
Decentralized Electronic Health Records (DEHR): A Privacy-preserving
Consortium Blockchain Model for Managing Electronic Health Records
Mahdi Ghadamyari
a
and Saeed Samet
Department of Computer Science, University of Windsor, Windsor, Canada
Keywords:
Blockchain, Healthcare, Smart Contract, Hyperledger Fabric, Electronic Health Records.
Abstract:
Blockchain applications have proven the potential of this disruptive technology to achieve a disintermediated
model for improving efficiency and reducing the additional costs. The de facto healthcare applications suffer
from lack of interoperability, which is a result of using traditional centralized platforms that create private data
silos with poor interoperability and a high maintenance cost. In this paper, we introduce a blockchain-based
Decentralized Electronic Health Records (DEHR) model that enables healthcare providers to control their
electronic health records and share them among other organizations involved in the system in a secure and
consortium manner.
1 INTRODUCTION
Lack of interoperability in healthcare systems not
only costs patients and health providers millions but
also costs lives. A survey by Deloitte in 2018
(”Stephanie Newkirchen, 2018) from 624 US pri-
mary care and specialty physicians shows that inter-
operability has remained the top demand from physi-
cians as 62 percent of physicians say that interoper-
ability needs improvement just as they said before in
a 2016 survey. Another survey by Deloitte in 2018
(sur, 2018), reported that 74 percent of the more than
1,000 executives worldwide believe that their orga-
nizations see a ”compelling business case” for the
use of blockchain. These surveys demonstrate how
blockchain is changing the industry and the impor-
tance of having a compatible and interoperable health
care platform. However, healthcare is far behind from
modern technologies, especially when it comes to
leveraging new technologies such as blockchain.
Blockchain technology can be used to connect
health providers and facilitate data sharing within or-
ganizations. It adds transparency and immutability to
the data and enables the peer-to-peer transfer of digi-
tal assets such as Electronic Health Records (EHRs).
In this work, we introduce a model for managing
EHRs based on a consortium blockchain network. In
our model, organizations such as health providers can
register their staff and patients in the system and con-
a
https://orcid.org/0000-0003-2105-9901
trol access to the health records. Professionals can
request for limited or unlimited access to a patient’s
data. Also, other organizations can transfer a pa-
tient to their organization and take control of the pa-
tient’s health records. To make our model in compli-
ance with privacy acts, we utilize access control lists
(ACLs) and define policies to manage access to the re-
sources. We implemented and evaluated this model,
using several performance testing measures.
The rest of the paper is organized as follows: I) An
overview of similar works, II) Definitions, III) struc-
ture of our model, IV) Implementation and experi-
mental results V) Discussions VI) Conclusions.
2 RELATED WORK
Following, we briefly review some of the research
works related to blockchain adoption in health record
management systems.
The authors in (Azaria et al., 2016) proposed
a blockchain-based and decentralized health records
management system called MedRec. They used
a public blockchain that incentives researchers to
mine new blocks in exchange for getting access to
anonymized medical data. The authors claimed that
their proposed system increases the transparency of
medical records, the stability of the network, and
the confidentiality of data. The mining process is
necessary for having a secure network in public
blockchains; however, it is a time-consuming pro-
Ghadamyari, M. and Samet, S.
Decentralized Electronic Health Records (DEHR): A Privacy-preserving Consortium Blockchain Model for Managing Electronic Health Records.
DOI: 10.5220/0009398101990204
In Proceedings of the 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2020), pages 199-204
ISBN: 978-989-758-420-6
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
199

cess and requires a high computation power. Besides,
transaction processing time mainly depends on the
number of available miners willing to mine the pend-
ing transactions, which currently can take up to 5 min-
utes.
The MedRec (Azaria et al., 2016) work was later
continued by the authors in (Nchinda et al., 2019).
The authors replaced miners with a network of trusted
providers that participate in a proof of authority con-
sensus mechanism. They used blockchain to store
permission contracts. In their work, providers can
join the network and grant patients, and other entities
access to their databases using their credentials.
The authors in (Mikula and Jacobsen, 2018) used
a federated and private blockchain to explore an
auditable identity and access management frame-
work for EHR systems. Evaluation of their system
showed a size of 3.8 MB for the initialization of the
blockchain with 2-3 seconds of mining time for new
transactions.
