). According to this report, health-
care personnel fear the loss of face-to-face contact
with patients, and both care-givers and care-receivers
are worried about the potential negative impact on
the quality of care by using virtual care. Respon-
dents also have serious concerns about the failure of
such systems as the patient’s health can suffer badly.
Researchers suggest, at all levels, clear leadership is
needed, creating opportunities for better collaboration
between different healthcare provides and educating
and supporting staff to achieve a common goal, i.e.
Sweden’s 2025 vision.
In 2017,
¨
Ostlund discussed challenges in digitiz-
ing healthcare in Sweden based on her experiences in
that domain (
¨
Ostlund, 2017). She in particular noted
that requirements are often not gathered from the ac-
tual end-users, especially the elderly, and stressed that
active involvement of older users, and proactive and
cooperative efforts are crucial for the digitization of
healthcare. Moreover, she expressed that the health-
care sector needs to deal with the challenges of digital
arenas that would foster a better understanding the ef-
fect digitalisation in a controlled setting much closer
to the real environment.
Barkman and Weinehall conducted a comparative
study in Ethiopia, Ghana, and Sweden, comparing the
policymakers and mobile-based healthcare (Barkman
and Weinehall, 2017). According to the researchers,
despite the well-developed system, Sweden faces few
challenges: integration of health data, use of digital
decision support to develop personalized medicine,
future funding, and quality and efficiency of health-
care systems.
¨
Oberg et al. conducted focus group interviews to
identify Swedish primary healthcare nurses’ concerns
and perceptions regarding the implementation and us-
age of digital healthcare systems (
¨
Oberg et al., 2018).
Nurses were concerned because of the scope of their
operational responsibilities would potentially expand
and the need to adopt to new practices and policies as-
sociated with digital healthcare. The researchers con-
cluded that there is a dire need to educate and train
nurses so they can be involved in the eHealth imple-
mentation.
In 2019, a survey was conducted to study Swedish
home care nursing providers and found that respon-
dents have more expectations with remote monitor-
ing and automation (Rydenf
¨
alt et al., 2019). It was
highlighted that a lack of suitable infrastructure, sys-
tems’ inability to adjust the context of use, and usabil-
ity are currently primary challenges in implementing

and adopting eHealth services. Furthermore, the au-
thors predicted that the digitalisation may massively
affects the workflow in healthcare organizations.
Frennert and Baudin performed a survey study
among representatives of different professions work-
ing within Swedish municipal eldercare (Frennert and
Baudin, 2019). It aimed at identifying challenges
and opportunities related to welfare technology in
Swedish municipal eldercare. The results show that
despite the fact that welfare technology is consid-
ered reliable and secure, it still faces many challenges
that slow down its implementation. Lack of funding
and infrastructure, high staff turn-over, uncertainties
about responsibility and laws, and difficulties with
procurement are key found challenges. Among other
mentioned challenges, resistance to change is the
same factor as identified by other researchers (Jung
and Loria, 2010). Lack of structured implementation
processes, availability and usage differences between
municipalities raise further issues.
This summary of related work shows that a sig-
nificant amount of work has been carried out to ex-
plore challenges regarding digital healthcare in Swe-
den. This body of work mostly focuses on healthcare
professionals and their perceptions, such as literature
review about politicians, regulators, and policymak-
ers and their rules, regulations, and policies, inter-
viewing or surveying doctors, nurses, or other staff
members and comparative analysis between Sweden
and other countries’ eHealth sector. All work pre-
sented vital insights, but to the best of our knowl-
edge, no paper is concerned with challenges as per-
ceived by IT professionals producing systems for the
healthcare sector. This is a gap that we intend to
bridge to see whether and which software develop-
ment methodologies and techniques should be poten-
tially adapted/refined. That’s why this paper is first of
its kind; a comprehensive study conducted to explore
challenges in eHealth domain.
3 RESEARCH METHOD
The motivation for this study is to explore challenges
in developing software for the Swedish healthcare
sector as perceived by IT experts in order to identify
potential directions for research related to software
development methods. For this purpose, a qualitative
research design was chosen (Berg, 1989) as it allows
for a systematic exploration of the area based on peo-
ple’s opinions and experiences (Holmstrom, 2007).
Semi-structured interviews were chosen as mean of
data collection as they provide the flexibility to fol-
low up on thoughts and ideas not envisaged upfront
(Corbin and Strauss, 2014). In the following subsec-
tions, we describe the applied research protocol in de-
tail.
3.1 Participants and Setting
The participants were selected through purposive,
snowball (Oates, 2005) and opportunistic sampling,
aiming at getting the preferred level of participants
having a wide range of experience related to the de-
velopment of Swedish digital healthcare solutions.
The respondents were informed that their participa-
tion was completely voluntary and anonymous. All
information from the interviews was be anonymised
before the publication of any results. Table 1 gives an
overview of the participants (detailed table
1
). Eight
interviewees were employed by in total six different
companies. Another participant worked as indepen-
dent developer. Participants P1-P6 and P8-P9 belong
to national and international organizations, interact-
ing with distributed stakeholders and software devel-
opment teams. Eight male (P1-P6, P8-P9) and one
female (P7) of variant backgrounds were interviewed
for approximately one hour on their opinions, expe-
riences, and knowledge of challenges faced during
the development of digital healthcare and welfare sys-
tems or services. Participants have a combined ex-
perience of approx. 34.75 years (mean= 3.86, me-
dian= 1), experiences ranging from 4 months (P5) to
15 years (P1), roles ranging from a software devel-
oper (P3-P6) to CEO (P1) and responsibilities rang-
ing from software development (P3-P6) to managing
teams (P8) in Sweden’s digital healthcare and welfare
sector.
All participants except P4 and P5 have played
more than one role or responsibility during working
in digital healthcare and welfare. Moreover, all par-
ticipants had the experience of working in different
roles with diverse responsibilities in additional do-
mains other than the digital healthcare and welfare
sector. We considered this diversity among the in-
terviewees essential to gather well-founded and rep-
resentative insights regarding the domain of interest.
3.2 Data Collection
Data collection was done through semi-structured in-
terviews for which we developed a protocol with top-
level themes. These themes touched upon perceptions
of challenges and their priorities as well as poten-
tial solutions while leaving enough space for more
specific follow-up questions. Each interview took
1
https://drive.google.com/file/d/
1CmzAIlsHYL0fv6DP5u0TX4BYB7DMZzkn/view.
