
Adopting Technological Devices in Hospital at Home: A Modelling
and Simulation Perspective
Ilaria Angela Amantea
1
, Emilio Sulis
1
, Guido Boella
1
, Andrea Crespo
2
, Dario Bianca
2
,
Enrico Brunetti
2
, Renata Marinello
2
, Marco Grosso
2
, Jan-Christoph Zoels
3
, Michele Visciola
3
,
Elena Guidorzi
3
, Luisa Miolano
3
, Giorgio Ratti
3
, Tommaso Mazzoni
3
, Ermes Zani
4
and Serena Ambrosini
5
1
Computer Science Department, University of Torino, 185 Corso Svizzera, 10149, Torino, Italy
2
City of Health and Science, 88 corso Bramante, 10126, Torino, Italy
3
Experientia, Via Cesare Battisti, 15, 10123, Torino, Italy
4
Santer Reply, Corso Francia, 110, 10138, Torino, Italy
5
Consoft Sistemi s.p.a., Via Pio VII, 127, 10127, Torino, Italy
{dbianca,ebrunetti, rmarinello, mgosso3}@cittadellasalute.to.it,
{jan-christoph, michele.visciola, elena.guidorzi, luisa.miolano, giorgio.ratt, tommaso.mazzoni}@experientia.com,
e.zani@reply.it, serena.ambrosini@consoft.it
Keywords: Business Process Analysis, Hospital-at-Home, Modelling and Simulation, e-Health.
Abstract: This article introduces a framework to integrate Business Process Management and Simulation to e-Health
solutions in the context of dehospitalization. Assistive technologies clearly have a direct and positive impact
on the quality of life of patients, but they also improve the overall management of the organizational
processes. In the framework of business process analysis, we introduce televisiting and telemedicine
applications. In particular, we define modeling and simulation of hospital services as a base to investigate
the role of technological innovations in order to explore the positive impact both on patient well-being as
well as on business process management perspective.
1
INTRODUCTION
The ageing of the general population is gradually
shifting the attention to integrate the classic hospital
model to alternative care. This fact increasing
interest in models of home care and focused on the
needs of patients often suffering from multiple
chronic diseases (Tibaldi et al., 2013; Ricauda et al.,
Marinello et al., n.a.).
Technological solutions have demonstrated a
positive impact on health, well-being and quality of
life. In particular, assistive technologies focus the
attention on the concepts of patient-centered care,
which is actually worldwide recognized an essential
dimension for the quality of care, as well as the so-
called patient empowerment. A recent literature
review on the topic reveals how about the half of the
articles focuses on technology applications to all
knowledge areas of health, as in the case of patient
education or medical information management
(Calvillo et al., 2013). From an organizational
perspective, Business Processes Management and
Simulations address healthcare managers, to better
allocate appropriate resources or to improve the
responsiveness of care to patients (Martinho et al.,
2016; Mans et al., 2015; Fernández-Llatas et al.,
2011). The aim of “La Casa nel Parco” (CANP)
project
1
, financed by Regione Piemonte with
European funds, is to show improved results in
different wards (geriatrics, pneumology, neurology,
physiotherapy) thanks to the application of Artificial
Intelligence (AI), integrated devices and machine
learning algorithms to e-Health software (Sulis et al.,
2019b).
In this work, we will focus on the application of
innovative telemedicine technologies supporting the
care of elderly patients in the context of a Hospital at
Home (HaH) for acute pathologies or exacerbation
of chronic pathologies. In this project, a multi-
disciplinary vision is adopted by the patient care
service, to increase the skills and competencies of
1
See website of the project: http://casanelparcoproject.it/
110
Amantea, I., Sulis, E., Boella, G., Crespo, A., Bianca, D., Brunetti, E., Marinello, R., Grosso, M., Zoels, J., Visciola, M., Guidorzi, E., Miolano, L., Ratti, G., Mazzoni, T., Zani, E. and Ambrosini,
S.
Adopting Technological Devices in Hospital at Home: A Modelling and Simulation Perspective.