The authors in (Chen et al., 2019) presented an in-
tegration of a cloud and blockchain storage scheme to
manage PHR data. They used off-chain cloud stor-
age for storing a large amount of medical data and the
blockchain for indexing and securing them. In their
work, patients are in control of their data. However,
the interoperability of their system is not examined.
In (Abouzahra, 2019), the authors proposed an in-
teractive model for a blockchain-based PHR system.
In the proposed system, smart contracts are utilized to
collect patients’ health records, and blockchain tech-
nology is used to make transactions immutable and
traceable. The authors claimed that their approach
encourages physicians to have more engagement with
their patients outside clinics resulting in better care
delivery.
3 DEFINITIONS
There are two types of blockchains: permissionless
(public) and permissioned (private/consortium) (Al-
hadhrami et al., 2017). Depending on the need, each
blockchain type has its advantages and disadvantages.
In public blockchains, anyone can join the net-
work, invoke transactions, write new blocks, and con-
tribute to the maintenance of the network. On the one
hand, this feature adds transparency to the data and
makes the data extremely secure and immutable. On
the other hand, redundancy in the network makes the
network slower and increases the maintenance cost,
significantly. Public blockchains are most suitable for
public digital assets such as cryptocurrencies, where
everyone needs access to read the ledger. However,
this level of transparency might endanger the pri-
vacy of users. Bitcoin(Nakamoto et al., 2008) and
Ethereum (Wood et al., 2014) are two well-known ex-
amples of public blockchains.
On the contrary, permissioned blockchains only
allow the pre-authorized participants to maintain the
ledgers and give access or add users to the network.
Permissioned blockchains can easily scale and have
significantly faster transaction processing time in ex-
change for the anonymity of the users. Further, since
the ledger is not open to the public, users in the net-
work have a higher level of privacy. Permissioned
blockchains can be categorized into two types: pri-
vate and consortium. In private blockchains, only one
participant has the right to add blocks to the chain or
allow others to read the transactions. In consortium
blockchains, a set of organizations control the consen-
sus process. Also, blocks can be added to the chain
only if the predefined nodes reach a consensus. For
an EHR system, a consortium blockchain is more ap-
pealing mainly because of the faster transaction pro-
cessing time and the higher level of privacy that it of-
fers to the participants in the system.
There are two major frameworks for deploying
a consortium blockchain network: 1) Quorum(quo,
2019), which is an enterprise-focused version of
Ethereum, and 2) Hyperledger Fabric(Androulaki
et al., 2018), a product by Linux Foundation which
is supported by enterprise companies like IBM, In-
tel, and SAP. In our work, we use Hyperledger Fabric
for model implementation because of its bigger com-
munity of developers, support from large enterprise
companies, and a wide variety of APIs.
There are five main concepts in a Hyperledger
Fabric model: assets, participants, transactions,
chaincodes, and access control lists (ACLs). Partic-
ipants are the users involved in the model, such as
patients and practitioners. Assets are tangible or in-
tangible properties that participants can own, such as
health records.
Transactions are abstract actions and trigger a
chaincode to modify the ledger. Chaincodes (or smart
contracts) are a set of procedures defined by the
blockchain network designer to process inputs and al-
ter the resources. Examples of transactions are trans-
ferring a patient to another organization or granting
permissions. Access control lists are a set of rules
that can be defined to control access to different oper-
ations on resources.
All permission managements are handled through
chaincodes and access control lists and are enforced
by all participating nodes in the network.
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
200
4 SYSTEM DESIGN
Our model is consists of three participant types, two
asset types, and three transactions. The three types
of participants are organizations, professionals, and
patients. The two types of assets are health records
and permission requests. The three transactions are
1) Patient transfer transaction: for transferring a pa-
tient to another organization, 2) Permission request
transaction: for requesting access to health records,
and 3) Change permission request status transaction:
To grant or deny a permission request.
Organizations can create records for their patients
or transfer an already existing patient in the system by
sending a transfer transaction. In the following sec-
tions, we will describe each part in detail.
4.1 Health Record Asset
Health records are consisting of five parameters:
health record ID, record type, details, and links to the
patient and the organization.
