
Reusability of Interfaces in Healthcare EAI Environments
Severin Linecker
1,2
and Wolfram W
¨
oß
1
1
Johannes Kepler University Linz, Austria
2
Vinzenz Gruppe, Linz, Austria
Keywords:
Enterprise Application Integration, EAI, Middleware, Message-oriented Middleware, MOM, HL7, System
Integration, Healthcare.
Abstract:
Enterprise Application Integration (EAI) and HL7 (Health Level Seven) messaging are well established tech-
nologies in healthcare environments. Due to the widely adoption of HL7 messaging, especially the version
2, in the healthcare domain and its flexibility, many vendor specific implementations exist. To integrate these
systems, messages have to be adapted to the vendor specific requirements, even if the functionality is nearly
the same. This leads to an increasing number of special interfaces and decreased maintainability. This paper
shows a generic architecture for reusable interfaces for HL7 messaging by considering reusability at data level
and interface level and the results when applied to a real production EAI environment of an austrian healthcare
provider.
1 INTRODUCTION
Exchanging clinical data between multiple heteroge-
neous medical information systems is very common
in healthcare environments. The Hospital Informa-
tion System (HIS) and other special (sub)systems,
such as the Radiological Information System (RIS)
need to be integrated for digital clinical workflows.
Therefore Enterprise Application Integration (EAI)
and HL7 (Health Level Seven) messaging are well es-
tablished technologies in healthcare environments.
Due to the message oriented nature of HL7,
Message-oriented Middleware (MOM) is a common
paradigm for implementing EAI in healthcare envi-
ronments (Bezerra et al., 2015). It allows systems to
communicate with each other by sending and receiv-
ing messages using interfaces directly connected to
the middleware, which is then responsible for rout-
ing these messages to their correct destinations. This
helps to reduce the total number of interfaces needed
to connect n systems from (n ∗(n−1))/2, when using
point-to-point interfaces, to n. Especially for com-
plex and big healthcare environments, which often
consist of 50 or more connected systems (like in the
case of the Vinzenz Gruppe, an association of seven
religious-order hospitals and other healthcare facili-
ties in Austria), this is a necessity. HL7 is a mes-
saging standard specifically developed for exchang-
ing data between information systems in healthcare
environments. Version 2 (HL7 V2.x) of the messag-
ing standard was first released in 1987 and, accord-
ing to (HL7 International, 2020), is one of the most
widely used standard for healthcare information ex-
change. The HL7 V2.x standard (ISO, 2009) defines
message types and their (real world) trigger events for
clinical, financial and administrative data exchange.
Messages have a data type and a trigger event, which
together define a specific sequence of segments and
segment groups. For example, the ADT (Admission,
Discharge and Transfer) message type and the trigger
event A02 is used for transmitting patient administra-
tion information about a patient transfer. The follow-
ing listing shows the message type definition of an
HL7 ADTˆA02 message:
MSH Message Header
[{ SFT }] Software Segment
EVN Event Type
PID Patient Identification
[ PD1 ] Additional Demographics
[{ ROL }] Role
PV1 Patient Visit
[ PV2 ] Patient Visit - Additional Info.
[{ ROL }] Role
[{ DB1 }] Disability Information
[{ OBX }] Observation/Result
[ PDA ] Patient Death and Autopsy
Segments are a logical grouping of data fields.
They may be required, optional or repetitive within
a message type. Two or more segments may be
Linecker, S. and Wöß, W.
Reusability of Interfaces in Healthcare EAI Environments.
DOI: 10.5220/0010242004170423
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 417-423
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
417

Figure 1: Example HL7 V2.5 ADTˆA02 message.
grouped together as a logical unit. Each segment has
a unique name called Segment ID with three upper
case characters (e.g., MSH, PID, PV1). Fields are char-
acter strings within a segment. They have an ordi-
nal position within the segment for reference (e.g.,
PID.3), have a data type, can be required or optional
and may be repetitive. Depending on its data type, a
field may consist of components, which in turn may
contain subcomponents. HL7 V2.x messages are typ-
ically plain text messages with certain special char-
acters used as delimiter. They can be negotiated be-
tween applications, but typically the HL7 recommen-
dation is used. Figure 1 shows an ADTˆA02 message
with the HL7 V2.x typical delimiters | for fields, ˆ
for components, & for subcomponents, ˜ for repetitive
fields and \ as escape character. Segments are always
terminated by a carriage return.