DOI: 10.5220/0009970801100119
In Proceedings of the 10th International Conference on Simulation and Modeling Methodologies, Technologies and Applications (SIMULTECH 2020), pages 110-119
ISBN: 978-989-758-444-2
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

patients/caregivers, rationalizing health processes
and, consequently, the management of economic
resources.
Furthermore, user experience is essential for a
systematic improvement of the process in the so-
called cognitive computing framework (Hull and
Nezhad, 2016). Similarly, the individual behavior of
stakeholders involved in business operation, as well
as corresponding interactions, are at the core of the
discipline “subject-oriented business process
management” (Fleischmann et al., 2013). From a
software engineering perspective, the attention to
business strategies and software development has to
be integrated with users’ concerns, as in the
framework of a Human-Centered Design (Forbrig,
2016). The recognition of the user experience is one
of the main objectives to be achieved in the current
business process analysis.
In the following section, we introduce our
methodology. In the third, we contextualize the HaH
service case of study, its processes, and their
business simulation with the data analysis results
and the two different platforms. In Section 4, we
provide our concluding remarks with some
considerations about future work.
2
METHODOLOGICAL
FRAMEWORK
The framework involves four different stages:
The analysis of the context aims to understand
what the actual situation is and what could be the
needs for improvements at different levels. In-
depth user experience (UX) research with
patients, caregivers, and hospital professionals
leading to a detailed understanding of the context
(AsIs), the definition of user requirements, and
opportunities for innovative solutions.
The business process analysis examines the
actual situation of the organization intending to
create the As-Is model of the process.
The introduction of technological applications
improves the healthcare process. In particular,
we investigate some devices for telemedicine
(Ticuro Reply platform), as well as prototype
applications aimed at helping the staff with the
management of visitors tour (GoCare platform).
The business process analysis and simulation
take into account performance indicators as well
as managing changes in the new process (To-Be)
via
scenario analysis.
2.1
Business Process Analysis
In order to analyse the business processes of this
type of home hospitalization, we exploit a Business
Process Management (BPM) methodology. One of
the central issues of BPM (Dumas et al., 2018; Van
der Aalst et al., 2010; Abo-Hamad and Arisha, 2013)
is change management. Using a process-centric
approach, due to describe the diagram of the process,
we will adopt the Business Process Model and
Notations (BPMN) standard language (Di Leva et
al., 2020; Allweyer, 2016). Primarily, in the context
of healthcare studies, BPMN standard language
acquires a peculiar consideration (Amantea et al.,
2020; Sulis and Di Leva, 2018; Müller and Rogge-
Solti, 2011). The adoption of a process-centric
approach relying on a process-aware information
system combining with a simulation tool (iGrafx
LCC, n.a.) allows the redesign of business processes
in an organization.
A set of process performance measures (also
called key performance indicators or KPIs) can
address both the general and specific functioning of
the process (Van Looy and Shafagatova, 2016).
Typical performance metrics include the dimensions
of time, cost, and quality. Several measures can be
unambiguously determined also for HaH process.
We focused our attention on the process
performance dimensions of time. Firstly, we are
interested in monitoring the throughput time to
investigate the process from the start to the
conclusion. Secondly, as we are interested in
consideration about the workload of operators
involved in the process, we included working time
metrics. In particular, we adopt metrics about the
average time worked by operators, as well as the
average waiting time.
The business process analysis aims to define and
engineer a model to be verified and validated with
system experts, resulting in the so-called As-Is
model. This step includes the creation of visual
models of processes (i.e., process map or flowchart).
These diagrams depict the sequence of activities and
various crossroads (gateways), which lead to
different routes depending on choices made. Other
information integrated includes resources that
perform the activities, their characteristics
(capability, schedules, costs), the execution time of
the activities, policy management, and the realistic
workload. Thus, the simulation it is possible to
obtain an evaluation of the performance indicators
based on which the stakeholders can validate the
model.
Adopting Technological Devices in Hospital at Home: A Modelling and Simulation Perspective
111

2.2
User Experience
Results stemming from UX research and
ethnography activities, involving patients and staff
of the Hospital at Home service, informed user-
centered design processes. These were adopted to
design a prototype concept for a solution aimed at
meeting user requirements as identified during UX
research activities. The prototype application value
proposition takes into consideration major pain-point
and user needs, specifically regarding the
management of the HaH service, and the planning of
logistics required for its delivery. The value
proposition is then translated into a digital platform
prototype designed for doctors and nurses who play
a vital role in the delivery of the home
hospitalization service.