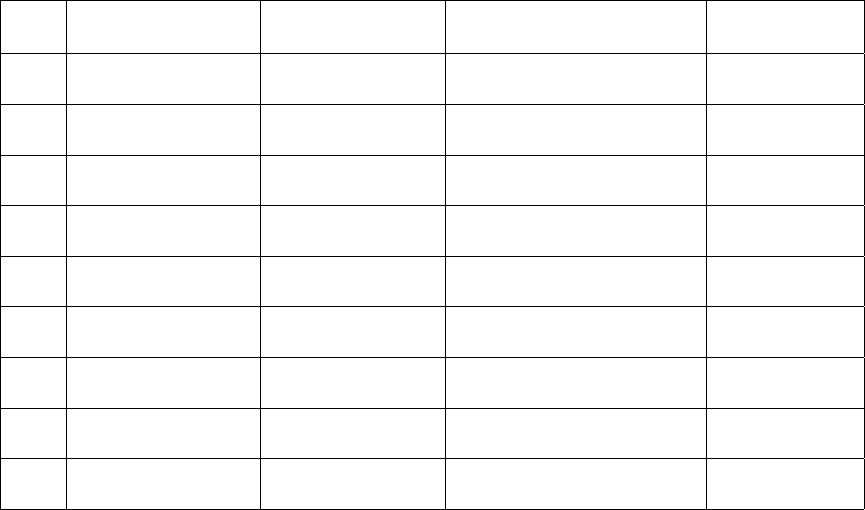
Table 1: Participant Information.
P. ID Domains/Systems
(Other)
Role
(eHealth)
Responsibilities
(eHealth)
Experience
(eHealth/Total)
P1 Finance
Gaming
Business Developer
CEO
Domain Exploration
Market Survey
15/15 years
P2 Education
Telecom
Software Tester
Team Lead
Planning & Impl. Test
Testing Support
6/20 years
P3 Commercial Apps
Navigation
Software Developer Requirement Elicitation
Software Development
4/5 years
P4 Commerce
Education
Software Developer Software Development <1/5 years
P5 Real Estate
Finance
Software Developer Software Development <1/9 years
P6 Navigation
Finance
Software Developer Design Architecture
Software Testing
1/4 years
P7 Gaming Researcher
Software Developer
Research
Software Development
<1/10 years
P8 Commerce Business Analyst Analyze Business
Software Testing
1/2 years
P9 Business Intelligence
Word Processor
Software Tester
Test Lead
Test and Report Software
Quality
6/22 years
about one hour and were carried out via remote au-
dio or video calls between February-May 2019 and
January-March 2020. The interviewees gave their
consent to be recorded such that the participating re-
searcher could transcribe the interviews. All inter-
view transcripts were cross-reviewed by the second
author. During the interview, participants were al-
lowed to call for a stop of the recording if they felt
uncomfortable with being recorded.
3.3 Data Analysis
The interpretation and analysis of research data are
comprised of epoche and bracketing (Braun and
Clarke, 2006). We tried to minimize the involvement
of our biased knowledge, and synthesis was done
using thematic analysis (Braun and Clarke, 2006).
Micro-analysis (open and axial coding) was con-
ducted to identify in-vivo codes (MacLure, 2013),
and meaning coding categories emerged from the data
during the analysis. In the inductive analysis, a mixed
model of open coding and pre or initial coding list
was used for overall analysis. The pre-coding list acts
as the initial point for discovering deeper ideas from
the research data and was later transferred into the
axial coding. We used the NVivo12 tool to perform
the analysis (Walsh, 2003). All coding types, includ-
ing open and axial codes, were tracked and mapped,
highlighting the codes, their connections, and emer-
gent codes.
We followed several stages to conduct qualitative
analysis. In the first stage, authors read the free-text
answers of each interview separately to familiarize
with data and to get a bigger picture of the interview
responses. In the next stage, the first author generated
initial codes by analyzing text in-depth and assigned
applicable codes to them (Charmaz, 2014). Mean-
while, the second author kept reviewing codes and the
initial analysis done by the first author. Then com-
ments and suggestions were made where required,
refining the overall analysis. In the next stage, the
first author performed the axial coding, and the sec-
ond author reviewed it in a similar routine. Interviews
and analyses were iteratively reviewed and discussed
during meetings between the authors. After agreeing
upon different comments and opinions, changes were
made. In the next stage, the authors analyzed for the
addition of new or deletion of old codes. In the fi-
nal stage, authors searched for themes, reviewed them
and then classified and characterized identified codes
into different themes.
3.4 Ethical Considerations
We have followed the guidelines given by the Swedish
Research Council for research ethics (Gustafsson
et al., 2017). Information gathered or observed dur-
ing the interview is reported and analyzed accurately
and honestly.
4 FINDINGS
The analysis of the interview data revealed challenges
that were categorized into five main themes. In the
following subsections, we present the findings for
each of the five themes.
4.1 Challenges Related to Integrity,
Privacy, Protection and Security
Data is considered a key component and that can be
used to automate systems and services in the digi-
tal healthcare sector. More and more data is stored
and available for processing. Hence, five out of nine
participants (P2, P4, P5, P8, and P9) discussed chal-
lenges related to data, i.e. data integrity, privacy, data
protection, and security.
P2, P8, and P9 rate data integrity as one of the
most critical challenges faced during the development
of eHealth systems. P2 and P9 noted that patients, es-
pecially doctors, have concerns about the integrity of
the data because it is essential for making decisions in
many health-related processes. P2 stated “...really im-
portant, the personal integrity and security for the pa-
tient” because the health of individuals or even lives
may depend on critical data (as P9 stated). P8 added
that IT professionals need to consider various aspects
related to data integrity, such as how data is handled
in an organization because handling data will affect
the integrity of the data. P9 referred to a problem of
doctors having incomplete data about patients nowa-
days as an example of the challenge of data integrity:
“Today we don’t have all data in Sweden... the doc-
tors are not sure that they see everything about the
patient... that could be a problem”. Complete patient
information should be available to the doctor because
a system based on incomplete data will have bugs,
and it does not optimally support professionals and
patients as P9 explained “we can’t miss the big bugs
that could affect the decision of a doctor...”.
