
Development of a Purchasing Portfolio Model for the Health Sector:
A Case Study of a Central Hospital
Amílcar Arantes
1a
and Andreia Frias Alhais
2
1
CERIS, CESUR, Instituto Superior Técnico, Universidade de Lisboa, Av. Rovisco Pais, Lisboa,1049-001, Portugal
2
DEG, Instituto Superior Técnico, Av. Prof. Dr. Cavaco Silva, Porto Salvo, 2744-016, Portugal
Keywords: Purchasing Portfolio, Kraljic Portfolio Matrix, Analytic Hierarchy Process, Health Sector.
Abstract: Over the years, the purchasing area has taken on an essential role in the management of companies in all
activity sectors. In the health sector, purchasing medicines is highly important considering the amounts
involved, the impact on the service quality, and the wide variety of purchased products. This research work
combined action research with a case study and aims to apply to a Central Hospital a Purchasing Portfolio
Model based on the Kraljic Purchasing Matrix (KPM). The KPM allows for the classification of different
classes of medicines in accordance with their impact on profits and supply risk dimensions, making it possible
to define differentiated purchasing strategies. This application used the Analytical Hierarchical Process (AHP)
tool for criteria prioritization and used direct measurement for criterion rating. By applying the model to a
Central Hospital, this study seeks to increase the areas of applicability of purchasing portfolio models.
Moreover, the results confirmed the model's value in defining medicine purchasing strategy at the Central
Hospital and also gave rise to guidelines for applying the model.
1 INTRODUCTION
In recent years in Portugal, the health sector has
evolved, in both the public and private sectors,
through the implementation of a set of structural
reforms, the reinforcement of the health care network,
and a process of modernization and digital
transformation (Ministério da Saúde, 2018). In 2018
total health expenditure (public and private)
represented about 9.1% of the Portuguese Gross
Domestic Product, with the general public spending
about 4.4%. These values demonstrate the importance
of the health sector in the Portuguese economy.
The hospital procurement of medicines involves a
wide range of financial resources and time. It carries
certain risks, especially in terms of storage, as most
handled products are fragile and must not be defective
when they are used. Furthermore, given the large
quantity and variety of products and services that
have to be purchased, not all medicines should be
managed and purchased in the same way. According
to Medeiros & Ferreira (2018), the purchase portfolio
can be an excellent tool for strategic management
hospital purchases.
a
https://orcid.org/0000-0003-1207-5854
The most recognized and commonly used
Purchasing Portfolio Model (PPM) was introduced by
Kraljic (1983). This model is considered an important
advance in purchasing area development and
considers a matrix that classifies product item classes
into four categories: non-critical, bottleneck,
leverage, and strategic; and according to two
dimensions – profit impact, and supply risk. This
matrix allows for the definition of purchasing
strategies according to the characteristics of each
product item class (Gelderman, 2003). A set of
criteria must be defined for each of the Kraljic
Purchasing Matrix (KPM) dimensions and be
weighted using the Analytic Hierarchy Process
(AHP) tool. The Kraljic matrix has already been
applied in several areas. However, in the literature the
number of reported applications in the health sector is
limited.
This paper is organized as follows: firstly, the
portfolio approach based on the Kraljic model is
presented; secondly, the research method is
described, then, thirdly, the selected case study is
summarily described; fourthly, the PPM is developed
with the help of the AHP for criteria prioritization;
Arantes, A. and Alhais, A.
Development of a Purchasing Portfolio Model for the Health Sector: A Case Study of a Central Hospital.
DOI: 10.5220/0010225903290337
In Proceedings of the 10th International Conference on Operations Research and Enterprise Systems (ICORES 2021), pages 329-337
ISBN: 978-989-758-485-5
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
329

fifthly, there is a report on the results obtained and
discussion thereof; and finally, in the conclusions, the
main findings and implications are presented.
2 LITERATURE REVIEW
The healthcare supply chain is a complex and
fragmented process, and management thereof
encompasses managing suppliers, procuring
resources, and delivering goods and services to
providers and patients. Moreover, the customer
service level of the healthcare supply chain is of
paramount importance, given the direct impact it has
on the health and safety of the patients (Uthayakumar
& Priyan, 2013).
Hospitals have many different departments
provide healthcare services, requiring a wide range of
products (and services) that the procurement area
seeks to provide, including consumables such as
medicines, and permanent material, such as medical
equipment (Almeida & Lourenço, 2009). Medicines
constitute the highest costs in running a hospital; they
usually account for between 40% and 60% of the
public sector budget (Medeiros & Ferreira, 2018).
Management of these products is critical because they
must be transported and stored in specific conditions,
there can be no stockout, and they come with an
expiration date. Thus, the purchasing experts must
carefully decide which products to order, in what
quantities, and when to place orders, so as to serve
patients in a timely and efficient way (Uthayakumar
& Priyan, 2013). Furthermore, considering the vast
differences in the characteristics of the products,
often it is necessary to organize and categorize them
in order to define adequate purchasing strategies. For
this, PPMs are useful tools to manage medicine
purchases strategically in accordance with the
specific characteristics of each product (Medeiros &
Ferreira, 2018).
Kraljic (1983) created the most frequently used
and recognized portfolio approach to purchasing
(Pardo et al., 2011). The KPM considers the strategic
impact and supply risk dimensions. It can be
beneficial to management, namely in having a
trustworthy insight into supply risk and negotiating
power and making it possible to define the most
appropriate purchasing strategies. Kraljic (1983)
highlights a matrix that classifies products (or classes
of products) purchased by a company in four
categories: non-critical, bottleneck, leverage, and
strategic; and according to two dimensions – the
supply risk and the profit impact (Table 1). However,
some authors have introduced changes to the matrix
dimensions in order to adjust them to their own
applications.
Table 1: Kraljic matrix (Kraljic, 1983).