The digital platform prototype, named GoCare,
consists of software that enables medical staff to
monitor the status of patients, schedule the home
visit calendar, manage logistics and medical teams.
The dashboard also allows the healthcare staff
(during the visit and back in hospital) to update and
share information helpful to manage the day-by-day
visit reschedule. Moreover, the collected data allows
health professionals to evaluate the workload of the
HaH department and its capacity to accept new
patients.
2.3
Telemedicine
Ticuro Reply (Santer, Reply S.p.A., Turin, To, Italy)
is a suite for telemedicine (TM), telemonitoring, and
the analysis of behavioral habits. It enables the
processes of guaranteeing the management and
continuity of care through real-time data monitoring
by integrated medical devices. The suite also
includes a secure channel that allows performing
Tele-visit and Teleconsultation sessions, ensuring
secure connections between patients and
professional users or amongst professionals. The
collected data and the possibility of remote and
continuous assistance, allow health professionals to
establish an interactive relationship with patients and
their caregivers, providing them with personalized
treatment paths, from anywhere.
2.4
Re-organizations and To-Be Model
The scenario analysis and process reorganization
introduce a simulation of business processes to
investigate changes in the As-Is model by generating
the new To-Be version, including both discrete-
event and agent-based simulation (Sulis and Di
Leva, 2017).
This detailed phase includes the As-Is model
solutions for restructuring the Process, improving
the detection and understanding of inefficiencies,
bottlenecks, constraints, and risks (Amantea et al.,
2018; Sulis et al., 2019a).
In this case, the framework allows investigating
the performance of the business process with the
introduction of technological applications and e-
Health technologies.
The simulation of the different scenarios, with
the same workload (What-if analysis), allows for
comparing the scenarios, amongst each other, and in
relation to the starting As-Is model. In this way, we
obtain a new model of the Process (the To-Be
model), which should be implemented.
3
THE CASE STUDY
For more than 30 years, the “City of Health and
Science” of Turin (Italy), has operated the Hospital
at Home (HaH). A home care service, defined by
Resolution DGR n. 85-13580 of 1 March 2010, as a
form of health care hospital character, which
provides for the organization of care in the home of
patients suffering from acute diseases, but who do
not require equipment with high technological
complexity and intensive or invasive monitoring. On
average, the service has covered half of the
metropolitan city of Turin. Unlike most home care
services; HaH Service handles acute patients or
chronic patients undergoing exacerbation of a
disease. Requests for activation of this service are
made by the emergency or regular departments and
by general medical doctors. After that, each patient
is evaluated by the team in order to establish the
feasibility of hospitalization under HaH. The service
is available every day from 8 am to 8 pm. In the case
of a night emergency, patients refer to the Regional
Emergency Service, with which they have a specific
memorandum of understanding. As an integrated
care service, the team is multidisciplinary and
includes 4 geriatric doctors, 14 nurses (including a
nursing coordinator and a patient acceptance
manager), 1 counselor, 1 social worker, 4 part-time
physiotherapists. Patients are visited daily by
medical or nursing staff, either jointly or by at least
one of these two professionals. For the individual
patient, the therapeutic objectives are programmed
during collective team meetings according to the
clinical trend, helping to offer the best possible care
to the patient and optimize available resources.
Telemedicine/Telemonitoring (TM) may represent a
SIMULTECH 2020 - 10th International Conference on Simulation and Modeling Methodologies, Technologies and Applications
112

potential and strong ally in the management of the
patient admitted under the HaH regime. The use of
communication systems in the remote management
of the patient could improve treatment outcomes,
increase access to care, and reduce health costs
(Caplan et al., 2012).
3.1
The As-Is Hospital at Home Service
Hospital at Home could be considered as an
alternative to the traditional ward for elderly
patients.