Three participants, P4, P5, and P6, talked about
challenges related to data protection but P6 did not
perceive this as a high priority challenge and hence
did not consider it for further discussion. P4 discussed
issues that need to be taken into consideration after re-
ceiving patient data. IT professionals need to ensure
that data is protected from any loss or unauthorized
access such that patients can trust the system. P5 also
stressed the potential impact on market reputation and
expressed: “if you lose that (patient) data, I think you
lose your reputation within the market, since no one
is able to trust you guys, not your app, not your com-
pany”.
Two participants P4 and P5, perceived data pri-
vacy as one primary challenge faced during the devel-
opment of eHealth systems. Patient data is very confi-
dential, especially information regarding their disease
history. They expressed concerns about the conse-
quences of leaks of personal data that could like il-
legal sharing of patient data or offenses like black-
mailing. This challenge affects decisions taken re-
garding the process and approach taken for handling
patient data. While talking about PDA (Personal Dig-
ital Assistants), P4 gave an example: for “generating
an email... we should only use our mobile side, no
data should be kept at the server side due to the pri-
vacy”, to deal with such circumstances P4 mentioned
to use decentralized architectures.
According to participants P2 and P4, data security
is as important to the patient as the integrity of the
data. IT professionals have to ensure data security to
satisfy patients. Giving an example of data security,
a data-related challenge, P5 discussed the need to put
extra efforts during software development. If the sys-
tem lacks data security, it becomes a threat not only to
the organization but also to the patient. To ensure data
security, IT professionals need to add some additional
security layers.
Interviewees have a several recommendations on
how to address mentioned challenges. IT profession-
als need exhaustive software testing to ensure data
integrity, P9 stated “We need to do more and better
testing...” to make sure “. . . that the data isn’t lost
or transformed in some other way. It’s one typical,
very important testing”. The P8 recommends that
the software development team include people with
good knowledge of data integrity laws. This can help
in developing a product that complies with different
laws, regulations, or standards. The P8 spoke on data
handling and said that the workforce should be made
aware of the security rules and in compliance with
various regulations, especially the GDPR (EU’s Gen-
eral Data Protection Regulation). So, IT professionals
can ensure the security, accuracy and consistency of
data over its lifetime.
According to P5, decentralized architectures are
recommended to overcome data protection challenges
as there will be no single point of failure: “If one
server is compromised... 4 servers remain... if it’s
distributed. But you have to apply the security layer
on all, and you have to keep monitoring”. P6 briefly
added a common known solution to address data pro-
tection challenges by implementing data encryption.
P4 mentioned that developers should be given
clear instructions on technical protocols to ensure the
privacy and security of the developing system. While
giving an example of how to send data from a system,
P4 explicitly mentioned that HTTP protocols should
be used: “... for the protocols such as HTTP should be
used to send (data)”. In addition, other business or ad-
ministrative policies that may affect privacy and secu-
rity decisions should be clearly communicated by the
hospital or the client. Close collaboration between so-
lution providers and stakeholders can help to address
such privacy and security challenges.
There are many security protocols available, P5
thinks that by following the security protocols and us-
ing them, IT professionals can ensure data security.
P5 suggested that centralized architectures should be
used to ensure data security: “Whenever you get the
data, it should be centralized somewhere”. Among
other solutions, as P6 mentioned about data protec-
tion, P5 also mentioned that data encryption and mul-
tiple security layers are needed to ensure data security
in a system: during the development cycle, data “has
to be secured with... password protection and there
should be multiple layers” of security.
The interviewees experienced most of the chal-
lenges mentioned above in other domains, too. As
compared to the banking sector and other domains,
P4 and P5 perceived the severity of data privacy chal-
lenges as higher in the eHealth sector. P5 perceived
severity of data protection and data security chal-
lenges high in the eHealth sector compared to the
banking sector. P8 perceived data integrity challenges
to be of higher severity than in other domains while
P9 had not faced such challenges in other domains so
far.
4.2 Challenges Related to Software
Testing
Four participants (P2, P3, P7, and P8) discussed
software testing challenges. According to P2, the
Swedish healthcare sector has experienced significant
digital innovation, however, quality assurance and
testing were not taken seriously enough. This, accord-
ing to P2, resulted in poorly tested systems: “qual-
ity assurance and testing of these systems weren’t
prioritized” and “systems in this business (were) so
untested”.
Access to the real patient and other critical data
is often desirable for proper testing which is rarely
granted due to privacy and security concerns. As P7
stated “doctors were not willing to give me informa-
tion and of course I understand security reasons”.
Developers often use synthetic data for testing, which
carries the risk of not representing reality thoroughly.
This affects the efficiency of software development
as the creation of proper test data consumes signifi-
cant time. Regarding test environments, P9 said, if
there are many different systems under the control of
different stakeholders (public and/or private) then it
will be a major challenge to access patient informa-
tion for creating test environments without spending
more time and money on this task.
P3 additionally highlighted the lack of testing in-
struments, especially medical hardware or equipment
that could be used for real environment testing. Due
to this challenge, solution providers are unable to
provide accurate results during software testing and
cannot predict the actual performance of the system.
Buying medical hardware for testing purposes will in-
crease production costs: “This was really costly for
me.. and I bought... just for testing purposes”.
Having multiple and different stakeholders creates
communication problems, P8 said. It becomes diffi-
cult to collaborate and communicate within the com-
pany or with other stakeholders: “a lot of the stake-
holders... want to (get) stuff (done) and it’s hard
for every sector... of the company to cooperate and
communicate...”. P8 added, it also becomes hard to
get and set functional requirements as companies set
higher demands. Due to unclear functional require-
ments and unrealistic deadline organizations often
sacrifice testing periods, so solution providers may
not meet the demands and software quality. There
will be bugs in the delivery system and it will not
work as intended. P8 stated “... their requirement in-
creases... (and) buggy system can... not save people’s
lives... (we) need more longer tests period”.
According to P2, lack of quality assurance and
software testing prioritization has created an oppor-
tunity for companies to enter the eHealth domain but
companies need to take quality assurance seriously
and quality needs to be prioritized to overcome such
challenges. If IT companies have close collaboration
and patient data-sharing agreements with stakehold-
ers then companies can overcome the lack of access
to patient information challenges. P7 stated, “coming
up with this idea to do agreement... can easily access
the information or data they (developer or researcher)
want about the patient and use for their research”.