Health record ID is the default identifier of the
record. Record type determines the type of the record
and is naturally an enumerated type. Examples of
record types are identity, prescriptions, lab results,
vaccinates, etc. Detailed information related to the
record, such as medicine and dosage, will be stored
in the ”Details” parameter. Listing 1 shows a sample
health record.
Listing 1: A Sample Health Record.
{
" $class ": " org . DEHR . H ealth R e cord " ,
" h e a lthRe c o rdId ": "577" ,
" re c o r dType ": " IDEN T I T Y " ,
" details ": "{ SIN : 1 11111111 , F a t h e r : ’
Bob ’}" ,
" patient ": " r e s ource : or g . DEHR . P atient
#1" ,
" or g a nizat i o n ": " resour c e : org . D EHR .
Org a n izati o n #2"
}
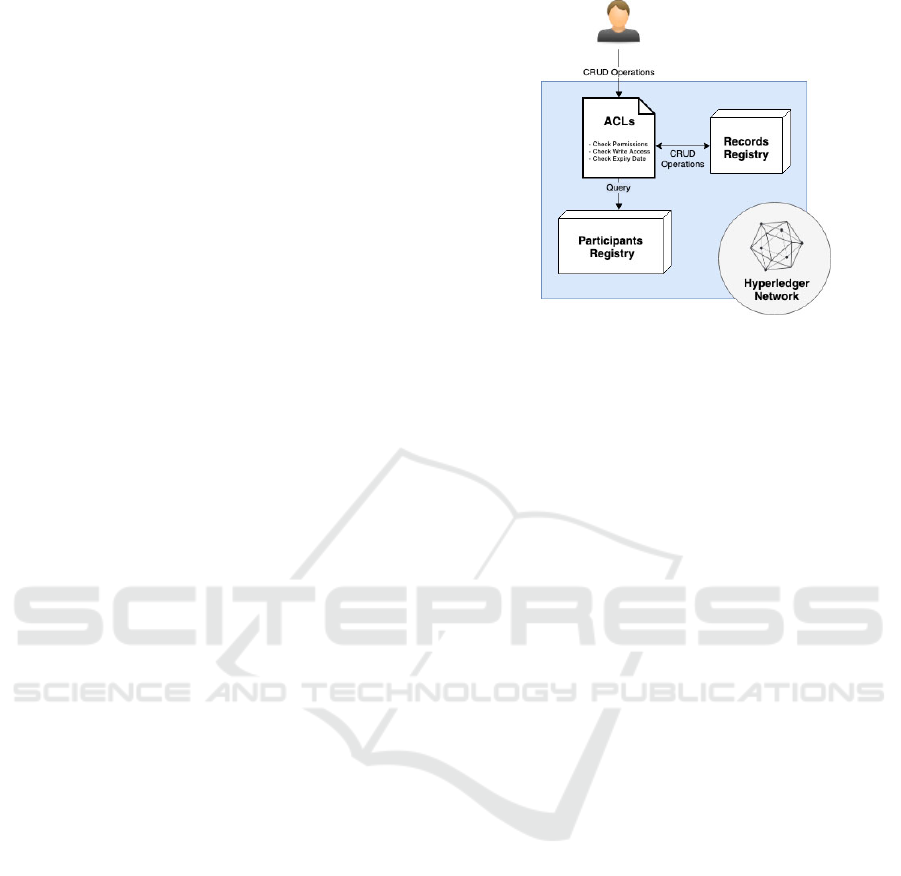
Permissions for CRUD (Create, Read, Update,
Delete) operations on health records will be con-
trolled by Hyperledger Access Control Lists (ACLs).
Upon submitting an operation, an ACL script will be
executed to verify that the participant has the permis-
sion to run that operation. Figure 1 shows the flow for
CRUD operations on health records.
4.2 Permission Request Transaction
To access health records, professionals must have re-
quired permissions. Permissions can be granted by
Figure 1: CRUD Operation Flow for a Health Record.
the organization that the patient is associated with.
There are five parameters that need to be determined
prior to send a permission request:
1. Record Types: Various types of health records can
be created for a patient. It is essential to grant
permissions based on their types to preserve pri-
vacy. As part of a permission request, profession-
als may determine what record types they need to
have access to using this parameter. A null value
for this parameter grants the professional access
to all types of records belong to that patient.
2. Write Access: This parameter determines whether
the professional should have access to add a new
record or modify an already existing record for the
patient in question. This parameter, along with the
record types parameter, will be used by the access
control rules to determine the write access for a
professional.
