
Historical Report Assist Medical Report Generation
Shan Ye
1
, Mei Wang
1
and Yijie Dong
2
1
School of Computer Science and Technology, Donghua University, Songjaing, Shanghai, China
2
Department of Ultrasound, Ruijin Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China
Keywords:
Automatic Report Generation, Historical Report, Encoder-decoder, Co-attention.
Abstract:
How to automatically generate diagnostic reports with accurate content, standardized structure and clear se-
mantics, brings great challenges due to the complexity of medical images and the detailed paragraph descrip-
tions for medical images. The structure and the semantic contents of the historical report are very helpful
for the current report generation. This paper proposes a text report generation method assisted by historical
reports. In the proposed method, both the previous report and the keywords generated from the current images
are modeled by using two encoders respectively. The co-attention mechanism is introduced to jointly learn the
historical reports and the keywords. The decoder based on the co-attention is used to generate a long descrip-
tion of the image. The progress that learns from the historical report and the current report in the training set
helps to generate an accurate report for the new image. Furthermore, the structure in the historical report helps
to generate a more natural text report. We conducted experiments on the practical ultrasound data, which is
provided by a prestigious hospital in China. The experimental results show that the reports generated by the
proposed method are closer to the reports generated by radiologists.
1 INTRODUCTION
Medical imaging plays a crucial role in the diagnos-
tic management and medical treatments, and imag-
ing inspection has become a very common inspec-
tion method. Imaging doctors need to browse numer-
ous images and write diagnostic reports with accurate
content, standardized structure and clear semantics,
which brings great challenges and workloads to doc-
tors’ work. In recent years, artificial intelligence es-
pecially deep learning has been making tremendous
progress in various tasks. Deep learning also pro-
vides more possibilities for the automatic generation
of medical reports. The automatic generation of med-
ical reports includes two steps, namely, understanding
the content of the image and generating natural lan-
guage text describing the content of the image. Such
a generation process is well suited to the encoder-
decoder framework. In the encoder step, features of
the images are extracted by using common conven-
tional neural structures (such as AlexNet, ResNet, In-
ception, etc.), and then in the decoder step, the re-
current neural network generates the corresponding
long text description based on the obtained features
extracted by the encoder. The above process has been
improved by attention mechanism (Mnih et al., 2014)
or knowledge base (Li et al., 2019). However, the
quality of the generated report is still unsatisfactory.
There are two reasons. First, a medical report always
consists of several sections describing medical obser-
vations in detail, which is a very long sequence. Take
the thyroid ultrasound report as an example, about
24349 reports consist of more than 100 words. It
is hard to model very long sequences and generate
accurate, smoothing paragraph description by using
the existing methods. More importantly, most exist-
ing works potentially learn to establish the connection
between images and keywords. However, even for
experienced specialists, the process of medical im-
age interpretation can be error-prone. For example,
in thyroid nodule diagnosis, calcification is an impor-
tant feature. However, it is not easy to distinguish
between micro-echoic focus and micro-calcification.
Due to the limitation of the resolution of the instru-
ment, the cognitive and judgment ability of the diag-
nostician, and many other factors, the micro-echoic
foci within many nodules were misjudged as micro-
calcifications. It is difficult for learning models to
build the correct connections between keywords and
images, which leads to inaccurate reports.
In a real situation, the dynamic change of some
features such as edge, size, calcification, echo in thy-
roid ultrasound can help radiologists to diagnose and
accurate generation of the current report. It means
166
Ye, S., Wang, M. and Dong, Y.
Historical Report Assist Medical Report Generation.
DOI: 10.5220/0010245601660174
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 166-174
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

the historical image report is of great significance to
the generation of the patient’s current image report.
As observed in the department of radiology, if the vi-
sual inspection is not enough to detect, describe, and
classify findings in medical images, radiologists often
open the patient’s most recent previous report, pay
special attention to the description of the abnormal
and suspicious areas. The inherent disease progress
helps them to obtain an accurate diagnosis and de-
scription of the current report. In fact, many diseases
are chronic diseases. The patient has multiple imag-
ing reports. Taking the thyroid nodules as an exam-
ple, based on the statistics of the hospital in the past
10 years, nearly 60% of patients have more than 2 re-
ports.
This paper proposes an automatic medical report
generation method assisted by historical reports. Fig-
ure 1 illustrates the basic idea of the proposed method.
Both the structure and the contents of the previous re-
port are exploited to generate the current report. Our
method adopts the encoder-decoder framework. The
most recent previous report and the keywords gener-
ated from the current images are modeled by using
two encoders respectively. The co-attention mech-
anism is introduced to jointly learn both the back-
ground information implied in the historical reports
and the abnormal information implied in the key-
words. The decoder based on the co-attention is used
to generate a long description of the image. The
progress learns from the historical report and the cur-
rent report in the training set helps to generate a more
accurate report for the new image. On the other hand,
the text structure in the previous report has a great cor-
relation with the current report, so a more natural text
report can be generated with the help of the previous
report in our method.
The main contributions of this work are:
• We propose a new medical report generation
method. The historical report structure and
semantics are both exploited in the proposed
method.
• We introduce a structure with two encoders and
one decoder. The historical report and image in-
formation are modeled by two encoders respec-
tively. The co-attention mechanism is further pro-
vided to joint learn the historical reports and the
keywords.
• We conducted the experiments based on practical
ultrasound texts from the thyroid ultrasound ex-
amination data of a prestigious hospital in China
to test the proposed system. The experimental re-
sults show that the proposed solution can generate
more accurate and smoothing reports.
