
A Model of Cost and Time-Effective Disease Screening for
Non-Communicable Diseases in India
Nibras K. Thodika
1a
, Srujan Janagam
2
, Smitha Thomas Kaniyampady
2
, Arkalgud Ramaprasad
1,3 b
,
Anupama Shetty
2
and Chetan Singai
1,4 c
1
Ramaiah Public Policy Center, Bengaluru, India
2
Narayana Health, Bengaluru, India
3
University of Illinois, Chicago, U.S.A.
4
Ramaiah University of Applied Sciences, Bengaluru, India
{srujan.janagam, smithathomas.kaniyampady, anupama.s.dr}@narayanahealth.org
Keywords: Non-Communicable Disease Screening, Mobile Health Technologies, Point-of-Care Technologies.
Abstract: Background: India has the largest burden of the NCDs globally. Screening and identification of clusters with
the common risk factors are crucial for early detection, prevention, and control at both individual and
population levels. Objective: This study documents a model of cost and time-effective disease screening for
NCDs. The model uses a combination of mobile health clinics-based point-of-care diagnostic technologies.
The model, for its easy-to-use, cost and time effective operation, should be scalable as a tool for community-
based disease screening and population level NCD surveillance. Method: The study documents the materials
and processes of NCD screening camps conducted in Bangalore, India. A time and motion study analysis and
cost analysis were undertaken to establish the time and cost effectiveness. Results & Discussion: The Study
found out a baseline time and cost components for a camp based NCD screening strategy using the mHealth
tools and mobile health facilities. This reinforces the potentials of integration of the NCD screening into the
public primary health care centres for effective scaling up and achievement of surveillance as well as
monitoring and evaluation of the NCD prevention and control programs in the country.
1 INTRODUCTION
This paper presents a model for population-based
screening for non-communicable diseases (NCD) in
India based on a combination of mobile health
clinics-based point-of-care diagnostic technologies
and mHealth applications. It describes the context of
NCD in India, the technology used in screening
camps, the data from the camps, a framework to
conceptualize the application, and conclusion about
generalizing the model.
1.1 Non-Communicable Disease
Burden and Response in India
The demographic transition in the low- and middle-
income countries has been accompanied by
a
https://orcid.org/0000-0001-9115-6382
b
https://orcid.org/0000-0003-1551-6854
c
https://orcid.org/0000-0002-7037-6033
increasing health risks in the form of NCD burden
(OMS, 2011; Shah & Mathur, 2010). Majority of the
low and middle-income countries have devoted
considerable attention to communicable diseases as
against NCDs. This is increasing the burden on their
health care systems and ultimately on the quality of
life in these countries (Kroll et al., 2015). India has
the largest burden of NCDs globally (Menon et al.,
2014). The disease burden is expected to worsen due
to the rapid urbanization, accompanying lifestyle
changes, and inadequacy in health system
preparedness (Prakash Upadhyay, 2012). The disease
burden in the country also poses the need for scalable
and affordable methods for NCD prevention and
control that can be expanded into the remote and rural
parts of the country. The National Programme for
Prevention and Control of Cancer, Diabetes,
Cardiovascular Diseases and Stroke (NPCDCS) was
312
Thodika, N., Janagam, S., Kaniyampady, S., Ramaprasad, A., Shetty, A. and Singai, C.
A Model of Cost and Time-Effective Disease Screening for Non-Communicable Diseases in India.
DOI: 10.5220/0010202103120319
In Proceedings of the 14th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2021) - Volume 5: HEALTHINF, pages 312-319
ISBN: 978-989-758-490-9
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

launched by the government to combat the risk
through strategies such as surveillance, early
diagnosis, and universal availability of treatment at
primary, secondary and tertiary levels of health
facilities (Ministry of Health and Family Welfare,
Government of India, 2017). Population-based
screening as part of comprehensive primary health
care has been recommended for the strategic
management of the disease. However, in contexts
such as India, it has been difficult to implement such
measures in a sustainable way.