No matter how detailed the specification is, HL7
V2.x is a standard for syntactic but not for semantic
interoperability. The context of a field is defined in
the standard, but leaves the implementers the flexibil-
ity to use a free text or a coded value from a stan-
dard terminology. These details have to be negotiated
between the issuer and the recipient of a message to
ensure correct interpretation. This step is not done
automatically, but usually in advance by the interface
developers of the corresponding systems.
In hospital environments the HIS is a central point
for data exchange. The connected systems send their
data to the HIS, but also require its data. Especially
patient administration data is required by most of the
systems. These are distributed to them with HL7 ADT
messages using middleware technology. The prob-
lem is that due to the flexibility of the HL7 standard,
the messages often have to be adapted to meet the re-
quirements of the receiving system. This leads to an
increased number of special interfaces and decreased
maintainability. In order to save time and resources
during the development of integration projects, it is
important to have reusable interfaces available that al-
low these adaptions using configuration. To meet the
objective above, this work introduces a generic archi-
tecture for creating reusable interfaces, by consider-
ing reusability 1) at data level by splitting up message
flow in multiple interfaces and 2) at interface level by
using twelve reusable components.
The remainder of the paper is organized as fol-
lows: Section 2 contains related work. In Section 3
the two levels of the architecture are described in de-
tail. In Section 4 the evaluation results of applying the
proposed architecture to a real production healthcare
EAI environment are shown. The paper finishes with
Section 5 with conclusion and future work.
2 RELATED WORK
The authors of (Bezerra et al., 2020) show a middle-
ware architecture consisting of a cloud service and lo-
cal clients. Reusability was taken into account by sep-
arating the business rules from the persistence layer
on the client side, and on the server side by providing
the middleware functionalities via a central cloud ser-
vice. Reusability is also considered in the work of (Li-
Fan Ko et al., 2006), where a SOA based middleware
framework for healthcare information systems was
proposed. Another SOA based EAI approach (non
healthcare) is done by (Jun Gui and Hebiao Yang,
2010), where service components can be reused for
existing or newly developed components.
Even though there are some more studies about
HL7, healthcare information exchange, EAI and mid-
dleware architecture in the healthcare domain like
(Alenazi and Alhamed, 2015), (Wadhwa et al., 2015),
(Liu and Huang, 2012), (Lu et al., 2010), (Bortis,
2008) or (Vargas and Pradeep Ray, 2003), their main
objective is not reusability. Their concern is the in-
tegration problem itself and not reusing integration
components for further integration needs.
The contribution of this work is a generic architec-
ture for HL7 based messaging, used for implementing
highly reusable interfaces and components in (exist-
ing) healthcare EAI environments.
3 ARCHITECTURE
In this section, an architecture for interfaces is pre-
sented, where reusability is considered in all parts of
an EAI environment. This includes the general design
of message flows between systems within the EAI en-
vironment (data level), which is shown in Section 3.1,
and a component based architecture for implementing
interfaces (interface level), shown in Section 3.2.
3.1 Messaging
Instead of creating one single interface for connect-
ing source and destination system(s), message paths
HEALTHINF 2021 - 14th International Conference on Health Informatics
418

Figure 2: Asynchronous message flow between multiple systems.
should be composed out of multiple interfaces inter-
connected with message queues. Figure 2 shows an
asynchronous message path from a source system to
two destination systems split up into three steps, each
with different responsibilities. This architecture al-
lows branching off messages after each step, reusing
the output of one interface as an input for another in-
terface. The following sections describe the function-
ality of each interface in more detail.
3.1.1 Receiver
The Receiver interface gets the message from a source
system via a communication channel (File, HTTP,
MLLP, SOAP, REST, ...). It checks the syntactical
correctness of the received message and generates an
appropriate response if required by the used com-
munication protocol. In HL7 messaging the Mini-
mal Lower Layer Protocol (MLLP) is widely used
for sending and receiving HL7 messages via network
sockets. After checking syntactical correctness, the
business keys of the message are extracted and stored
together with the raw message in a message back-
up/journal. This is needed for searching and resend-
ing messages manually in case of an error. Finally,
the message is passed to one or many message queues
or gets filtered due to specified filter criteria. After-
wards, processing of the receiver interface ends.