The service of hospitalisation is a geriatric
department for taking charge of patients in acute
phases still in their own homes. We present the
service by dividing it into acceptance of the patients
in Figure 1 and the real tour for the visits for each
patient in Figure 2. All activities in the images
represent the whole As-Is service. Due to limitations
of space, we cannot describe each in detail, so we
will only describe some in the To-Be section,
activities that may change with the introduction of
healthcare devices that use artificial intelligence to
provide a superior experience. The detail for the
acceptance process is published in the paper
(Amantea et al., 2019).
3.2
GoCare Platform
The Experientia prototype platform named GoCare
is a management tool that helps doctors and nurses
optimize organization and logistic tasks
management. The platform provides medical staff
with a visual and interactive dashboard to manage
and organize the patient’s assignment, grouping
them into different visiting equips and time slots
according to the impact of specific indices (Figure
3). The most relevant are the medical and nursing
complexity care, as well as the condition of the
caregiver and the geographical location of the
various patients. Such indexes are already evaluated
manually by the medical staff to schedule and
prepare the visits. As shown in Figure 4, it is
possible to see on a map how patients are distributed
within the territory, and the dashboard allows
manual changes. Also, the platform provides doctors
and nurses the possibility of accessing the personal
patient page (Figure 5). Here it is possible to update
all information regarding the patient trend (including
complexity and priority indices), exams to be
considered, supplies and drugs required to be
prepared for the next visit, and a section to fulfill
with notes, useful to analyze and evaluate patient’s
status. The possibility to quickly update this
information as soon as the visit is complete allows
for time savings and reduction of risk of having stray
information. Also, unlike the current procedure,
which consists of transcribing handwritten notes on
paper and then returning them to the hospital, it
allows having all information in one single shared
place accessible to all the relevant medical staff.
3.3
Ticuro Reply Platform
During the intervention group each patient/main
caregiver pair will be given the necessary tools for
the TM via Ticuro Reply platform (Santer, Reply
S.p.A., Turin, To, Italy), these include
sphygmomanometer, pulse oximeter, balance,
thermometer, glucometer, electrocardiograph,
spirometer (see attached technical datasheet). Upon
delivery of the instruments, a brief training will be
given to the primary caregiver and, if possible, the
patient, about the operation of the various equipment
by specially trained nurses. During pre-established
time slots, the caregivers should carry out the
detection of arterial pressure, peripheral arterial
hemoglobin saturation, and tympanic body
temperature twice a day, or once a day concerning
body weight. The glucometer will be used
exclusively by healthcare professionals in the case of
patients requiring capillary blood sugar monitoring.
The electrocardiograph will be used according to the
clinical progress of the patient, always by the health
care professional. The data recorded by the
instruments will be automatically sent to the data
collection platform Ticuro Reply and will be
viewable by medical and nursing staff on the same
platform (as shown in Figure 6), to allow for timely
interventions.
3.4
The To-Be e-Health Hospital at
Home Service
In Figure 1 and 2 there are some activities in other
colors. Activities in full or half color are those
affected by the improvement of healthcare devices.
The blue ones represent activities improved by the
GoCare platform, the yellow ones represent
activities improved by the Telemedicine of Santer,
and the ones in blue and yellow are affected by both
of the new technologies.
