
A Reinforcement Learning and IoT based System to Assist Patients with
Disabilities
Muddasar Naeem
1 a
, Antonio Coronato
2
, Giovanni Paragliola
2
and Giuseppe De Pietro
2
1
Universita’ Degli Studi di Napoli Parthenope, Napoli, Italy
2
ICAR-CNR, Napoli, Italy
Keywords:
Artificial Intelligence, Disability, Healthcare, IoT, Pill Reminder, Reinforcement Learning.
Abstract:
One of the important aspect of clinical process is to complete treatment according to given plan. The suc-
cessful completion of this task is more challenging when a person have some physical or mental disability
and requires resources and man power for personalized treatment and care. We can mitigate this problem by
an intelligent guidance and monitoring system who can assist elderly persons and patients in their treatment
schedule. Reinforcement learning and IoT systems have received considerable credit of significant contribu-
tion in healthcare over last few years, could be suitable choice for said objective. We propose a pill reminder
system using Bayesian reinforcement learning assisted with IoT devices to help people (having mental and/or
physical disability) in their treatment plan. The proposed intelligent system is able to successfully communi-
cate with the person through a suitable audio, visual and textual message. The proposed pill-reminder system
has been demonstrated for a specific treatment plan of a hypertension patient.
1 INTRODUCTION
An important aspect of treatment for all stake holders
connected to healthcare sector in continuous improve-
ment to patient treatment which ensure provision of
satisfaction to patients (Ross et al., 1993). Success
to this objective is not dependent on single factor
instead it depends on many factors like trained per-
sonal, quality care centers, medical and nuclear exam-
ination equipment, use of suitable medication (Gul-
lapalli N Rao, 2002)and use of modern technology
i.e Artificial Intelligence (AI) and Machine Learn-
ing (ML). We have witnessed the revolution of AI
and transformation it has brought to our living style
(Patel et al., 2009), (A Testa, ). Some of appeal-
ing applications are: diagnostic systems (Ling et al.,
2017), virtual assistants , personalized treatment (Pe-
tersen et al., 2018), DTR, a multi-step clinical de-
cision processes ((Lavori, 2004), (Chakraborty, )),
medical imaging (Sahba et al., 2006), dialogue sys-
tems and chat-bots (Kearns et al., 2011), risk manage-
ment ((Giovani Paragliola, 2019), (Antonio Coronato,
2019) ), control systems (Prasad et al., 2017) and re-
habilitation (Reinkensmeyer et al., 2012), (G Paragli-
ola, ). That is why billion dollars have been investing
a
https://orcid.org/0000-0003-0815-4883
on use of AI and ML especially Reinforcement Learn-
ing (RL) in healthcare.
RL is an ML approach much more focused on
goal-directed learning from interaction, than other ap-
proaches of machine learning i.e. supervised and un-
supervised learning (Sutton and Barto, 1998). In the
last decade, we have seen much application on the
use of RL in healthcare departments. This is due to
the similar objective of RL algorithms and clinicians.
This is to say that the goal of doctors is to find an op-
timal sequence of treatments for a particular patient.
This scenario is in accordance with the major objec-
tive to RL which is to find an optimal policy for a
given problem in a given environment. Hence, RL
has achieved considerable success to help clinicians
in optimizing and personalizing treatment sequences
(Thall and Wathen, 2005) (Murphy et al., 2006).
Normally, caregivers are being used to assist pa-
tients and elderly persons in their activities of daily
living (ADL) through the use of cues, signals and ver-
bal reminders. Then we saw the development of a
computer-based solution ’ Cognitive Ortosis for As-
sisting activities in the Home (COACH)’ (M.A.Sc.
et al., 2001) to assist dependent persons, an agent
based platform for task distribution in virtual envi-
ronments (A Coronato, ). Few research work on use
of computer vision technology to assist patients are:
Naeem, M., Coronato, A., Paragliola, G. and De Pietro, G.
A Reinforcement Learning and IoT based System to Assist Patients with Disabilities.
DOI: 10.5220/0009783804910498
In Proceedings of the 5th International Conference on Internet of Things, Big Data and Security (IoTBDS 2020), pages 491-498
ISBN: 978-989-758-426-8
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
491
(Wren et al., 1997), (Oliver et al., 2004), (D. F. Llorca,
2007), (Llorca et al., 2011).
In this century, we have moved to the use of
AI and ML in the healthcare sector e.g predictive
analysis, development of intelligent robotic care-
givers, making the ICU smarter (Suresh et al., 2017).
The systems based on ML decision making ap-
proaches like ’Partially Observable Markov Deci-
sion Process (POMDP)’ are: the assisted cognition
project (H. Kautz, 2002), a situation-aware system
for the detection of motion disorders of patients with
autism spectrum disorders (A Coronat0, ) aware home
project (Mynatt et al., 2000), the adaptive house
(Mozer, 2005), nursebot project (Pineau et al., 2003)
and automated hand-washing assistance (30, 2010).
Most of these works assist elder persons and patients
with dementia in one of ADL like hand washing.
The contribution of the present work is to assist
patients of any disease and elderly persons having any
mental or physical disabilities like audio and visual
instead of assisting with physical activities. We mod-
eled the problem as an MDP and provide a solution
by using Bayesian Thompson sampling.
The proposed intelligent system first sends a
reminder to patients according to one’s treatment
plan and then guide the patient to specific medicine
through an appropriate type of message. We have
also demonstrated our work on a practical treatment
plan which was advised to a patient of hypertension.
The message type is very critical and the choice of
message is performed by considering a person’s skills
i.e. physical and mental. After learning, the RL agent
can choose a suitable type of audio message or visual
message or text message depending upon one’s phys-
ical and mental abilities.
The next part of the paper is organized as follows.
Section 2 presents a brief introduction of RL followed
by the system model section, results and discussion
and finally the conclusion of work.