For P3, with increased collaboration between de-
velopers and stakeholders, availability and access of
medical hardware for testing, IT professionals can
overcome challenges related to the lack of testing in-
struments: “bridge between developers and the sector
(is needed), (in) which developers get access to more
hardware and sensors..., like for testing of eHealth
systems or apps”. P9 assumes that this will take time,
but by working closely with different stakeholders
and developing or integrating pre-existing test envi-
ronments, IT professionals can overcome the prob-
lems related to the test environment. P8 added that
more time needs to be spend on exhaustive testing
to ensure the correctness of the system. Moreover,
IT professionals can use agile practices to bridge the
stakeholder communication gap.
According to P2 and P7, the lack of software
testing prioritization and lack of access to relevant
patient data are high in the eHealth sector as com-
pared to the telecommunication domain. Participant
P3 mentioned that the lack of testing instruments was
a less pronounced challenge when testing navigation
systems and/or applications other domains he had
worked in before. The lack of testing environments
are high in the eHealth sector than in other domains,
perceived by P9. According to P8, the gaps in com-
munication with stakeholders are equally common in
other domains.
4.3 Challenges Related to Usability and
User Experience
Three participants (P4, P5, and P7) discussed chal-
lenges of usability and user experience in detail. P3
and P6 also briefly touched upon these topics. Ac-
cording to P4 and P5, IT professionals aim to make
applications easy to use but face some major chal-
lenges in the eHealth sector, especially for elder or
disabled users: “have to consider the old people as
well (as) disabled people... so I think the user experi-
ence matters a lot” as both groups may be affected by
poor eyesight, hearing problems, and other conditions
requiring special support for using software systems.
P5 went as far as to say that lacking usability de-
fies the whole purpose of applications in this domain.
According to P7, the language barrier is an additional
usability and user experience challenge, especially for
newcomers to Sweden. Regarding usage problems P3
said, if IT professionals have less or missing infor-
mation about usage perspectives then it would also
decrease the usability of the software or system.
According to P4, P5, and P7, user interface de-
sign and other usability aspects need to be empha-
sized already early in the development process. P4
mentioned, these challenges will affect the develop-
ment process during prospective design. P5 said,
IT professionals need to research how they can im-
prove usability and user experience, and seek con-
stant feedback from customers, consumers, and user
experience (UX) teams. However, P5 also highlighted
that time constraints in development might restrict the
effort that could be spent on usability engineering.
Additionally, P5 elaborated on another challenge for
healthcare system providers, i.e. the need to guide and
train patients, doctors, and other professionals on how
to use novel applications. This would make systems
easier to use and affect their acceptance positively but
would require extra efforts from system providers.
P7 added, IT professionals need to involve end-
users in the design phase from the beginning and work
closely with them: “user involvement is very impor-
tant, extremely, especially in the first phase of the de-
sign”. According to P5, IT professionals can keep
stakeholders on-board during the development lifecy-
cle. IT professionals need to collaborate with stake-
holders to better understand problems as it is impor-
tant to get feedback from customers on a regular basis.
P5 thinks, if IT professionals can provide better user
experience then they would have to put less effort into
training users.
P5 said, nowadays every company has specialized
UX designers and with their help developers can think
more about users and develop user-oriented solutions.
For P4, there should be clear design guidelines re-
garding making the application more useful and IT
professionals need to follow those guidelines to en-
hance user experience. P6 added, thinking about dif-
ferent user perspectives, user experience, and usage
scenarios, IT professionals can produce a product that
fulfills user’s needs. Also IT professionals need to in-
volve special user interface (UI) designers to enhance
usability and user experience. P5 believes that beta
testing can also play an important role to understand
and mitigate flaws in user experience.
P4 perceived challenges related to usability high
in the eHealth sector as compared to other domains
but P7 has no experience of usability challenges in
other domains. P5 perceives user experience chal-
lenges high in the eHealth sector as compared to the
banking sector but has no experience with other do-
mains. P5 perceived the same severity of user training
challenges in the eHealth sector as compared to soft-
ware for the construction, banking, or other domains.
4.4 Challenges Related to Rules and
Regulations
Four participants (P1, P2, P8, and P9) discussed chal-
lenges related to rules and regulations. P8 states, pro-
viding digital healthcare solutions has become more
challenging due to a variety of requirements caused
by administrative or legal constraints: “A lot of orga-
nizations (have) a lot of requirements regarding how
to develop solutions”. The digital healthcare system
involves many different stakeholders which makes
managing systems challenging.
This is especially true for Sweden’s decentralized
administration of the healthcare sector, which to a
large degree, is in the hands of the 21 counties. Ac-
cording to P9, this leads to integration issues: “...have
a lot of systems that are interconnected and... differ-
ent people would be responsible for different things...
the challenge will be to make sure that we have as
many real integrations as we can within reasonable
resources”. P1 added that the development of soft-
ware solutions is often delayed because the systems to
be developed have to be adapted to the regulations in
different counties. In the same way, P9 said that im-
plementing the technical means to ensure interoper-
ability between different systems is not the main chal-
lenge but the large number of stakeholders operating
the systems that adds to the complexity of designing
a system. IT professionals need to plan how com-
plex rules will affect the integration of different sys-
tems and the exchange of data between them. These
challenges are not difficult to tackle, but they demand
extra time and resources, P9 stated “it takes time and
money to make the data available in the right format”.
P1 additionally highlighted that having complex
regulations and administrative decisions in each in-
dividual county multiply the effort required to adapt
to changes in the regulations. This is not only true
for existing companies in the healthcare sector but in
particular for new and small companies trying to en-
ter the healthcare domain in Sweden and improving it
with new innovations. They have to either face the is-
sue of having to comply with a large set of regulations
or limit their product to counties with similar regula-
tions which may not be feasible. P1 summarised:: “It
makes Sweden unattractive... because the market will
be so limited...”.
The lack of technical knowledge or consideration
of technical stakeholders during political decision-
making in healthcare was perceived as another chal-
lenge. P1 referred to the example of one county
that decided to force all healthcare providers to use
one specific EHR system, effectively putting them
into a vendor lock-in and shutting out other solution
providers from this market. The decision was moti-
vated by the believe that this would increase the data
security. However, according to P1, this would have
been solved in a more sustainable and less market-
restricting way instead by an administrative decision
on technical standards regarding secure storage and
processing of EHR.