The acceptance process (Figure 1) represents an
assessment of the patient’s suitability for this service
as an alternative to the usual hospital admission. The
activities of this process consist purely of medical
evaluations and explanations of the service to
patients and caregivers. Following these interviews,
Adopting Technological Devices in Hospital at Home: A Modelling and Simulation Perspective
113
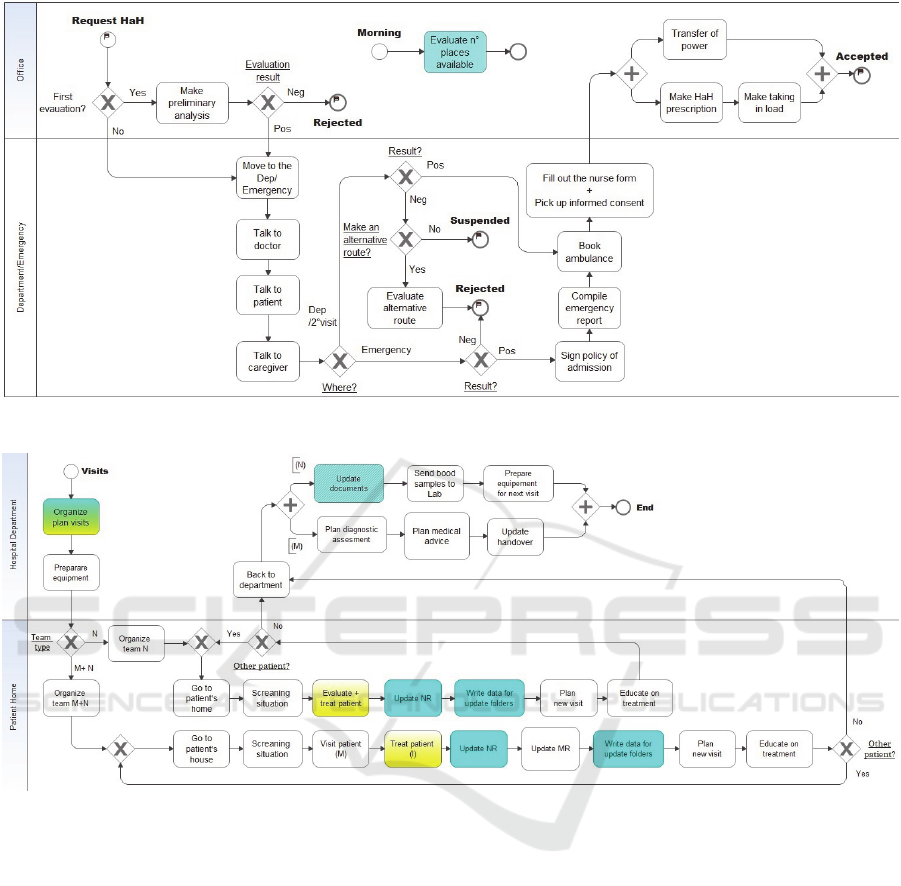
Figure 1: Process of acceptance of requests for the HaH service.
Figure 2: Process of domicile visits.
the hospital’s manager will decide whether the
patient is suitable and, on the other hand, the patient
and the caregiver will decide whether to accept this
type of hospitalization or whether to opt for the
traditional one. Therefore, the only activity that can
be supported at this stage is the evaluation of the
actual workload. As there are no physical beds, the
maximum number of
patients that can be accepted
by the department each day is calculated based on
the complexity of the patients they are already in
charge of and the staff available. The average patient
load is about 28, but the more complex the patients’
conditions are, the more this number will tend to
drop; likewise, close to holidays staff will reduce,
and so will the maximum number of patients, and
vice versa. Table 1 shows the differences between
As-Is and To-Be processes in terms of Activities,
Actions, Human Resources, Equipment Resources,
and Time on average.
Regarding the real visits tour (Figure 2), there
are different possible improvements. For planned
visits, the GoCare platform could support the
organization before leaving the hospital. During this
phase, the medical staff has to check the
measurements of the vital parameters measured with
the telemedicine devices. These results may affect
the choice of pharmaceuticals to bring to home
patients. Currently, these vital parameters are
detected by the nurse for each visit as a first step.
If they are measured by caregivers several times
a day, this action is not necessary during the tour
visit. At the moment, nurses have paper folders in
which they take notes; once in the office, they
transcribe these in three different paper dossiers.
SIMULTECH 2020 - 10th International Conference on Simulation and Modeling Methodologies, Technologies and Applications
114

Figure 3: Screenshot of the tool that shows the team composition and assignment of patients to teams, distributed over the
potential expected working time of the different patients based on the inserted complexity indices.
Table 1: Comparison between the As-is and the To-be
model for the acceptance process.
As-is To-be
Activity
Action
HR
ER
Time
Evaluate places
available
Evaluate
workload
Case Manager
Paper dossier of:
patient organize,
patient visits,
nursing records
for each patient
90 min
Evaluate places
available
Evaluate
workload
Case Manager
Tablet
15-20 min
This process leads to problems: waste of time in
reporting the same things twice, increasing the
chance of making mistakes and since the files are the
same for all the patients and the staff comes back at
about the same time, every nurse will have to wait
that the previous ones finish the transcript. Thanks to
the GoCare platform, the nurses can write directly
on a personal tablet at the patient’s house, saving
both the transcript activity in the office and the wait
to do it.
