
Swiss Francs Seem to Make Insured Move: Comparing Daily and
Monthly Financial Incentives of a Scalable Digital Health
Intervention
Gisbert W. Teepe
1a
and Tobias Kowatsch
1,2 b
1
Center for Digital Health Interventions, ETH Zürich, Zürich, Switzerland
2
Institute of Technology Management, University of St. Gallen, St. Gallen, Switzerland
Keywords: Observational Field Study, Physical Activity, Digital Health Intervention, Financial Incentives.
Abstract: Despite the widely known necessity to counteract the increase in physical inactivity, only small strides have
been achieved so far. Digital health interventions (DHIs) are proposed to reach both healthy and at-risk
populations on a large scale. However, designing scalable DHIs that are engaging in the long term remains a
challenge. Small financial incentives may help to achieve such long-lasting behaviour changes. This work
thusly investigates the effects of daily or monthly paid small financial incentives on step counts and goal
achievements in physical activity. Six-month observational field data of a physical activity DHI (PADHI),
offered by a Swiss health insurer, was used for this investigation. From 1623 contacted customers, 742
(45.7%) joined the PADHI. Step counts and times the challenging goal was reached were significantly higher
in the condition of daily paid incentives. The findings from objectively measure daily step counts and goal
achievements indicate better outcomes when incentives are paid daily. Further findings indicate the
importance of recording various physical activities and not only step counts.
1 INTRODUCTION
Despite various attempts and approaches, physical
inactivity remains an immense problem as a health
risk factor. At least 20% of the world’s population is
insufficiently active and doesn’t meet the
recommended 150 minutes of moderate-intensity or
75 minutes of vigorous-intensity aerobic physical
activity (PA) per week (Sallis et al., 2016). Findings
from further studies underline the necessity to
promote PA. These findings show that PA decreases
the risk of mortality (Lear et al., 2017), the risk of
noncommunicable diseases such as diabetes, cancer
or coronary heart diseases (Kyu et al., 2016; Lee et
al., 2012,), and the cox hazard ratio of cardiovascular
events and fractures (Harris et al., 2019). Western
societies are increasingly becoming older. One
problem of this demographic change is that older
people tend to suffer longer and more frequently from
sicknesses and chronic diseases. Therefore, a cost
a
https://orcid.org/0000-0002-2264-9797
b
https://orcid.org/0000-0001-5939-4145
increase in healthcare is imminent making affordable
and scalable changes in healthcare inevitable.
One frequently discussed solution is the use of
digital health interventions (DHI) delivered via
smartphones, wearable devices, or websites
(Kowatsch, Otto, Harperink, Cotti, & Schlieter,
2019). They inform individuals about their current
health condition and are capable of delivering
personalized interventions to the masses at low costs
(Steinhubl, Muse, & Topol, 2015; Troiano et al.,
2008).
However, reaching vulnerable individuals that
would most benefit from DHIs remains a key
challenge. This selection bias is even higher when
participation is voluntary and not "prescribed" by a
doctor (Chinn, White, Howel, Harland, &
Drinkwater, 2006). Furthermore, the maintenance of
these behaviour adjustments for a substantial amount
of time poses a difficult challenge (Finkelstein et al.,
2016).
A promising approach to attract and maintain
participation in DHIs is the use of financial
Teepe, G. and Kowatsch, T.
Swiss Francs Seem to Make Insured Move: Comparing Daily and Monthly Financial Incentives of a Scalable Digital Health Intervention.
DOI: 10.5220/0009396308270833
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 827-833
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
827

incentives. Studies using relatively large incentive
values of an average maximum amount of $ 20.75 per
week seem to effectively change the amount of PA
(Strohacker, Galarraga, & Williams, 2014). These
relatively high incentives improved different
objective measures of PA (Barte & Wendel-Vos,
2017), the number of times PA exercises attended
(Barte & Wendel-Vos, 2017; Mitchell et al., 2013;
Strohacker et al., 2014), and exercise behaviour
(Mitchell et al., 2013).