3. Status: Permissions can be denied, granted, or
revoked. This parameter determines the current
state of permission, which by default is set to
”Pending”.
4. Expiry Date: A permanent access to a health
record might not always be desired. This param-
eter can be defined to determine an expiry date
for the associated permission. Expirations will be
enforced by access control rules embedded in the
blockchain, automatically.
5. Patient: The patient that owns the health record
will be linked in this parameter. Chaincodes and
access control rules use this parameter to access
the patient.
By calling the ”RequestPermission” transaction
with the above parameters, a new ”Permission Re-
quest” asset will be instantiated and assigned to the
professional participant (Listing 2). By using the Hy-
perledger events feature, organizations and patients
Decentralized Electronic Health Records (DEHR): A Privacy-preserving Consortium Blockchain Model for Managing Electronic Health
Records
201

can be automatically notified about the new permis-
sion request.
Listing 2: A sample permission request transaction.
{
" $class ": " org . dehr . R equ e s tPer m i ssio n
" ,
" pe r m i ssion ": {
" $class ": " org . dehr . P ermissi o n " ,
" re c o r dType ": [" M E D ICATIO N "] ,
" wr i t eAcces s ": true ,
" patient ": " r e s ource : or g . dehr .
Patient #10"
} ,
" pr o f essio n a l ": " resour c e : org . d ehr .
Pro f e ssion a l #1"
}
After submitting a permission request, the orga-
nization that controls the health record(s) can either
accept or deny the request by calling the ”ChangePer-
missionStatus” transaction. (Listing 3).
Listing 3: A sample respond to a permission request.
{
" $class ": " org . dehr .
Ch a n geP e rmis s ionS t atus " ,
" p e r miss i o nRe q u est ": " res o u r c e : org .
dehr . Pe r m issi o n Req u e st #1" ,
" status ": " GRANTED "
}
This transaction triggers a set of chaincodes to up-
date the status of the related permission request asset
and also add or remove the permission from the pro-
fessional participant’s record.
4.3 Transfer Patient Transaction
To transfer a patient, organizations can invoke the
”TransferPatient” transaction. Listing 4 shows a sam-
ple ”TransferPatient” transaction that transfers the pa-
tient to another organization.
Listing 4: A sample transfer request transaction.
{
" $class ": " org . dehr . T rans f e rPat i e nt " ,
" patient ": " r e s ource : or g . dehr . P atient
#2" ,
" or g a nizat i o n ": " resour c e : org . d ehr .
Org a n izati o n #4"
}
4.4 Access Control Lists
Access Control Lists (ACLs) can be used to manage
access to different operations (Read, Write, Update,
and Delete) on resources. We use ACLs to enforce
permissions declared by chaincodes and stored in par-
ticipants and assets records. Listing 5 shows a sample
ACL function that permits authorized professionals
reading access to health records. The function vali-
dates the record type, patient, and expiry date of the
permission and returns a boolean, which determines
the final decision.
Listing 5: ACL for granting authorized professionals read
access to health records.
funct i o n h e a lthR e c ords A C L (
professional , r e c o r d ) {
return p r ofess i o n al .
gr a n ted P e rmis s i ons . some (
funct i o n ( gr a n tedP e r mis s i on ) {
const pe r m i ssion =
gr a n tedP e r mis s i on . pe r m i ssion ;
return (
per m i s sion . r e c o r dType . i n d e x O f (
record . re c o r dType ) >= 0 &&
per m i s sion . patie n t .
ge t I d enti f i e r () === r e c o r d .
patient . g e tIde n t i fier () &&
(! p e r missio n . e x piryDa t e ||
new D ate () < new Date (
per m i s sion . e x p i r yDate .
getTime () ))
) ;
}) ;
}
5 EXPERIMENTAL RESULTS
We implemented the model using Hyperledger Com-
poser and Hyperledger Fabric framework. The model
includes chaincodes for the three transactions that
were discussed in the previous section, access rules,
and the business model. We performed several per-
formance testings to evaluate the scalability and re-
sponse time of different features of our platform. We
used an OS X machine with a 3.5 GHz Intel Core i7
CPU and 16 GB 2133 MHz LPDDR3 memory during
our experiments.