Strategic impact Supply Risk
Low High
Low Non-critical Bottleneck
High Leverage Strategic
The non-critical category represents products that
are purchased frequently and are low in value;
however, they take up 80% of purchasing department
time and account for less than 20% of the purchasing
volume. The bottleneck category represents products
whose suppliers have a dominant position due to
supply shortage (Caniëls & Gelderman, 2005). The
leverage category represents products that are used
regularly and in large quantities. Finally, strategic
items represent products with a small number of
suppliers in the market and a high strategic impact
(Gelderman & Van Weele, 2003). Each category has
a set of recommended strategies that can be found in
the literature (Caniëls & Gelderman, 2005; Kraljic,
1983). In order to allow purchasers to get to know
their bargaining power better and identify an
appropriate strategy to reduce corporate risk and
increase purchasing efficiency, Kraljic (1983)
defined a set of criteria for each matrix dimension
(Ferreira et al., 2015; Kraljic, 1983). Kraljic (1983)
took the volume of purchases or the total costs into
consideration in assessing the strategic impact. In
determining supply risk, he recommended
incorporating the supply market complexity, which
includes supply shortage, technological advances,
substitute products, entry barriers, logistics costs, and
monopoly and oligopoly conditions. Montgomery et
al. (2018) assert that the Kraljic approach is the most
important diagnostic and prescriptive tool in
purchasing management. Gelderman & Van Weele
(2003) consider KPM an innovative procurement
practice.
Gelderman & Mac Donald (2008) applied the
KPM to a logistics infrastructure developed within an
oil company. Arantes et al. (2014) used the KPM in
two branches in markets with differing characteristics
in which a multinational construction company
operates and compared the results. Botes et al. (2017)
investigated mechanisms whereby the buyer-supplier
relationship enables the petrochemical industry's
resilience. These examples in the literature confirmed
the versatility of the Kraljic matrix, as it can be
applied to a wide range of areas and contexts, some
of them very distinct.
ICORES 2021 - 10th International Conference on Operations Research and Enterprise Systems
330
Accordingly, this study aims to expand the
applicability of the PPMs in the health sector by
applying the KPM to a Central Hospital (CH) in
Portugal using a simplified model (practitioner wise),
combined with an action research approach.
3 RESEARCH METHOD
This study combined Action Research (AR) with a
case study in a CH in Portugal and had the main
objective of supporting the change to a more
structured process in defining medicine purchasing
strategies for the CH, integrating supply risk and
strategic impact. Due to difficulties in medicine
purchasing, namely the perceived misalignment
between purchasing strategies and product
characteristics, the CH invited the researchers to
develop a process of establishing suitable and
practicable purchasing strategies.
The CH under study comprises six hospital units,
with the Purchasing, Logistics and Distribution
Department (PLDD) responsible for medicine
purchases for all units. In hospitals, the purchase
processes are complex, given that they deal with a set
of constraints; for this reason, they are continually
looking for new solutions (Serrou & Abouabdellah,
2016). The supply policy must meet the
organizational and patient needs (Almeida &
Lourenço, 2009). In 2017, the CH's purchases
exceeded 144 million euros, about 52% of the total
annual budget, with medicines accounting for around
46% of the volume of purchases. This figure is in line
with Medeiros & Ferreira (2013), who stated that,
generally speaking, medicines make up about 45% of
total hospital purchases.
Combining Action Research (AR) with a case
study in a CH in Portugal, this research project is
exploratory in nature. AR is used to solve existing
problems in organizations in a group decision
context, and it is centered on solving issues (Rytter,
Boer, and Koch, 2007). Kurt Lewin (1946) defines
AR as “comparative research on the conditions and
effects of various forms of social action and research
leading to social action”. Middel et al. (2006) claimed
that the use of AR models contributes to research on
collaborative and continuous improvements,
contributing both to the body of knowledge and
practitioners’ concerns.
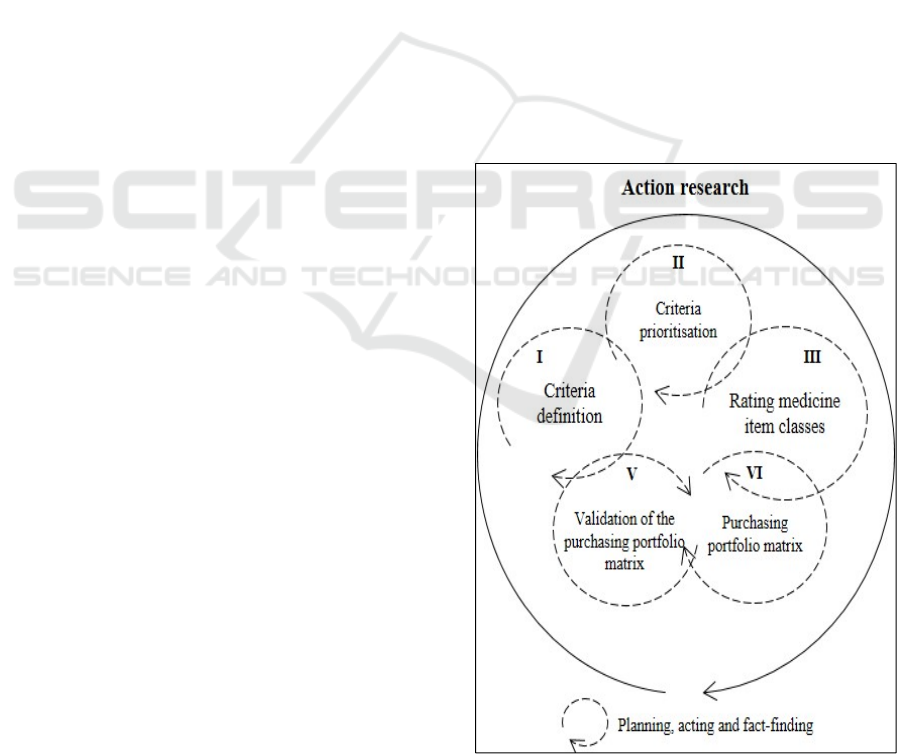
The research method presented in Figure 1, made
up of five phases, required close collaboration
between the researchers and six representatives from
the CH divided into two independent groups, Group
1 (G1) and Group 2 (G2). The utilization of two
groups allows for the consistency and validity of
results (Lee & Drake, 2010; Padhi et al., 2012):
G1 is used to define the dimension criteria (Phases
I and II);
And, G2 to apply the criteria to the products under
analysis, develop the PPM and validate it (Phases
III, IV, and V).