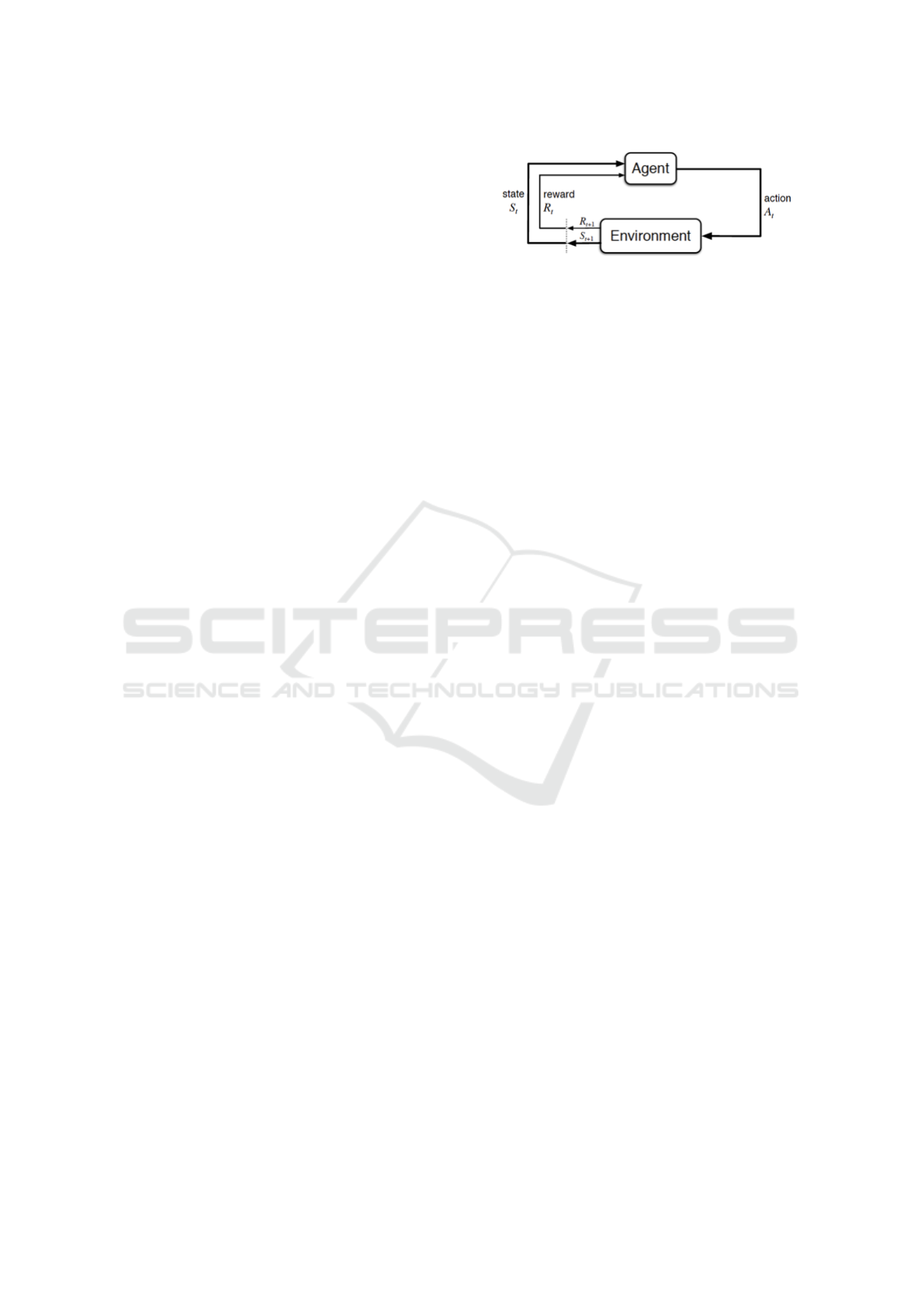
2 BACKGROUND
Markov Decision Process (MDP) is the central con-
cept of all RL problems. The goal of the RL algo-
rithms is to find the solution to an MDP. Ans MDP
model has the following components:
-Set of states: S =
{
s
1
, s
2
, s
3
, .....s
n
}
-Set of actions: A =
{
a
1
, a
2
, a
3
, .....a
n
}
-Transition model: T (s
t
, a, s
t+1
)
-Reward R
Reward and transition model depend upon on cur-
rent state s
t
, selected action a
t
and resulting state s
t+1
.
Figure 1: The Reinforcement Learning problem.
The target of RL algorithms is to interact with
a given world either with some prior knowledge i.e
reward and transition model (model-based RL e.g
Dynamic Programing which includes value iteration
and policy iteration) or without any prior knowledge
(model-free RL). Examples of model-free algorithms
are Monte Carlo and Temporal difference (TD) learn-
ing. Q-learning and SARSA are widely used as
TD algorithms (Russell and Norvig, 2009). After
many repetitive interactions with the environment, the
agent learns the characteristics of the environment.
The target of RL agent is to find an optimal action
out of available actions in each state. Optimal action
returns best desired numerical reward to the agent.
An agent choose an action in each state which results
in a policy π. An optimal policy maximizes the ag-
gregated future reward for a specific problem. The
working framework of RL is shown in figure 2.
An RL agent should maintain a balance between
exploitation and exploration while learning i.e. an
equilibrium between maximizing reward from al-
ready known useful actions or to explore new moves
which even give better rewards. In exploitation, the
priority of the agent is to select the best action based
on his learning and knowledge and in exploration,
the agent attempts actions in a stochastic way to im-
prove his experience and learning to get more re-
ward. Bayesian methods can be a solution to the
exploitation-exploration dilemma due to their ability
to capture uncertainty in learned parameters and avoid
over-fitting (Welling and Teh, 2011). Few famous
methods used for Bayesian approximations are My-
opic (Dearden et al., 2013) and Thompson Sampling
(Strens, 2000) which will be used in present work.