The differences from As-Is and To-Be processes
are shown in detail (potential for changing actions),
Human Resources, Equipment Resources, and Time
on average for each activity.
Table 2 shows the difference made with the
implementation of GoCare platform, and Table 3
shows the difference made with the implementation
of the Ticuro Reply platform.
Adopting Technological Devices in Hospital at Home: A Modelling and Simulation Perspective
115

Figure 4: Screenshot of the tool that shows the geolocation of the various patients, the assignment of patients to teams, and
the proposed road hogs.
Figure 5: Screenshot of the tool that shows the patient’s page where it is possible to consult and update the patient’s actual
data, his level of complexity, and information about the visit he needs.
SIMULTECH 2020 - 10th International Conference on Simulation and Modeling Methodologies, Technologies and Applications
116

Figure 6: Example of Ticuro Reply platform screen visible to hospital staff. For each patient active telemedicine devices are
visible and for each device it is possible to view the data collected directly concerning the patient.
4
RESULTS
By integrating telemedicine and user experience into
an already innovative service like home
hospitalization, we could see that every transaction
could gain on average from 1.3 to 4 hours. Starting
from the premise that the entire visits tour must be
within the working time of the hospital staff and the
time of care cannot decrease because it would
diminish the service quality, the geographical area of
the service and the number of the patients in charge
is limited. Thanks to these improvements maintain-
ing the service quality with the current human
resources, two different scenarios would be possible:
It would be possible to increase the overall
number of patients in charge. The service
could be available for about 6 12 more
patients, depending on the severity of the
patients’ clinical conditions and the time of
year (hospital staff decreases in periods like
Christmas or holidays).
It would be possible to increase the extension
of the geographical area covered by the
service. Currently, the movements from one
patient to another (and the related search for
parking, not always easy in a metropolitan city
like Turin) is between 5 and 25 minutes.
Therefore, it appears that the displacements
between one patient and another could
increase by a range of about 9.36 28.8 min. It
would be potentially possible for the service to
cover the entire geographical area of the city.
5
CONCLUSIONS
This paper introduced a framework of modeling and
simulation effort concerning an innovative hospital
service. The main goal is to define and implement a
robust technological and organizational model in a
healthcare context and obtain high adherence,
compliance, and engagement of users.
Furthermore, it supports the long-term
sustainability and efficiency of health and social care
systems by providing a solution that allows people
to live longer in their homes and to ease
communication with the healthcare and social care
systems. The proposed framework demonstrates
how to improve patient’s wellbeing and autonomy,
and how better and more sustainable healthcare
interventions may lead to a reduction of healthcare
and social costs. The expected implementation
results of this framework of business process
analysis suggest an improvement of professional and
informal care processes, leading to a higher patient’s
autonomy during acute, post-acute, and
rehabilitation phases.
Additionally, thanks to the innovativeness,
adaptability and diffusion on the territory of this
service, it is able to give a significant positive
Adopting Technological Devices in Hospital at Home: A Modelling and Simulation Perspective
117

Table 2: Visits tour comparison between the As-is and the
To-be model after the implementation of GoCare platform.
As-is To-be
Activity
Action
HR
ER
Time
Organize
Plan Visits
Organize
plan visits
All staff
Paper dossier of:
patient organize,
patient visits,
addresses,
nursing records
90-120 min
Organize
Plan Visits
Organize
plan visits
All staff
Tablet
30-50 min
Activity
Action
HR
ER
Time
Update NR
Update on
paper
Nurse
Nurse record/
folder
10min
Update NR
Update on
platform
Nurse
Tablet
10-20 min
Activity
Action
HR
ER
Time
Update documents
Update paper dossier
patient organize,
patient visits,
delivered materials,
nursing records,
All nurses
Paper dossier
1 patient organize for all,
1 patient visits for all,
1 delivered materials for all,
1 nursing records for each,
(30 min X 6 nurses)
No activity
-
-
-
0 min
contribution even in a state of emergency. In these
days, the TELEMACO project
2
was launched. The
purpose of this study is to test the use of telemedicine
(TM) device to support the management of patients
suspected of COVID-19 or discharged from the
hospital departments with diagnosis of COVID-19,
hospitalized under HaH service. We suppose to have
soon some significant results.