The research lasted for eight months, and several
group sessions were held for data collection,
development, and results validation. In the sessions,
all group members had equal weight in decision-
making processes, and the session coordinator (one of
the researchers) always endeavored to reach a
consensus. When consensus was not reached, the
final decision was by majority vote.
Finally, the list of the CH’s medicines contains
over 2000 items with different characteristics, which
was too much to be dealt with in this study. Hence, an
ABC analysis was carried out to classify medicines’
importance by purchasing cost, whereby only those in
category A were considered in this research,
accounting for 5.3% of the medicines and 80.09% of
the amount spent. Lastly, category A medicines were
grouped according to their characteristics, resulting in
22 Medicine item classes (MICs) (Table 2).
Figure 1: Research method based on AR principles (adapted
from Ferreira et al. (2015)).
Development of a Purchasing Portfolio Model for the Health Sector: A Case Study of a Central Hospital
331
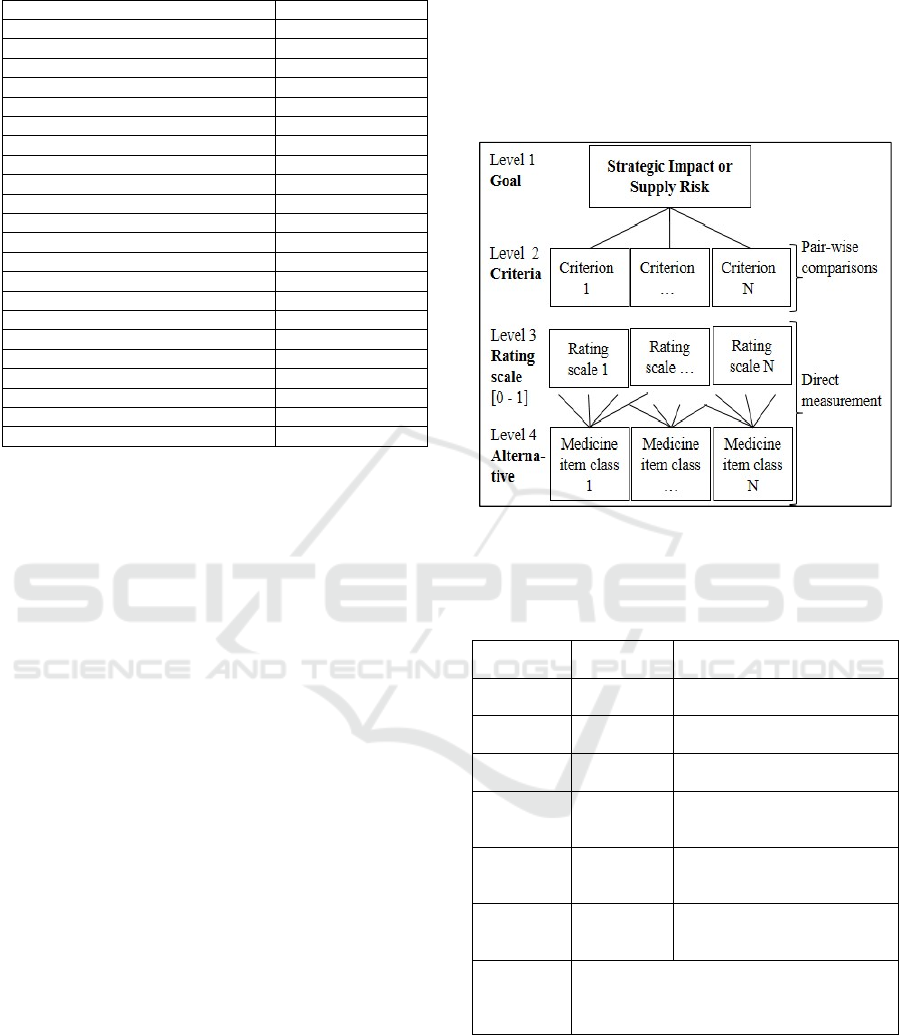
Table 2: MICs by the total annual amount spent.
Medicine item class Purchase Volume
Antivirals 29.50%
Antiretrovirals 15.13%
Immunomodulators A 14.38%
Immunomodulators B 10.45%
Hemostatics A 6.42%
Cytotoxic 3.61%
Immunoglobulins 3.28%
Enzymes 2.26%
Medicinal Gases 2.21%
Hemostatics B 1.87%
Eye disorders medicines 1.67%
Nervous system 1.65%
Antifungals 1.26%
Tyrosinacinase inhibitors 1.25%
Antibacterials 0.98%
Plasma substitutes 0.97%
Hypothalamic hormones 0.96%
Electrolyte Changes 0.80%
Intoxications antidotes 0.65%
Cardiovascular system medicines 0.25%
Breathing system medicines 0.25%
Medical ultrasound 0.19%
4 PURCHASING PORTFOLIO
MODEL
To apply the Kraljic matrix required the use of a
multiple criteria decision-making tool, which is
essential in problem-solving situations characterized
by various actors, criteria, and objectives (Kumar et al.,
2017). This tool’s main goal is to support decision-
makers, as there is usually not just one optimal solution
for problem-solving, and it’s is often necessary to
differentiate between existing solutions (Saaty, 1980).
Analytical Hierarchical Process (AHP) is a
technique that supports reducing the uncertainty in
subjective assessments (Saaty, 1980). Complex
decision-making requires the establishment of
different “trade-offs” between criteria. The decision
elements are compared with each other and weights
assigned to define the priorities in the decision-
making process (Subramanian & Ramanathan, 2012).
In this study, an AHP model with four levels is the
basis for the development of the KPM (Figure 2). At
Level 1, the goal provides the overall score of each
MIC in terms of the two dimensions of the KPM,
namely strategic impact and supply risk (chosen by
the G1 experts).