1.2 Prevention and Control of NCDs
through Surveillance
NCDs have multiple causes, the combined effects
from which lead to a disease rate in the population.
Estimates from habit and risk factors are needed to
plan public health interventions and clinical
programmes (Kontis et al., 2014). It has been
identified that interventions to prevent and treat
NCDs at the earlier stages are cost-effective (Ministry
of Health and Family Welfare, Government of India,
2017). Integrating the NCD screening and diagnosis
at existing primary healthcare centres has been
suggested (World Health Organization, 2010).
However, operational issues persist in terms of
implementing population-level screening, especially
in resource-limited settings (Deepa et al., 2011). This
requires scalable and cost-effective models of
population-based screening of NCDs in various
regions in the country with divergent ground-realities.
Screening and identification of clusters with common
risk factors are crucial for early detection, prevention,
and control at both individual and population levels
(Ahmed et al., 2009) to reduce morbidity and
mortality. Innovative methods using cutting-edge
technologies to enhance screening capabilities have
been on the rise. They include non-laboratory-based
diagnostics, point-of-care technologies, mobile health
clinics. and mHealth applications in the pursuit of
achieving access and scale-ups (Bertoncello et al.,
2020; Gaziano et al., 2008; Malcolm et al., 2019;
Pandya Ankur et al., 2014). Apart from their
screening capabilities, the methods are considered
effective vehicles for information and awareness-
raising strategies as well (Bertoncello et al., 2020).
However, challenges persist on the field in terms of
their cost-effectiveness and broadening access to
them. This demands scalable methods that consider
issues of cost-effectiveness, access, and scalability
(Subramanian et al., 2018) and can be
institutionalized as part of the public health care
systems.
1.3 Objective
This study documents a camp-based population
screening model tested for NCD surveillance in India.
The model is a combination of mobile health clinics-
based point-of-care diagnostic technologies and
mHealth applications. The model ensures cost
effective NCD screening. For its easy-to-use, cost and
time effective operation, the model should be scalable
as a tool for community-based disease screening and
population level NCD surveillance using community
health resources. Integrating this into the public
health care systems should provide individual and
population level insights on NCD risk factors on a
routine basis at primary care centres. In this respect,
the study will set the baselines regarding the
materials, tools, and human and financial resources
incurred for the same. It will also compare them with
the existing standards available and contribute to
improving the existing NCD prevention and control
strategies.
2 METHODS AND MATERIALS
The study will describe the method and materials
utilized during the population-based NCD screening
camps conducted in Bengaluru, India. Using the time
and cost related data from the mobile health camps, it
will undertake time and motion study and cost
effectiveness analysis to understand and analyse the
uniqueness of the model, explore the scope for future
improvements, and provide learning for existing
practices.
2.1 NCD Screening Camps
The NCD screening camps were conducted in the city
of Bengaluru, Karnataka, India as part of the
Harnessing Oncological Preventive and Early
detection services (HOPE) program. The HOPE
program, as a population-based opportunistic
screening program for underserved populations,
aspires to improve awareness of oral and breast
cancer, initiating early detection through appropriate
technologies, and creating a continuum of follow-up,
further investigations, and curative services for
relevant cases. The program recognises the need for
lifestyle modification and behaviour change to
manage NCDs. It therefore focuses on creating and
spreading awareness about oral cancer, breast cancer,
and other NCDs amongst the general population.
Taking into consideration the shortage of health care
human resource in the country, all the devices and
A Model of Cost and Time-Effective Disease Screening for Non-Communicable Diseases in India
313

software taken on are simple. The screening is
conducted by a trained staff who do not necessarily
have to be from a medical/paramedical background.
The staff are trained on use of point-of-care devices,
mHealth technologies, interpretation of results, and
basic counselling of respondents.