3 SYSTEM MODEL
This section presents the proposed approach based on
Bayesian RL agent, planner and checker (IoT system)
to assist patients and elderly persons at home hav-
ing one or a combination of more than one disabil-
ity. We consider audio, visual disabilities and condi-
tion of patient working memory and attention. The
goal of the RL agent is to provide assistance to the
patient according to his/her treatment plan through a
AI4EIoTs 2020 - Special Session on Artificial Intelligence for Emerging IoT Systems: Open Challenges and Novel Perspectives
492
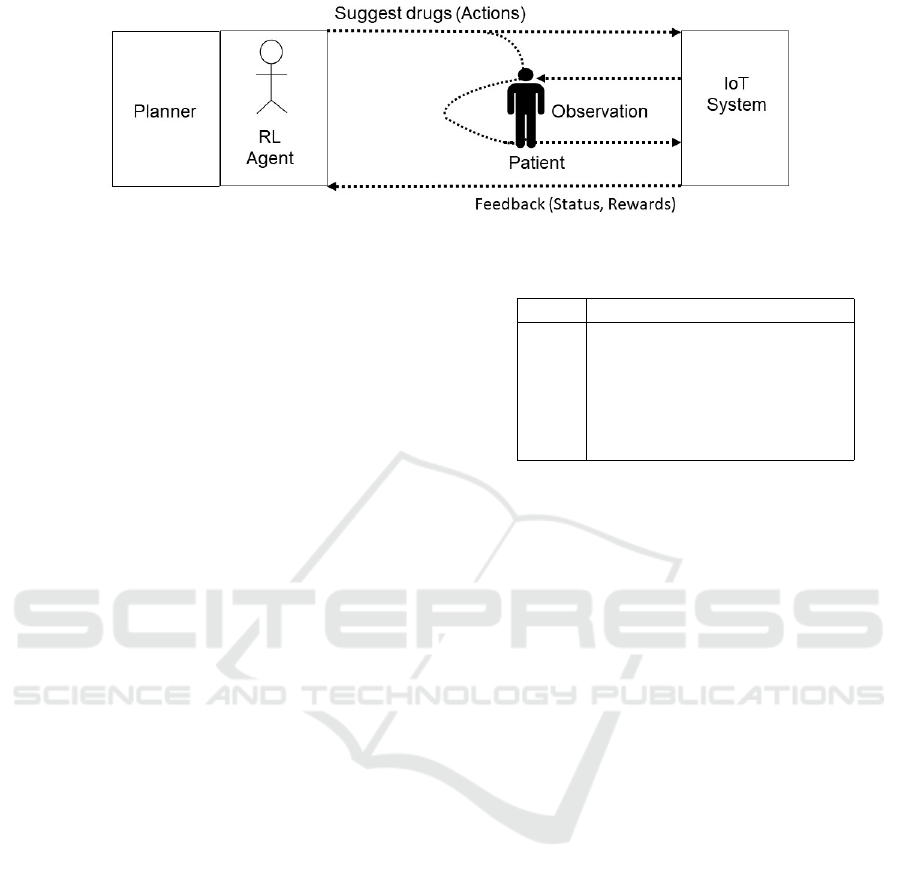
Figure 2: The proposed model.
suitable message. Figure 2 shows the proposed model
which has three main components such as planner, tu-
tor (agent) and IoT system as checker or observer.
The planner sends a reminder to both tutor and
checker according to the advised treatment plan. The
tutor’s role is most important which is to choose a
suitable choice of message for communication with
the patient. The tutor considers the physical and men-
tal abilities of the patient before selecting the way of
communication. The role of the checker is to monitor
the patient takes the right drug. It observes the status
and sends it along with the reward to the Tutor
The audio, visual, working memory and attention
abilities which tutor must consider are defined below:
Auditory Perception
- Audio Skill (AU
s
) in [0− > 1] : The audio skill
plays an important role in the treatment process of
any patient and reduces dependency on caregivers.
Our intelligent reminder system takes account of au-
dio disability before choosing a message. If a patient
has a lower skill of audio perception then the proba-
bility that he/she can listen to an audio message will
be low and consequently the chance of discontinuity
of in planned treatment. In that case, we have to check
for other skills of the patient like visual perception.
Visual Perception
- Visual Skill (V S
s
) in [0− > 1] : It is another im-
portant skill that must be considered when assisting
patients and the elderly population. The lower visual
skill means that the probability to view a visual mes-
sage will be minimal. Our agent has alternative op-
tions to select in case someone has a week of visual
perception.
Working Memory
- Working Memory High Skill (W M
hs
) in [0− >
1] : The lower the skill, the lower the probability to
understand a “complex” message. For example, if a
patient’s working memory high skill is in good condi-
tion then he can understand audio or visual scientific
messages depending on his/her audio and visual dis-
ability level.
- Working Memory Low Skill (W M
ls
) in [0− >
1] : The lower the skill, the lower the probability to
Table 1: Basic Messages.
Label Message Type
C1 Audio Scientific Message
C2 Audio Simple Message
C3 Visual Pill-Box Image
C4 Visual Pill-Box and pill Image
C5 Scientific Textual Message
C6 Simple Textual Message
understand “simple” audio or visual message.
Attention
- Attention Skill (AT
s
) in [0− > 1] : The lower the
skill, the higher the probability to ignore the message.
The attention of the patient is critical in the successful
completion of the task. It’s feedback which when pos-
itive, motivates our agent to select and send messages
to the patient.
We define six types of messages as shown in table
1 by using the first four skills. For example, a suit-
able message for the patient who has a good audio
ability and working memory is a scientific audio mes-
sage e.g ’take ’Adalat Crono 30mg’ pill’. When hav-
ing reasonably good audio skills but with lower work-
ing memory then a simple audio message is a better
choice instead of a scientific message i.e. ’take the pill
from the red, white, green, etc box’. Similarly, when
a patient’s audio skills are not good but visual ability
is good then the agent has options to select an image
of pill-box or image of a pill or a scientific or simple
text message depending on the condition of working
memory.