The criteria that the experts considered relevant
for measuring the strategic impact or supply risk are
located at Level 2. Level 3 contains the rating scale
for measuring each MIC in each criterion. Finally,
Level 4 includes alternative MICs. To find the
relative weight of the criteria, pair-wise comparisons
based on a “1 to 9” relative importance scale were
utilized (Table 3). To score each alternative (MIC) for
each criterion, a direct (or absolute) measurement was
chosen, which is an advantage over pair-wise
comparisons, which would require a high and
impractical number of comparisons (Bruno et al.,
2012; Drake & Lee, 2009).
Figure 2: AHP model for each KPM dimension (adapted
from Ferreira et al. (2015)).
Table 3: Pair-wise comparisons “1 to 9” scale for AHP
(adapted from Saaty (2008)).
Intensity of
importance
Definition Explanation
1
Equal
importance
Two criteria contribute equally
to the objective
3
Moderate
importance
Experience and judgment
slightly favor one over another
5
Strong
importance
Experience and judgment
strongly favor one over another
7
Very strong
importance
A criterion is strongly favored,
and its dominance is
demonstrated in practice
9
Absolute
importance
The importance of one over
another is recognized
unassailably.
2, 4, 6, 8
Intermediate
values
Used to represent a
compromise between the
priorities listed above
Reciprocals o
f
above
If criterion i has one of the above non-zero
members assigned to it when compared with
criterion j, then j has the reciprocal value when
compared with i.
4.1 Criteria Definition
The choice of the dimension criteria in PPMs was a
complicated matter. In this study, the criteria and
respective assessment scales were developed by the
G1 experts in accordance with their experience and
knowledge (stages I and II of the research method).
ICORES 2021 - 10th International Conference on Operations Research and Enterprise Systems
332
4.1.1 Strategic Impact
From criteria found in the application of KPM
available in the literature, experts selected a set of
three criteria as appropriate for classifying the
strategic impact of the MICs. Moreover, two criteria
were adjusted, and a new criterion was added
(importance of the product in the patient’s life),
considering that they must be comprehensive, non-
redundant, operational, thrifty, and independent
(Saaty, 1980).
To complete the definition of the strategic impact
criteria, the experts were requested to develop a rating
scale for each qualitative criterion (Table 4). The first
criterion chosen was the ‘purchase volume’, as a
generic criterion suggested by Kraljic (1983). The
second was ‘importance of the product in the patient’s
life,’ giving that a lack of certain medicines can
endanger patients’ lives. Finally, ‘expected growth in
demand’ allowed the experts to anticipate changes in
purchasing strategies in the long-term.
Table 4: Criteria rating scales for the Strategic Impact (SI)
dimension. (*) The final rating is presented on a 0 to 1 scale.
Criteria Rating scale
SI1 - Purchase volume
(Purchase Volume/Maximum
Purchased Volume)^2
SI2 - Expected growth in
demand (%)
1: Lower; 2; 3: Remains equal;
4; 5: Higher
SI3 - Importance of the
product in the patient’s
life (*)
1: No risk; 2; 3: Medium; 4; 5:
High risks
4.1.2 Supply Risk
For classifying the supply risk dimension, four
criteria were selected by the experts (Table 5). For the
first criterion, experts agreed that the ‘number of
suppliers’ is key, as in hospitals the trade-off between
price and quality depends on the number of potential
suppliers available on the market (Medeiros &
Ferreira, 2018). The second criterion is ‘substitute
products’ because alternative medicines, for example,
can help to solve some of the problems that managers
face daily, such as delays in delivery, damaged
products, suppliers’ stockouts. The third is ‘logistic
proximity,’ given that, for hospitals, the logistics risk
is a mix between distance and complexity if the
supply chain, which is highlighted by the fact that the
medicines purchased come from Portugal and all over
the world. Lastly, the criterion ‘transportation
requirements’ is essential, given that certain
medicines require specific packaging and conditions
during transportation.
Table 5: Criteria rating scales for the supply risk dimension.
(*) The final rating is presented on a 0 to 1 scale.
Criteria Rating scale
SR1 - Number of
suppliers
Number of suppliers^-1.1
SR2 - Substitute
products (*)
1/(n+1)
n – average number of acceptable
substitutes in the MIC
SR3 - Logistic
proximity (*)
1: Local; 2; 3: Distant or
complex; 4; 5: Distant and
complex
SR4 - Transportation
requirements (*)
1: None; 2; 3: Some complexity;
4; 5: Specific and complex
4.2 Criteria Prioritization
The next step was determining the relative weights of
each criterion, which must reflect their “importance”
in the dimensions of the PPM (Olsen & Ellram,
1997). For calculating the weights, the pair-wise
comparisons inherent in the AHP application were
carried out as a team exercise in sessions with G1.
The final results were reached by consensus (Table 6
and Table 7).
According to the results, the most important
criterion in the strategic impact dimension is the
“purchase volume,” which has a relative weight of
63.5%, as was already expected. However, in the
literature, the values found for similar criteria lie at
around 50% (Lee & Drake, 2010; Padhi et al., 2012).
Next, the second most important criterion is the
“importance of the product in the patient’s life” which
has a weight of 28.7%, reflecting hospitals’ primary
goal of ensuring efficient treatment for all their patients
by providing quality services (Medeiros & Ferreira,
2018). Lastly, the criterion “expected growth in the
demand”, which has a weight of 7.8%, is the least
important criterion. The consistency ratio (CR) for the
strategic impact criteria is 9.8%, which is acceptable,
as it is less than the threshold of 10% (Saaty, 1980).
