
Physical Burden in Manual Patient Handling:
Quantification of Lower Limb EMG Muscle Activation Patterns of
Healthy Individuals Lifting Different Loads Ergonomically
Anna Brinkmann
a
, Conrad Fifelski-von Böhlen
b
, Sandra Hellmers
c
, Ole Meyer
d
,
Rebecca Diekmann
e
and Andreas Hein
Assistive Systems and Medical Device Technology, Carl von Ossietzky University of Oldenburg,
26129 Oldenburg, Germany
Keywords: Manual Patient Handling, Nursing, Care, Health Monitoring, EMG, Muscle Activity, Biomechanics.
Abstract: Manual patient handling is a challenging part of daily care and leads to high mechanical loads as well as to
the development of degenerative diseases, e.g. lower back pain. To prevent musculoskeletal overload effects,
the use of ergonomic working techniques is essential as well as improving caregivers’ functional ability.
However, most of the studies do not consider these aspects and biomechanical evaluations including dynamic
electromyography (EMG) are rarely analyzed. In this work, we focus on the quantification of lower limb
EMG muscle activation patterns of healthy caregiver students in an experimental setup. The extent of lifting
different loads ergonomically is analyzed and similarities/dissimilarities of dynamic EMG data of three lower
limb muscles are investigated via cross-correlation calculation. One of the main findings of our investigation
is an indication of a more consistent mean activity of the quadriceps and hamstring musculature, as the load
to be lifted increases. Furthermore, we found an intra- as well as an interindividual similarity of EMG muscle
activation patterns regarding time and shape of the signals generated during all of the conducted lifting tasks
with a predominantly high cross-correlation coefficient for the selected muscles of the lower limb.
1 INTRODUCTION
Manual patient handling is one of the most significant
challenges in care and leads to high mechanical loads
as well as to the development of degenerative dis-
eases, e.g. lower back pain (Hwang et al., 2019; Choi
and Brings, 2016; Jäger et al., 2013). In particular,
lift, hold and handle especially overweight and obese
patients manually is physically demanding and leads
to a compressive strength of the lumbar spine of up to
9 kN (Choi and Brings, 2016; Jäger et al., 2013).
To prevent musculoskeletal overload effects sig-
nificantly, the correct use of technical devices as well
as ergonomic caregiving strategies like supervised er-
gonomic exercise training programs are essential
(Hwang et al., 2019; Choi and Brings, 2016; Weißert-
a
https://orcid.org/0000-0001-5228-4947
b
https://orcid.org/0000-0002-6118-2755
c
https://orcid.org/0000-0002-1686-6752
d
https://orcid.org/0000-0002-9964-5591
e
https://orcid.org/0000-0001-9793-3832
Horn et al., 2014; Jäger et al., 2013; Michaelis and
Hermann, 2010).
A functional approach to ergonomic working
strategies and the improvement of caregivers’ power
as well as functional ability is squat training (Kusma
et al., 2015; Jäger et al., 2013; Baum et al., 2012) as
the squat is biomechanically as well as neuromuscu-
lar similar to many activities of daily living, e.g.
standing up from a chair, demanding the musculo-
skeletal system of the human body more than 50 times
per day (Wang et al., 2019). As squatting positions
are also part of ergonomic manual caregiving rou-
tines, e.g. standing a patient up for transfer, the squat
is frequently used in exercise programs of strength
and conditioning as well as in physical therapy (Ya-
vuz and Erdag, 2017). In this case, lumbosacral loads
can be compensated by strengthening the lower limb
Brinkmann, A., Böhlen, C., Hellmers, S., Meyer, O., Diekmann, R. and Hein, A.
Physical Burden in Manual Patient Handling: Quantification of Lower Limb EMG Muscle Activation Patterns of Healthy Individuals Lifting Different Loads Ergonomically.
DOI: 10.5220/0010247804510458
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 451-458
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
451

and back muscles. Thus, effective load transfer from
the lumbar spine to the pelvis is achieved and shear-
ing of the sacroiliac joints through compression is
prevented (Vleeming and Stoeckart, 2007; Richard-
son et al., 2002).
Common faults in squatting exercises of daily liv-
ing as well as in the context of professional caregiving
are faster rising hips than shoulders and thus resulting
in an increasing flexion of the trunk (Hellmers et al.,
2021; Yavuz and Erdag, 2017). In this case, the dis-
tance between hips and shoulders is diminished in
vertical direction when rising upright from squatting
and the lumbar load increases (Hellmers et al., 2021;
Yavuz and Erdag, 2017). The aim of squatting exer-
cises is to train quadriceps musculature around the
knee and hip joints, thereby strengthening the lower
back (Yavuz and Erdag, 2017). By using the squat as
an ergonomic working strategy for lifting patients,
quadriceps muscles are activated, resulting in a more
consistent mean activation of the back extensor mus-
cles (Brinkmann et al., 2020a; Brinkmann et al.,
2020b).
In recent literature, various scientific articles on
analyzing caregiving activities exist. These deal with
both the identification of psychological as well as
physical stress of healthcare workers and the
enhancement of existing strategies for preventing job-
related back disorders (Cheung et al., 2020; Vinstrup
et al., 2020; Hwang et al., 2019; Choi and Brings,
2016; Höhmann et al., 2016; Zhao et al., 2016; Kusma
et al., 2015; Weißert-Horn et al., 2014; Jäger et al.,
2013; Baum et al., 2012; Aiken et al., 2012; Michaelis
and Hermann, 2010). However, most of the studies do
not consider functional aspects in this context, such
as physical functionality of the caregivers. In
addition, the effects of applying ergonomic working
techniques and its biomechanical evaluation, in-
cluding dynamic electromyography (EMG) for
quantifying muscle activation patterns objectively,
are rarely analyzed (Cheung et al., 2020; Vinstrup et
al., 2020; Hwang et al., 2019).