The planner sends a reminder to the RL agent on
a scheduled hour with the name of the medicine. It
wakes up both tutor and checker when it is time for
the patient to take a drug In the current simulation
setup, we use a timer to keep track of hours and day
of the treatment plan. In the next version, we will use
the system input to keep track of hours and days.
Then tutor i.e. the agent chooses a single or com-
bination of the audio, visual and textual message. Af-
ter receiving a message from the RL agent, the possi-
ble directions for the patient is going to the right pill-
A Reinforcement Learning and IoT based System to Assist Patients with Disabilities
493

box or wrong pill-box as graphically shown in figure
3.
The checker monitors the patient’s actions through
suitable IoT devices and sends feedback to the RL
agent (Muddasar Naeem, 2020). It checks the drug
that the patient is going to take, observes the status
and sends it along with the reward to the Tutor. The
reward for the RL agent to guide a patient to the right
box is one and zero otherwise .
Before sending a message, the agent checks
whether a patient is attentive or no and in case, the pa-
tient is not attentive, the agent waits and sends repet-
itive alerts to catch the attention of the patient. Once
the patient gets attentive then the agent will start send-
ing a suitable message by considering the audio, vi-
sual and working memory skills.
In figure 3, large open circles are states and small
solid circles are action nodes for each state-action
pair. This is a finite MDP model (Sutton and Barto,
1998) and the resulting destination state depends on
the probability of the current state-action pair. The pa-
tient will be directed to the right box if he/she under-
stands the message sent by the agent. The probability
that a patient will understand a message or ignore a
message is calculated as:
Probability that the message understood = P
mu
P
mu
= f (AU
s
,V S
s
,W M
hs
,W M
ls
)
Probability that the message ignored = P
mi
P
mi
= f (AT
s
)
(1)
Equations 3 and 1 indicate the probability that a
patient understands a message is a function dependent
on the audio, visual and working memory abilities of
that patient. Similarly, the probability that a patient
will ignore a message depends on the attention sta-
tus of the patient. This can be further elaborated in
equations 2 and 3.
P
mu
= min(1,C1 ∗ AU
s
∗WM
hs
+C2 ∗ AU
s
∗WM
ls
+
C3 ∗V S
s
∗WM
hs
+C4 ∗V S
s
∗WM
ls
+
C5 ∗V S
s
∗WM
hs
+C6 ∗V S
s
∗WM
ls
)
(2)
P
mi
= 1 − AT
s
(3)
The state value and action-value function for an
RL problem using the Bellman equation can be writ-
ten as shown in equations 4 and 5 respectively.
V π(s
0
) =
∑
a
π(s, a)
∑
s
0
p(s
0
|s, a)[R(s, s
0
, a) + γV
π
(s
0
)]
(4)
Q
π
(s, a) =
∑
s
0
p(s
0
|s, a)[R(s, s
0
, a) + γQ
π
(s
0
, a
0
)] (5)
The target of value function approaches is to cal-
culate state and action-value function and then drive
the optimality policy through maximum value func-
tion in every state. Optimal state value function using
Bellman optimally equation 6 is given as:
V
π∗
(s
0
) = max
a∈A(s)
∑
s
0
p(s
0
|s, a)[R(s, s
0
, a) + γV
π∗
(s
0
)]
(6)
By using equation 6, we can write optimal equa-
tion for our model. For example, the Bellman opti-
mality equation at wait and message selection states
abbreviated as w and MS respectively, may be written
as shown in equations 7, 8 and 9.
V
∗
(w) = max
|{z}
a
p(w|w, a)[r(w, a, w) + γV
∗
(w)]+
p(MS|w, a)[r(MS, a, w) + γV
∗
(MS)]
(7)
V
∗
(w) = max
|{z}
a
P
mi
[r(w, a, w)+ γV
∗
(w)]+
(1 − P
mi
)[r(MS, a, w) + γV
∗
(MS)]
(8)
V
∗
(MS) = max
|{z}
a
P
mu
[r(RB, a, MS) + γV
∗
(RB)]+
(1 − P
mu
)[r(W B, a, MS) + γV
∗
(WB)]
(9)
Q
π
∗
(s, a) =
∑
s
0
P(s
0
|s, a)[R(s, s
0
, a) + γ ∗ max
a
0
Q
π∗
(s
0
, a
0
)]
(10)
The Bellman equation we need to solve for
Bayesian RL is given in 11.
V
π∗
(x, b) = max
a
∑
x
0
Pr(x
0
|x, b, a)[X
0
r
+ γV
π∗
(x
0
, b
xax
0
)]
(11)
Where X, b and Pr(x
0
|x, b, a) represents set of
states, distribution (belief) over the unknown θ used
for exploration and transition probabilities respec-
tively. Each selected message will guide a patient to
the right box with a certain probability. The higher
the probability the more likely the person reached the
right box. This unknown probability θ is modeled
based on our initial probabilities given in 2 and 3.