As far as the supply risk dimension is concerned,
the “number of suppliers” is the most important
criterion, having a relative weight of 54.6%. This
figure can be explained by the high impact that the
number of suppliers has on the hospital service level,
given that the hospitals are responsible for supplying
the required products for health care activities and
treatment of the patients. In second place, experts
considered the “substitute products” criterion, which
has a 29.5% relative weight, because it is important
to have alternative medicines so that the supply of
medicines does not fail. In third place comes the
“logistic proximity” criterion with 11.3%; in last
place is the criterion “transportation requirements”,
with 4.6%. In the supply risk dimension, CR is 8.8%,
which is an acceptable value, as it is less than 10%.
Development of a Purchasing Portfolio Model for the Health Sector: A Case Study of a Central Hospital
333
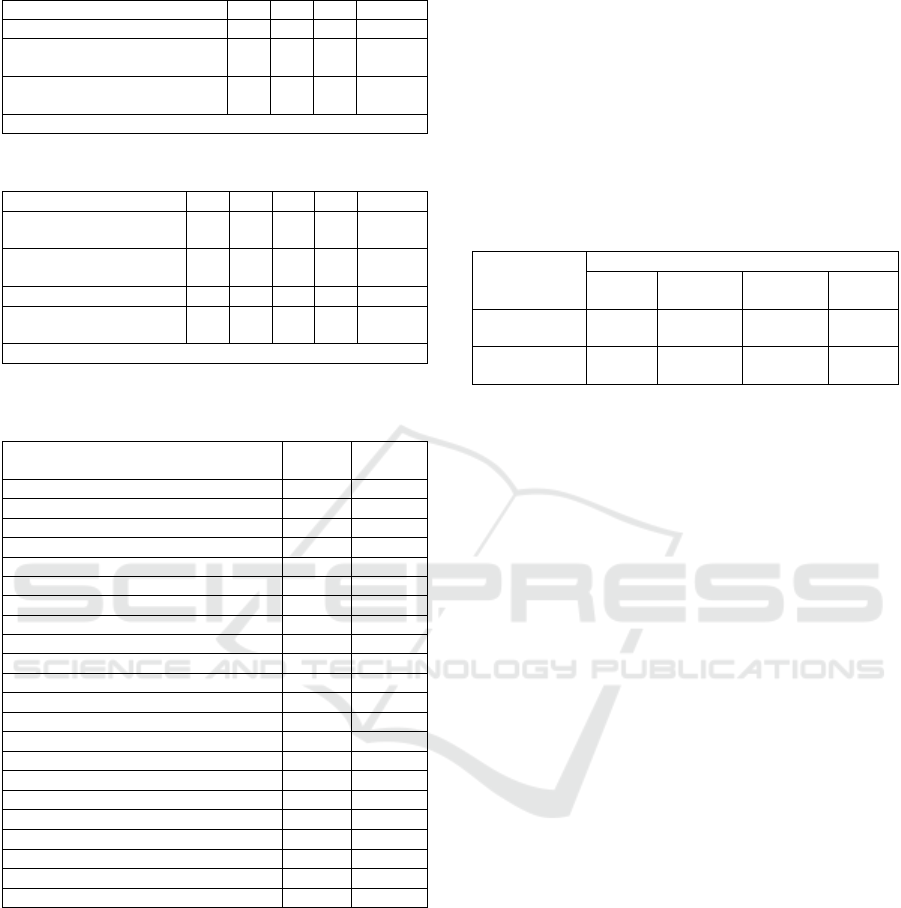
Table 6: Relative weights of the strategic impact criteria.
Criteria SI1 SI2 SI3 Weight
SI1 - Purchase volume 1 6 3 63.5%
SI2 - Expected growth in
demand
1/6 1 1/5 7.8%
SI3 - Importance of the product
in the patient’s life
1/3 5 1 28.7%
Consistency Ratio (CR) = 0.098
Table 7: Relative weights of the supply risk criteria.
Criteria SR1 SR2 SR3 SR4 Weight
SR1 - Number of
suppliers
1 3 5 7 54.6%
SR2 - Substitute
products
1/3 1
4
7 29.5%
SR3 - Logistic proximity 1/5 1/4 1 4 11.3%
SR4 - Transportation
requirements
1/7 1/7 1/4 1 4.6%
Consistency Ratio (CR) = 0.088
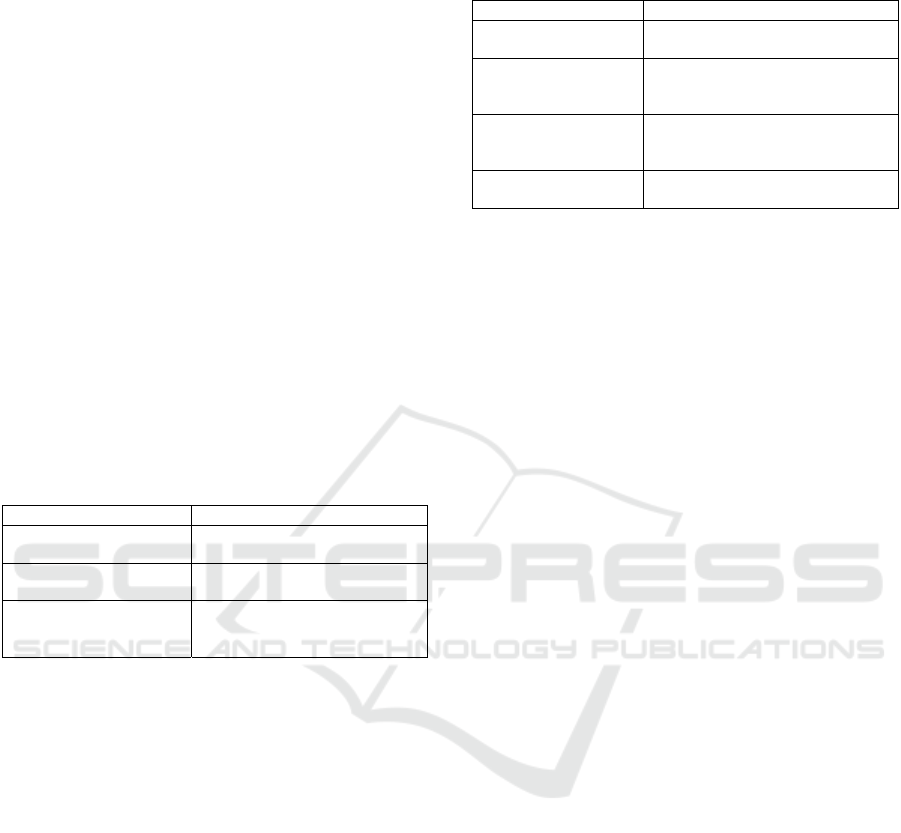
Table 8: Classification of medicines item classes according
to both matrix dimensions.