The program aims to reach semi-urban and rural
populations as well as low income groups who would
not have access to routine screening and diagnosis for
NCDs. This is achieved through a screening
procedure that includes NCD screening (blood
pressure, SPo2, blood sugar, body mass index,
Haemoglobin, and vision testing), along with the
one-on-one counselling at the end of the screening
process, as well as scheduled periodic follow-up with
identified high-risk cases. A mobile Mammography
Bus is part of the screening camps conducted across
urban and rural regions in the state of Karnataka,
India (including Bengaluru). It makes use of software
applications with integrated medical devices,
available on offline basis to enable capture of clinical
data, data management, remote monitoring, and
evaluation of data. Using systematic documentation,
training, and special referral protocols, dedicated
follow up of cases is done by a separate team that
helps track cases across locations. In the long run, it
aims at training frontline healthcare workers from the
public sector. Also, creating awareness of risk factors
is emphasised in all the screening camps. Apart from
screening camps, the awareness sessions are also
conducted in schools and colleges. It has been
conducted in various settings such as factories,
educational institutions, and community living
spaces.
The list of activities undertaken during the camps
are as follows in their respective order:
Registration/Consent form filling, height and weight
measurement, MAC/Hip/Waist measurement, Pulse-
Oximeter reading, six-lead ECG, Blood pressure, HB
and blood sugar test, vision test, and explanation of
results with reference scale to the beneficiary.
The data collected using the model are
demographic, medical history, community risk
assessment, physical and behavioural risk factors,
habit history and physical measurements following
the WHO STEP guidelines(NCDs | STEPS Manual,
2002.).
2.2 Materials and Resources
The device kit being used by the trained staff (Figure
1) includes the following devices:
• 6 lead ECG: Used to collect the 15 secs ECG
record which is then interpreted using the
Artificial Intelligence tools based on the
Glasgow algorithm
• Digital BP Device: Used to collect Blood
pressure reading. It operates on
oscillometric method with options for
manual reading as well
• Glucometer: Used for measuring blood
glucose level, either random or fasting. A
single drop of blood needs to be drawn from
the individual by means of a small prick on
their finger
• Haemoglobinometer: used to measure the
hemoglobin level, also measured from a
drop of blood
• Digital stadiometer: used to measure height
• Digital weighing scale: used to measure
weight
• Tablet loaded with NCD screening software
application: for data entry purposes and inference
of results.
Figure 1: Device kit used for Screening.
All devices in the kit have been approved by
standards control bodies. The methodology of
operating the device and interpreting results is
straightforward and undemanding. The output from
the software application is colour-coded enabling the
healthcare worker to easily make an inference.
The data collected through the application can be
broadly classified into the following groups:
1. Socio-demographic details: for following up
and monitoring the program
2. Past Medical History: to identify newly
detected cases, understand management of
existing cases
HEALTHINF 2021 - 14th International Conference on Health Informatics
314
3. Community based risk assessment: risk
profiling is conducted in line with the
protocol adopted by the National Health
Mission
4. Habit History: behavioural aspects and risk
factors known to directly impact onset of
NCDs
5. Vital Parameters: to understand the current
health status of the beneficiary
More than sixty-five variables are collected. The
number of variables is higher for women as breast and
cervical cancer screening are also done.
The screening process involves history taking,
risk assessment, performing tests and counselling
based on the results. The data collected using a
mobile application are stored in a local mobile
database. When the internet is available this local
database is pushed to the server database using
application interfaces. The data is populated from the
server database to the dashboard using the Angular
and Java programming languages.
Taking into consideration the large number of data
variables collected and tests performed, it is
necessary to optimise the process workflow to ensure
that quantity was increased without denting the
quality. A time and motion study was undertaken for
this purpose.