Based on initial probabilities, we model the poste-
rior distribution of θ using Bayes rule as follows:
P(θ|x) =
P(x|θ)P(θ)
P(x)
(12)
AI4EIoTs 2020 - Special Session on Artificial Intelligence for Emerging IoT Systems: Open Challenges and Novel Perspectives
494
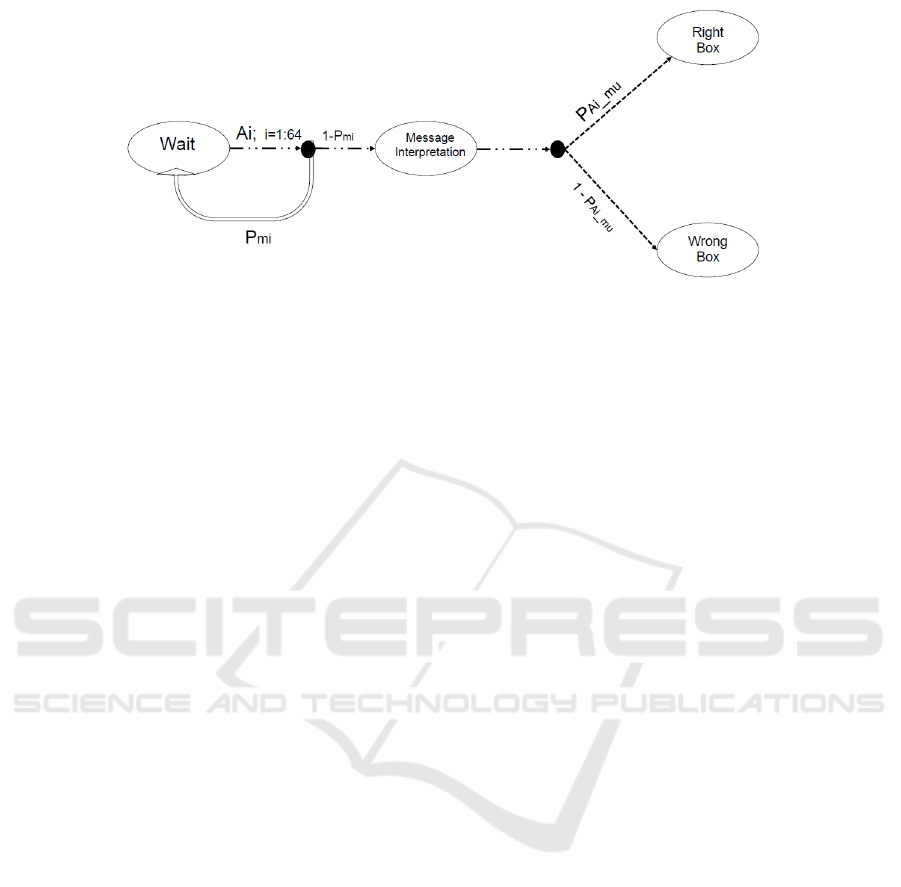
Figure 3: The Reinforcement Learning block.
The terms P(x|θ)P(θ) and prior P(θ) are likeli-
hood function which follows Bernoulli distribution
and Beta distribution. Sutton considers a similar prob-
lem of multi-armed bandit in his book (Sutton and
Barto, 1998) and he used Gaussian distribution. As
P(θ) Beta distributed and P(x|θ)P(θ) is Bernoulli
distributed, the term P(θ|x) is also Beta distributed
which is to say that when a patient reached to right
box then posterior will become Beta(α + 1, β) and if
patient reached to wrong box then posterior will be
Beta(α, β + 1). We use Thompson sampling (Prasad
et al., 2017) to solve the problem of exploration-
exploitation in which for each message, the probabil-
ity θ is sampled from the prior and then the message
with the highest sampled probability is selected. Fig-
ure 5 shows the convergence of 12 to different num-
bers of iterations.
4 DISCUSSION
We have implemented the proposed study in general
and have demonstrated our system for a specific treat-
ment plan which was advised by a clinician to a pa-
tient of hypertension as shown in table 2. The work-
ing of the proposed model is shown in figure 4. The
information from the planner to the RL agent con-
sists of drug name and time hour. Then the tutor
(RL agent) by using Thompson sampler decides how
to communicate with the patient about the scheduled
drug. As can be seen in figure 4, that agent can
send one or combination of the image of a scheduled
medicine, image of pill, scientific or simple name of
message through text or audio.
To explain better working of proposed system and
figure 4, let consider the table 2. According to this
treatment plan, the patient of hypertension need to
take drug Adalat Crono 30mg at 08 : 00 and 20 : 00
every day for a period of forty days. So at 08 : 00
and 20 : 00 each day, the system first learns the status
of the patient’s mental and physical skills separately
i.e. system does not use the information he learned at
08 : 00 for a drug which patient will take at 20 : 00. In
the second step, the system decides how to communi-
cate drug information to the patient. More precisely,
at 08 : 00 and 20 : 00, the system has to choose one
or combination of more than one out of the following
six.
- Scientific Audio Message as: take the ’Adalat
Crono 30mg’.
- Simple Audio Message as take ’the medicine
from the white, red and yellow box’ (this is a sample
message, one can set it to a more preferred and better
way).
- Scientific Visual Message as: simply send the
box image of the ’Adalat Crono 30mg’ as can be seen
in figure 4.
- Simple Visual Message as: simply send the pill
image of the ’Adalat Crono 30mg’ as can be seen in
figure 4.
- Scientific Text Message as: a text message like
this: ”take ’Adalat Crono 30mg’.” will appear on
screen e.g mobile phone or tablet of pepper robot
- Simple Text Message as: a text message like
this: ”take ’the medicine from the white, red and yel-
low box’.” will appear on screen e.g mobile phone or
tablet of pepper robot.
The next question is the choice of RL algorithms
for the current work. We have briefly introduced most
of the RL algorithms in the background section. We
have not compared our work with previous work as
according to our best knowledge to date, no work of
such nature exists before. This will be the first work
of its kind. So we tested different algorithms for our
work and set two performance metrics. One is the
Average Utility Distribution (AUD) of each 63 mes-
sages at message interpretation state and second is to
convergence time i.e number of iterations need to get
experimental probabilities given the initial probabili-
ties.