In this work, we focus on the quantification of
lower limb muscle activity of healthy caregiver
students in an experimental setup. The extent of
lifting different loads ergonomically is analyzed and
similarities/dissimilarities of dynamic EMG data of
three lower limb muscles are investigated via cross-
correlation. We hypothesize a similar EMG activation
for all three conditions while mean muscle activity
increases with lifting heavier weights. The aim is the
assessment of potential amplitude independent
changes of EMG muscle activation patterns as a
function of different ergonomic lifting conditions.
2 MATERIALS & METHODS
2.1 Study Design
In the case study (ethical vote: Drs.EK/2019/004),
five healthy caregiver students (n = 5, 3 female and 2
male students aged between 21 to 45) conduct three
different dynamic lifting tasks:
(1) lifting the own body weight by rising from a
chair to an upright position (Figure 1a, (1)),
(2) lifting a patient simulator (13 kg) from the edge
of a motorized care bed to a standing position
(Figure 1a, (2)),
(3) lifting a patient-imitating subject (patient)
(female, 28 years, 63 kg) upright from the edge
of a motorized care bed (Figure 1a, (3)).
To avoid overloading the caregivers while lifting, a
physiotherapist supervises the tasks.
In the first task (Figure 1a, (1)), the caregivers’
initial position is a vertical trunk with crossed arms.
The feet are placed flat on the floor in shoulder width
and the knee angle is > 90° to avoid extreme joint load
(Slater and Hart, 2017). While rising to fully standing
upright, stability is maintained through muscle
activation. In this case, the components balance,
coordination and lower limb strength as well as power
are covered, which are important in view of analyzing
caregivers’ physical function quantitatively (Hardy et
al., 2010). All in all, each caregiver student repeats
the task five times. The second as well as the third
lifting task (Figure 1a, (2) and (3)) are conducted in
accordance to the Kinaesthetics (Hatch, 2003) care
conception. Therefore, the lifting is executed in
different stages and is foresighted ergonomic planned
with a consistent use of aids. The care bed is adjusted
to an appropriate working height, so that the patient’s
as well as the patient simulator’s feet are flat on the
floor while sitting at the bed’s edge. The caregiver
stands parallel to the patient and slightly squats
bending down to the patient for lifting up. The knee
angle is > 90°, as extreme joint load is thus prevented
(Slater and Hart, 2017). In the second task, the
caregiver puts his arms around the simulated patient
and lifts while rising from squatting (Figure 1a, (2)).
Then, both are in an upright position. Compared to
the second lifting task, there is an active interaction
between patient and caregiver in the third lifting task.
In this case the patient puts his arms around the
caregiver (Figure 1a, (3)), so that the functionality of
the patient can be used for cooperation while lifting.
Then, the caregiver also puts his arms around the
patient and shifts the own body weight while
remaining a straight back to finally lift up.
HEALTHINF 2021 - 14th International Conference on Health Informatics
452
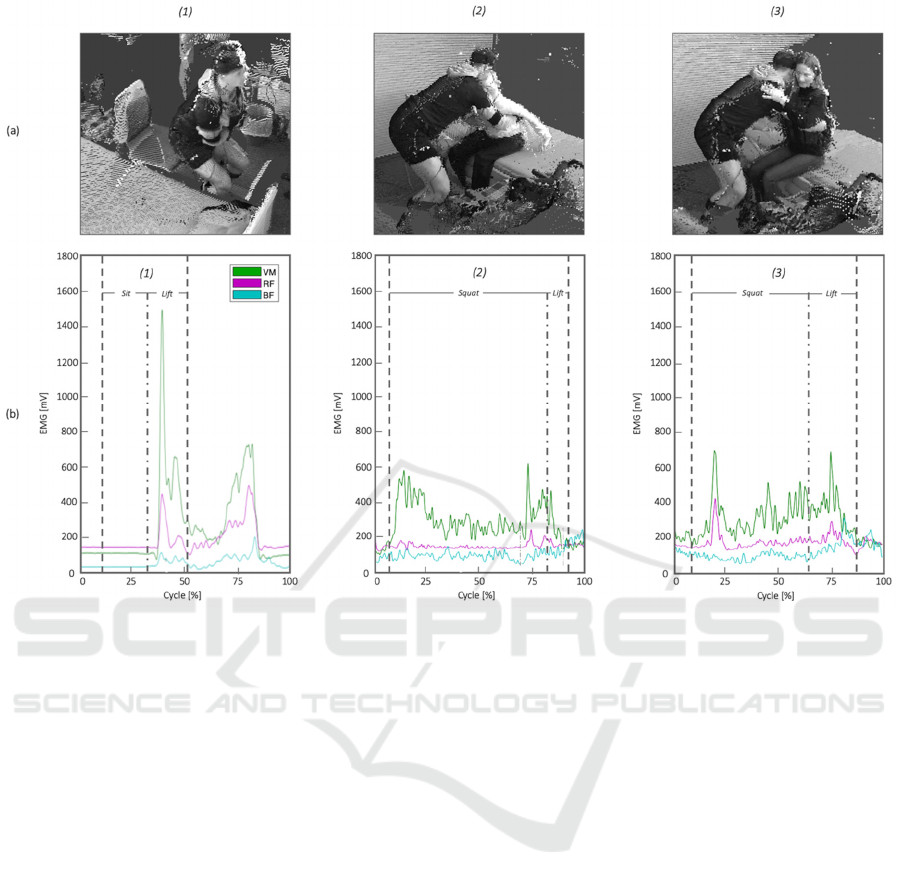
Figure 1: Kinematic (a) and EMG data (b) of three different ergonomic lifting tasks of one exemplary study participant.