The rest of the paper is organized as follows. Sec-
Figure 1: The basic idea of the proposed method. Both the
structure and the contents of the previous report can help to
generate the current report.
tion 2 reviews related works. Section 3 introduces the
proposed method. Section 4 presents the experimen-
tal results and Section 5 concludes the paper.
2 RELATED WORK
For medical report generation, one possibility is to
generate the report based on the templates. In these
approaches, tags and labels are learned first, then the
target report is generated based on the predefined tem-
plates. The previous work proposed to segment med-
ical images by using a semi-automatic segmentation
method. Then the support vector machine classifies
the image segments to get tags. Finally, the report is
generated by embedding tags into candidate template
sentences(Kisilev et al., 2015a; Kisilev et al., 2015b).
The above methods were improved by using convolu-
tional neural networks to obtain tags from the medical
images (Kisilev et al., 2016). However, the template-
based report generation method depends heavily on
the image feature extraction, template sentence selec-
tion, and grammar rules. The generated report often
has problems with single sentence structure, low flu-
ency, and incoherent content.
With the development of deep learning, the
encoder-decoder framework is widely used in medi-
cal report generation(Cho et al., 2014). Encoder and
decoder can choose to use various convolutional neu-
ral networks and recurrent neural networks includ-
ing RNN(Zaremba et al., 2014), LSTM(Hochreiter
and Schmidhuber, 1997), GRU(Cho et al., 2014),
BiRNN(Schuster and Paliwal, 1997) units. The
encoder-decoder method was used to generate the de-
scriptions of medical images(Shin et al., 2016), which
exploit NIN architecture(Lin et al., 2013) as encoder
and LSTM/GRU(Hochreiter and Schmidhuber, 1997;
Cho et al., 2014) as decoder. However, the text gener-
ated by the model is the combination of multiple key-
Historical Report Assist Medical Report Generation
167

words, not a coherent diagnostic report. The above
method was improved by using the attention mecha-
nism(Zhang et al., 2017). The attention mechanism
can help the decoder module locate the most rele-
vant encoder module output (context vector) in each
step of the decoding process. A multi-task learn-
ing framework was proposed that jointly performs the
prediction of medical image tags and the generation
of the diagnostic report(Jing et al., 2017). And a hi-
erarchical recurrent neural network was used as the
decoder(Xue et al., 2018). The advantages of tem-
plate generation methods and deep learning gener-
ation methods are combined in subsequent work(Li
et al., 2018).
Attention mechanism (Mnih et al., 2014) is a com-
monly used method to improve the effectiveness of
the deep learning models. The attention mechanism is
exploited to improve the performance of report gener-
ation(Jing et al., 2017; Wang et al., 2018; Xue et al.,
2018). Models that combine technologies such as re-
inforcement learning or knowledge graphs have also
achieved excellent generation effects. The knowledge
graph was incorporated into the report generation(Li
et al., 2019). The visual features of the medical im-
ages were transformed into a structured abnormality
graph by incorporating prior medical knowledge.
Although the above methods have improved the
performance of the model in various ways, the im-
pact of historical information is not considered when
generating the report. For various chronic diseases in
medicine, the historical information of patients has an
important role as a reference in diagnosing the disease
at the current time.
3 THE PROPOSED METHOD
3.1 Framework
The input to the proposed model is a pair of text, in-
cluding the keyword set obtained from the image and
the previous report of the given patient. Each keyword
set consists of multiple keywords. Each keyword de-
scribes the attribute name or the attribute value which
observed from the medical image. The output is
the report corresponding to the given medical image
z = {z
1
, . . . , z
n
}, where n is the report length. Fig-
ure 2 illustrates the overall architecture of our model
which consists of four modules: (a) keyword mod-
ule extracts context-related and potential information
from the keyword set. (b) report module learns the
underlying structure and semantic information from
the historical report. (c) attention module takes the
hidden states of the keyword module and report mod-
ule at all time steps as input to generate the weighted
average context vector. (d) report output module pro-
duces the diagnostic report given the weighted aver-
age context vector.
3.2 Encoder 1: Report Module
The input to report module is historical report t
r
=
{t
r
1
, t
r
2
, ...t
r
p
}, p is the length of the historical report.
First, we embed historical report text input into em-
bedding vectors. Since the historical report has a long
length and carries rich semantic information. A bidi-
rectional recurrent neural network with GRU units
(Cho et al., 2014) is used as the encoder. BiRNN
(Schuster and Paliwal, 1997) connects two hidden
layers of opposite directions to the output. The model
is therefore able to exploit information both from the
past and the future. The complete context information
of the historical report is hoped to be learned in this
module, in which the forward hidden states is com-
puted as follows:
−→
H
r
= [
−→
h
r
1
,
−→
h
r
2
, . . . ,
−→
h
r
p
]. (1)
We also obtained the backward hidden states:
←−
H
r
= [
←−
h
r
1
,
←−
h
r
2
, . . . ,
←−
h
r
p
]. (2)
Then, a fully connected layer is used to concate-
nate the forward and backward hidden states
−→
h
r
i
and
←−
h
r
i
. To obtain the hidden state H
r
i
, then we have:
H
r
= [H
r
1
, H
r
2
, . . . , H
r
p
] (3)
where H
r
i
represents the bidirectional hidden layer
state at i-th time step.