A Reinforcement Learning and IoT based System to Assist Patients with Disabilities
495
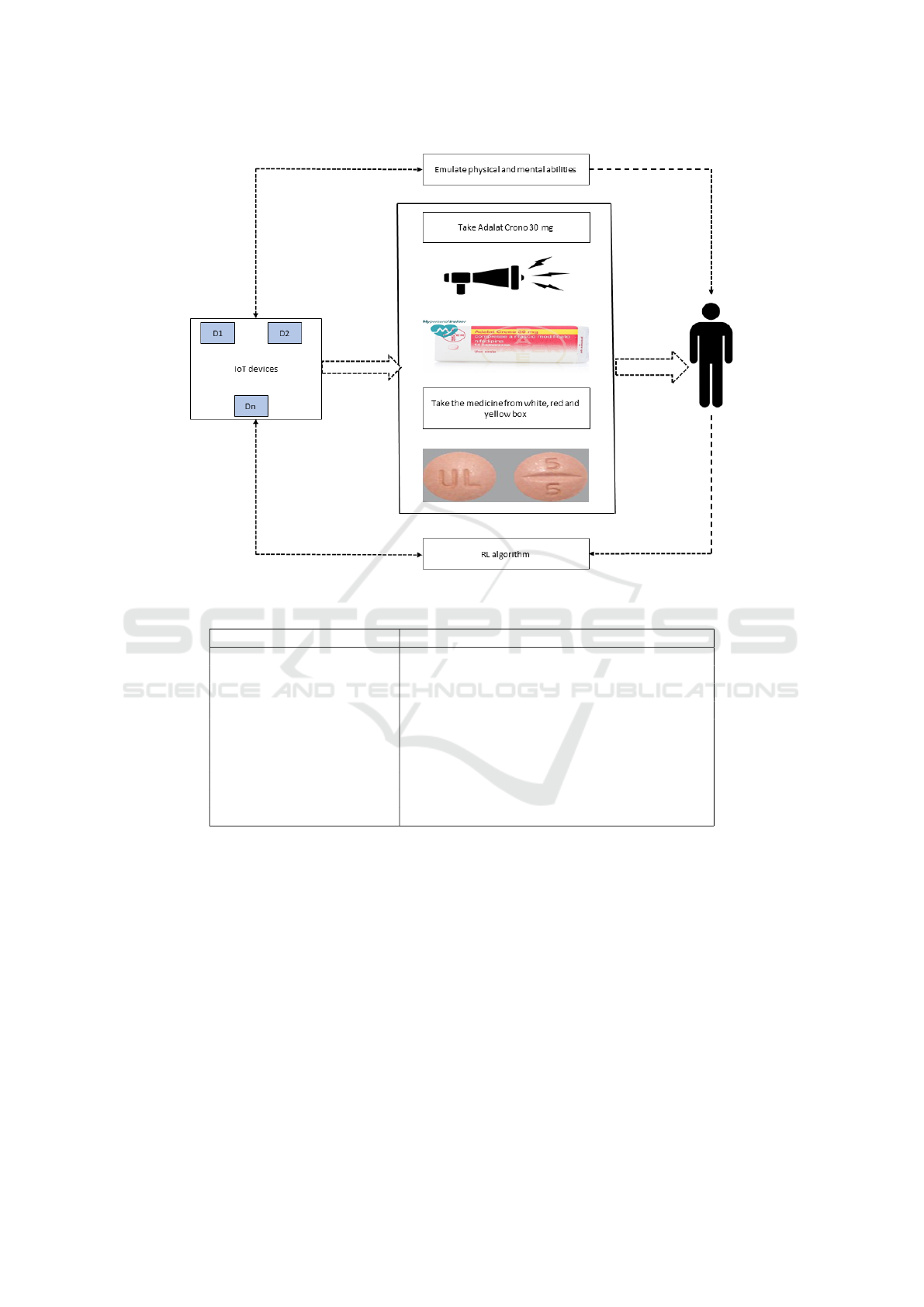
Figure 4: Working of the proposed model.
Table 2: Treatment plan for a patient of hypertension.
Medicines Time
Sp/ Duoplavin 75+100 mg 1 cp at 14:00 after lunch
Sp/ Torvast 80 mg 1 cp at 22:00
Sp/ Bisoprololo 1.25 mg 1 cp at 08:00
Sp/ Adalat crono 30 mg mg 1 cp at 08:00 and 22:00
Sp/ Prefolic 15 mg 1 cp at 14:00
Sp/ Sideral forte 1 cp at 13:00
Sp/ KCl retard 600 mg 1 cp ∗ 3
Sp/ Humulin R 4 UI after breakfast, 6 UI after lunch and dinner
Sp/ Spiriva respimat 1 puff at 18:00
Sp/ Pulmaxan 200 mcg 1 cp before breakfast
Moreover, as we have sixty-three available mes-
sages to choose one and in the future, this list can get
even bigger, it is important to have a delicate balance
between exploration and exploitation as explained in
the background section. Here we use Average Ag-
gregated Reward (AAR) and ’Root Mean Square Er-
ror (RMSE) to measure exploitation and exploration
respectively. When both RMSE and AAR are low
then the agent is doing exploration and exploit already
known actions when both RMSE and AAR have high
values.
As can be seen in table 3, the results of Thomp-
son sampling with Boltzman, Epsilon-decreasing,
Epsilon-greedy, Greedy, Random, and Softmax are
being compared and Thompson sampling has a com-
paratively better average reward. Similarly, in figure
5, we can see most of the actions need only a few
trials to reach an estimate of experimental probabili-
ties from initial probabilities. Furthermore, Thomp-
son sampling maintains a decent balance between ex-
ploitation and exploration as evident from row two
and three of table 3.