Kinematic data is shown in three-dimensional point clouds of the respective lifting task. The time courses for muscle activity
data of three muscles of the lower limb (vastus medialis (VM), rectus femoris (RF) and biceps femoris (BF)) are shown as a
function of the respective lifting task cycle for squatting and lifting for task (1) – (3).
2.2 Biomechanical Data Collection
The procedure for biomechanical data collection is
based on our existing Healthcare Prevention System
(Brinkmann et al., 2020a; Brinkmann et al., 2020b).
Thus, the kinematics of the moving body and its seg-
ments, the kinetics (external ground reaction forces)
and muscle activities of the caregivers’ lower limb are
recorded in order to quantify, assess and evaluate the
executed processes biomechanically.
By direct measurement techniques, a 3D multi-
depth image camera system (Fifelski et al., 2018)
record the data required for motion analysis and a
force plate is used for the measurement of occurring
external ground reaction forces while transferring the
patient. Non-invasive surface EMG records electrical
action potentials associated with muscle contraction
and is the main focus in this work. EMG is used in
order to gain information on the activation behavior
of the following selected muscle groups of the
caregivers’ thigh in task (1) – (3): vastus medialis
(VM), rectus femoris (RF) and biceps femoris (BF).
These muscles are part of the knee extensors as well
as the hip extensors and are thus primarily active
during the conducted dynamic squat exercises. The
electrodes are placed in accordance with SENIAM
guidelines (Hermens et al., 1999). For the acquisition
process, Dasy-Lab 4.010 software as well as an EMG
device from Biovision (Biovision Inputbox) and
bipolar surface electrodes (Ø 14 mm; 10 mm inter-
electrode distance) are used (GE Medical/Hellige).
By local amplifiers, an amplification of the signal
with 2500 Hz is done.
2.3 Data Analysis
In a first step, recorded dynamic EMG data is recti-
fied and then smoothed via Root Mean Square (RMS)
(Figure 2). Then, the data recorded while lifting the
own body weight is cut according to kinematic and
kinetic data representing the basis for analyzing the
different lifting tasks. In task (1), a lifting cycle starts
with sitting and ends with fully standing (Figure 1b,
(1) and Figure 2).
Physical Burden in Manual Patient Handling: Quantification of Lower Limb EMG Muscle Activation Patterns of Healthy Individuals Lifting
Different Loads Ergonomically
453
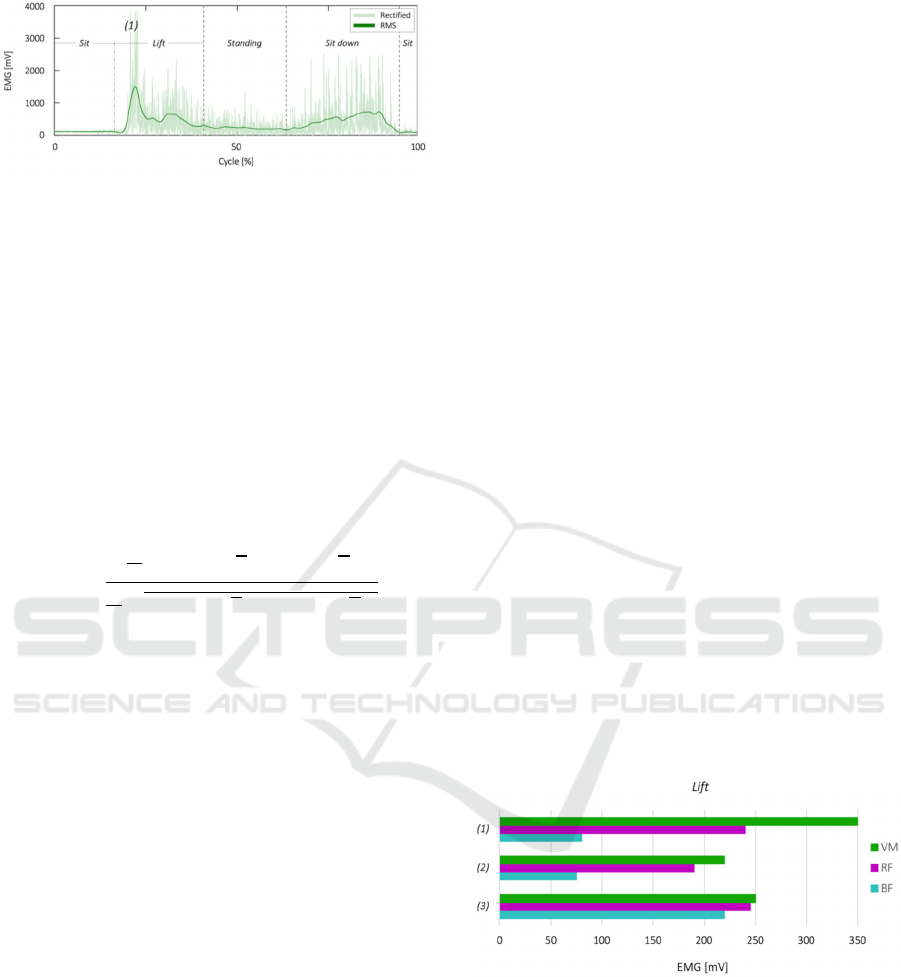
Figure 2: Rectified and RMS smoothed EMG data of VM
activity in task (1) for one exemplary study participant.