Errors during message processing are reported to
the administrator, who is responsible for monitoring
the EAI environment. This applies to all other inter-
faces as well and is not mentioned anymore in the fol-
lowing sections.
3.1.2 Transformer
First, the Transformer interface reads the message
from a message queue. Afterwards, it transforms the
message as needed. This can be format conversion,
like transforming an XML message or a proprietary
HIS message format to an HL7 V2.x message, or per-
forming changes to a HL7 message. Finally, the trans-
formed message is passed to one or many message
queues or gets filtered. Processing of the Transformer
interface ends afterwards.
The Transformer interface is not needed in all
message streams between source and destination sys-
tem and can be omitted in cases where no message
transformation is needed at all. But even if there
is no transformation needed, there are scenarios that
require special routing and filtering capabilities be-
tween Receiver and Sender interfaces. In this case the
transformation part is skipped and only the routing
and filtering part is done. These interfaces are called
Router or Forwarder interfaces.
3.1.3 Sender
The Sender interface reads a message from a message
queue. It checks the syntactical correctness and the
presence of all needed data for the destination system.
Like the Receiver interface, it also extracts business
keys from the message and stores them with the raw
message in a backup/journal. Finally, the message is
transmitted to the destination system using a commu-
nication channel (e.g., File, MLLP, SOAP, REST, DB,
SAP RFC). Restricting the number of outbound com-
munication channels to one has reliability reasons. If
Sender 1 in Figure 2 would also send to Destination 2,
and Destination 1 is not reachable, messages could
not be delivered to Destination 2 as well.
3.2 Interface Components
Reusable interfaces are built to reduce the amount of
effort and time needed to build integration solutions.
The main idea is to build an abstraction layer on top
of an existing EAI platform to abstract limitations re-
garding reusability and interface architecture in gen-
eral, and to provide a generic API for interface devel-
opment. The goal is that code, once written, can be
reused multiple times, saving a vast amount of time
in integration projects and in case of migrating to new
platforms.
Reusability is achieved by splitting up an inter-