5 CONCLUSIONS
We have proposed a RL based system to provide clin-
ical support to patients having audio or visual or both
disabilities. The pill-reminder system is able to assist
AI4EIoTs 2020 - Special Session on Artificial Intelligence for Emerging IoT Systems: Open Challenges and Novel Perspectives
496
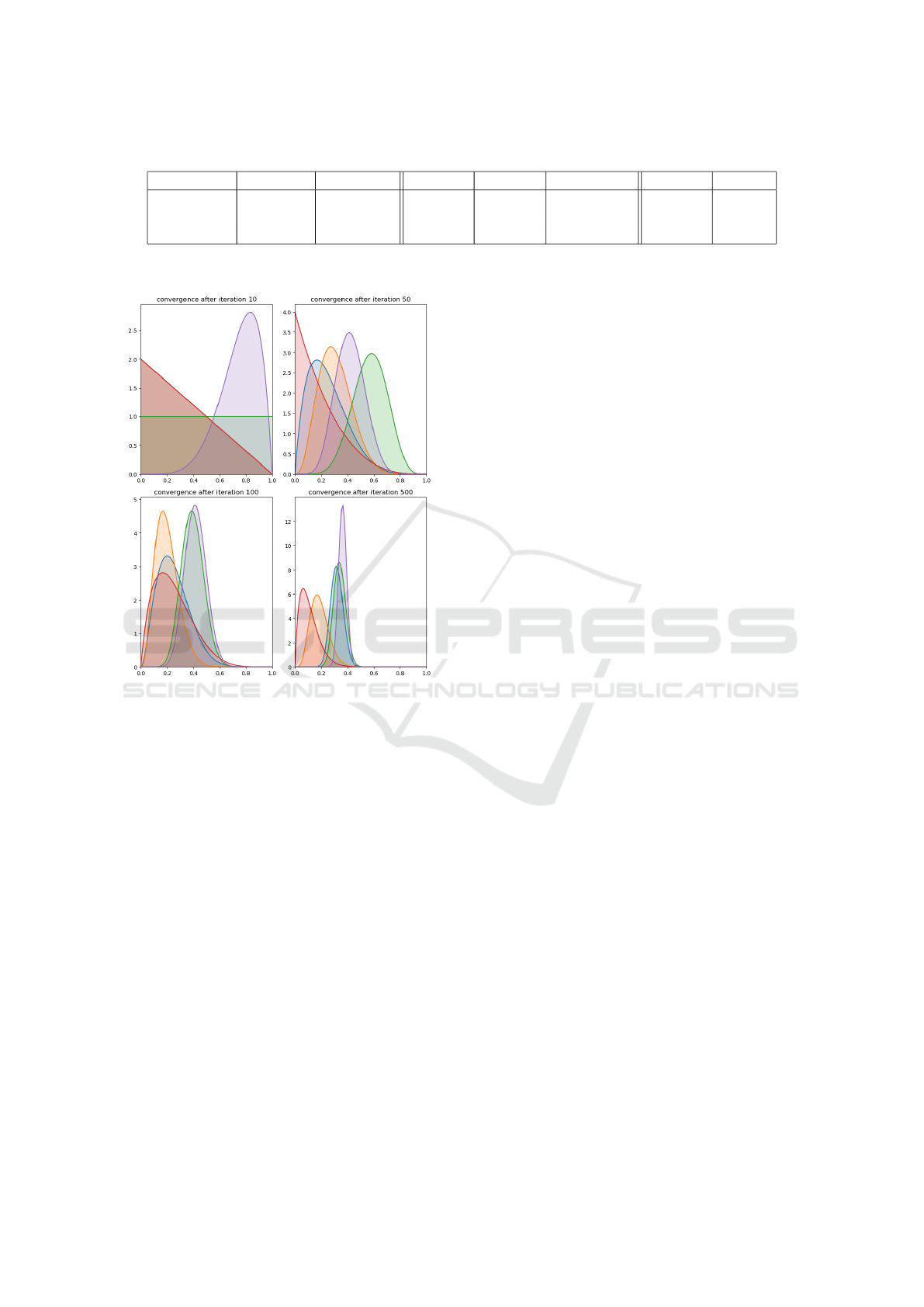
Table 3: Comparison of AUD, AAR and RMSE of different algorithms.
Algo =⇒ Boltzman Thompson Softmax Eps-Dec Eps-Greedy Random Greedy
AUD =⇒ 0.0156 0.9190 0.0642 0.04025 0.0668 0.4019 0.5199
AAR =⇒ 44.17 38.55 45.42 44.35 45.5 36.39 32.76
RMSE =⇒ 0.7522 0.2593 0.7023 0.7265 0.6986 0.3531 0.4557
Figure 5: Convergence at Different Numbers of Iterations.
patients with single audio, visual, textual or combi-
nation of more than one message choice out of six
types of message in their treatment plan. Depending
upon a patient’s disability, RL agent send an appropri-
ate type of message according to one’s schedule time
of treatment. In next version of our tutoring system
project, we will include implementation of proposed
work on interrelated computing devices i.e IoT sys-
tem and will try to generalize the proposal to more
complex scenarios.
ACKNOWLEDGEMENTS
This work is partially supported by AMICO project
which has received funding from the National Pro-
grams (PON) of the Italian Ministry of Education,
Universities and Research (MIUR):
code ARS0100900(DECREEN. 1989,26 July 2018).
REFERENCES
(2010). Automated handwashing assistance for persons
with dementia using video and a partially observable
markov decision process. Computer Vision and Image
Understanding, 114(5):503 – 519. Special issue on
Intelligent Vision Systems.
A Coronat0, G. De Pietro, G. P. A situation-aware system
for the detection of motion disorders of patients with
autism spectrum disorders. In Expert systems with ap-
plications 41 (17), 7868-7877.
A Coronato, G De Pietro, L. G. An agent based platform for
task distribution in virtual environments. In Journal of
Systems Architecture 54 (9), 877-882.
A Testa, A Coronato, M. C. J. A. Static verification of
wireless sensor networks with formal methods. In
2012 Eighth International Conference on Signal Im-
age Technology and Internet.
Antonio Coronato, Giovani Paragliola, M. N. G. D. P.
(2019). Reinforcement learning-based approach for
the risk management of e-health environments: A case
study.
Chakraborty, B., . M. E. E. Statistical methods for dynamic
treatment regimes.
D. F. Llorca, F. Vilarino, J. Z. G. L. (2007). A multi-class
svm classifier for automatic hand washing quality as-
sessment. Proc. of the British Machine Vision Confer-
ence.
Dearden, R., Friedman, N., and Andre, D. (2013). Model-
based bayesian exploration. CoRR, abs/1301.6690.
G Paragliola, A. C. Gait anomaly detection of subjects with
parkinson’s disease using a deep time series-based ap-
proach. In IEEE Access 6, 73280-73292.
Giovani Paragliola, M. N. (2019). Risk management for nu-
clear medical department using reinforcement learn-
ing.
Gullapalli N Rao, L. V. P. (2002). How can we improve
patient care?.