Medicine item class
Supply
risk
Strategic
impact
Antivirals 0.48 0.96
Antiretrovirals 0.10 0.51
Immunomodulators A 0.44 0.26
Immunomodulators B 0.27 0.17
Hemostatics A 0.38 0.29
Cytotoxic 0.43 0.34
Immunoglobulins 0.41 0.06
Enzymes 0.55 0.12
Medicinal Gases 0.52 0.01
Hemostatics B 0.53 0.19
Eye disorders medicines 0.70 0.01
Nervous system 0.39 0.16
Antifungals 0.52 0.05
Tyrosinacinase inhibitors 0.08 0.30
Antibacterials 0.13 0.22
Plasma substitutes 0.57 0.22
Hypothalamic hormones 0.35 0.18
Electrolytes 0.45 0.07
Intoxications antidotes 0.96 0.14
Cardiovascular system medicines 0.88 0.22
Breathing system medicines 0.96 0.18
Medical ultrasound 0.84 0.04
5 RESULTS AND DISCUSSION
Once the criteria and prioritization of the PPM’s
dimensions have been defined, the next step is to rate
all 22 MICs using the rating scales presented in
Tables 4 and 5 (stage III of the research method). For
the qualitative criteria, the experts in G2 met and used
direct measurement. When it came to the quantitative
criteria, the rating scales were used. Finally, after
accounting for the weights of the criteria defined in
the AHP model (Tables 6 and 7), the results are
presented (stage IV of the research method):
The classification of MICs according to Strategic
impact and Supply risk (Table 8);
The distribution of the purchasing amount in the
quadrants of the PPM (Table 9);
The PPM plot (Figure 3);
And, the mapping of the MICs in the quadrants of
the PPM (Figure 4).
Table 9: Distribution of the purchased amount among the
four categories.
Categories
Strategic Leverage Bottleneck
Non-
critical
No. of classes
(%of 22)
1
(4.5%)
3
(13.7%)
5
(22.7%)
13
(59.1%)
Purchasing
volume
29.5% 17.4% 3.0% 50.1%
However, at first glance the results in Figure 3
seem misleading. Distributing the MICs across the
PPM quadrants can be both challenging and
subjective. The MultiDimensional Scaling (MDS)
approach was adopted to position the MICs in the
PPM (Padhi et al., 2012). Considering the Euclidean
distances between MICs, calculated using the scores
presented in Table 8, MDS looks for possible clusters,
which contain MICs that are inter-related, and
provides a visual representation of the pattern of
proximities. This approach allowed for a clear link
between these clusters and the four purchasing
categories, as shown in Figure 4.
In the final G2 session, the experts had the
opportunity to discuss and comment on the results
presented in Figure 5 (phase V of the research
method), based on their specific and practical
expertise. They helped explain the results and
confirmed PPM’s potential, as developed for their
hospital, while also showing its general applicability
to the health sector, thus satisfying this study’s main
objective.
The non-critical category has the largest number
of MICs, accounting for 50.1% of the total purchasing
volume (Table 9). These MICs are of low supply risk,
mainly due to the existence of many suppliers and
substitute products, and a low strategic impact, given
the small purchase volumes for each MIC. Thus, for
these MICs, it is recommended that one reduce
logistical and administrative complexity through
standardization and aggregation with a view to
reducing transaction costs (Caniëls & Gelderman,
2005).
ICORES 2021 - 10th International Conference on Operations Research and Enterprise Systems
334
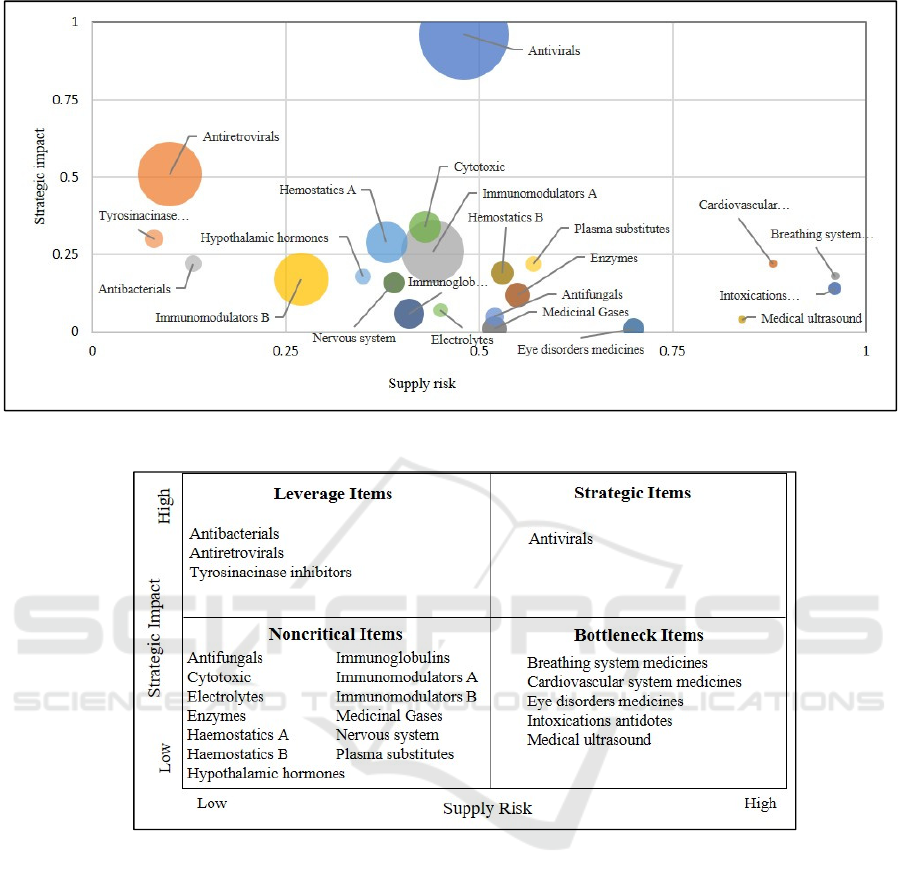
Figure 3: PPM plot (bobble proportional to the amount spent).