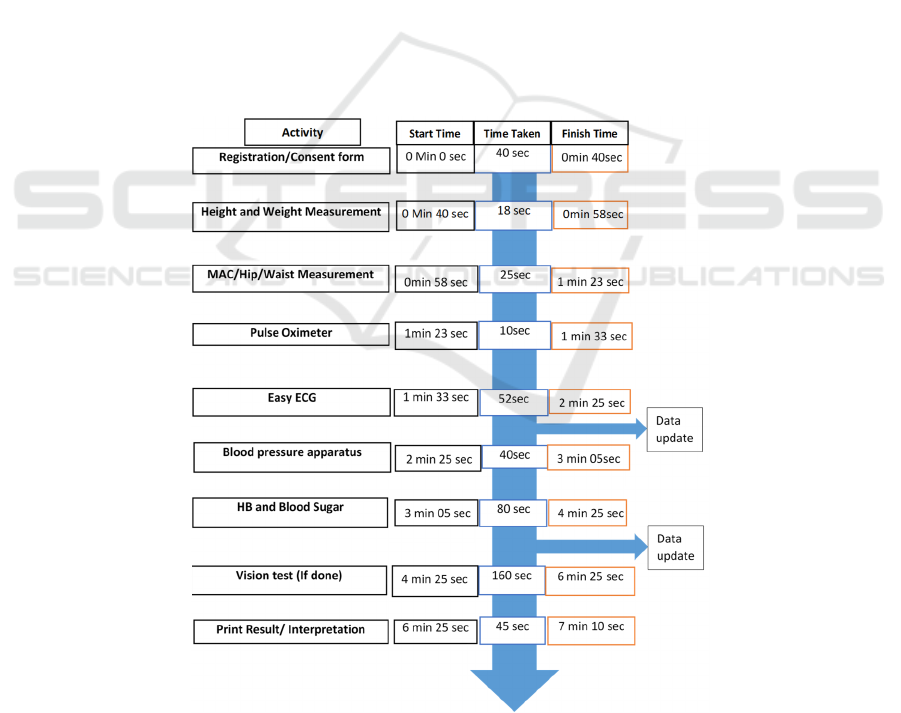
2.3 Time and Motion Analysis
The time and motion study intends to set a baseline
that can be used for future application of the presented
model on a larger scale. The analysis used data from
the screening camps conducted in 3 NCD mobile
camps conducted in Bengaluru, India. Data from the
screening of a total of 70 individuals are considered.
The data was recorded by observing the time taken
for each designated activity individually. The
activities are scheduled according to the order of data
to be entered in the mobile application being used for
documentation. The study analysed two person-
device kits combinations. (i) 2 resource persons and 2
kits, as well as (ii) 3 resource persons and 2 kits. The
process chart along with observed timings using the
second combination has been illustrated in Figure 2.
The differences in the outcomes are explained in the
results of time and motion analysis.
Figure 2: Time and Motion Study Results.
A Model of Cost and Time-Effective Disease Screening for Non-Communicable Diseases in India
315
2.4 Cost Analysis
The overall cost incurred for the screening program
was recorded. The average screening cost was
derived using the average number of screening that
could be done in a month, considering the time
observed in the study. Costs incurred for human
resources payments and other consumable resources
have been factored for calculating total costs.
3 RESULTS
3.1 Time and Motion
The results of the time and motion study are
illustrated in Table 1. It details the activity-wise
duration for screening process, parallel activities if
any, and the number of personnel involved at each
step. The total duration of each screening activity was
found to be 430 seconds. When the tolerance time of
45 seconds is added the total screening, time is 475
seconds i.e. 8 minutes approximately. This is
including the vision screening, without which the
duration taken was 5 minutes 56 seconds for one
screening using one kit. 10 screenings can be done
using one kit; hence two kits can do up to 20
screening in the specified time frame. The results
were achieved when 3 personnel were involved in the
screening. When compared with the combination of
two kits and two personnel, the results also showed
that optimal time utilization was achieved when 3
personnel and 2 kits were used for the screening.
Thus, the latter combination is considered for further
analysis.