With their experience with working in agile set-
tings, P1 and P8 discussed how issues are raised if
stakeholders or organizations are following different
software development practices. P8 said, the soft-
ware development industry is working in a modern
agile way, but the government organizations that for-
mulate and govern the regulations lack agility, mak-
ing it difficult to cooperate and work effectively:
“They’re not that agile, so it’s hard for them to take
on changes. Two systems have different development
life-cycles...”.
According to the P2, due to different rules and reg-
ulations, developers also lack knowledge about laws.
Always there remains a gap between knowledge about
different laws applying to different types of users:
“Different laws are applicable to different cases... the
same information, but different laws”. Sometimes
laws are too rigid, perhaps unintentionally, preventing
innovation but IT professionals need to comply with
laws otherwise they will face legal issues.
According to P1, to overcome these challenges, IT
professionals need to understand the market to know
the boundaries that have been set by politicians for
the healthcare system. Hence rules and regulations
will become very clear. P8 added some regulations
are outdated and do not reflect the way new technol-
ogy is applied in healthcare and stressed that more
agility among those deciding on regulations would
be desirable. P2 expressed the opinion that in or-
der to overcome challenges regarding lack of knowl-
edge about laws, some regulations need to be relaxed
by the authorities. He added that software compa-
nies need to educate teams about rules and regula-
tions, follow regulations especially GDPR. In order to
overcome the interoperability challenges, P9 recom-
mended close collaboration with the different stake-
holders in the Swedish healthcare system. Further-
more, P1 proposed to intensify the efforts in estab-
lishing interoperability standards.
According to P1 and P8, following rules and regu-
lations is more challenging in the eHealth sector than
in finance and other domains. For P2, challenges re-
garding the lack of knowledge about laws are high in
the eHealth sector as compared to the telecommuni-
cation domain. P8 mentioned, due to different stake-
holders and systems, challenges of interoperability
are high in the eHealth sector as compared to finance
and other domains. P9 said that the involvement of
and dealing with different stakeholders in the eHealth
sector is more challenging than in other domains.
4.5 Challenges in Problem Domain
Analysis
Two participants (P3 and P6) discussed challenges in
problem domain analysis. Lack of documentation re-
lated to the problem domain and code pose further
challenges during the development phase. P3 reported
an example in which an existing system they were
asked to maintain was extremely difficult to compre-
hend and hard to be run due to lacking documenta-
tion. P6 added, IT professionals need better insight
into the area of expertise or application to understand
and solve the actual problem. P6 highlighted that de-
velopers start developing an application with less in-
formation about the problem domain and ended up
with a faulty or incomplete system. Getting feed-
back from customers at the end of the development
phase consumes more time to rectify issues. More-
over, both participants stressed the importance of an
elaborative requirements elicitation, P3 stated “if the
requirements aren’t clear for each perspective, then
how can you (IT professionals) develop the entire ap-
plication or software”.
P3 discussed developer perspective and their lim-
ited knowledge of the medical domain, a major chal-
lenge related to developer’s perspective during the de-
velopment of the eHealth system. The mobile appli-
cation developer’s perspective focuses more on better
managing healthcare application platforms. IT pro-
fessionals have difficulty learning medical ideas and
their understanding of the medical domain becomes
limited. As P3 said, things are getting better day by
day, and over time, IT professionals became aware of
the flow of the project. But we (authors) believe that
it has steep learning curve that uses critical time that
could be used to develop or test software or systems.
According to P3, collaboration between stake-
holders and stakeholders on-board can help to bet-
ter learn and understand the domain of the problem:
“to overcome this challenge. . . , on-board stakehold-
ers needed...”. P6 added that once the requirements
are elicited, instead of working directly on a project,
IT professionals need to do brainstorming and build
a prototype. Moreover, instead of getting feedback at
the end do it early to avoid time loss.
The eHealth sector lacks documentation related
to problem domains more than finance and other do-
mains. P6 added that the challenge is almost the
same, but IT professionals need to be more careful
in eHealth as they are dealing with important real-life
situations.
5 DISCUSSION
5.1 Discussion on Integrity, Privacy,
Protection and Security
In eHealth, data is being used to provide useful in-
formation not only to care providers but also to care
receivers (Frennert and Baudin, 2019). Challenges re-
garding incorrect or incomplete data were previously
reported when observing the use of the software by
tele-nurses (Holmstrom, 2007). Our findings confirm
that this issue is considered a general challenge by
IT experts, too. Based on the replies of our partic-
ipants we assume that such issues are only partially
due to the complexity of the domain but are rather
caused to a large degree by incomplete requirements
elicitation, testing, and lack of knowledge about laws
related to data integrity. Further research is needed on
how these activities can be improved and proactive
solutions can be taken in eHealth.
Challenges related to data integrity, privacy, and
security were also reported by other researchers while
mentioning the importance of reliable infrastructure
and trust in healthcare, respectively (
¨
Ostlund, 2017;
Jung and Loria, 2010). Additionally, we found that
private companies or organizations have to put extra
efforts to build such confidence. We noticed different
perceptions of potential architectural solutions (cen-
tralised vs. decentralised) to privacy, data protection,
and security which might point at the need to clarify
the properties of different architectures and the qual-
ity attributes they support.
Additionally, several participants stressed the
need to use data encryption for data protection, which
seems surprising as this is a commonly known tech-
nology. Poor encryption are among the security con-
cerns and researchers also recommended the need to
encrypt data in eHealth, especially for transmitting
data over insecure public networks (Al-Issa et al.,
2019; Sahama et al., 2013). It seems worthwhile in-
vestigating to which degree sensitive data is actually
encrypted in the software landscape of the Swedish
healthcare sector.
We also recommend investigating standardized
methods, architectures, and additional security layers
(like HTTP over SSL) that are needed to be imple-
mented during the development phase to solve current
theme challenges. A survey paper also suggests sev-
eral possible solutions related to current theme chal-
lenges (Al-Issa et al., 2019). Furthermore, we sug-
gest exploring privacy by design approaches or any
conceptual framework to analyze privacy and security
threats and develop secure applications in the health-
care domain (Al-Issa et al., 2019).