Unfortunately, different studies show that after
withdrawing incentives, the PA changes typically do
not sustain and therefore need to be paid over a long
time (Finkelstein et al., 2016; Harkins, Kullgren,
Bellamy, Karlawish, & Glanz, 2017; Patel, Asch,
Rosin, Small, Bellamy, Eberbach, et al., 2016; Patel,
Asch, Rosin, Small, Bellamy, Heuer, et al., 2016;
Patel et al., 2018). To provide these necessary
financial incentives on a large scale and for a long
time, a crucial feature would be to keep them
relatively small (Kramer, Tinschert, Scholz, Fleisch,
& Kowatsch, 2019). Relatively small financial
incentives having a significant impact on PA were
around $1 per day (Patel, Asch, Rosin, Small,
Bellamy, Heuer, et al., 2016; Shin et al., 2017;
Strohacker et al., 2015). In a cluster-randomized trial
study, small personal or charity financial incentives
(monthly payment between CHF 5.00 to 10.00) led to
an increase of PA (Kramer et al., 2019). Surprisingly,
participation and reached step goals declined even
while the study was running and incentives not yet
withdrawn. The authors argue that incentives may
need to be modified to counter this decline in
participation and achieve lasting changes in
behaviour. Accordingly, prior studies (Barte &
Wendel-Vos, 2017; Strohacker et al., 2014) showed
relatively stable effects as long as the participants
received financial incentives.
Against this background, this study aims to
propose and discuss different incentives schemes for
physical activity digital health interventions
(PADHIs). The research question of this study is
whether a small daily paid incentive or a small
monthly paid incentive leads to an improvement in
daily steps, daily step goal achievements, and a
attrition rate reduction.
The next section describes the characteristics of
the study population and the evaluated PADHI. We
then describe the methods of data analysis to answer
the research question. Afterwards, results of the six-
month observational field study are presented and
discussed. A summary concludes this paper.
2 METHOD
We cooperated with a large Swiss health insurer to
answer the research question. The insurer started to
offer a PADHI to their customers in 2015 (Kramer et
al., 2019). In the last quarter of 2018, an average of
10.530 (SD = 5547) daily steps were achieved by
13799 customers. Compared to all other self-service
health promotion interventions of the insurance this
PADHI has the most continuous users. Data for the 6-
month study of the current paper was collected from
a subset of these customers between April 1
st
and
September 30
th
2016.
Participants, that already participated in a
previous study by Kramer et al. (2019) were invited
by e-mail. Participants were required to be at least 18
years old, enrolled in the complimentary insurance
program (see Section 2.2 below), and had to accept
the terms of participation and privacy policy.
Furthermore, they had to confirm that they were not
under any medical treatment that forbid PA. Although
no eligibility criteria were defined on the canton
(federal state of Switzerland) state-level, all
participants that provided demographic information
resided in a German-speaking canton. In the
invitation text, a brief description of the initiative and
a link to the insurer’s platform with more detailed
information was provided. On the linked platform the
participants signed up and were asked to complete a
survey to collect demographic data such as gender,
age, and level of activity. In total 1632 individuals
that already participated in a previous study by
Kramer et al. (2019) were contacted for recruitment.
The institutional review board of the University of
St. Gallen, Switzerland, approved the study (HSG-
EC-2016-06-13-A).
2.1 Incentive Schemes
Participants received financial incentives if they
reached specific daily step goals. For the first three
months, participants received a monthly payment if
they reached the daily step goal averaged over the
entire month. They received CHF 10.00 if the average
daily step of the month was above 10000 steps or
received CHF 5.00 if they achieved at least 7500 steps
per day but didn’t reach the goal of 10000 steps per
day. Participants with an average daily step count
below 7500 didn’t receive any financial incentive.
After three months the incentive scheme was
changed. The participants received daily payments
for three months if they reached the same goals as
defined above. Participants reaching at least 10000
steps per day received a payment of CHF 0.40 on that
Scale-IT-up 2020 - Workshop on Best Practices for Scaling-Up Digital Innovations in Healthcare
828

day. Participants reaching 7500 steps per day but not
10000 steps per day received CHF 0.20 on that day.
Table 1 shows the paid financial incentives by the
goal that was achieved and the incentive scheme. Due
to these different financial schemes for the first and
last three months, all participants could earn a total
amount between CHF 33.00 and CHF 66.00
depending on their performance within each of the
parts.
Table 1: Incentive mechanisms of the evaluated PADHI.