3.2 Cost
The NCD screening model is a minimalistic, low
resource model. The operational expenditure of the
model comes down to the human resource cost of the
team (Rs. 48000/Month and Rs.16/screening) and the
consumables required for conducting the tests
(Rs.34/screening) namely, cotton swabs, needles for
pricking, blood glucose and haemoglobin testing
strips to mention a few. This model relies on other
stakeholders, such as the community partner or
organising partner, to bear the cost of transport.
Therefore, the latter costs have not been factored.
The optimal performance of a team of 3 members
would be to conduct 20 camps a month screening at
least 150 people at each camp. The cost for screening
per person would be Rs. 50 (0.68 USD). This includes
follow up of high-risk cases at least 3 times.
Table 1: Results of Time and Motion Study Personnel-Wise.
Session Sl. No Activity Duration Parallel Activity Personnel In
Wor
k
1
Step-1 Registration/Consent for
m
40sec
1
Step-2 Hei
g
ht and Wei
g
h
t
Measuremen
t
18sec
Step-3 MAC/Hip/Waist Measuremen
t
25sec
Total Time For 1
s
t
staff 1 min 23sec
2
Step-4 Pulse Oximete
r
10 secs
2
Step-5 Easy ECG 52 secs Details to be
updated in Tablet
(1-min)
Step-6 Blood pressure apparatus 40 secs
Total time for 2
n
d
staff 1 min 42 sec
3
Step-7 HB and Blood Suga
r
1 min 20 sec
(80 sec)
Details updated
in Tablet
(30sec)
3
Step-8 Vision test (If done) 2 mins
Step-9 Print Results + Explanation
with reference scale
45 secs
Total time for 3
r
d
Staff 4 min
Total Duration
430 Seconds (7
Minutes 16
seconds)
HEALTHINF 2021 - 14th International Conference on Health Informatics
316

4 DISCUSSION
This study documents a camp-based population
screening strategy for NCD risk factors. The cost,
time, and human resource factors involved in the
model were documented and analysed. These factors
are critical for wide-scale operational feasibility of
the disease screening and thus have implications in
addressing the disease surveillance for NCDs in the
country.
The study documents a baseline for the resource
requirements for the population-level NCD screening
for risk factor assessment. It identifies its uniqueness
in terms of non-requirement of the medical
professionals for screening. Trained community
workers or volunteers can contribute to the human
resource requirements in the model which throws
open possibilities of operationalizing routine
screening in resource constrained conditions. This is
achieved through the utilization of a combination of
point-of-care and mHealth technologies woven
together into an efficient process.
While the study could not compare the cost with
existing standards in the Indian context due to the
non-availability of data (apart from Amarchand et al.
2015 which identified below 1 USD per-screening
without collecting blood pressure and sugar levels), it
provides a baseline for research and
operationalization of the screening activities on
similar lines. The study found out the costs for human
resources and consumables are below 1 USD.
International comparisons are consumer side
payments which has been documented as 4 USD in
Kenya (Subramanian et al., 2018) and as 3.95 USD
per person identified when an all-inclusive NCD
screening was integrated into existing HIV screening
in South Africa (Golovaty et al., 2018).
The cost analysis in the study only considered the
human resources and other consumable costs only
since the other costs for the presented model were
provided by the community. The study thus, was not
able to account for the other costs, especially
infrastructure and other fixed costs. However, the
model presented collects a lot of important data
including the blood pressure, blood glucose level and
ECG etc. and should provide a solid baseline for
wide-scale operationalization.
Also, the time taken for the disease diagnosis and
screening has a significant impact on the behavioural
trends of the patient population especially in the
context of low- and middle-income countries such as
India. Time taken for Out-Patient Department (OPD)
and their impact on the health seeking behaviour has
been studied. It was found out that the longer waiting
time and affordability significantly impact the health
seeking behaviour among the target population.
Lower waiting times at OPDs for instance, results in
higher satisfaction rate among patients (Aswar et al.,
2014). The time motion study results provided show
the very little time required for the screening.