Figure 4: Mapping of the MICs in the quadrants of the PPM.
Despite having the second-largest number of
MICs, the bottleneck category has the lowest volume
of purchases (3%). These classes present a high
supply risk on account of the reduced number of
suppliers and the fact that there is no substitute in case
of need. They also have a low strategic impact due to
their low purchase volumes and the low impact of
growing demand on the organization. Accordingly,
the recommendation is to guarantee availability of
these medicines through larger stocks at the CH or
suppliers, the latter being preferable (Caniëls &
Gelderman, 2005).
The leverage category comprises three MICs
corresponding to 17.4% of the total purchasing
volume. These MICs are characterized by low supply
risk, which can be explained by the fact that there are
several substitute medicines and many suppliers
located in Portugal. Furthermore, the high strategic
impact of this category on the CH is due to the high
purchase volumes for the MICs. The recommendation
for the CH is to use purchasing strategies that exploit
its buying power through price negotiation, such as
competitive bidding (Lee & Drake, 2010). The
experts stated that they are already using this strategy;
however, they recognize they may not be applying it
to the right medicines.
Finally, the strategy category has only one MIC
(Antivirals) but one that has a high relative weight
(29.5%) in the total purchasing volume. This MIC has
a high strategic impact, as it presents a high
purchasing volume, demand is expected to grow in
the near future, and also represents an increased risk
Development of a Purchasing Portfolio Model for the Health Sector: A Case Study of a Central Hospital
335

in patients’ lives in cases of stockout. Furthermore,
the number of suppliers or substitute medicines is
small. Accordingly, experts recommend establishing
long-term contracts with the suppliers of this
category’s medicines based on information exchange
(at operational and strategic levels), ensuring that
there are guarantees of supply, and sharing updated
information concerning the CH’s medicines demand,
present and future.
6 CONCLUSIONS
The contribution of this study deals with the
identified research gap regarding the application of a
PPM to the health sector, particularly medicine
purchasing, and successful criteria prioritization
using the AHP technique in both dimensions of the
matrix. The purchasing process at the CH was studied
and analyzed. It was concluded that the misalignment
between the medicine’s characteristics and CH’s
purchasing strategy is one of the root causes of the
problems identified in purchasing medicines.
Furthermore, the CH’s current medicines purchasing
strategy is based only on the purchasing price
criterion. In this sense, KPM is a fundamental tool
because it considers more criteria defined according
to the CH and clients’ interests. Its application
allowed us to position the 22 item classes in the
KPM's most appropriate quadrant, permitting the CH
to develop adequate purchasing strategies. The results
show that 13 of the MICs are in the non-critical
category, representing 59.1% of the purchased
volume of medicines; the main strategy proposed to
the CH is to reduce logistical and administrative
complexity through standardization and aggregation
of medicines. With regard to the bottleneck category,
which includes five MICs and accounts for only 3%
of the purchased amount, the proposed strategy is to
guarantee medicines’ availability through having
larger stocks at the CH or, preferably, the suppliers.
Regarding the leverage category, which comprises
only three MICs but accounts for 17.4% of the
purchased volume, the proposed strategy is
competitive bidding, exploiting the CH’s buying
power. Finally, for the critical category, which only
includes one MIC but accounts for almost 30% of the
purchased volume, the recommended strategy points
to establishing long-term contracts with the suppliers
based on information exchange, at operational and
strategic levels.
This study has also shown that the combination of
AHP and MDS is a practical way of dealing with
PPM’s critical issue – its subjectivity – while keeping
it simple and usable by the CH employees. The CH
management agreed on the value of taking a
structured approach to developing purchasing
strategies in the CH, so that supply risk and strategic
impact are integrated into the purchasing decision
process. They also recognized the value of the new
approach in the process of defining purchasing
strategies for each category. They recommended its
application regularly. Nevertheless, they also agreed
that it is crucial to interpret and reflect on the results.
The construction of the PPM matrix should not be the
end of the portfolio analysis. Discussions offer more
in-depth understanding and may lead more quickly to
decisions grounded in consensus. Lastly, the CH
management agreed that the PPM facilitates strategic
talks to a large degree, taking purchasing to a strategic
level.
The main limitation of the present study is that
only one case was used, so caution must be taken
when generalizing the findings to the whole health
sector. Despite that limitation, the principal objective
of the study was achieved, having developed and
applied the purchasing portfolio model to a hospital
and simultaneously shown its value.
Lastly, by way of future work, it was suggested to
the CH management that they expand the application
of the KPM to products/services other than
medicines, so that their buyers can manage their
acquisition effectively and economically. The
development of the CH’s information systems and the
implementation of a more powerful warehouse
management system was also recommended.
ACKNOWLEDGMENTS
The authors would like to express their profound
gratitude to all Central Hospital experts for their
participation and support in developing the
Purchasing Portfolio Model.
REFERENCES
Almeida, A., & Lourenço, L. (2009). As diferenças
regionais ao nível das práticas de aprovisionamento nos
hospitais públicos portugueses. Revista Portuguesa De
Saúde Pública, 27(1), 81–94.
Arantes, A., Ferreira, L. M. D. F., & Kharlamov, A. (2014).
Application of a Purchasing Portfolio Model in a
Construction Company in Two Distinct Markets.