Averaged
Daily Steps
Monthly Payment
(Apr-Jun)
Daily Payment
(Jul-Sep)
< 7500 CHF 0.00 CHF 0.00
7500 – 10000 CHF 5.00 CHF 0.20
> 10000 CHF 10.00
CHF 0.40
For two weeks after the first three months, no
financial incentive was paid. This break arose due to
a technical problem by switching from monthly to
daily payments, leading to no steps being recorded
within those two weeks. Unfortunately, this break
resulted in different amounts of data points for further
analysis. To address this, only the first 76 days within
every three months of the study were used for further
analysis.
2.2 Study Sample
Due to legal reasons, the PADHI could not be part of
the statutory health insurance program. It could only
be offered to insureds with a complimentary
insurance plan. It is important to take into
consideration, that 75% of the Swiss population is
enrolled in such an insurance plan (Eisler & Lüber,
2016).
2.3 Measures and Statistical Analysis
Participants recorded their daily steps via commercial
pedometers offered by Garmin, Jawbone, or Fitbit, or
a specific smartphone app by Fitbit. The app option
was offered because buying a compatible pedometer,
although at a reimbursed price, was the most cited
reason for non-participation (41%) of participants
that did not want to participate in a prior study by
Kramer et al. (2019). Demographic data were in
addition to the data from the pedometer measured via
a self-report questionnaire.
From the provided data the average daily step
count, the number of days the app was used, the last
day the app was used, and the dropout rate were
calculated. Depended two-tailed t-tests with and α-
level of 0.05 to compare the average daily step count,
and the number of days the 10000 or 7500 goal was
reached within each of the different financial
incentive scheme were used for statistical analysis.
For the initial description and some analyses, all
participants, that used the app at least once and had an
average step count that did not exceed four standard
deviations from the mean, were included. Average
step counts exceeding four standard deviations from
the mean were considered a technical fault or
personal manipulation. For further analyses,
participants not providing data for at least 150 days of
the study were excluded. This is corresponding to
non-participation of more than one month.
Participants were marked as a dropout if they
provided no data for at least one week and did not
provide any further data afterwards at any point until
the end of the study. These dropouts were still
included in the analysis as they provided at least 150
days of data, which can be considered to be sufficient
in the remaining window of time (Guertler,
Vandelanotte, Kirwan, & Duncan, 2015).
The effect of the two different incentive schemes
on the number of goals achieved was calculated by a
four-field Chi-Square Test, with an α-level of 0.05.
3 RESULTS
From initially 1632 contacted insurance members 742
(45.5%) signed up and provided at least one day of
data. Of these only one participant exceeded the mean
number of steps by four standard deviations, leaving
741 (45.4%) participants that met this criterion. Data
for at least 150 days was provided by 392 (24.0%)
participants. Table 2 compares the number of
participants and the dropout rate for all participants
and those providing at least 150 days of data. Except
the initial attrition considering the number of people
that were contacted, the dropout rate within the study
was 174 (23.5%) for the participants that used the app
at least once and 10 (2.6%) for the participants that
provided at least 150 days of data. Figure 1 shows the
attrition rate for all participants of the study and the
attrition rate for all participants of the study by gender
and age groups.
The following descriptions are for the 392
participants included in the analysis. Demographic
data was provided by 371 (94.6%) participants, 207
(55.8%) being males. The mean age was 46.4 (SD =
13.8) ranging from 21 to 92 years. An overview of the
analysed measures and their distribution are reported
in Figures 2 for averaged daily steps and Figure 3 for
reached goals within each financial incentive scheme.