Monitoring and evaluation of the NCD
interventions are crucial for learning and
improvement. Evolving sustainable systems for
surveillance aligned to the national health programs
is one of the way forward (Krishnan et al., 2011). In
this context, integrated disease surveillance has
become crucial in deciding and planning strategies for
NCDs especially in the wake of Covid-19 (Mathur &
Rangamani, 2020) which has exacerbated the
vulnerabilities due to NCD risk factors (Gopalan &
Misra, 2020). The need for implementation and
operational research on the disease screening has
become ever more critical.
Figure 3: Ontological framework of the NCD screening model.
Functions Data Setting Instruments Resources Outcome
Identification Determinants Individual Questionnaire Tools/Devices Efficient
Collection Socio‐Economic Household ClinicalExamination mHealth Affordable
Curation Income Community BiochemicalTests ImagingTechnology Effective
Analysis Urban/Rural Institutional GIS Accessible
Interpretation Demographic Services
Application Age EHR
Feedback Gender SMS
Literacy SocialMedia
RiskFactors Models
Physical HealthCareCenter
Behavioral MobileHealthClinics
Biochemical PointofCare
HumanResources
CommunityHealthWorkers
Volunteers
[informationfrom
]
[of]
[NCDSurveillance]
[using]
[for]
[settingthrough]
A Model of Cost and Time-Effective Disease Screening for Non-Communicable Diseases in India
317

As such, the documented model along with its
baseline figures regarding the operational details
could be useful for the integration of the monitoring
and evaluation of NCD programs with the primary,
secondary, and tertiary health care centres especially
in the rural areas. It has been found that integrating
the NCD screening and awareness components into
the existing primary health care system is the way
forward for its cost-effectiveness (Amarchand et al.,
2015). The WHO PEN recommends using the
technology supported solutions for scaling up of
disease screening for risk factors using person-
oriented risk factor screening(World Health
Organization, 2010).
Modelling future disease trends is a useful tool for
policymakers so that they can allocate resources
effectively and implement policies to prevent NCDs.
Future research will allow real policy interventions to
be tested; however, better surveillance data on NCDs
and their risk factors are essential for research and
policy (Webber et al., 2014). The screening process
facilitates collection of data that can be deployed for
modelling and risk prediction.
We frame the overall assessment of the model
presented by the paper in the form of an ontological
framework in Figure 3. It lists the dimensions and
elements of the aspired NCD screening strategy. The
assessed model undertakes functions of collection,
interpretation, application, and feedback on a real-
time basis and collects data pertaining to all elements
in the Data dimension of the framework which is
based on the WHO STEP Manual. In terms of Setting,
while the model was tested in institutional settings it
can be scaled up into other settings as well. It used all
the instruments listed including questionnaires,
clinical examination and biochemical tests using
mHealth devices, Point-Of-Care Technologies. While
the model has proved to be efficient and affordable in
terms of time and cost, other aspects of the outcomes
needs to be further researched.
While the lack of extensive comparative analysis
and the resulting inability to provide uniform
baselines are limitations, the study provides insights
into the operational issues of NCD risk factor
surveillance. It adds evidence regarding the scope for
integrating screening into the existing public health
system for routine and informed decision making.
5 CONCLUSIONS
This paper systematically documents the NCD
screening process followed by a population-based
screening program. It sets an operational baseline in
terms of the cost and time for the camp-based
population NCD screening. The process was analysed
for their uniqueness in terms of time and cost
effectiveness in the context of their scalability and
applicability for large scale NCD surveillance in low-
and middle-income countries. The analysis and
discussion have been framed in the form of an
ontology which illustrates the existing and future
potentials of the surveillance models in the NCD
scenario.
ACKNOWLEDGEMENTS
Authors acknowledge the contribution of Mr.
Harikrishnan S in the undertaking of the time and
motion study used in this paper.