3.3 Encoder 2: Keyword Module
Keyword module also adopts the bidirectional re-
current neural network with GRU units (Cho et al.,
2014). The input to the keyword module is the key-
word set t
k
= {t
k
1
, t
k
2
, ...t
k
l
}, where l is the length of
t
k
. We first use an embedding layer to convert multi-
ple keyword input into the corresponding embedding
vector. The corresponding hidden layer state H
k
gen-
erated by keyword module is:
H
k
= Keyword encoder(embedding(t
k
)) (4)
where H
k
= [H
k
1
, H
k
2
, . . . , H
k
l
], H
k
i
represents the bidi-
rectional hidden layer state at i-th time step in key-
word module.
3.4 Attention Module
By introducing the historical report information, ra-
diologists could concentrate on observing the abnor-
mal areas of the current medical image. The hidden
HEALTHINF 2021 - 14th International Conference on Health Informatics
168
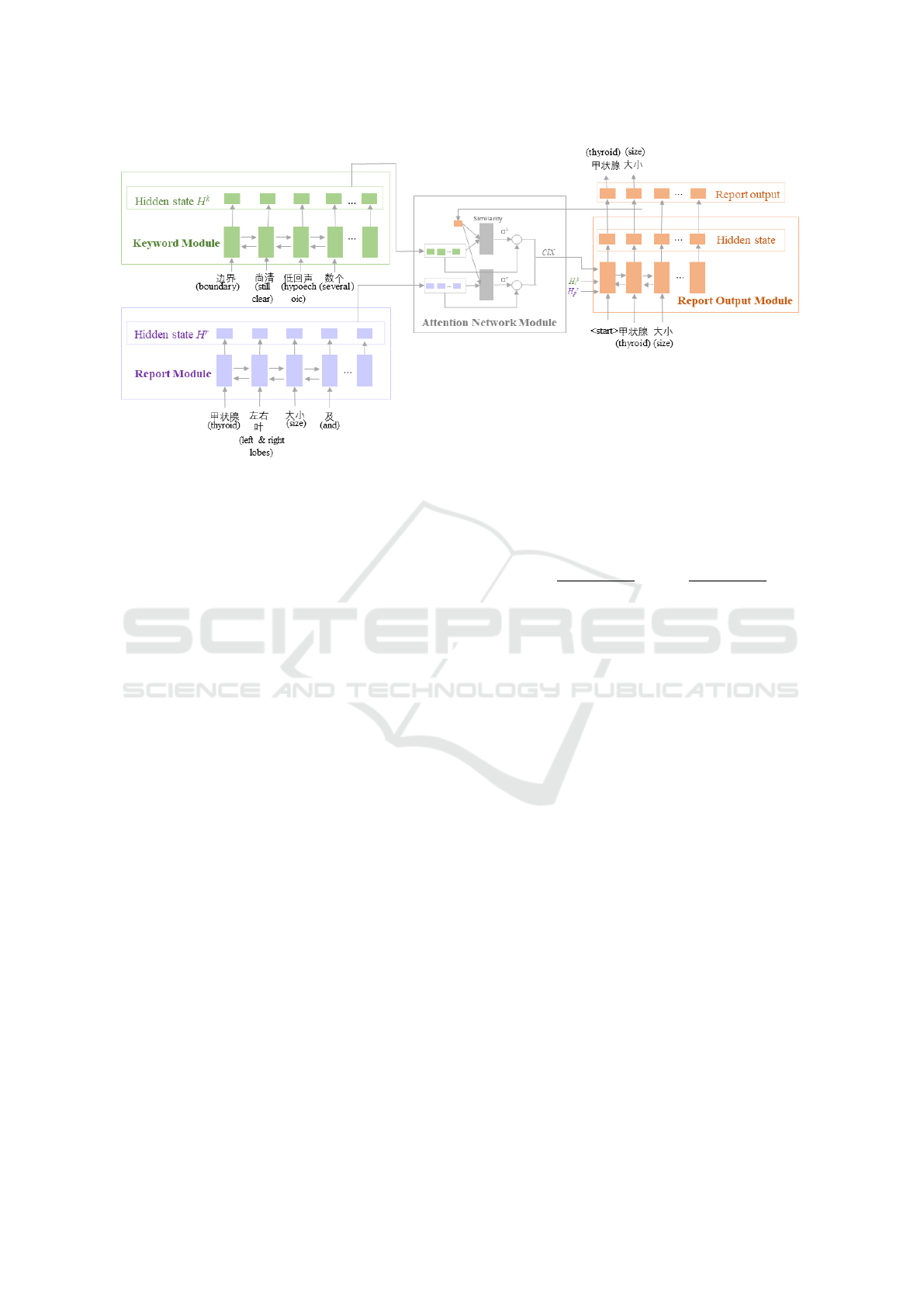
Figure 2: Overall architecture of the proposed model. Encoder 1 is the keyword module which takes multiple keyword set as
input. Encoder 2 is the report module that uses the patient’s historical diagnosis report as input.
state generated from the keyword module mainly pro-
vides abnormal information for the generation report.
The historical reports can provide potential template
information for the generation report. And it is also
expected to provide background information for the
generation report. For example, when there is a ”bor-
der blur” in the keyword set, the ”bounder blur” will
be mentioned in the generation report. However, the
”surface” attribute related to the border that is not
mentioned in the keyword set, can be supplemented
from the sentence ”the boundary is clear, the surface
is smooth” in the historical report.