face implementation into different components, each
with its own responsibility within the whole integra-
tion task. Figure 3 shows twelve components used for
interface implementation. The provided structure and
Reusability of Interfaces in Healthcare EAI Environments
419
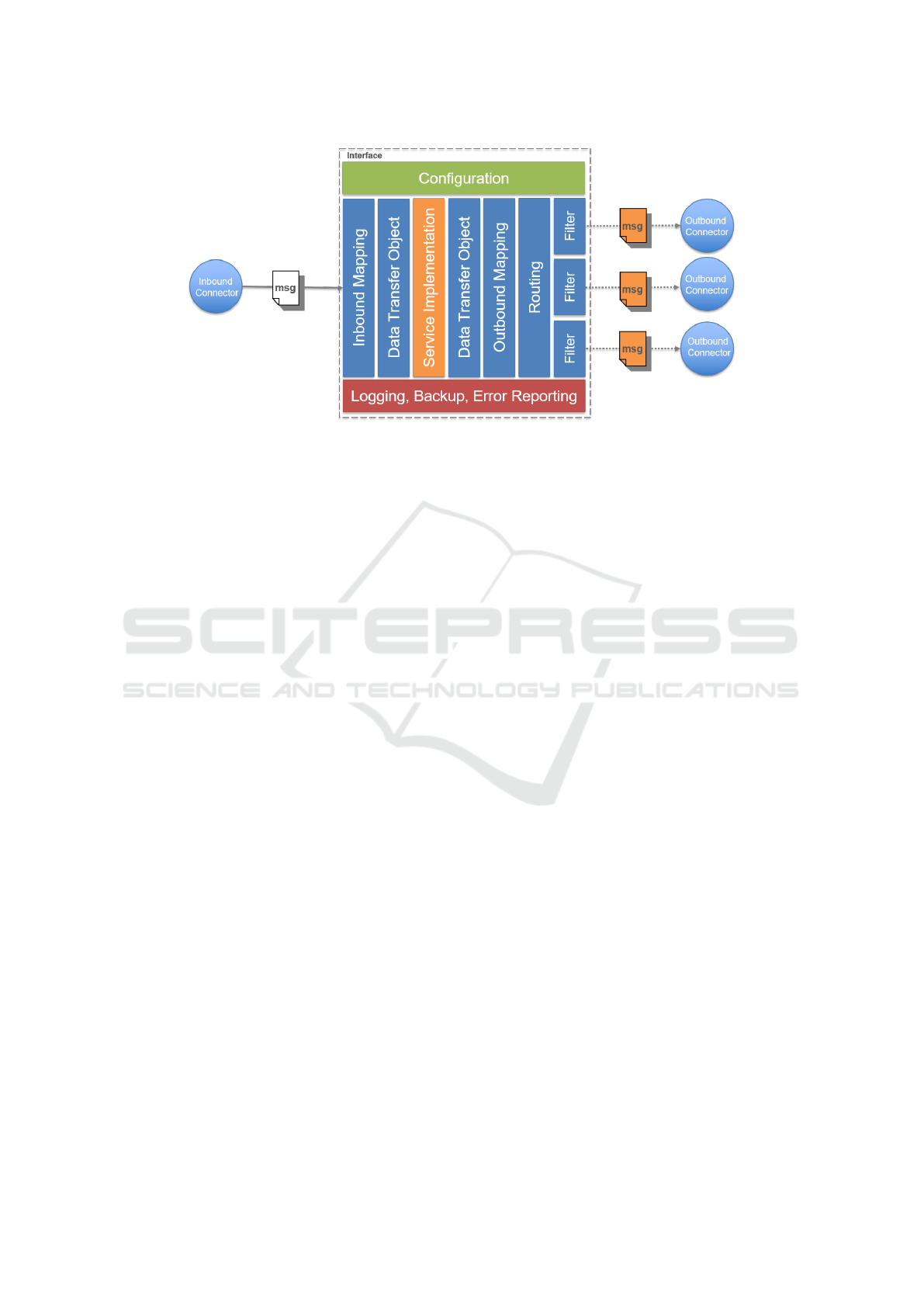
Figure 3: Components of an interface.
components can be implemented on top of an existing
EAI platform, or for standalone integration solutions.
The following twelve components are used to
build (reusable) interfaces:
• Inbound Connector:
The Inbound Connector component is used for
reading raw messages (e.g., text messages) from
a communication channel (File, Message Queue,
Socket, HTTP, ...).
• Data Transfer Object:
A Data Transfer Object (DTO) defines a data
structure, which is used by the Service Implemen-
tation during processing. It is an abstract repre-
sentation of the data being used by an interface.
DTOs form the basis for generic reusable inter-
faces by providing access to the required data in a
message structure independent way.
• Inbound Mapping:
The Inbound Mapping transforms the incoming
raw message to a DTO structure. Therefore it
uses appropriate parsers (e.g., HL7 parser) to ver-
ify the syntactic correctness of the incoming mes-
sage and to access its fields for extraction.
After parsing and DTO field extraction, the data
has to be verified. This includes checking the
presence of all required fields and their semantic
correctness. After the successful completion of
all Inbound Mapping steps, the result is a DTO
message containing all fields necessary for the
Service Implementation component to perform its
task. Errors during parsing or field validation get
logged by the Logging component and/or reported
using the Error Reporting component.
• Service Implementation:
The Service Implementation component is re-
sponsible for performing the business logic of the
interface. This is the main part of any interface
implementation. It only operates on DTOs and is
therefore independent of the original and/or target
message structure. Accessing other data, which is
not present in the DTO, requires the usage of Data
Access Objects (DAO).
• Outbound Mapping:
The Outbound Mapping component performs the
inverse operation to an Inbound Mapping. It takes
a DTO and transforms it to a target message struc-
ture (e.g., HL7 V2.x message). If necessary, char-
acter set transformation and proper escaping of
certain special characters is done here.