5.2 Discussion on Software Testing
Our finding on low testing prioritization is in line with
previous research, which reported that testing budgets
are often limited and testing periods are short (Fren-
nert and Baudin, 2019). This was confirmed in partic-
ular by participants responsible for testing. It seems
hence worthwhile, to ensure the quality of eHealth so-
lutions in the future, to investigate possibilities of test
automation. The feedback provided by our intervie-
wees also points to improving the efficiency and accu-
racy of other development activities, such as require-
ments engineering, in order to allow for more time
for testing. Many requirements engineering practices
have been ineffective in real world projects and yet
have been a problem in eHealth (Fricker et al., 2015).
It seems worthwhile to investigate which methods
in particular for requirements engineering are com-
monly used in the domain of interest and how their
efficiency can be increased.
We found that most IT professionals and re-
searchers do not have access to real data due to
privacy issues. We suggest investigating potential
challenges associated with patient data-sharing agree-
ments. What will happen if data owners belong to
different companies or countries that have different or
even conflicting rules regarding data sharing? We rec-
ommend exploring a better way that not only ensures
the privacy and protection of personal data, but also
gives access to patient and critical data to IT profes-
sionals and researchers working in the eHealth sector
as, for example, proposed by Frotoni et al. (Frontoni
et al., 2014).
Our finding shows that a lack of access to testing
instruments makes it challenging to test systems. In
addition to that, a researcher mentioned, the lack of
knowledge about social contexts also affects the test-
ing of eHealth systems (
¨
Ostlund, 2017). We suggest
exploring different solutions for better access to test-
ing instruments like efficient and safe testing of sys-
tems outside the controlled environments and simula-
tion of required instruments, for example, digitizing
new arenas (
¨
Ostlund, 2017). We recommend explor-
ing better ways of test prioritisation while keeping
medical testing instrument availability challenges in
mind. Relevant techniques could be risk-based testing
(RBT) and cost-oriented prioritisation of test cases
(Huang et al., 2012).
Our finding shows that stakeholders’ communica-
tion issues are perceived as one cause of faulty sys-
tems. Considering the example of tele-nurses, soft-
ware programs were not fully up-to-date, inconsis-
tent with current practices, and much information
was missing (Holmstrom, 2007). Such issues can be
caused by unclear functional requirements, higher de-
mands, and unrealistic deadlines raised due to com-
munication gaps found during our findings. Our find-
ing recommended agile approaches to ensure well-
structured teams and processes, better cooperation,
and work efficiency. Customer collaboration depends
on the application under development and organisa-
tional context of development (Robinson and Sharp,
2010). Therefore, we recommend further research,
whether agile practices help collaboration and com-
munication, or consume more resources than benefits
in eHealth.
5.3 Discussion on Usability and User
Experience
We found that challenges on usability and user experi-
ence were also reported by (Svanborg-Sj
¨
ovall, 2014;
Hollmark et al., 2015;
¨
Ostlund, 2017;
¨
Oberg et al.,
2018; Rydenf
¨
alt et al., 2019; Frennert and Baudin,
2019) in their studies. It is difficult to ensure the us-
ability and user experience for the elderly and dis-
abled. In addition, our research highlighted language
barriers and usage perspective challenges that can
lead to difficulties in using eHealth systems or soft-
ware. We suggest that more efforts be made to inves-
tigate the reasons for ignoring input from elder or dis-
abled people. Furthermore, we found that sometimes
usefulness is considered more important than the us-
ability of eHealth, also reported by (Jung and Loria,
2010;
¨
Ostlund, 2017;
¨
Oberg et al., 2018). Therefore,
we recommend exploring testing strategies to eval-
uate the usefulness of eHealth systems or services.
Eliciting design requirements is beyond the usabil-
ity knowledge of most developers, requirements en-
gineers, and users (Juristo et al., 2007). We therefore
recommend further investigation to determine who is
responsible for providing clear design guidelines and
whether this always guarantees the usefulness of the
application.
There is a belief that usability concerns can be
considered in the final stages of the development pro-
cess (after testing), as it should not take time to rework
for this quality attribute (Juristo et al., 2007). But our
research and literature emphasizes the need to ensure
usability during the early stages of the development
process. We recommend inquiring whether IT com-
panies in eHealth focus entirely on user interface de-
sign and leave usability and user experience during
the design phase or if there are any other unexplored
issues.
Furthermore, we suggest investigating how to
keep elderly and disabled users on-board from the
beginning of development and get constant feedback
as multiple challenges are associated with it. In ad-
dition to guidelines (Smeltzer et al., 2017), imple-
mented practices in the IT sector can be explored for
better collaboration. Further research is needed to ex-
plore better methods for usability engineering in the
eHealth sector, as there is a belief that there should be
usability engineering throughout the lifecycle of an
eHealth application (Price et al., 2016).
Sometimes usability testing is confused with beta
testing and the first is believed to be sufficiently cov-
ered if integrated in the latter stage as users are al-
ready involved in beta testing. However, usability
and beta testing are very different as developers and
testers can ask questions on the fly during usability
testing but not so much in beta testing (Decker, 2014).
Moreover, beta testing is used to be performed to-
wards the end of application development while us-
ability should be evaluated continuously throughout
the design phase. That’s why we recommend explor-
ing how beta testing would be helpful in understand-
ing and mitigating flaws in the user experience.
Some research studies have highlighted the chal-
lenges of educating consumers to use healthcare soft-
ware programs (Holmstrom, 2007) and (
¨
Oberg et al.,
2018). Our finding also agreed to this challenge and
discussed the additional efforts that IT professionals
put into training users and considering their usage per-
spectives. We have found that usability is indirectly
proportional to efforts to train consumers, but still,
further investigation is needed to conclude.
5.4 Discussion on Rules and Regulations
We found challenges related to the fragmented and
distributed administration which was also referred to
in previous studies (Wadmann et al., 2009; Hollmark
et al., 2015; Barkman and Weinehall, 2017;
¨
Ostlund,
2017; Frennert and Baudin, 2019). We have found
that fragmented administration makes it difficult for
all counties to develop the same system. We recom-
mend looking for software product lines that can help
IT professionals to understand the general needs of
different counties (Strobl et al., 2010).
We found that there is a lack of technological un-
derstanding in political decision making. Sometimes
complex and rigid laws prevent innovation in the
eHealth domain. A study added that such challenges
could result in time, cost inefficiency, and untested
systems (Hollmark et al., 2015).
Furthermore, we have found that unclear and dif-
ferent regulations in different counties make it diffi-
cult for new companies to develop eHealth solutions.