To capture such dependencies between keyword
set and historical report, we make use of the attention
module as shown in Figure 2. The input to attention
module is the hidden layer states at all time steps of
the keyword module H
k
and the report module H
r
.
s
m−1
is the decoder GRU units (Cho et al., 2014) hid-
den state at time step m-1. At first, H
k
and s
m−1
, H
r
and s
m−1
are used to calculate the alignment scores
e
k
m−1
and e
r
m−1
respectively:
e
k
m−1
= W
k
att
·tanh(W
k
H
k
+W
k,n
s
m−1
+ b
ek
) + b
k
,
e
r
m−1
= W
r
att
·tanh(W
r
H
r
+W
r,n
s
m−1
+ b
er
) + b
r
.
(5)
e
k
m−1
and e
r
m−1
measure how well the keywords
and the historical report around position “j” and the
output at position “m-1” match. For example, the
higher the score e
k
m−1
, s
m−1
and the hidden layer
states of the corresponding time steps in H
k
are more
similar. Then the decoder module will pay attention
to the corresponding keyword observed from the im-
age at the time step m.
Next, we apply the softmax activation function to
the alignment scores to obtain the attention weights.
α
k
=
exp(e
k
m−1
)
∑
exp(e
k
m−1
)
, α
r
=
exp(e
r
m−1
)
∑
exp(e
r
m−1
)
(6)
where W
k
att
, W
k
, W
k,n
, b
ek
, b
k
are parameters of the key-
word part of attention network. W
r
att
, W
t
, W
r,n
, b
er
, b
r
are parameters of the report part of attention network.
Then, we can obtain the context vector as follows:
V
k
=
N
∑
n=1
α
k,n
· H
k
, V
r
=
L
∑
l=1
α
r,n
· H
r
(7)
V
k
, V
r
is the corresponding context vectors of key-
word module and report module. The joint context
vector can be obtained as follows.
ctx
m
= [V
k
m
: V
r
m
] (8)
where [:] indicates vector concatenation.
3.5 Report Output Module
Another recurrent neural network with GRU units
(Cho et al., 2014) is used as the decoder in this mod-
ule. Initialize the hidden layer state of the decoder
with the sum of the last state of the keyword module
H
k
l
and the report module H
r
p
. By passing the con-
text vector ctx and all the previously predicted words
{y
1
, y
2
, ..., y
m−1
} to the report output module, the de-
coder predicts the next word y
m
:
p(y
m
|{y
1
, y
2
, . . . , y
m−1
}, ctx) (9)
At the decoding step m, the input of GRU units
(Cho et al., 2014) is the joint vector of the embedding
Historical Report Assist Medical Report Generation
169

of the previously predicted word y
m−1
and the context
vector ctx
m
:
q
m
= W
f c
· [ctx
m
: y
m−1
] (10)
The hidden state of GRU units (Cho et al., 2014)
at m-th step is calculated:
s
m
= GRU(s
m−1
, q
m
) (11)
Then the probability of the word y
m
distribution at
m-th step can be calculated as follows:
p(y
m
|{y
1
, y
2
, . . . , y
m−1
}, ctx) = so f tmax
y
m
(W
y
s
m
+b
y
)
(12)
where W
f c
, W
y
, b
y
are parameters and |V
y
| are the vo-
cabulary size.
3.6 Training and Inference
The purpose of our model is to minimize the dif-
ference between the generation report and the re-
port written by the radiologists. Given a train-
ing example (t
k
, t
r
, z), where z denotes the report
written by the radiologists, our model performs
encoder-decoder and produces a distribution ˆy
m
=
p(y
m
|{y
1
, y
2
, . . . , y
m−1
}, ctx) over the words. We can
also obtain the ground-truth word distribution y
m
by
examining the presence and absence of words in z.
The training loss of the model is the sparse cross-
entropy losses as follows:
Loss =
∑
Loss
i
=
1
N
∑
i
−
v
∑
m=1
y
im
· log ˆy
im
(13)
where N is the size of the training set. During
the training, the parameters of two encoders, decoder
and attention module will be updated to the direction
of lower loss through the gradient descent algorithm.
The model with updated parameters has a lower loss,
can generate the report which is closer to the report
written by the radiologists.
4 EXPERIMENTS
4.1 Experimental Setup
4.1.1 Data
Our data set generated from a real-world thyroid ul-
trasound set from the reputable hospital in Shanghai,
China, in which there are 38042 patients having thy-
roid ultrasound examinations. There are 21965 pa-
tients having more than one examination report. We
select these patients with more than one report in our
final dataset. There are 70539 ultrasound examina-
tions reports. Also, there are 133 reports whose length
exceeds 200. Since reports with long text and low
proportion of reports will cause too many neurons to
initialize, and most of the neurons cannot train effec-
tively. That will increase the difficulty of the model’s
convergence during the training process. We remove
the report with more than 200 words.
Recall that our training sample is the triple, in-
cluding the most recent previous report t
r
, the key-
word set k
t
and the current report z. So we organize
each patient’s report as a sequence {t
1
, t
2
, . . . , t
m
} ac-
cording to the report time. For the report t
i
, i ≥ 2 in
the sequence, we choose t
i−1
and t
i
as t
r
and z. We
also extract abnormal keyword description of report t
i
to obtain the keyword set t
k
. In this way, we obtain
30597 triple samples in total. We divide the samples
into a training set and a test set. The training set con-
sists of 27,537 samples. There are 3060 samples in
the test set.