• Routing:
Selecting the correct destination Outbound Con-
nector for a given message is done by the Routing
component. Static and dynamic routing is sup-
ported and is achieved using configuration or Fil-
ter components.
• Filter:
A Filter component produces a boolean output for
a given arbitrary input. Filters can be conjuncted
with the logical operations and, or and not.
• Outbound Connector:
Outbound Connectors are used for sending raw
message data to an outbound communication
channel (File, Message Queue, Socket, HTTP, ...).
• Configuration:
Each component has to provide useful configu-
ration options, but always has a runnable default
configuration suitable for most integration scenar-
ios. The principle convention over configuration
applies here. Each interface has its own configu-
ration possibility, containing all configuration op-
tions set for all components.
HEALTHINF 2021 - 14th International Conference on Health Informatics
420

• Logging:
The Logging component is used by all other com-
ponents. For traceability of message flows at least
the incoming and the outgoing message(s) should
be logged.
• Backup:
The Backup component is used on messages en-
tering and leaving the EAI environment. The raw
data and business keys of the message are stored
in a database to enable searching and resending of
messages in case of errors during processing.
• Error Reporting:
When an error occurs, the Error Reporting com-
ponent is used to send notifications to responsible
addressees. To distinguish between different error
conditions, hierarchical error codes are used.
Not every component has to be used in a specific in-
terface implementation. They are to be seen as build-
ing blocks that enable or facilitate the development
of interfaces. There are three different approaches to
achieve reusability at interface level:
1. Implementation of multiple generic components
that serve as building blocks for interfaces. The
interfaces themselves cannot be reused, but their
individual components can. For example, a
generic Filter component can be implemented
which checks the content of a field. Both the
specific field (e.g., PID.3 from an HL7 message)
and the check itself (e.g., a REGEX) can be pro-
vided as a configuration option. This approach is
most suited for environments having a (manage-
able) range of functionality that has to be com-
posed in many different ways and there is less or
no need of reusing an interface as a whole.
2. Implementation of interfaces using type specific
components. Here the interfaces are reusable
themselves, but not their individual compo-
nents. Therefore the components have to be re-
implemented for each type of interface. This ap-
proach is best suited for (smaller) environments
where interfaces can be grouped together based on
their functionality. For example, having only in-
terfaces for patient administrative data using HL7
ADT messages. This approach also suits well for
simple ad-hoc integration solutions, which may
not need an implementation for all different com-
ponent types.
3. A hybrid approach, where the implementation of
interfaces uses both, generic and specific compo-
nents. This approach suits well for environments,
having interfaces of certain types (patient admin-
istration, observations results, MLLP communi-
cation, ...) and also special interfaces which do
share some functionality. Furthermore some com-
ponents are available in a generic reusable way
(Logging, Backup, Error Reporting, Routing, Fil-
ter, ...).
4 EVALUATION
This architecture was implemented and deployed
in the EAI production environment of the Vinzenz
Gruppe. At the end of 2014 the production EAI envi-
ronment consisted of 342 interfaces deployed to three
production servers. Each of these interfaces was im-
plemented using its own Java class, thus class reusage
was not present at all, even many of the existing in-
terfaces did similar tasks. Code reusage was primar-
ily based on copy and paste with subsequent manual
adaptation. As a result many interfaces had a com-
mon basis, but there were numerous extensions and
variants concerning for example, the message struc-
ture, the use of free text fields, additional fields and
data mappings.
With the beginning of 2015 an analysis was ini-
tiated to find interface categories sharing common
functionality. The hybrid approach for interface
reusability was then used to implement a config-
urable standard implementation for each interface
category. The four most important ones were: a
MLLP Sender interface [A], a MLLP Receiver in-
terface [B], an interface for routing and forward-
ing of arbitrary messages [C], and a standard HL7
ADT Transformer interface [D]. Furthermore, con-
figurable generic components were implemented for
functionalities that were required by many interfaces.
These were Logging, Backup, Error Reporting, Rout-
ing, Filter, Inbound- and Outbound Connector com-
ponents.
For new interfaces the standard interfaces were
used where appropriate, and the rollout was done by
configuring instances of them accordingly. Further-
more old legacy interfaces were replaced with the
equivalent standard implementation whenever possi-
ble, or have been reimplemented with the proposed
architecture. This led to an increasing number of
reusable components and interface classes.