In general, administrative rules and regulations don’t
reflect technological advancements. Such issues raise
interoperability challenges, loss of market, and cus-
tomer issues. We suggest exploring standardisation
efforts like HL7 and we have to find out what pieces
are missing in current efforts for interoperability in
the Swedish eHealth sector. Furthermore, we suggest
investigating how understanding the market will help
to raise awareness of the limitations that politicians
have set on the healthcare system and how it will in-
crease awareness and acceptance level among people.
Regarding the lack of agility in administration, we
suggest that researchers need to explore how to han-
dle the use of traditional software methods in govern-
ment organizations. Furthermore, we believe that the
transition from the traditional process to agility will
present itself with a variety of challenges. If there
is no other way than transforming, then how can this
transformation be made in order to work effectively
and efficiently with other organizations while keeping
discovered challenges in mind.
Our findings show that knowledge of laws or stan-
dards among developers could be extended. Develop-
ers need to put extra effort and time to acquire such
knowledge. We believe that higher staff turnover will
create more problems, as the participant points out
that the gaming industry is attracting more develop-
ers. Agile practices could help in better communi-
cation and early detection of issues. Continuous in-
volvement of stakeholders would help to get a clear
understanding of rules and regulations. Furthermore,
we suggest investigating techniques that could effi-
ciently solve problems of knowledge about different
laws applicable to different users and regulatory com-
pliance in the eHealth sector.
5.5 Discussion on Problem Domain
Analysis
Our finding shows that if IT professionals don’t have
proper documentation, then it becomes challenging
to understand and analyze the problem domain. This
can lead to problems with implementation and usabil-
ity, especially during the maintenance of a project.
Our findings suggest requirement engineers need to
ensure that developers must have complete informa-
tion regarding the problem domain so that they can
effectively meet customer needs. We recommend
exploring efficient requirement engineering methods
and domain-driven design and development concepts.
Our finding on lack of medical domain knowl-
edge among developers is in line with previous re-
search, which reported that tele-nurses believe that IT
experts lack insight into the problem domain analy-
sis and medical domain knowledge (Hollmark et al.,
2015). We think teaching medical domain knowledge
to every developer has a steep learning curve and it
consumes essential resources that could be used for
other important activities. Considering the case of P1
from our findings, software companies can dedicate
a few key people responsible for having medical do-
main knowledge, and they will share it with IT pro-
fessionals. Therefore, not every IT professional will
need to have this knowledge explicitly.
On-board stakeholders, brainstorming, prototyp-
ing, and close collaboration may be solutions to the
lack of medical domain analysis and knowledge chal-

lenges. Since these are key features of agile practices
that most IT professionals apply, it seems worthwhile
to investigate whether they actually work in the do-
main of interest of this study.
It can be seen, many of the recommendations
found during our study were the most common in ag-
ile practices, but still, the eHealth sector faces vari-
ous challenges. We suggest investigating this issue
further, whether the technology or requirements are
evolving or changing rapidly compared to the recom-
mended solutions, or there is something else that is
still unexplored.
5.6 Threats to Validity
One aspect influencing the external validity of a study
is the number of observed cases (Yin, 1994). Eight
cases are often considered a reasonable minimum
threshold to draw generalizable conclusions in qual-
itative studies (McCracken, 1988). We hence believe
that with the given number of participants (n=9), we
managed to obtain generalizable findings about exist-
ing challenges in the domain of interest. However, a
larger number of cases would be desirable to get a bet-
ter picture of the prevalence of challenges. We deem
the variety among interviewees regarding their level
of experience and area of expertise to reflect the tar-
get population fairly and hence to support the external
validity of the study.
The performed data analysis is heavily based on
human interpretation of collected data. Therefore, it
might be compromised by biases, inconsistencies, and
missed aspects in the interpretation, reducing the reli-
ability of the study. To counteract this threat, contin-
uous mutual reviewing was performed by the authors
to ensure the developed code and themes quality.
All interviews were conducted before the Covid-
19 pandemic seriously affected the Swedish health-
care system. We are aware of potential shifts in the
perceived challenges based on experiences with de-
veloping and operating eHealth systems during the
pandemic. A replication of the study today might
hence lead to slightly different conclusions. We be-
lieve though that the identified potential research di-
rections are relevant in the long run.
6 CONCLUSIONS
It has been noticed that a lot of work has been done
to explore challenges in the Swedish eHealth sector,
but it was not done from the software developers’ per-
spective. The results suggest that further research is
required regarding agile methods, efficient require-
ment engineering, and testing in eHealth as well as
in privacy and usability engineering. There are also
some problems in realizing the vision, but better regu-
lations, user-centric, pro-active, and collaborative ef-
forts are needed to fulfill Sweden’s 2025 vision. Other
domains primarily, the banking sector is working hard
to increase the effectiveness and quality of the ser-
vice to increase customer satisfaction. We think there
is hope, potential, and expectation that soon eHealth
will have the same. Further research is required to
look into how other domains in Sweden or digital
healthcare solution providers in other countries are
dealing with such challenges.
ACKNOWLEDGEMENTS
This work was funded by Region V
¨
armland via the
DigitalWell Arena project (Dnr RV2018-678).
REFERENCES
Al-Issa, Y., Ottom, M. A., and Tamrawi, A. (2019). ehealth
cloud security challenges: A survey. Journal of
Healthcare Engineering, 2019.
Barkman, C. and Weinehall, L. (2017). Policymakers and
mhealth: Roles and expectations, with observations
from Ethiopia, Ghana and Sweden. Global health ac-
tion, 10(sup3):1337356.
BBC (2019). Millions of medical calls exposed online.
https://www.bbc.com/news/technology-47292887.
Accessed: 23.08.2020.
Berg, B. L. (1989). Qualitative Research Methods for the
Social Sciences, volume 1. Pearson Boston, MA.
Bhavnani, S. P., Narula, J., and Sengupta, P. P. (2016). Mo-
bile technology and the digitization of healthcare. Eu-
ropean heart journal, 37(18):1428–1438.
Bjorkman, J. (2019). Healthcare resource guide:
Sweden. https://2016.export.gov/industry/health/
healthcareresourceguide/eg main 116247.asp. Ac-
cessed: 04.07.2020.
Braun, V. and Clarke, V. (2006). Using thematic analysis
in psychology. Qualitative research in psychology,
3(2):77–101.
Charmaz, K. (2014). Constructing Grounded Theory. Sage.