H. Kautz, L. Arnstein, G. B. O. E. D. F. (2002). An
overview of the assisted cognition project. In Proceed-
ings on the 2000 Conference on Universal Usability.
AAAI-2002 Workshop on Automation as Caregiver:
The Role of Intelligent Technology in Elder Care, Ed-
monton.
Kearns, M. J., Litman, D. J., Singh, S. P., and Walker, M. A.
(2011). Optimizing dialogue management with rein-
forcement learning: Experiments with the njfun sys-
tem. CoRR, abs/1106.0676.
Lavori, P. W., . D. R. (2004). Dynamic treatment regimes:
practical design considerations. clinical trials. 1(1).
A Reinforcement Learning and IoT based System to Assist Patients with Disabilities
497

Ling, Y., Hasan, S. A., Datla, V. V., Qadir, A., Lee, K.,
Liu, J., and Farri, O. (2017). Learning to diagnose:
Assimilating clinical narratives using deep reinforce-
ment learning. In IJCNLP.
Llorca, D. F., Parra, I., Sotelo, M.
´
A., and Lacey, G. (2011).
A vision-based system for automatic hand washing
quality assessment. Machine Vision and Applications,
22(2):219–234.
M.A.Sc., A. M., P.Eng., Ph.D., G. R. F., P.Eng., Ph.D., J.
C. B., and C.Eng. (2001). The use of artificial intel-
ligence in the design of an intelligent cognitive ortho-
sis for people with dementia. Assistive Technology,
13(1):23–39.
Mozer, M. C. (2005). Lessons from an Adaptive Home,
chapter 12, pages 271–294. John Wiley Sons Ltd.
Muddasar Naeem, Antonio Coronato, G. P. G. D. P. (2020).
A cnn based monitoring system to minimize medica-
tion errors during treatment process at home.
Murphy, S. A., Oslin, D. W., Rush, A. J., and Zhu, J. (2006).
Methodological challenges in constructing effective
treatment sequences for chronic psychiatric disorders.
Neuropsychopharmacology, 32(2):257–262.
Mynatt, E. D., Essa, I., and Rogers, W. (2000). Increasing
the opportunities for aging in place. In Proceedings
on the 2000 Conference on Universal Usability, CUU
’00, pages 65–71, New York, NY, USA. ACM.
Oliver, N., Garg, A., and Horvitz, E. (2004). Layered rep-
resentations for learning and inferring office activity
from multiple sensory channels. volume 96, pages
163–180. Elsevier.
Patel, V. L., Shortliffe, E. H., Stefanelli, M., Szolovits, P.,
Berthold, M. R., Bellazzi, R., and Abu-Hanna, A.
(2009). The coming of age of artificial intelligence in
medicine. Artificial Intelligence in Medicine, 46(1):5
– 17. Artificial Intelligence in Medicine AIME’ 07.
Petersen, B. K., Yang, J., Grathwohl, W. S., Cockrell, C.,
Santiago, C., An, G., and Faissol, D. M. (2018). Preci-
sion medicine as a control problem: Using simulation
and deep reinforcement learning to discover adaptive,
personalized multi-cytokine therapy for sepsis. CoRR,
abs/1802.10440.
Pineau, J., Montemerlo, M., Pollack, M., Roy, N., and
Thrun, S. (2003). Towards robotic assistants in nurs-
ing homes: Challenges and results.
Prasad, N., Cheng, L., Chivers, C., Draugelis, M., and En-
gelhardt, B. E. (2017). A reinforcement learning ap-
proach to weaning of mechanical ventilation in inten-
sive care units. CoRR, abs/1704.06300.
Reinkensmeyer, D. J., Guigon, E., and Maier, M. A. (2012).
A computational model of use-dependent motor re-
covery following a stroke: Optimizing corticospinal
activations via reinforcement learning can explain
residual capacity and other strength recovery dynam-
ics. Neural networks : the official journal of the Inter-
national Neural Network Society, 29-30:60–9.
Ross, C. K., Steward, C. A., and Sinacore, J. M. (1993). The
importance of patient preferences in the measurement
of health care satisfaction. Medical care, pages 1138–
1149.
Russell, S. and Norvig, P. (2009). Artificial Intelligence: A
Modern Approach. Prentice Hall Press, Upper Saddle
River, NJ, USA, 3rd edition.
Sahba, F., Tizhoosh, H. R., and Salama, M. M. A. (2006). A
reinforcement learning framework for medical image
segmentation. In The 2006 IEEE International Joint
Conference on Neural Network Proceedings, pages
511–517.
Strens, M. J. A. (2000). A bayesian framework for re-
inforcement learning. In Proceedings of the Seven-
teenth International Conference on Machine Learn-
ing, ICML ’00, pages 943–950, San Francisco, CA,
USA. Morgan Kaufmann Publishers Inc.
Suresh, H., Hunt, N., Johnson, A. E. W., Celi, L. A.,
Szolovits, P., and Ghassemi, M. (2017). Clinical inter-
vention prediction and understanding using deep net-
works. CoRR, abs/1705.08498.
Sutton, R. S. and Barto, A. G. (1998). Reinforcement Learn-
ing: An Introduction. MIT Press.
Thall, P. F. and Wathen, J. K. (2005). Covariate-
adjusted adaptive randomization in a sarcoma trial
with multi-stage treatments. Statistics in Medicine,
24(13):1947–1964.
Welling, M. and Teh, Y. W. (2011). Bayesian learning via
stochastic gradient langevin dynamics. In Proceed-
ings of the 28th International Conference on Inter-
national Conference on Machine Learning, ICML’11,
pages 681–688, USA. Omnipress.
Wren, C. R., Azarbayejani, A., Darrell, T., and Pentland,
A. (1997). Pfinder: Real-time tracking of the hu-
man body. IEEE Trans. Pattern Anal. Mach. Intell.,
19:780–785.
AI4EIoTs 2020 - Special Session on Artificial Intelligence for Emerging IoT Systems: Open Challenges and Novel Perspectives
498