Due to the fact, that every cycle reveals a slightly dif-
ferent duration for each participant as well as between
all participants, time normalization is applied using
linear interpolation function. Thus, a mean lifting
signal is calculated separately for each participant and
muscle. Then, an intraindividual as well as an in-
terindividual normalized cross-correlation analysis is
done by calculating cross-correlation coefficient (R-
value) at zero time lag to test dynamic EMG data for
similarities/dissimilarities (Geiger et al., 2019; Nel-
son-Wong et al., 2009; Wren et al, 2006) for each
muscle and each lifting task as follows:
𝑅
𝜏
1
𝑁
∑
𝑥
𝑥𝑦
∙
𝑦
1
𝑁
∑
𝑥
𝑥
∑
𝑦
𝑦
(1)
with 𝑥
and 𝑦
as the two signals to be compared. 𝜏 is
the discrete temporal time shift, 𝑁 is the number of
data points in the respective signal and 𝑓
is the
original sample frequency (Nelson-Wong et al.,
2009).
Via cross-correlation the comparison of two signals
regarding timing and shape is possible, while
amplitude is not considered. Therefore, the signals
mean power is also reflected by using RMS, while its
mean value qualifies gross innervation input for
respective muscles. This step is then followed by
comparing mean EMG activity for each study
participant when lifting their own body weight in task
(1). In this case, we analyse the data due to similar
mean muscle activation patterns while lifting with an
interindividual point of view. The participants, who
show plausible mean muscle activation patterns in
task (1) while rising from a seated position to an
upright position and thereby lifting the own body
weight (Wang et al., 2019; Roldán-Jiménez et al.,
2015; Cuesta-Vargas and Gonzáles-Sanchez, 2013;
Roebroeck et al., 1994) are therefore constituted to
one functional group and considered for the
evaluation via cross-correlation calculation.
3 RESULTS
For concentric knee extension when lifting (Figure
1a), VM and RF contract at the same time while
hamstring muscle activation (BF) sustains the hip
(Figure 1b). All in all, three out of five study
participants show plausible mean muscle activation
patterns while rising from a seated position to an
upright position and thereby lifting the own body
weight in task (1) (Figure 1a, (1)). This means, that
the gross innervation input of the analyzed muscles is
highest for VM, followed by RF and BF (Wang et al.,
2019; Roldán-Jiménez et al., 2015; Cuesta-Vargas
and Gonzáles-Sanchez, 2013; Roebroeck et al.,
1994). Accordingly, these participants are constituted
to one functional group and therefore considered for
the evaluation (Figure 3). The other group of partici-
pants show different mean activation patterns with a
predominantly high activation level of RF and are not
considered for further analysis in this work.
For the functional group of study participants,
mean muscle activities of VM, RF and BF while lift-
ing the own body weight in task (1) (Figure 1a, (1))
are: VM = 350 mV, RF = 240 mV and BF = 80 mV
(Figure 3, (1)).
While lifting the patient simulator in task (2) (Fig-
ure 1a, (2)), mean muscle activities of VM, RF and
BF are: VM = 220 mV, RF = 190 mV and BF = 75
mV (Figure 3, (2)).
In task (3), while lifting the patient (Figure 1a,
(3)), mean muscle activities of VM, RF and BF are:
VM = 250 mV, RF = 245 mV and BF = 220 mV (Fig-
ure 3, (3)).
Figure 3: Mean muscle activity data of VM, RF and BF for
task (1) – (3).
Comparing the dynamic mean muscle activity data of
the conducted lifting tasks regarding the functional
group of study participants, similar mean muscle
activation patterns are present (Figure 3). Due to the
gross innervation input of the analyzed muscles while
lifting different loads ergonomically, the highest
value is found for VM, followed by RF and BF
(Figure 3). Comparing the tasks (1), (2) and (3), the
highest mean muscle activity values for VM and RF
HEALTHINF 2021 - 14th International Conference on Health Informatics
454
are found for lifting the own body weight from a
seated position (Figure 3, (1)), followed by lifting the
patient (63 kg) (Figure 3, (3)) and lifting the patient
simulator (13 kg) (Figure 3, (2)).
The delta between mean muscle activity of VM
and RF is 110 mV while standing up, 30 mV while
standing the patient simulator up (13 kg) and 15 mV
while standing the patient up (63 kg). Accordingly,
the delta between mean muscle activity of RF and BF
is 160 mV while standing up, 115 mV while standing
the patient simulator up and 25 mV while standing the
patient up. Furthermore, there is an increase of BF’s
mean muscle activity for all of the three lifting tasks
of up to 145 mV while standing the patient up com-
pared to lifting the own body weight as well as lifting
the patient simulator. In detail, comparing task (2)
and (3), the deviation of the delta of RF and BF is
78% while lifting the higher weight (63 kg) in com-
parison to lifting the patient simulator (13 kg) (Figure
3). In this case, the deviation of the delta of VM and
RF is 50 %.