4.1.2 Training Configuration
The dimensions of all hidden states in two encoders
and one decoder are set to be 512. The dimensions
in the embedding layer are set to be 256. Models are
trained for 30 epochs with Adam optimizer (Kingma
and Ba, 2014). The learning rate of Adam is 1e-3.
The batch size is set to be 4. All models are imple-
mented in the Tensorflow framework.
4.1.3 Baseline Methods
We compared our method with the baseline methods
the neural machine translation model with attention:
seq2seq attention (Xu et al., 2015) and the related
version of our model: pair2text-show-attention. The
hidden state dimensions and the embedding layer di-
mension of the baseline models are the same as our
model. In the first baseline method, we only use the
keyword set to generate the report. The length of the
input sequence and the output sequence in seq-to-seq
are not fixed. In order to further testify the effective-
ness of the proposed method, we also implement the
related version pair2text show attention. In this ver-
sion, both the historical report and the keyword set
are modeled by using two encoders. While in the at-
tention module, layers for alignment score calculation
share the parameters for the two hidden state inputs.
4.1.4 Evaluation Metrics
We use the following evaluation metrics in the experi-
ments: BLEU (Papineni et al., 2002), ChrF (Popovi
´
c,
HEALTHINF 2021 - 14th International Conference on Health Informatics
170

Table 1: Main results of the models on the generation report tasks. BLUE-N denotes that the BLEU score uses up to N-grams.
Methods BLEU-1 BLEU-2 BLEU-3 BLEU-4 ChrF NIST
seq2seq attention 0.4815 0.4394 0.4154 0.3965 0.6086 2.3744
pair2text show attention 0.7629 0.7239 0.6918 0.6654 0.7892 4.8157
pair2text two attention 0.8084 0.7694 0.7487 0.7305 0.8621 5.1217
2015) and NIST (Doddington, 2002). BLEU is al-
ways used to measure the similarity between gener-
ated sentences and reference sentences in machine
translation. Here we use BLEU measurement to mea-
sure the similarity between the report generated by the
model and the report written by radiologists. N-gram
overlaps are calculated in BLEU-N measurement. It
has been demonstrated that BLEU is sensitive to the
high-frequency words (Dugonik et al., 2014). The
NIST metric is designed to improve BLEU by reward-
ing the translation of infrequently used words. ChrF
is proposed to use character N-gram F-score for au-
tomatic evaluation, which helps to identify different
word combinations.
4.2 Experimental Results
4.2.1 Quantitative Results
We compare the performance of the proposed method
pair2text two attention with baseline methods in Ta-
ble 1.
It can be seen that pair2text two attention
significantly outperforms two baseline methods
in all evaluation metrics. We can also see that
pair2text two attention and pair2text share attention
are both much better than seq2seq attention
method. Specifically, for BLEU-1 score,
pair2text two attention is about 67% higher than
seq2seq attention. For BLEU-4 score, it is about 84%
higher. This indicates that the previous report is very
useful to generate the current report, especially it is
helpful to generate longer N-grams that appear in the
medical report. Also compared to seq2seq attention,
pair2text two attention is an increase of 41% on
ChrF, which means the proposed method learns
well the word combination and the context structure
from the historical diagnostic report. On NIST,
pair2text two attention has also increased by about
115% compared to seq2seq attention, which shows
that the model learned well in the keywords which
appear less frequently in the training data set.
The difference between pair2text share attention
and pair2text two attention is that parame-
ters are shared in alignment score calculation.
Since fewer parameters are needed to learn,
pair2text share attention is more efficient in the
training period. However, the shared parameters
may ignore the difference of weight information
in the historical report and keyword set. From
Table 1, we can see that pair2text two attention
outperforms pair2text share attention method. It is
well known that the longer n-gram scores account
for the fluency of the translation, or to what extent
it reads ”good”. Therefore, from Bleu-1 to Bleu-4,
the difficulty of evaluation gradually increases. Cor-
respondingly the scores show a gradual downward
trend. According to the table 1, the downward trend
of pair2text two attention is the slowest. From
Bleu-1 to Bleu-2, it only decreased by 4%. While
for pair2text share attention, it decreased by 5%. It
demonstrates that by using the different parameters
of the attention module, the relevance of the words
before and after is strongly learned.
4.2.2 Qualitative Results
Table 2 illustrates some patients examples whose
reports are generated by using the proposed method
pair2text two attention. The most previous recent
report, the keyword set, the generated report and the
ground-truth reported are provided in the table.
According to the first record of Table 2, our
method can make good use of the information in
the historical report to supply the lack of the key-
word set. Comparing the historical report and the
current report, it can be seen that most of the current
report and the historical report have a high degree
of similarity in contents and structure, only some
attributes may be different. Take the first record as an
example, information such as “thyroid shape, thyroid
size” and “no obvious abnormality” can be learned
from the historical report, and the information of
“echo distribution” and “echo type” can be obtained
from the keyword set. Using our model, we can
use the information from the historical report and
the keyword set to generate the report with clear
semantics and complete structure.
Comparing the second and third records in Table
2, the keywords of the two records are the same,
however since their historical reports are different,
the generated reports are different and each generated
report is very similar to the ground-truth report.