We created a blockchain database with an entry
of 10,000 patients. In this database, a single query
from the patients’ registry took 252 ms, and calling
the patient transfer transaction took 2399ms to pro-
cess. We extended the experiment and simulated up
to 100 concurrent users and computed the median re-
sponse times of the network [Figure 2]. The experi-
ment shows a faster growth in transaction processing
time with an increase in the number of active users.
This behavior shows that the mining process takes
more time with an increase in the number of pending
transactions.
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
202
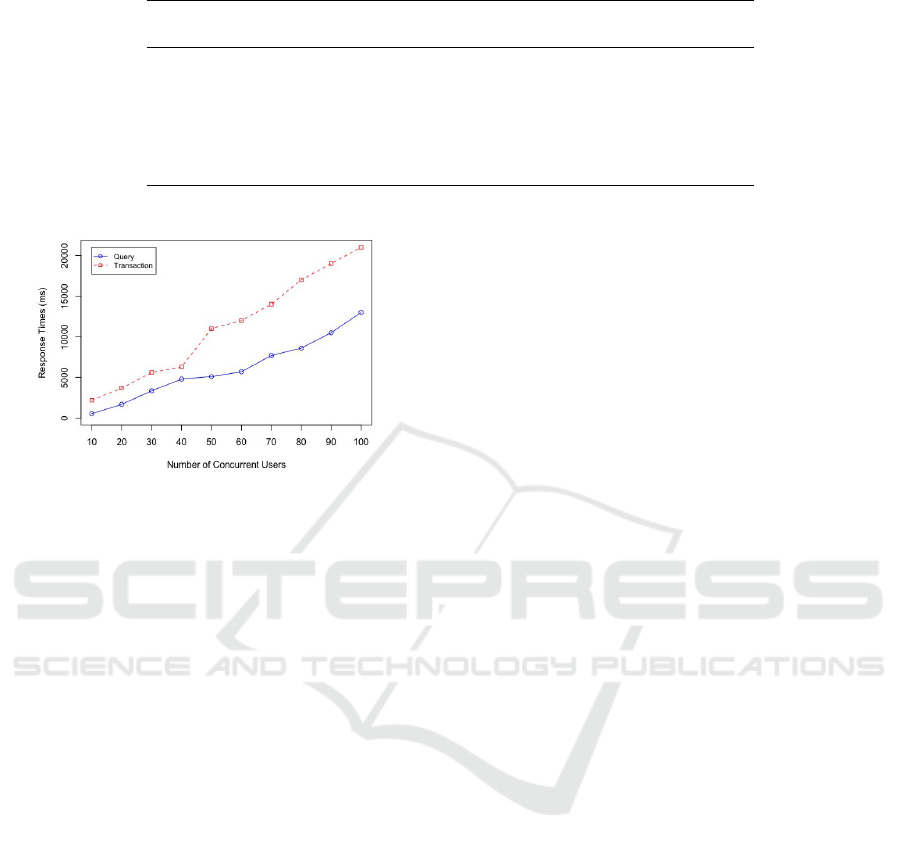
Table 1: Performance Results Based on the Number of Entries (N).
Action Mean ± Standard Deviation (s)
N < 6k N ∈ [6k, 10k] N ∈ [10k, 14k]
Add patient 2.512 ± 0.072 2.521 ± 0.041 2.523 ± 0.038
Delete patient 2.508 ± 0.054 2.522 ± 0.053 2.508 ± 0.051
Transfer patient 2.380 ± 0.037 2.381 ± 0.039 2.379 ± 0.035
Request permission 2.477 ± 0.074 2.435 ± 0.0435 2.426 ± 0.047
Grant permission 2.470 ± 0.924 2.455 ± 0.126 2.373 ± 0.353
Query patient 0.154 ± 0.021 0.156 ± 0.018 0.157 ± 0.019
Figure 2: Query and Transaction Processing Time per Ac-
tive User for the Proposed EHR Model.
In the next experiment, we gradually added
14,000 of various resources in the network and com-
puted the average response time of sending queries
and invoking transactions.
The result [Table 1] shows a relatively consistent
response time, which indicates that the number of
stored records does not remarkably affect the process-
ing time of mining a new block.