Journal of Management in Engineering, 30(5),
04014020. https://doi.org/10.1061/(ASCE)ME.1943-
5479.0000290
ICORES 2021 - 10th International Conference on Operations Research and Enterprise Systems
336

Botes, A., Niemann, W., & Kotzé, T. G. (2017). Buyer-
supplier collaboration and supply chain resilience: A
case study in the petrochemical industry. South African
Journal of Industrial Engineering, 28(4), 183–199.
https://doi.org/10.7166/28-4-1736
Bruno, G., Esposito, E., Genovese, A., & Passaro, R.
(2012). AHP-based approaches for supplier evaluation:
Problems and perspectives. Journal of Purchasing and
Supply Management, 18(3), 159–172.
https://doi.org/10.1016/j.pursup.2012.05.001
Caniëls, M. C. J., & Gelderman, C. J. (2005). Purchasing
strategies in the Kraljic matrix—A power and
dependence perspective. Journal of Purchasing and
Supply Management, 11(2), 141–155.
https://doi.org/https://doi.org/10.1016/j.pursup.2005.1
0.004
Drake, P. R., & Lee, D. M. (2009). Component
prioritisation for strategic purchasing and the case study
of a South Korean elevator manufacturer. International
Journal of Advanced Manufacturing Technology, 43(9–
10), 883–895. https://doi.org/10.1007/s00170-008-
1766-0
Ferreira, L. M. D. F., Arantes, A., & Kharlamov, A. (2015).
Development of a purchasing portfolio model for the
construction industry: an empirical study. Production
Planning & Control, 26(5), 377–392.
https://doi.org/10.1080/09537287.2014.906679
Gelderman, C. J. (2003). A Portfolio Approach to the
Development of Differentiated Purchasing Strategies.
https://doi.org/10.6100/IR569453
Gelderman, C. J., & Mac Donald, D. R. (2008). Application
of Kraljic’s purchasing portfolio matrix in an
undeveloped logistics infrastructure: The staatsolie
suriname case. Journal of Transnational Management,
13(1), 77–92.
https://doi.org/10.1080/15475770802059610
Gelderman, C. J., & Van Weele, A. J. (2003). Handling
measurement issues and strategic directions in Kraljic’s
purchasing portfolio model. Journal of Purchasing and
Supply Management, 9(5–6), 207–216.
https://doi.org/10.1016/j.pursup.2003.07.001
Kraljic, P. (1983). Purchasing must become supply
management. Harvard Business Review, September-
(83509), 109–117. https://doi.org/10.1225/83509
Kumar, A., Sah, B., Singh, A. R., Deng, Y., He, X., Kumar,
P., & Bansal, R. C. (2017). A review of multi criteria
decision making (MCDM) towards sustainable
renewable energy development. Renewable and
Sustainable Energy Reviews, 69(October 2016), 596–
609. https://doi.org/10.1016/j.rser.2016.11.191
Lee, D. M., & Drake, P. R. (2010). A portfolio model for
component purchasing strategy and the case study of
two South Korean elevator manufacturers.
International Journal of Production Research, 48(22),
6651–6682.
https://doi.org/10.1080/00207540902897780
Lewin, K. (1946). Action Research and Minority Problems.
Journal of Social Issues, 2(4), 34–46.
https://doi.org/10.1111/j.1540-4560.1946.tb02295.x
Medeiros, M., & Ferreira, L. (2018). Development of a
purchasing portfolio model: An empirical study in a
Brazilian hospital. Production Planning and Control,
29(7), 571–585.
https://doi.org/10.1080/09537287.2018.1434912
Middel, R., Coghlan, D., Coughlan, P., Brennan, L., &
McNichols, T. (2006). Action research in collaborative
improvement. International Journal of Technology
Management, 33(1), 67–91.
https://doi.org/10.1504/IJTM.2006.008192
Ministério da Saúde. (2018). Retrato da Saúde 2018,
Portugal.
Montgomery, R. T., Ogden, J. A., & Boehmke, B. C.
(2018). A quantified Kraljic Portfolio Matrix: Using
decision analysis for strategic purchasing. Journal of
Purchasing and Supply Management, 24(3), 192–203.
https://doi.org/10.1016/j.pursup.2017.10.002
Olsen, R. F., & Ellram, L. M. (1997). A portfolio approach
to supplier relationships. Industrial Marketing
Management, 26(2), 101–113.
https://doi.org/10.1016/S0019-8501(96)00089-2
Padhi, S. S., Wagner, S. M., & Aggarwal, V. (2012).
Positioning of commodities using the Kraljic Portfolio
Matrix. Journal of Purchasing and Supply
Management, 18(1), 1–8.
https://doi.org/10.1016/j.pursup.2011.10.001
Pardo, C., Missirilian, O., Portier, P., & Salle, R. (2011).
Barriers to the “key supplierization” of the firm.
Industrial Marketing Management, 40(6), 853–861.
https://doi.org/10.1016/j.indmarman.2011.06.029
Rytter, N. G., Boer, H., & Koch, C. (2007).
Conceptualizing operations strategy processes.
International Journal of Operations and Production
Management, 27(10), 1093–1114.
https://doi.org/10.1108/01443570710820648
Saaty, T. L. (1980). The Analytic Hierarchy Process:
Planning, Priority Setting, Resource Allocation
(Decision Making Series). 287.
Serrou, D., & Abouabdellah, A. (2016). Logistics in the
hospital: Methodology for measuring performance.
ARPN Journal of Engineering and Applied Sciences,
11(5), 2950–2956.
Subramanian, N., & Ramanathan, R. (2012). A review of
applications of Analytic Hierarchy Process in
operations management. International Journal of
Production Economics, 138(2), 215–241.
https://doi.org/10.1016/j.ijpe.2012.03.036
Uthayakumar, R., & Priyan, S. (2013). Pharmaceutical
supply chain and inventory management strategies:
Optimization for a pharmaceutical company and a
hospital. Operations Research for Health Care, 2(3),
52–64. https://doi.org/10.1016/j.orhc.2013.08.001
Development of a Purchasing Portfolio Model for the Health Sector: A Case Study of a Central Hospital
337