Corbin, J. and Strauss, A. (2014). Basics of Qualitative
Research: Techniques and Procedures for Developing
Grounded Theory. Sage publications, 4th edition.
Decker, R. (2014). Usability vs beta testing (the
what & when). http://www.uxsisters.com/2014/08/
usability-vs-beta-testing. Accessed: 24.11.2020.
Della Mea, V. (2001). What is e-health (2): The death of
telemedicine? Journal of medical Internet research,
3(2):e22.
Frennert, S. and Baudin, K. (2019). The concept of welfare
technology in swedish municipal eldercare. Disability
and Rehabilitation, pages 1–8.
Fricker, S. A., Grau, R., and Zwingli, A. (2015). Require-
ments engineering: best practice. In Requirements En-
gineering for Digital Health, pages 25–46. Springer.
Frontoni, E., Baldi, M., Zingaretti, P., Landro, V., and Mis-
ericordia, P. (2014). Security issues for data sharing
and service interoperability in ehealth systems: the
nu. sa. test bed. In 2014 International Carnahan Con-
ference on Security Technology (ICCST), pages 1–6.
IEEE.
Galin, D. (2005). Software Quality Assurance: From The-
ory to Implementation. Pearson Education India.
Gustafsson, B., Hermeren, G., and Petersson, B. (2017).
Good Research Practice. Stockholm: Veten-
skapsr
˚
adet, Sweden.
Hollmark, M., Skjoldebrand, A. L., Andersson, C., and
Lindblad, R. (2015). Technologyrready to be
launched, but is there a payer? challenges for im-
plementing ehealth in sweden. In PHealth 2015:
Proceedings of the 12th International Conference on
Wearable Micro and Nano Technologies for Personal-
ized Health, Sweden, volume 211, page 57. IOS Press.
Holmstrom, I. (2007). Decision aid software programs
in telenursing: not used as intended? experiences
of swedish telenurses. Nursing and health sciences,
9(1):23–28.
Huang, Y.-C., Peng, K.-L., and Huang, C.-Y. (2012). A
history-based cost-cognizant test case prioritization
technique in regression testing. Journal of Systems
and Software, 85(3):626–637.
Jung, M. L. and Loria, K. (2010). Acceptance of swedish
e-health services. Journal of multidisciplinary health-
care, 3:55–63.
Juristo, N., Moreno, A., and Sanchez-Segura, M.-I. (2007).
Guidelines for eliciting usability functionalities. IEEE
Transactions on Software Engineering, 33(11):744–
758.
MacLure, M. (2013). Classification or wonder? coding as
an analytic practice in qualitative rresearch. Deleuze
and research methodologies, pages 164–183.
Magrabi, F., Habli, I., Sujan, M., Wong, D., Thimbleby, H.,
Baker, M., and Coiera, E. (2019). Why is it so difficult
to govern mobile apps in healthcare? BMJ Health and
Care Informatics.
McCracken, G. (1988). The Long Interview (Qualitative
Research Methods). Sage, 1st edition.
Oates, B. J. (2005). Researching Information Systems and
Computing. Sage.
¨
Oberg, U., Orre, C. J., Isaksson, U., Schimmer, R., Lars-
son, H., and H
¨
ornsten,
˚
A. (2018). Swedish primary
healthcare nurses’ perceptions of using digital ehealth
services in support of patient self-management. Scan-
dinavian journal of caring sciences, 32(2):961–970.
¨
Ostlund, B. (2017). Digitizing health care: Welfare technol-
ogy as a way to meet digital and demographic chal-
lenges in sweden. In 2017 4th International Confer-
ence on Systems and Informatics (ICSAI), pages 78–
83. IEEE.
Price, M., Weber, J., Bellwood, P., Diemert, S., and Habibi,
R. (2016). Evaluation of ehealth system usability and
safety. Handbook of eHealth Evaluation.
PwC (2016). The digital patient is here — but is healthcare
ready?
Robinson, H. and Sharp, H. (2010). Collaboration, commu-
nication and co-ordination in agile software develop-
ment practice. In Collaborative software engineering,
pages 93–108. Springer.
Rydenf
¨
alt, C., Persson, J., Erlingsdottir, G., and Johansson,
G. (2019). ehealth services in the near and distant fu-
ture in swedish home care nursing. CIN: Computers,
Informatics, Nursing, 37(7):366–372.
Sahama, T., Simpson, L., and Lane, B. (2013). Security
and privacy in ehealth: Is it possible? In 2013 IEEE
15th International Conference on e-Health Network-
ing, Applications and Services (Healthcom 2013),
pages 249–253. IEEE.
Smeltzer, S., Mariani, B., and Meakim, C. (2017). Com-
municating with people with disabilities. http:
//www.nln.org/professional-development-programs/
teaching-resources/ace-d/additional-resources/
communicating-with-people-with-disabilities. Ac-
cessed: 24.11.2020.
Strobl, S., Bernhart, M., and Grechenig, T. (2010). An ex-
perience report on the incremental adoption and evo-
lution of an spl in ehealth. In Proceedings of the 2010
ICSE Workshop on Product Line Approaches in Soft-
ware Engineering, pages 16–23.
Svanborg-Sj
¨
ovall, K. (2014). Swedish healthcare is the
best in the world, but there are still lessons to learn.
http://www.theguardian.com/public-leaders-network/
2014/jan/03/sweden-healthcare-coordinate-oecd.
Accessed: 06.07.2020.
Ventola, C. L. (2014). Mobile devices and apps for health
care professionals: Uses and benefits. Pharmacy and
Therapeutics, 39(5):356.
Wadmann, S., Strandberg-Larsen, M., and Vrangbæk, K.
(2009). Coordination between primary and secondary
healthcare in denmark and sweden. International
journal of integrated care, 9.
Walsh, M. (2003). Teaching qualitative analysis using QSR
NVivo. The Qualitative Report, 8(2):251–256.
Wiklund Axelsson, S., Nyberg, L., N
¨
aslund, A., and Me-
lander Wikman, A. (2013). The anticipated positive
psychosocial impact of present web-based e-health
services and future mobile health applications: An in-
vestigation among older swedes. International Jour-
nal of Telemedicine and Applications, 2013.
Yin, R. K. (1994). Case Study Research: Design and Meth-
ods. Sage, Thousand Oaks, CA, 1st edition.