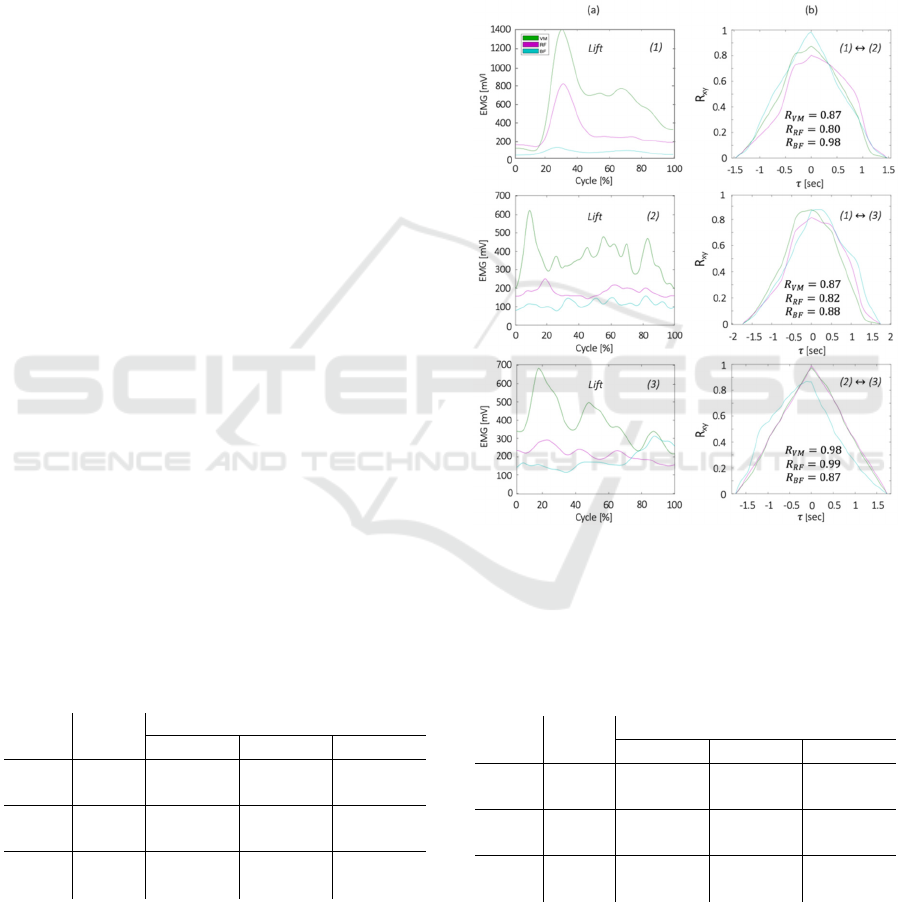
Figure 4 shows the dynamic EMG data of the lift-
ing parts of task (1), (2) and (3) for one exemplary
study participant and the calculation of the R-values
is presented as a function of phase shift with an
intraindividual high similarity of EMG activation for
all three conditions.
All calculated intraindividual R-values for the
functional group of study participants are shown in
Table 1. Here, the R-values show high to very high
correlation for each muscle among the different lift-
ing tasks and for each study participant. However,
lower R-values and greater variability are found for
the BF within the execution of the different lifting
task of one participant (437, Table 1).
Interindividual comparison of the dynamic EMG
data (Table 2) show very high R-values for VM,
averaging > 0.90. In this case, the similarity for the
Table 1: Intraindividual R-values for each muscle and the
respective lifting task correlation.
ID Muscle
R
(1) ↔ (2) (1) ↔ (3) (2) ↔ (3)
424
VM 0.87 0.87 0.98
RF 0.80 0.82 0.99
BF 0.98 0.88 0.87
437
VM 0.89 0.86 0.95
RF 0.89 0.94 0.97
BF 0.68 0.80 0.67
471
VM 0.89 0.90 0.96
RF 0.99 0.99 0.99
BF 0.96 0.91 0.92
VM within the functional group of study participants
is R = 0.96 ± 0.005 for test (1), R = 0.96 ± 0.014 for
test (2) and R = 0.96 ± 0.005 for test (3) (Table 2).
The interindividual cross-correlation result for RF is
R = 0.91 ± 0.026 for test (1), R = 0.89 ± 0.069 for test
(2) and R = 0.97 ± 0.012 for test (3) (Table 2). By
comparing muscle activity data for BF within the
different study participants (Table 2), the R-value is
R = 0.95 ± 0.022 for test (1), R = 0.96 ± 0.025 for test
(2) and R = 0.86 ± 0.043 for test (3).
Figure 4: EMG data (a) and R-values (b) for task (1) – (3)
and for one exemplary study participant. EMG time courses
of VM, RF and BF are shown as a function of the respective
lifting task cycle. R-value calculation is presented as a func-
tion of phase shift.
Table 2: Interindividual R-values for each muscle and the
respective lifting task correlation.
Muscle Test
R
424 ↔ 437 424 ↔ 471 437 ↔ 471
VM
(
1
)
0.95 0.96 0.96
(
2
)
0.94 0.97 0.97
(
3
)
0.96 0.96 0.97
RF
(
1
)
0.93 0.87 0.92
(
2
)
0.83 0.99 0.86
(
3
)
0.96 0.99 0.97
BF
(
1
)
0.93 0.98 0.94
(
2
)
0.99 0.95 0.93
(
3
)
0.92 0.82 0.84
Physical Burden in Manual Patient Handling: Quantification of Lower Limb EMG Muscle Activation Patterns of Healthy Individuals Lifting
Different Loads Ergonomically
455

4 DISCUSSION
We focused on the quantification of lower limb EMG
muscle activation patterns of healthy caregiver
students while lifting different loads ergonomically.