In the fourth record of Table 2, the
pair2text two attention model not only accurately
obtains the information from the keyword set about
Historical Report Assist Medical Report Generation
171
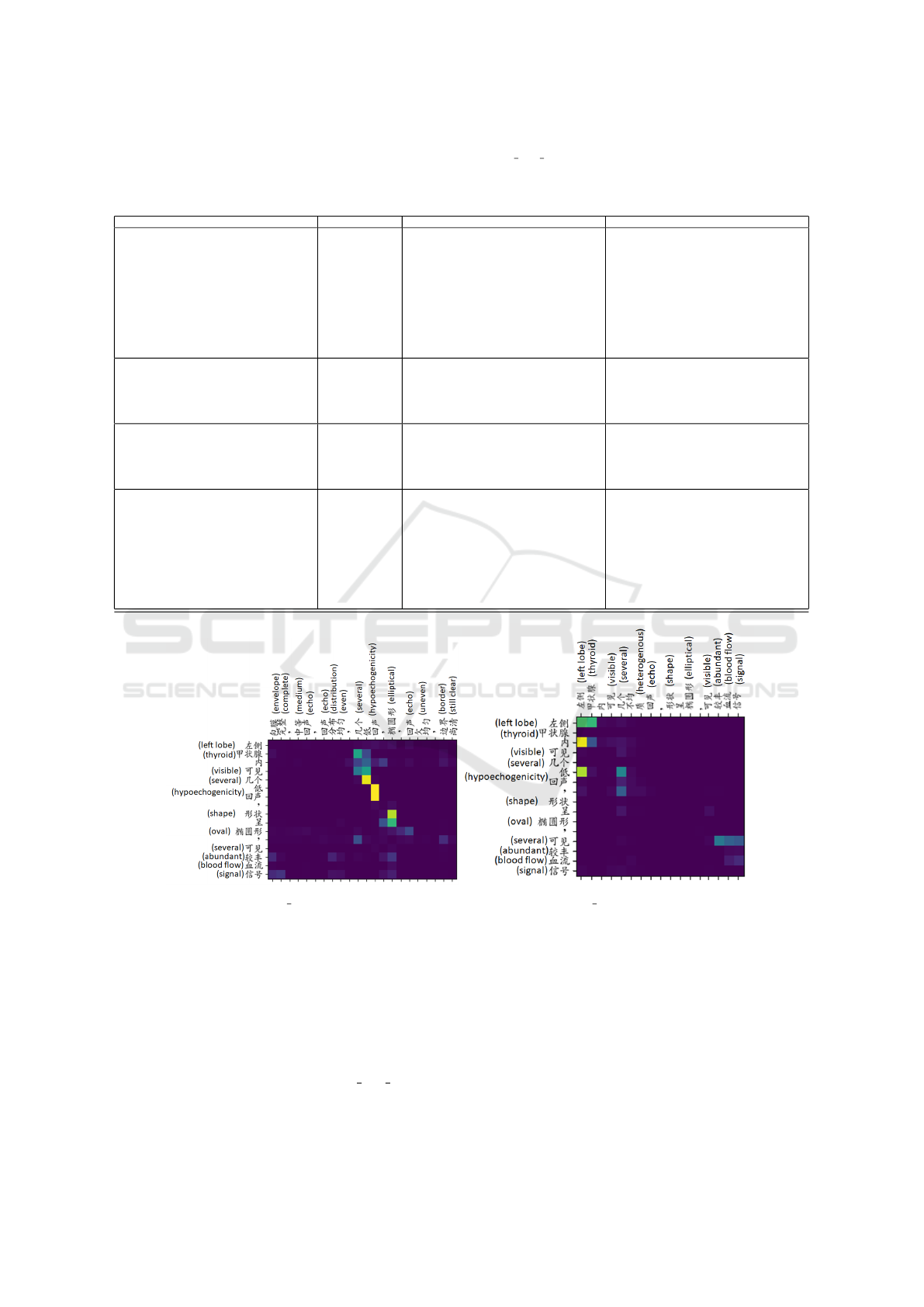
Table 2: Four patient examples whose reports are generated by pair2txt two attention based on the input of keyword set and
historical report. The first example illustrates the association between the current report with the keyword set, historical report
and generated report. The second and third examples have the same keyword set, but different historical reports. The fourth
example shows the trend of nodules over time.
Historical report Keyword set Generated report Ground-truth report
The left and right lobes of the thyroid gland are
normal in shape, the thickness of the isthmus is
normal, the border is clear, the surface is smooth,
the envelope is complete, and the internal echo
is a dense medium echo, and the echo distribu-
tion is heterogenous. CDFI: No obvious abnor-
mal blood flow signal. Several hypoechogenicity
can be seen in the left thyroid gland, the shape
is elliptical, the internal echo is heterogenous,
the border is still clear, and there is no obvious
point-like strong echo inside. CDFI: an abun-
dant blood flow signal is visible. . . . .
Envelope com-
plete, medium
echo, echo dis-
tribution even,
several hypoe-
chogenicity,
elliptical, echo
uneven
The left and right lobes of the thyroid gland are
normal in size and shape, the thickness of the isth-
mus is normal, the boundary is clear, the surface is
smooth, the envelope is complete, and the inside
echo is a dense medium echo, the echoes distribu-
tion is even. CDFI: No obvious abnormal blood
flow signal. Several hypoechogenicity in the left
thyroid gland, the shape is elliptical, the inter-
nal echo is uneven, the boundary is still clear,
and there is no obvious point-like strong echo
inside. CDFI: an abundant blood flow signal is
visible. . . . .
The left and right lobes of the thyroid gland are
normal in size and shape, the thickness of the isth-
mus is normal, the boundary is clear, the surface is
smooth, the envelope is complete, and the inside
echo is a dense medium echo, the echo distribu-
tion is even. CDFI: No obvious abnormal blood
flow signal. Several hypoechogenicity in the left
thyroid gland, the shape is elliptical, the inter-
nal echo is uneven, the boundary is still clear,
and there is no obvious point-like strong echo
inside. CDFI: an abundant blood flow signal is
visible. . . . .