The current EAI production environment con-
sists of 534 interfaces, deployed to seven production
servers. 86 interfaces are legacy interfaces which do
not conform to the architecture presented in this pa-
per. Table 1 shows the number of interface classes
and the number of instances of each class running in
the production environment.
The pie chart of Figure 4 shows that the top four
interface classes which have a reusage count N >= 25
Reusability of Interfaces in Healthcare EAI Environments
421
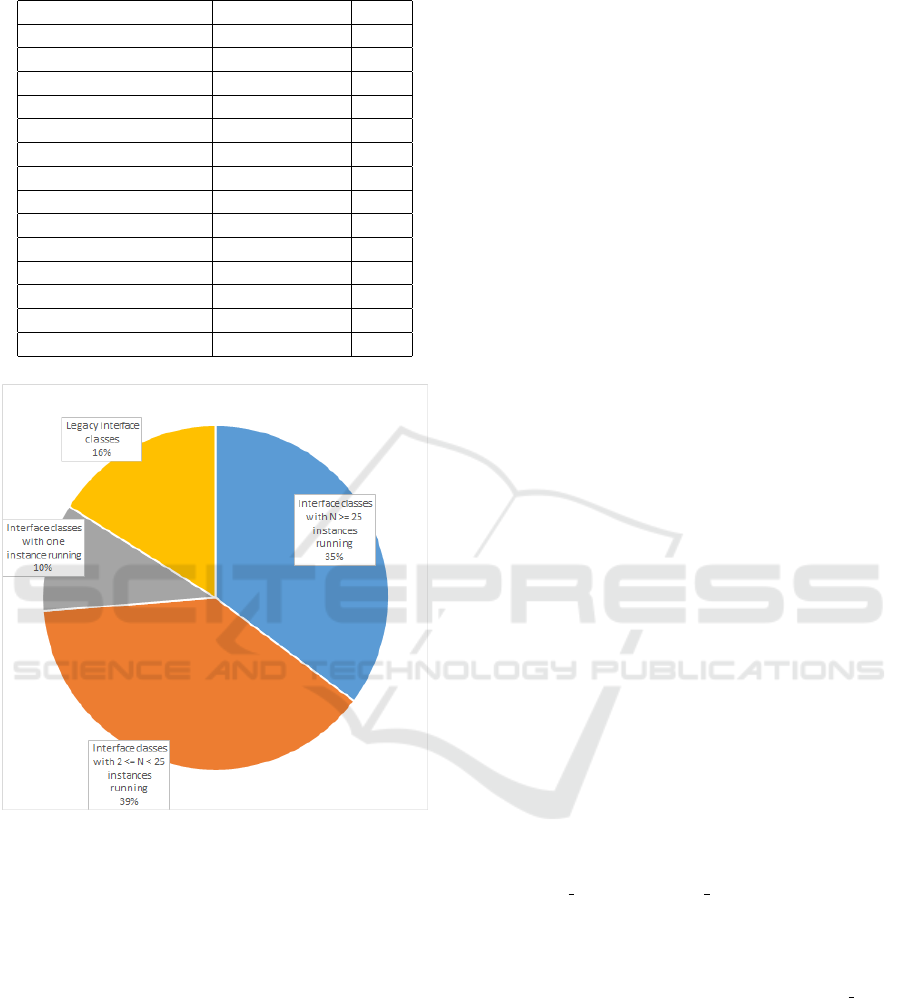
Table 1: Reusage statistics of different interface classes.
N.o. interface classes Instances each Sum
1 [A] 70 70
1 [B] 46 46
1 [C] 45 45
1 [D] 27 27
3 9 27
4 8 32
9 7 63
2 6 12
5 5 25
4 4 16
3 3 9
11 2 22
54 1 54
legacy 86 86
Figure 4: Pie chart of interface class reusage.
make up 35 % of all interfaces running. Adding the
39 % of all interface classes with a reusage count
2 <= N < 25, 74 % of all running interface instances
reuse an interface class. Using the proposed architec-
ture we could increase interface class reusage from
0 % to 74 % which helped saving time and money on
new integration projects.