6 DISCUSSION
The immutability of data can be considered as one of
the most important features of blockchains. Blocks
are chained and secured with hashes to immune the
ledger against any manipulations. However, this may
not always be an acceptable feature. Many privacy
acts grant patients the right to correct their data or
to instruct health information custodians not to share
their personal health information with others. In pub-
lic blockchains that ledgers are shared and open to the
public, one approach to comply with privacy acts is to
store identifiable data in a separate secure database
and only store anonymized data in blockchains and
linking them using a unique identifier. This approach
is used in MedRec (Azaria et al., 2016). In private
blockchains, access to health records can be precisely
controlled and granted only with the consent of pa-
tients. Besides, while the history of a ledger cannot be
modified, access to the history of changes can be man-
aged and restricted to the patient. Another approach
is to use the private data feature offered in the Hy-
perledger Fabric platform. Hyperledger fabric stores
a hash of the private data on the public ledger as a
shred of evidence for the existence of the data. Later,
private data can be destroyed by the authorized au-
thorities and become inaccessible permanently from
the blockchain.
7 CONCLUSIONS
In this work, we proposed a Privacy-Preserving De-
centralized EHR platform based on a permissioned
blockchain framework. In our model, different orga-
nizations involved in the health care industry can join
the network; they can add their staff and patients in
the network and manage the electronic health records.
We have introduced chaincodes for transferring a pa-
tient, controlling access to health records based on
record types, and access controls for automatically re-
voking permissions after their expiry date. In future
works, we will further examine the scalability of our
model, try to improve the efficiency and investigate
solutions for integration of legacy systems with the
proposed model.
REFERENCES
(2018). Deloitte survey: For blockchain-savvy executives,
movement expected over next year and ’pragmatism’
the new mindset. https://www.prnewswire.com/news-
releases/deloitte-survey-for-blockchain-savvy-
executives-movement-expected-over-next-year-and-
pragmatism-the-new-mindset-300648480.html.
(2019). Quorum. www.jpmorgan.com/global/Quorum.
Abouzahra, M. (2019). Using blockchain technology to en-
hance the use of personal health records.
Alhadhrami, Z., Alghfeli, S., Alghfeli, M., Abedlla, J. A.,
and Shuaib, K. (2017). Introducing blockchains for
Decentralized Electronic Health Records (DEHR): A Privacy-preserving Consortium Blockchain Model for Managing Electronic Health
Records
203

healthcare. In 2017 International Conference on Elec-
trical and Computing Technologies and Applications
(ICECTA), pages 1–4. IEEE.
Androulaki, E., Barger, A., Bortnikov, V., Cachin, C.,
Christidis, K., De Caro, A., Enyeart, D., Ferris, C.,
Laventman, G., Manevich, Y., et al. (2018). Hyper-
ledger fabric: a distributed operating system for per-
missioned blockchains. In Proceedings of the Thir-
teenth EuroSys Conference, page 30. ACM.
Azaria, A., Ekblaw, A., Vieira, T., and Lippman, A. (2016).
Medrec: Using blockchain for medical data access
and permission management. In 2016 2nd Inter-
national Conference on Open and Big Data (OBD),
pages 25–30. IEEE.
Chen, Y., Ding, S., Xu, Z., Zheng, H., and Yang, S. (2019).
Blockchain-based medical records secure storage and
medical service framework. Journal of medical sys-
tems, 43(1):5.
Mikula, T. and Jacobsen, R. H. (2018). Identity and access
management with blockchain in electronic healthcare
records. In 2018 21st Euromicro Conference on Digi-
tal System Design (DSD), pages 699–706. IEEE.
Nakamoto, S. et al. (2008). Bitcoin: A peer-to-peer elec-
tronic cash system.
Nchinda, N., Cameron, A., Retzepi, K., and Lippman,
A. (2019). Medrec: A network for personal infor-
mation distribution. In 2019 International Confer-
ence on Computing, Networking and Communications
(ICNC), pages 637–641. IEEE.
”Stephanie Newkirchen, N. E. (2018). Electronic health
records: Can the pain shift to value for physicians?
https://www2.deloitte.com/us/en/insights/industry/
health-care/ehr-physicians-and-electronic-health-
records-survey.html.
Wood, G. et al. (2014). Ethereum: A secure decentralised
generalised transaction ledger. Ethereum project yel-
low paper, 151(2014):1–32.
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
204