Postoperation, right lobe: anteroposterior di-
ameter, left lobe (resected), isthmus: resected.
In the residual thyroid, the internal echo is a dense
medium echo, and echo distribution is even. . . . .
Envelope com-
plete, medium
echo, echo
distribution
even
Postoperation, left lobe (resected), the residual
right thyroid gland is normal in size and shape,
the boundary is clear, the surface is smooth, the
envelope is complete, and the inside echo is a
dense medium echo, and the echo distribution is
even. . . . .
In the residual right lobe of the thyroid gland
is normal in size and shape, the boundary is clear,
the surface is smooth, the envelope is complete,
and the inside echo is a dense medium echo, and
echo distribution is even. . . . .
The left and right lobes of the thyroid gland are
normal in size and shape, the thickness of the isth-
mus is normal, the boundary is clear, the surface
is smooth, the envelope is complete, and the in-
side echo is a dense medium echo, and the echo
distribution is even. . . .
Envelope com-
plete, medium
echo, echo
distribution
even
The left and right lobes of the thyroid gland are
normal in size and shape, the thickness of the isth-
mus is normal, the boundary is clear, the surface
is smooth, the envelope is complete, and the in-
side echo is a dense medium echo, and the echo
distribution is even. . . .
The left and right lobes of the thyroid gland are
normal in size and shape, the thickness of the isth-
mus is normal, the boundary is clear, the surface
is smooth, the envelope is complete, and the in-
side echo is a dense medium echo, and the echo
distribution is even. . . .
The left and right lobes of the thyroid gland are
normal in size and shape, the thickness of the isth-
mus is normal, the boundary is clear, the surface
is smooth, the envelope is complete, and the in-
side echo is a dense medium echo, and the echo
distribution is even. CDFI: No obvious abnormal
blood flow signal. A mixed echo in the left thy-
roid gland. The shape is elliptical, the internal
echo is uneven, the boundary is still clear, and
there is no obvious point-like strong echo inside.
. . . .
Envelope com-
plete, medium
echo, echo dis-
tribution even,
a liquid mixed
echo, elliptical,
echo distribu-
tion uneven
point-like strong
echo
The left and right lobes of the thyroid gland are
normal in size and shape, the thickness of the isth-
mus is normal, the boundary is clear, the surface
is smooth, the envelope is complete, and the in-
side echo is a dense medium echo, and the echo
distribution is even. CDFI: No obvious abnormal
blood flow signal. A liquid mainly mixed echo
in the left thyroid gland. The shape is ellipti-
cal, the internal echo is uneven, the boundary
is still clear, and there is a spot-like strong echo
(colloid agglutination). . . . .
The left and right lobes of the thyroid gland are
normal in size and shape, the thickness of the isth-
mus is normal, the boundary is clear, the surface is
smooth, the envelope is complete, and the inside
echo is a dense medium echo, and the echo distri-
bution is even. CDFI: No obvious abnormal blood
flow signal. A liquid mainly mixed echo in the
left thyroid. The shape is elliptical, the internal
echo is uneven, the boundary is still clear, and
there is a spot-like strong echo (colloid aggluti-
nation). . . . .
(a) Matrix Keywords-record1 (b) Matrix Report-record1
Figure 3: The attention weight matrix for the first example in Table 2. The row lists the generated report, the column of Figure
(a) is the keyword set, and the column of Figure (b) is the historical report.
the nodule, such as ”a liquid mixed echo”, but also
learn information from ”a mixed echo left thyroid
gland” in the historical report. Then the model can
infer that this is a description of the same nodule
at different times. The echo type of the nodule
changes over time, from ”mixed echo” to ”liquid
mainly mixed echo”. In the pair2text two attention
model, the progress of the disease is learned from the
historical report and the current report in the training
set.
4.2.3 Attention Weight Matrix
To further understand how the historical report and
keyword set to help generate the current report, we
provide the attention weight matrix when the patient
examples’ reports in Table 2 are generated. Since
there are two attention layers in the proposed method,
HEALTHINF 2021 - 14th International Conference on Health Informatics
172

each example has two attention weight matrices (de-
note as Matrix Report and Matrix Keywords in the
following part) corresponding to historical report and
keyword sets. By visualizing the attention weight ma-
trix, we focus on analyzing what the proposed method
learned.
Figure 3 illustrates parts of Matrix Report and
Matrix Keywords of the first report in Table 2. In both
Figure 3a and 3b, each row represents a set of weights
to construct the new vector. For example, there is a
higher weight between row 7 with “hypoechogenic-
ity” and “hypoechogenicity” of keyword set in Figure
3a. Since “left lobe” does not appear in the keyword
set, in the first row of Figure 3a, the weights are all
close to 0. In contrast, in the first row of Figure 3b,
the corresponding words “left” and “ thyroid” have
higher weight.
By comparing Figure 3a and 3b, it can be seen that
the model learns “left thyroid” from historical reports
and “several hypoechogenicity visible” from keyword
set. We can also infer that potential relevance between
phrases is learned, such as “left” and “thyroid”. Such
relevance could be exploited to estimate the probabil-
ity distribution of the words to be generated. Let’s see
the rows in Figure 3b. the generated words “visible,
abundant” and “ blood, flow, signal” in the historical
report have higher weights. However, the generated
word “visible” and ”visible” in the historical report
the historical report has small weight. At the same
time, the subsequent words “blood flow signal” in the
generated report depends on the generated word “vis-
ible”. The potential reason might be that the learned
relevance influences the probability distribution cal-
culated based on the part of the generated report.