In an experimental setup in the field, the extent of
kinematic, kinetic and muscular activity is investi-
gated while three different dynamic lifting tasks are
conducted (Figure 1).
In each task, the caregivers’ stability is maintained
through muscle activation while distributing the own
body weight evenly before standing up from a seated
position as well as lifting the simulated patient (13
kg)/the patient (63 kg). In accordance with literature
findings (Yavuz and Erdag, 2017; Aspe and Swinton,
2014; Paoli et al., 2009; Boyden et al., 2000; McCaw
and Melrose, 1999), mean muscle activity increases
with lifting higher loads in our experimental case
study. A more consistent mean activity of the quadri-
ceps and hamstring musculature is indicated, as the
load to be lifted gets higher. Thereby, concentric knee
extension and eccentric resistance to knee flexion
activates the quadriceps muscles (Figure 1b). The
hamstrings are quadriceps’ antagonists, as these mus-
cles oppose knee extensor moments (Yavuz and
Erdag, 2017). However, in squatting exercises RF and
BF paradoxically co-contract. With increasing load,
BF muscle activity increases as well (Figure 1b, (3)).
The effect of increasing mean muscle activity of BF
in our case study could be due to co-contraction for
stabilizing the knee as well as the pelvis while turning
from an eccentric to a concentric movement. In future
research, muscle fatigue could be another relevant
topic. Literature findings indicate an increasing
muscle fatigue of the knee extensors with increasing
task repetitions (Roldán-Jiménez et al., 2015). For
this purpose, the repetitions of task (1) should be in-
creased in future studies.
For the quantification of the EMG muscle
activation patterns generated in our experimental case
study, we use cross-correlation calculation for com-
paring the data from different lifting scenarios and
different individuals objectively. In a first step, the
muscle activation patterns of lifting the own body
weight in task (1) are intraindividual analyzed for the
functional group of study participants. Here, cross-
correlation results (R-values) show similar activation
for the five lifting cycles with slightly differences in
form as well as in duration. By using linear in-
terpolation function for intraindividual normalized
cross-correlation analysis at zero time lag, the R-
values indicate a high similarity between different
lifting patterns (Table 1) and a significant similarity
when comparing task (2) and (3) with somewhat
moderate correlation for the BF of one participant
(Table 1, 437, R = 0.72 0.060). This may reflect a
greater variability regarding muscle activation within
different lifting scenarios as well as a sensitivity of
this muscle due to its biarticular function (Wren et al.,
2006). In this case, a greater variability could be also
due to a knee angle < 90°, which has to be verified in
future studies. Furthermore, muscle’s length and
overlying fat mass could be the reason for an in-
creasing sensitivity to EMG electrode placement
(Wren et al., 2006). Although the BF as well as the
RF in some cases exhibit a greater variability than the
VM (Table 1), the R-values are still high. Comparing
the dynamic EMG data of the functional group of
study participants interindividual (Table 2), very high
R-values for VM, averaging > 0.90, are found for all
lifting scenarios. In future research, the constitution
of study participants to functional groups needs to be
further investigated. In this case, cross-correlation
analysis could be used to verify inter- as well as intra-
individual similarities/dissimilarities.
It should be noted, that no real patient was
recruited for our case study. Although, the use of the
patient simulator in task (2) prevents unintentional
subliminal cooperation and supportive behavior
throughout the tests, the variety of possible non-co-
operating patient behavior of e.g. anesthetized or
obese patients is not fully covered. This is due to the
low weight of the patient simulator (13 kg). However,
the weight of the patient (63 kg) is within a realistic
range and by using the patient’s functionality in task
(3), cooperative patient behavior is represented. Nev-
ertheless, it still has to be distinguished from lifting a
real patient. Therefore, it can be assumed, that muscle
activity data under realistic circumstances may be
higher than provided in this work.
The main findings of our experimental case study
are an intraindividual as well as an interindividual
similarity of EMG muscle activation patterns regard-
ing time and shape of the signals generated during all
of the three conducted lifting tasks. In this case, the
R-values are predominantly high for the selected mus-
cles of the lower limb, especially for the VM. These
results provide a first insight into the quantification of
EMG muscle activation patterns of healthy caregivers
lifting different loads ergonomically and serve as a
basis for further investigations with a larger study
population. Based on future research, the results may
enhance both supervised ergonomic exercise pro-
grams in the education of caregivers and to allow for
a more targeted use in training interventions from a
functional point of view.
HEALTHINF 2021 - 14th International Conference on Health Informatics
456

ACKNOWLEDGEMENTS
The authors would like to thank the Evangelische Al-
tenpflegeschule e.V. in Oldenburg (Evangelic Nurs-
ing School of Oldenburg) for participating the case
study.
REFERENCES
Aiken, L.H., Sermeus, W., Van den Heede, K., Sloane,
D.M., Busse, R., McKee, M., Bruyneel, L., Rafferty,
A.M., Griffiths, P., Moreno-Casbas, M.T., et al.
(2012). Patient safety, satisfaction, and quality of
hospital care: cross sectional surveys of nurses and
patients in 12 countries in Europe and the United
States. Bmj 2012, 344, doi: 10.1136/bmj.e1717
Aspe, R. R. and Swinton, P.A. (2014). Electromyo-
graphic and kinetic comparison of the back squat and
overhead squat, Journal of Strength and Condition-
ing Research, 28(10), pp. 2827-2836, doi:
10.1519/JSC.0000000000000462
Baum, F., Beck, B.B., Fischer, B., Gllüsing, R.,
Graupner, I. et al. (2012). Prävention von
Rückenbeschwerden; TOPAS_R–Konzept der BGW
für Pflege und Betreuung. Hamburg, Germany:
Berufsgenossenschaft für Gesundheitsdienst und
Wohlfahrtspflege.