5 CONCLUSION AND FUTURE
WORK
In this paper an architecture for reusable interfaces
using a multi step message flow design and reusable
components for interface implementation was shown.
The introduction of an abstraction layer between an
EAI platform and the interface implementations eases
the implementation of generic reusable interfaces.
Code, that has been written once, can now easily be
reused either as a component in a new interface imple-
mentation or as an entire interface. This helps to save
resources when developing new integration projects.
The abstraction of the EAI platform is the first step
to replace the existing system with a new one. It is
planned to analyse the reusability capabilities of in-
terfaces implemented with the architecture shown in
this paper when migrating them to a new EAI plat-
form.
REFERENCES
Alenazi, T. M. and Alhamed, A. A. (2015). A middleware
to support hl7 standards for the integration between
healthcare applications. In Balakrishnan, P., Srivat-
sava, J., Fu, W.-T., Harabagiu, S. M., and Wang, F.,
editors, ICHI, pages 509–512. IEEE Computer Soci-
ety.
Bezerra, C., Araujo, A., Sacramento, B., Pereira, W., and
Ferraz, F. (2015). Middleware for heterogeneous
healthcare data exchange: a survey. In ICSEA 2015
Tenth International Conference on Software Engineer-
ing Advances, pages 409–414.
Bezerra, C. A. C., de Ara
´
ujo, A. M. C., and Times, V. C.
(2020). An hl7-based middleware for exchanging data
and enabling interoperability in healthcare applica-
tions. In Latifi, S., editor, 17th International Con-
ference on Information Technology–New Generations
(ITNG 2020), pages 461–467, Cham. Springer Inter-
national Publishing.
Bortis, G. (2008). Experiences with mirth: An open source
health care integration engine. In Proceedings of the
30th International Conference on Software Engineer-
ing, ICSE ’08, page 649–652, New York, NY, USA.
Association for Computing Machinery.
HL7 International (2020). Hl7 version 2 prod-
uct suite. https://www.hl7.org/implement/standards/
product
brief.cfm?product id=185. Last checked on
Sep 09, 2020.
ISO (2009). ISO/HL7 27931:2009 Data exchange standards
– health level seven version 2.5 – an application pro-
tocol for electronic data exchange in healthcare en-
vironments. http://www.iso.org/iso/catalogue detail.
htm?csnumber=44428.
Jun Gui and Hebiao Yang (2010). Realization of eai based
on service-oriented architecture. In 2010 Interna-
tional Conference on Educational and Information
Technology, volume 2, pages V2–424–V2–428.
Li-Fan Ko, Jen-Chiun Lin, Chi-Huang Chen, Jie-Sheng
Chang, Faipei Lai, Kai-Ping Hsu, Tzu-Hsiang Yang,
Po-Hsun Cheng, Chia-Chang Wen, Jun-Lian Chen,
and Siao-Lin Hsieh (2006). Hl7 middleware frame-
work for healthcare information system. In HEALTH-
COM 2006 8th International Conference on e-Health
HEALTHINF 2021 - 14th International Conference on Health Informatics
422

Networking, Applications and Services, pages 152–
156.
Liu, L. and Huang, Q. (2012). An extensible hl7 mid-
dleware for heterogeneous healthcare information
exchange. In 2012 5th International Conference
on BioMedical Engineering and Informatics, pages
1045–1048.
Lu, X., Gu, Y., Yang, L., Jia, W., and Lei Wang (2010).
Research and implementation of transmitting and in-
terchanging medical information based on hl7. In The
2nd International Conference on Information Science
and Engineering, pages 457–460.
Vargas, B. and Pradeep Ray (2003). Interoperability of
hospital information systems: a case study. In Pro-
ceedings 5th International Workshop on Enterprise
Networking and Computing in Healthcare Industry
(HealthCom), pages 79–85.
Wadhwa, R., Mehra, A., Singh, P., and Singh, M. (2015).
A pub/sub based architecture to support public health-
care data exchange. In 2015 7th International Conf.
on Communication Systems and Networks (COM-
SNETS), pages 1–6.
Reusability of Interfaces in Healthcare EAI Environments
423