REFERENCES
Ahmed, S. M., Hadi, A., Razzaque, A., Ashraf, A., Juvekar,
S., Ng, N., Kanungsukkasem, U., Soonthornthada, K.,
Minh, H. V., & Bich, T. H. (2009). Clustering of
chronic non-communicable disease risk factors among
selected Asian populations: Levels and determinants.
Global Health Action, 2(s4), 1986.
https://doi.org/10.3402/gha.v2i0.1986
Amarchand, R., Krishnan, A., Saraf, D., Mathur, P., Shukla,
D., & Nath, L. (2015). Lessons for addressing
noncommunicable diseases within a primary health-
care system from the Ballabgarh project, India. WHO
South-East Asia Journal of Public Health, 4(2), 130.
https://doi.org/10.4103/2224-3151.206682
Aswar, N. R., Kale, K. M., Rewatkar, M. P., Jain, A. A., &
Barure, B. S. (2014). Patients Waiting Time and their
Satisfaction of Health Care Services Provided at
Outpatient Department of Government Medical
College, Nanded Maharashtra-India. International
Journal of Contemporary Medicine, 2(2), 72.
https://doi.org/10.5958/2321-1032.2014.01031.6
Bertoncello, C., Cocchio, S., Fonzo, M., Bennici, S. E.,
Russo, F., & Putoto, G. (2020). The potential of mobile
health clinics in chronic disease prevention and health
promotion in universal healthcare systems. An on-field
experiment. International Journal for Equity in Health,
19(1), 59. https://doi.org/10.1186/s12939-020-01174-8
Deepa, M., Pradeepa, R., Anjana, R., & Mohan, V. (2011).
Noncommunicable Diseases Risk Factor Surveillance:
Experience and Challenge from India. Indian Journal
of Community Medicine : Official Publication of Indian
Association of Preventive & Social Medicine,
36(Suppl1), S50–S56. https://doi.org/10.4103/0970-
0218.94709
Gaziano, T. A., Young, C. R., Fitzmaurice, G., Atwood, S.,
& Gaziano, J. M. (2008). Laboratory-based versus non-
laboratory-based method for assessment of
HEALTHINF 2021 - 14th International Conference on Health Informatics
318

cardiovascular disease risk: The NHANES I Follow-up
Study cohort. The Lancet, 371(9616), 923–931.
https://doi.org/10.1016/S0140-6736(08)60418-3
Golovaty, I., Sharma, M., Van Heerden, A., van Rooyen,
H., Baeten, J. M., Celum, C., & Barnabas, R. V. (2018).
Cost of Integrating Noncommunicable Disease
Screening Into Home-Based HIV Testing and
Counseling in South Africa: JAIDS Journal of Acquired
Immune Deficiency Syndromes, 78(5), 522–526.
https://doi.org/10.1097/QAI.0000000000001713
Gopalan, H. S., & Misra, A. (2020). COVID-19 pandemic
and challenges for socio-economic issues, healthcare
and National Health Programs in India. Diabetes &
Metabolic Syndrome: Clinical Research & Reviews,
14(5), 757–759.
https://doi.org/10.1016/j.dsx.2020.05.041
Kontis, V., Mathers, C. D., Rehm, J., Stevens, G. A., Shield,
K. D., Bonita, R., Riley, L. M., Poznyak, V.,
Beaglehole, R., & Ezzati, M. (2014). Contribution of
six risk factors to achieving the 25×25 non-
communicable disease mortality reduction target: A
modelling study. The Lancet, 384(9941), 427–437.
https://doi.org/10.1016/S0140-6736(14)60616-4
Krishnan, A., Gupta, V., Ritvik, Nongkynrih, B., & Thakur,
J. (2011). How to Effectively Monitor and Evaluate
NCD Programmes in India. Indian Journal of
Community Medicine : Official Publication of Indian
Association of Preventive & Social Medicine,
36(Suppl1), S57–S62. https://doi.org/10.4103/0970-
0218.94710
Kroll, M., Phalkey, R. K., & Kraas, F. (2015). Challenges
to the surveillance of non-communicable diseases – a
review of selected approaches. BMC Public Health,
15(1), 1243. https://doi.org/10.1186/s12889-015-2570-
z
Malcolm, S., Cadet, J., Crompton, L., & DeGennaro, V.