Boyden, G., Kingman, J. and Dyson, R. (2000). A
comparison of quadriceps electromyographic
activity with the position of the foot during the
parallel squat, Journal of Strength and Conditioning
Research, 14(4), pp. 379-382, doi: 10.1519/
00124278-200011000-00002
Brinkmann, A., Fifelski, C., Lau, S., Kowalski, C.,
Meyer, O., Diekmann, R., Isken, M., Fudickar, S.
and Hein, A. (2020a). The AAL/Care Laboratory –
A Healthcare Prevention System for Caregivers.
Nanomaterials, 9(1), pp.1-10, doi:
10.1680/jnaen.19.00021
Brinkmann, A., Fifelski, C., Lau, S., Kowalski, C.,
Meyer, O., Diekmann, R. and Hein, A. (2020b).
Quantification of Lower Limb and Spine Muscle
Activity in Manual Patient Handling – A Case Study.
Proceedings of the 18th annual International
Conference on Informatics, Management, and
Technology in Healthcare (ICIMTH 2020), Athens,
Greece, 3-5 July 2020, pp. 249-252. doi:
10.3233/SHTI200541
Cheung, K., Dai, J., Cheung, C.L., Cho, H.K., Chow,
Y.L., Fung, K.Y., Lam, W.S., Li, H.L.C., Ng, S.Y.,
Ngan, M.J. and Szeto, G. (2020). The biomechanical
evaluation of patient transfer tasks by female nursing
students: With and without a transfer belt, Appl.
Ergon., 82. doi: 10.1016/j.apergo.2019.102940
Choi, S.D. and Brings, K. (2016). Work-related
musculoskeletal risks associated with nurses and
nursing assistants handling overweight and obese
patients: a literature review. Work, 53(2), pp. 439-
448, doi: 10.3233/WOR-152222
Cuesta-Vargas, A.I. and González-Sanchez, M. (2013).
Differences in Muscle Activation Patterns during Sit
to Stand Task among Subjects with and without
Intellectual Disability. BioMed Res Int. doi:
10.1155/2013/173148
Fifelski, C., Brinkmann, A., Ortmann, S.M., Isken, M.
and Hein, A. (2018). Multi Depth Camera System for
3D Data Recording for Training and Education of
Nurses. Proceedings of the 2018 International
Conference on Computational Science and
Computational Intelligence (CSCI). Las Vegas,
Nevada, USA, 12-14 December 2018, pp. 679-684,
doi: 10.1109/CSCI46756.2018.00137
Geiger, E.D., Behrendt, F., Schuster-Amft, C. (2019).
EMG Muscle Activation Pattern of Four Lower
Extremity Muscles during Stair Climbing, Motor
Imagery, and Robot-Assisted Stepping: A Cross-
Sectional Study in Healthy Individuals. BioMed
Research International 2019, doi:
10.1155/2019/9351689
Hardy, R., Cooper, R., Shah, I., Harridge, S., Guralnik,
J. and Kuh, D. (2010). Is chair rise performance a
useful measure of leg power? Aging Clin Exp Res,
22(5-6), pp. 412-8, doi: 10.1007/BF03324942
Hatch, M. (2003). Kinaesthetics. In: Health
Development and Human Activity. Urban and
Fischer, Munich, Germany, pp. 34-75.
Hellmers, S., Brinkmann, A., Fifelski- von Böhlen, C.,
Lau, S., Diekmann, R. and Hein, A. (2021).
Assessing Postures and Mechanical Loads during
Patient Transfers. 14
th
International Conference on
Health Informatics (HEALTHINF 2021).
Hermens, H.J., Freriks, B., Merletti, R., Stegeman, D.,
Blok, J. and Rau. G. (1999). European
Recommendations for Surface Electromyography:
Results of the SENIAM Project. Roessingh Research
Development, Enschede, the Netherlands. 8(2), pp.
13-54.
Höhmann, U., Lautenschläger, M. and Schwarz; L.
(2016). Belastungen im Pflegeberuf:
Bedingungsfaktoren, Folgen und Desiderate. In:
Pflege-Report 2016 – Die Pflegenden im Fokus.
Schwinger, A. (eds.). Schattauer, Stuttgart,
Germany, pp. 73-89.
Hwang, J., Kuppam, V.A., Chodraju, S.S.R., Chen, J.
and Kim, J.H. (2019). Commercially available
friction-reducing patient-transfer devices reduce
biomechanical stresses on caregivers’ upper
extremities and low back. Hum. Factors, 61(7), pp.
1125-1140. doi: 10.1177/0018720819827208
Jäger, M., Jordan, C., Theilmeier, A., Wortmann, N.,
Kuhn, S., Nienhaus, A. and Luttmann, A. (2013).
Lumbar-load analysis of manual patient-handling
activities for biomechanical overload prevention
among healthcare workers. Ann Occup Hyg., 57(4),
pp. 528-544. doi: 10.1093/annhyg/mes088
Jordan, C., Theilmeier, A. and Luttmann, A. (2010).
Biomechanische Bewertung der Belastung der
Physical Burden in Manual Patient Handling: Quantification of Lower Limb EMG Muscle Activation Patterns of Healthy Individuals Lifting
Different Loads Ergonomically
457

Lendenwirbelsäule von Pflegepersonen beim
Bewegen von schwergewichtigen Patienten, Shaker,
Düren, Germany, 2010.