As other future work, we plan to exploit data from
devices by applying process mining techniques.
Considering the intersection between data mining and
business processes modeling and analysis is
promising and aim to automatically discover and
measure processes, by adopting automatic recordings
of healthcare events (so called “event logs”). In the
context of our BPM framework, we plan to exploit
process mining techniques to improve both clinical
and administrative processes analysis.
2
Telemedicine for elderly patients COVID-19 positive
treated by Hospital at Home Service, approved by the
Ethics Committee on 6 May 2020.
Table 3: Visits tour comparison between the As-is and the
To-be model after the implementation of the telemedicine
of Ticuro Reply platform.
As-is To-be
Activity
Action
HR
ER
Time
Organize
Plan Visits
-
All staff
-
-
Organize
Plan Visits
Check vital signs
for all patients
All staff
Tablet
15-20 min
Activity
Action
HR
ER
Time
Evaluate+
Treat patient
Evaluate+treat
+Check vital signs
Nurse
Medical equipment
Treat+(3-15 min)
Evaluate+
Treat patient
Evaluate+treat
-Check vital signs
Nurse
Medical equipment
Treat+ 0 min
Activity
Action
HR
ER
Time
Treat patient
Treat+
Check vital signs
Nurse
Medical equipment
Treat+(3-15 min)
Treat patient
Treat-
Check vital signs
Nurse
Medical equipment
Treat+0 min
ACKNOWLEDGEMENTS
This research was conducted in the project “CANP
CAsa Nel Parco” of Regione Piemonte funded by
POR FESR PIEMONTE 2014-2020. We are grateful
for the collaboration of the “City of Health and
Science” of Torino (Italy).
REFERENCES
Abo-Hamad, W. and Arisha, A. (2013). Simulation-based
framework to improve patient experience in an
emergency department. European Journal of
Operational Research, 224(1):154–166.
Allweyer, T. (2016). BPMN 2.0: introduction to the
standard for business process modeling. Books on
Demand.
Amantea, I. A., Arnone, M., Leva, A. D., Sulis, E.,
Bianca, D., Brunetti, E., and Marinello, R. (2019).
Modeling and simulation of the hospital-at-home
service admission process. In Obaidat, M. S., Ören, T.
I., and Szczerbicka, H., editors, Proceedings of the 9th
International Conference on Simulation and Modeling
Methodologies, Technologies and Applications,
SIMULTECH 2019, Prague, Czech Republic, July
2931, 2019, pages 293–300. SciTePress.
Amantea, I. A., Di Leva, A., and Sulis, E. (2018). A
simulation-driven approach in risk-aware business
process management: A case study in healthcare. In
Proceedings of 8th International Conference on
SIMULTECH 2020 - 10th International Conference on Simulation and Modeling Methodologies, Technologies and Applications
118

Simulation and Modeling Methodologies,
Technologies and Applications, volume 1, pages 98–
105. SciTePress.
Amantea, I. A., Di Leva, A., and Sulis, E. (2020). A
simulation-driven approach to decision support in
process reorganization: A case study in healthcare. In
Exploring Digital Ecosystems, pages 223–235.
Springer.
Calvillo,
J.,
Roma´n,
I.,
and
Roa,
L.
(2013).
How
technology
is empowering patients. A literature
review.
Caplan, G. A., Sulaiman, N. S., Mangin, D. A., Aimonino
Ricauda, N., Wilson, A. D., and Barclay, L. (2012). A
meta-analysis of “hospital in the home”. Medical
Journal of Australia, 197(9):512–519.
Di Leva, A., Sulis, E., De Lellis, A., and Amantea, I. A.
(2020). Business process analysis and change
management: The role of material resource planning
and discrete-event simulation. In Exploring Digital
Ecosystems, pages 211–221. Springer.
Dumas, M., La Rosa, M., Mendling, J., and Reijers, H.
(2018). Fundamentals of business process
management, volume 1. Springer, 2nd edition.