Swiss Francs Seem to Make Insured Move: Comparing Daily and Monthly Financial Incentives of a Scalable Digital Health Intervention
829
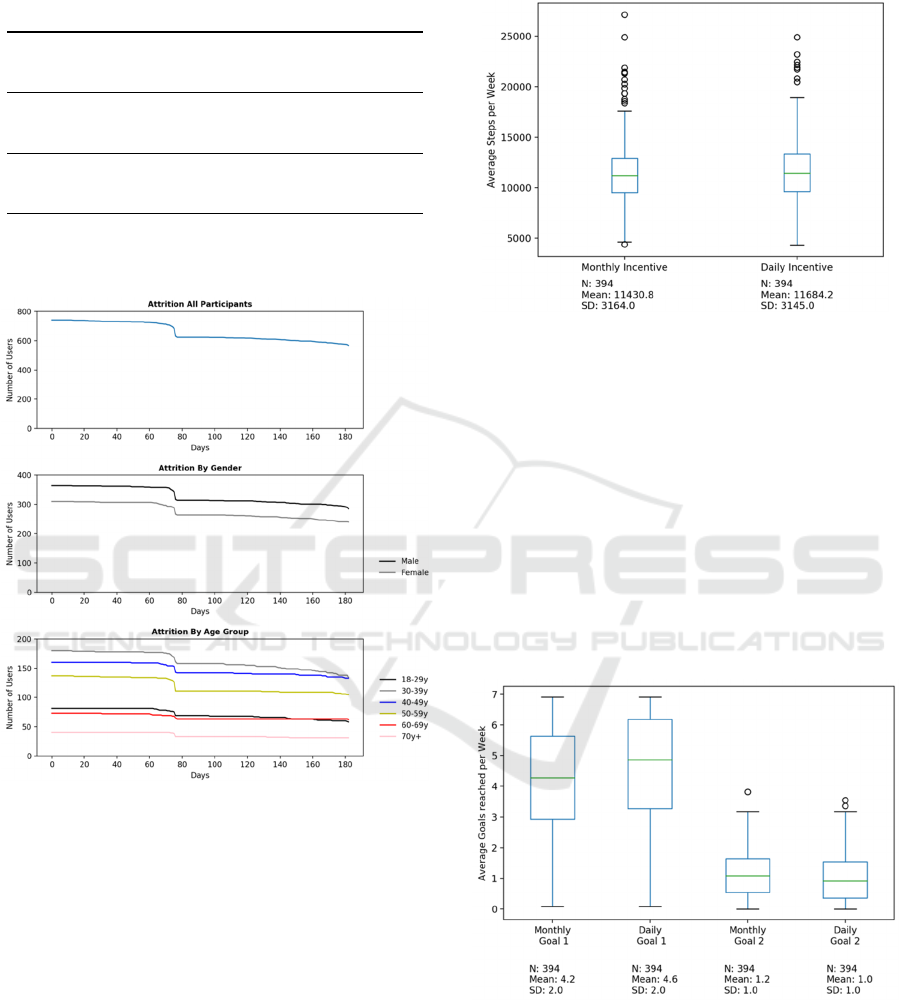
Table 2: Number (#) and attrition of participants.
Used DHI at
least once
Used DHI at
least 150 days
# participants at start
741
(54.5%)
392
(76%)
# participants after three
months
631
(14.8%)
392
(0%)
# participants after
incentive change
623
(15.9%)
392
(0%)
# participants after six
months (end of study)
567
(23.5%)
382
(2.6%)
Figure 1: Attrition for all participants that used the PADHI
and attrition for all participants that used the DHI by gender
or age.
There was a highly significant increase of average
daily step data from the monthly incentive payments
(M = 11552.8, SD = 2962.6) to the daily incentive
payments (M = 11971.9, SD = 3047.1), t(391) = 4.85,
p < .001. A significant increase from the average days
per week the 10000-step goals reached from the
monthly incentive payment (M = 4.1, SD = 1.8) to the
daily incentive payments (M = 4.6, SD = 1.8) was
observed, t(391) = 7.48, p < .001. The average
number of days per week the 7500-step goal was
reached significantly decreased from the monthly
incentive payments (M = 1.2, SD = 0.8) to the daily
incentive payments (M = 1.0, SD = 0.8), t(391) =
5.27, p < .001.
Figure 2: Distribution of weekly averaged steps counts by
financial incentive scheme.
The number of days the 10000 daily step goal was
reached significantly differed by which incentive
scheme was used, X
2
(1, N = 50270) = 167.9, p < .01.
The daily incentive scheme displays more days the
more challenging goal was reached (19739 number of
days for daily incentives vs 17973 for monthly
incentives). The number of days the 7500 daily step
goal was reached did not significantly differ by which
incentive scheme was used, X
2
(1, N = 21863) = 0.8,
p = .39. Figure 4 illustrates the number of days the
different goals were reached and the days the goals
were not reached.
Figure 3: Distribution of Weekly Averaged Reached Goals
by the financial incentive scheme (Goal 1 = 10000 daily
steps reached, Goal 2 = 7500 daily steps reached).