(2019). A model for point of care testing for non-
communicable disease diagnosis in resource-limited
countries. Global Health, Epidemiology and Genomics,
4. https://doi.org/10.1017/gheg.2019.6
Mathur, P., & Rangamani, S. (2020). COVID-19 and
noncommunicable diseases: Identifying research
priorities to strengthen public health response.
International Journal of Noncommunicable Diseases,
5(2), 76. https://doi.org/10.4103/jncd.jncd_33_20
Menon, J., Joseph, J., Thachil, A., Attacheril, T. V., &
Banerjee, A. (2014). Surveillance of
Noncommunicable Diseases by Community Health
Workers in Kerala: The Epidemiology of
Noncommunicable Diseases in Rural Areas (ENDIRA)
Study. Global Heart, 9(4), 409–417.
https://doi.org/10.1016/j.gheart.2014.07.003
Ministry of Health and Family Welfare, Government of
India. (2017, July 13). Cardiovascular, Respiratory,
and Related Disorders: Key Messages on Essential
Interventions to Address its Burden in Low-and Middle-
Income Countries | DCP3
. National Programme for
Prevention and Control of Cancer, Diabetes,
Cardiovascular Diseases and Stroke (NPCDCS).
http://dcp-3.org/chapter/2306/overview
NCDs | STEPS Manual. (2002). WHO; World Health
Organization. Retrieved April 10, 2020, from
http://www.who.int/ncds/surveillance/steps/manual/en
/
OMS. (2011). Global status report on noncommunicable
diseases 2010. OMS (Organizacion Mundial de la
Salud).
Pandya Ankur, Weinstein Milton C., Salomon Joshua A.,
Cutler David, & Gaziano Thomas A. (2014). Who
Needs Laboratories and Who Needs Statins?
Circulation: Cardiovascular Quality and Outcomes,
7(1), 25–32.
https://doi.org/10.1161/CIRCOUTCOMES.113.00039
7
Prakash Upadhyay, R. (2012). An overview of the burden
of non- communicable diseases in India. Iranian
Journal of Public Health, 41(3), 1–8. Scopus.
Shah, B., & Mathur, P. (2010). Surveillance of
cardiovascular disease risk factors in India: The need &
scope. The Indian Journal of Medical Research, 132(5),
634–642. https://doi.org/10.4103/0971-5916.73420
Subramanian, S., Gakunga, R., Kibachio, J., Gathecha, G.,
Edwards, P., Ogola, E., Yonga, G., Busakhala, N.,
Munyoro, E., Chakaya, J., Ngugi, N., Mwangi, N., Von
Rege, D., Wangari, L.-M., Wata, D., Makori, R.,
Mwangi, J., Mwanda, W., & on behalf of the East
African Economics and Implementation Group
(EAEIG). (2018). Cost and affordability of non-
communicable disease screening, diagnosis and
treatment in Kenya: Patient payments in the private and
public sectors. PLOS ONE, 13(1), e0190113.
https://doi.org/10.1371/journal.pone.0190113
Webber, L., Divajeva, D., Marsh, T., McPherson, K.,
Brown, M., Galea, G., & Breda, J. (2014). The future
burden of obesity-related diseases in the 53 WHO
European-Region countries and the impact of effective
interventions: A modelling study. BMJ Open, 4(7),
e004787–e004787. https://doi.org/10.1136/bmjopen-
2014-004787
World Health Organization. (2010). Package of essential
noncommunicable (PEN) disease interventions for
primary health care in low-resource settings.
http://www.who.int/nmh/publications/essential.
A Model of Cost and Time-Effective Disease Screening for Non-Communicable Diseases in India
319