Fernández-Llatas, C., Garcia-Gomez, J. M., Vicente, J.,
Naranjo, J. C., Robles, M., Benedi, J. M., and Traver,
V. (2011). Behaviour patterns detection for persuasive
design in nursing homes to help dementia patients. In
2011 Annual International Conference of the IEEE
Engineering in Medicine and Biology Society, pages
6413–6417. IEEE.
Fleischmann, A., Schmidt, W., and Stary, C. (2013).
Subject-oriented bpm = socially executable bpm. In
2013 IEEE 15th Conference on Business Informatics,
pages 399–407.
Forbrig, P. (2016). Continuous software engineering with
special emphasis on continuous business-process
modeling and human-centered design. In Proceedings
of the 8th International Conference on
SubjectOriented Business Process Management, S-
BPM ’16, New York, NY, USA. Association for
Computing Machinery.
Hull, R. and Nezhad, H. R. M. (2016). Rethinking bpm in
a cognitive world: Transforming how we learn and
perform business processes. In International
Conference on Business Process Management, pages
3–19. Springer.
iGrafx LCC. iGrafx Process 2015 for Six Sigma.
Mans, R., Van der Aalst, W., and Vanwersch, R. (2015).
Process mining in healthcare: evaluating and
exploiting operational healthcare processes. Springer.
Marinello, R., Rocco, M., Tibaldi, V., Bardelli, B., and
Tamone, C. Ospedalizzazione a domicilio: cronaca di
un’esperienza.
Martinho, R., Domingos, D., and Resp´ıcio, A. (2016).
Evaluating the reliability of ambient-assisted living
business processes. In ICEIS (2), pages 528–536.
Mu¨ller,
R.
and
Rogge-Solti,
A.
(2011).
Bpmn
for
health
care processes. In Proceedings of the 3rd
CentralEuropean Workshop on Services and their
Composition (ZEUS 2011), Karlsruhe, Germany,
volume 1.
Ricauda, N. A., Marinello, R., Rocco, M., Tibaldi, V.,
Maddalena, M., Boscarino, G. I., Bertone, P., and
Isaia,
G. C. Lo sviluppo del servizio di ospedalizzazione a
domicilio.
Sulis, E., Amantea, I. A., and Fornero, G. (2019a).
Riskaware business process modeling: A comparison
of discrete event and agent-based approaches. In 2019
Winter Simulation Conference, WSC 2019, National
Harbor, MD, USA, December 8-11, 2019, pages
3152–3159. IEEE.
Sulis, E., Cena, C., Fruttero, R., Traina, S., Feletti, L. C.,
de Cosmo, P., Armando, L., Ambrosini, S., Amantea,
I. A., Boella, G., Marinello, R., Bianca, D., Brunetti, E.,
Bo, M., Bianco, A., and Cattel, F. (2019b). Monitoring
patients with fragilities in the context of
dehospitalization services: An ambient assisted living
healthcare framework for e-health applications. In
IEEE 23rd International Symposium on Consumer
Technologies, ISCT 2019, Ancona, Italy, June 19-21,
2019, pages 216–219. IEEE.
Sulis, E. and Di Leva, A. (2017). An agent-based model
of a business process: The use case of a hospital
emergency department. In International Conference
on Business Process Management, pages 124–132.
Springer.
Sulis, E. and Di Leva, A. (2018). Public health
management facing disaster response: a business
process simulation perspective. In Proceedings of the
2018 Winter simulation Conference, pages 2792–
2802. Winter Simulation Conference.
Tibaldi, V., Ricauda, N. A., Rocco, M., Bertone, P.,
Fanton, G., and Isaia, G. (2013). L’innovazione
tecnologica e l’ospedalizzazione a domicilio. Recenti
Progressi in Medicina, 104(5):181–188.
Van der Aalst, W. M., Nakatumba, J., Rozinat, A., and
Russell, N. (2010). Business process simulation. In
Handbook on BPM 1, pages 313–338. Springer.
Van Looy, A. and Shafagatova, A. (2016). Business
process performance measurement: a structured
literature review of indicators, measures and metrics.
SpringerPlus, 5(1):1797.
Adopting Technological Devices in Hospital at Home: A Modelling and Simulation Perspective
119