Kusma, B., Glaesener, J.-J., Brandenburg, S., Pietsch,
A., Fischer, K, Schmidt, J., Behl-Schön, S. and
Pohrt, U. (2015). Der Pflege das Kreuz stärken.
Germany: Berufsgenossenschaft für
Gesundheitsdienst und Wohlfahrtspflege. Trauma
und Berufskrankheit, 17(4), pp. 244-249.
McCaw, S.T. and Melrose, D.R. (1999). Stance width
and bar load effects on leg muscle activity during the
parallel squat, Medicine and Science in Sports and
Exercise, 31(3), pp. 428-436, doi: 10.1097/
00005768-199903000-00012
Michaelis, M. and Hermann, S. (2010). Evaluation des
Pflegekonzepts rückengerechter Patiententransfer in
der Kranken-und Altenpflege. Langzeit-Follow-Up
zur Ermittlung der Nachhaltigkeit präventiver
Effekte. In: Schriftenreihe der Bundesanstalt für
Arbeitsschutz und Arbeitsmedizin (F2196). Dort-
mund.
Nelson-Wong, E., Howarth, S., Winter, D.A., Callaghan,
J.P. (2009). Application of Autocorrelation and
Cross-Correlation Analyses in Human Movement
and Rehabilitation Research. Journal of Orthopaedic
& Sports Physical therapy, 39/4, pp.287 – 295.
Paoli, A., Marcolin, G. and Petrone, N. (2009). The ef-
fect of stance width on the electromyographical ac-
tivity of eight superficial thigh muscles during back
squat with different bar loads, Journal of Strength
and Conditioning Research, 23(1), pp. 246-250, doi:
10.1519/JSC.0b013e3181876811
Richardson, C.A., Snijders, C.J., Hides, J.A. et al.
(2002). The relationship between the transversus ab-
dominis muscle, sacroiliac joint mechanics and low
back pain. Spine J, 27(4), pp. 399-405, doi:
10.1097/00007632-200202150-00015
Roebroeck, M.E., Doorenbosch, C.A.M., Harlaar, J., Ja-
cobs, R. and Lankhorst, G.J. Biomechanics and mus-
cular activity during sit-to-stand transfer. Clin Bio-
mech 1994, 9, pp. 235-244. doi: 10.1016/0268-
0033(94)90004-3
Roldán-Jiménez, C., Bennett, P. and Cuesta-Vargas, A.I.
(2015). Muscular Activity and Fatigue in Lower-
Limb and Trunk Muscles during Different Sit-To-
Stand Tests. PLOS ONE, 10(10), doi: 10.1371/jour-
nal.pone.0141675
Slater, L.V. and Hart, J.M. (2017). Muscle activation
patterns during different squat techniques. Journal of
strength and conditioning research, 31(3), pp. 667–
676.
Vinstrup, J., Jakobsen, M.D., Madeleine, P. and Ander-
sen, L.L. (2020). Biomechanical Load during Patient
Transfer with Assistive Devices: Cross-sectional
Study, Ergonomics, doi: 10.1080/ 00140139.2020.
1764113
Vleeming, A. and Stoeckart, R. (2007). The role of the
pelvic girdle in coupling the spine and the legs: a
clinical-anatomical perspective on pelvic stability.
In: Movement, Stability & Lumbopelvic Pain, 2nd
ed.; Vleeming, A.; Mooney, V.; Stoeckart, R.; Eds.;
Churchill Livingstone, Edinburgh, UK, pp. 113-137.
Wang, J., Siddicky, S.F., Oliver, T.E., Dohm, M.P.,
Barnes, C.L. and Mannen, E.M. (2019). Biomechan-
ical Changes Following Knee Arthroplasty During
Sit-To-Stand Transfers: Systematic Review, J Ar-
throplasty, 34(10), pp. 2494-2501, doi:
10.1016/j.arth.2019.05.028
Weißert-Horn, M., Meyer, M., Jacobs, M., Stern, H.,
Raske, H.-W. and Landau, K. (2014). „Ergonomisch
richtige‟ Arbeitsweise beim Transfer von
Schwerstpflegebedürftigen. Zeitschrift für
Arbeitswissenschaft, 68(3), pp. 175-184.
Wren, T.A.L., Do, K.P., Rethlefsen, S.A., Healy, B.
(2006). Cross-correlation as a method for comparing
dynamic electromyography signals during gait. Jour-
nal of Biomechanics 2006, 39, pp. 2714 – 2718. doi:
10.1016/j.biomech.2005.09.006
Yavuz, H.U. and Erdag, D. (2017). Kinematic and Elec-
tromyographic Activity Changes during Back Squat
with Submaximal and Maximal Loading. Applied Bi-
onics and Biomechanics, doi: 10.1155/2017/90
84725
Zhao, W., Lun, R., Gordon, C., Fofana, A.B., Espy,
D.D., Reinthal, M.A., Ekelman, B., Goodman, G.,
Niederriter, J. Luo, C. and Luo, X. (2016). A pri-
vacy-aware Kinect-based system for healthcare pro-
fessionals. Proceedings of the 2016 IEEE Interna-
tional Conference on Electro Information Technol-
ogy (EIT). Grand Forks, ND, USA, 19-21 May 2016,
pp. 205-210, doi: 10.1109/EIT.2016.7535241.
HEALTHINF 2021 - 14th International Conference on Health Informatics
458