5 CONCLUSION
This paper proposed the method that generates the
current medical report both from the most recent
previous report and the keyword set observed from
the current medical image. The experimental re-
sults demonstrated the effectiveness of the proposed
method. In the future, we plan to design a more effi-
cient learning strategy for model inference. Also, the
method that the previous report helps the generation
of the keyword set is to be investigated.
ACKNOWLEDGEMENTS
This work were supported by the National Key
R&D Program of China (2019YFE0190500) and the
Shanghai Innovation Action Project of Science and
Technology (18511102703).
REFERENCES
Cho, K., Van Merri
¨
enboer, B., Gulcehre, C., Bahdanau,
D., Bougares, F., Schwenk, H., and Bengio, Y.
(2014). Learning phrase representations using rnn
encoder-decoder for statistical machine translation.
arXiv:1406.1078.
Doddington, G. (2002). Automatic evaluation of machine
translation quality using n-gram co-occurrence statis-
tics. In Proceedings of the second international con-
ference on Human Language Technology Research,
pages 138–145.
Dugonik, J., Boskovic, B., Maucec, M. S., and Brest, J.
(2014). The usage of differential evolution in a statis-
tical machine translation. In 2014 IEEE Symposium
on Differential Evolution (SDE), pages 1–8.
Hochreiter, S. and Schmidhuber, J. (1997). Long short-term
memory. Neural computation, 9(8):1735–1780.
Jing, B., Xie, P., and Xing, E. (2017). On the
automatic generation of medical imaging reports.
arXiv:1711.08195.
Kingma, D. P. and Ba, J. (2014). Adam: A
method for stochastic optimization. arXiv preprint
arXiv:1412.6980.
Kisilev, P., Sason, E., Barkan, E., and Hashoul, S. (2016).
Medical image captioning: Learning to describe med-
ical image findings using multi-task-loss cnn. Deep
Learning for Precision Medicine.
Kisilev, P., Walach, E., Barkan, E., Ophir, B., Alpert, S.,
and Hashoul, S. Y. (2015a). From medical image to
automatic medical report generation. IBM Journal of
Research and Development, 59(2/3):2–1.
Kisilev, P., Walach, E., Hashoul, S. Y., Barkan, E., Ophir,
B., and Alpert, S. (2015b). Semantic description of
medical image findings: structured learning approach.
In BMVC, pages 171–1.
Li, C. Y., Liang, X., Hu, Z., and Xing, E. P. (2019).
Knowledge-driven encode, retrieve, paraphrase for
medical image report generation. In AAAI, volume 33,
pages 6666–6673.
Li, Y., Liang, X., Hu, Z., and Xing, E. P. (2018). Hybrid
retrieval-generation reinforced agent for medical im-
age report generation. In NIPS, pages 1530–1540.
Lin, M., Chen, Q., and Yan, S. (2013). Network in network.
arXiv preprint arXiv:1312.4400.
Mnih, V., Heess, N., Graves, A., et al. (2014). Recurrent
models of visual attention. In Advances in neural in-
formation processing systems, pages 2204–2212.
Papineni, K., Roukos, S., Ward, T., and Zhu, W. (2002).
Bleu: a method for automatic evaluation of machine
translation. In Proceedings of the 40th annual meet-
ing of the Association for Computational Linguistics,
pages 311–318.
Popovi
´
c, M. (2015). chrf: character n-gram f-score for au-
tomatic mt evaluation. In Proceedings of the Tenth
Historical Report Assist Medical Report Generation
173

Workshop on Statistical Machine Translation, pages
392–395.
Schuster, M. and Paliwal, K. K. (1997). Bidirectional re-
current neural networks. IEEE transactions on Signal
Processing, 45(11):2673–2681.
Shin, H., Roberts, K., Lu, L., Demner-Fushman, D., Yao, J.,
and Summers, R. M. (2016). Learning to read chest
x-rays: Recurrent neural cascade model for automated
image annotation. In CVPR, pages 2497–2506.
Wang, X., Peng, Y., Lu, L., Lu, Z., and Summers, R. M.
(2018). Tienet: Text-image embedding network for
common thorax disease classification and reporting in
chest x-rays. In CVPR, pages 9049–9058.
Xu, K., Ba, J., Kiros, R., Cho, K., Courville, A., Salakhudi-
nov, R., Zemel, R., and Bengio, Y. (2015). Show, at-
tend and tell: Neural image caption generation with
visual attention. In ICML, pages 2048–2057.
Xue, Y., Xu, T., Long, L. R., Xue, Z., Antani, S., Thoma,
G. R., and Huang, X. (2018). Multimodal recurrent
model with attention for automated radiology report
generation. In International Conference on Medical
Image Computing and Computer-Assisted Interven-
tion, pages 457–466.
Zaremba, W., Sutskever, I., and Vinyals, O. (2014). Re-
current neural network regularization. arXiv preprint
arXiv:1409.2329.
Zhang, Z., Xie, Y., Xing, F., McGough, M., and Yang, L.
(2017). Mdnet: A semantically and visually inter-
pretable medical image diagnosis network. In CVPR,
pages 6428–6436.
HEALTHINF 2021 - 14th International Conference on Health Informatics
174