Scale-IT-up 2020 - Workshop on Best Practices for Scaling-Up Digital Innovations in Healthcare
830

Figure 4: Times the 10000 daily step goal, the 7500 daily
step goal, or no goal was reached by the incentive scheme.
4 DISCUSSION
This study investigates the effect of different financial
incentive schemes (monthly vs. daily payments) on
attrition, PA (measured by the number of steps), and
goal achievements of a large scale PADHI.
The percentage of people responding to the initial
recruitment was fairly good (45.5%). It is important
to take into consideration that participants were
recruited from a previous study investigating the effect
of DHIs. The number of participants that provided
sufficient data (at least 150 days of data) to be analysed
is in contrast low. Only 14% of the initially contacted
1623 participants met this criterion.
In contrast, within the 6-months of the study, the
attrition rate was very low compared to the prior work
by Kramer et al. (2019). Interestingly the two weeks
of no financial activity had almost no drop-out effect.
The attrition rate of the group that provided at least
150 days of data was only 2.6%. This finding could
be important for future work as it shows that frequent
users once engaged seem to consistently interact with
the DHI regardless of a break in the payment of the
financial incentive.
The results from analysing the average daily steps
made, the average number of times the more
challenging 10000 steps goal was reached per week,
and the total number of days the more challenging
10000 steps goal was reached seem to favour the daily
paid incentive. Only the average number of days per
week the less challenging 7500 steps goal was
reached seems to favour the monthly paid incentives.
The analysis revealed no significant difference for the
total amount of days the less challenging 7500 steps
goal was achieved. Due to the fact, that the number of
days the 10000 daily step goal was reached, was
higher over both financial incentive schemes it seems
that participants either aim high and in turn achieve
the higher goal or do not try to reach a goal and in turn
do not achieve any goal at all. For further research, it
could be interesting to investigate whether providing
only one goal has a positive effect due to the reduction
of the complexity or if more but very challenging
goals have a positive influence on PA and continuous
participation. Both approaches could be supported by
the theory of implementation intentions (Gollwitzer,
1999) stating that goals should be specific and
challenging. Taken this tendency to reach the higher
goal and the average steps made per week into
account the results suggest that a daily financial
incentive seems to have a positive effect on the
number of steps for every day.
The findings of the current work are limited in
several ways. First, it can be assumed that the
contacted individuals are already relatively active due
to the fact, that they participated in an earlier study
that investigated the use of DHI as well and that
voluntary PA initiatives, in general, tend to attract
people that are already sufficiently active and show
health-supportive behaviour.
Second, the findings of the current work may be
country or at least region-specific. It is, therefore,
possible that other countries are less or more open to
the use of tracking devices and digital coaching
applications.
Finally, causal inferences cannot be drawn from the
current study due to the nature of the observational
study design. Therefore, the results are limited in their
generalizability. They rather give interesting insights
into possible future studies investigating the differen-
ces between monthly and daily financial incentive
schemes that have the goal to increase physical.
5 SUMMARY
Relatively small daily paid financial incentives (CH
0.20 – 0.40) seem to lead to higher daily steps counts
compared to relatively small monthly paid financial
incentives (CH 5.00 – 10.00). Participants seemed to
aim for the higher goal or not bother to reach any goal
at all on that specific day. Future work should investi-
gate the importance of setting clear but ambitious
goals and financial incentives to further promote PA.
ACKNOWLEDGEMENTS
The authors would like to thank Jan-Niklas Kramer
and the two anonymous reviewers for their valuable
support and comments.
Swiss Francs Seem to Make Insured Move: Comparing Daily and Monthly Financial Incentives of a Scalable Digital Health Intervention
831

REFERENCES
Barte, J. C. M., & Wendel-Vos, G. C. W. (2017). A
Systematic Review of Financial Incentives for Physical
Activity: The Effects on Physical Activity and Related
Outcomes. Behavioral Medicine, 43(2), 79-90.
doi:10.1080/08964289.2015.1074880
Chinn, D. J., White, M., Howel, D., Harland, J. O. E., &
Drinkwater, C. K. (2006). Factors associated with non-
participation in a physical activity promotion trial.
Public Health, 120(4), 309-319. doi:10.1016/j.puhe.
2005.11.003
Eisler, R., & Lüber, A. (2016). Wie wichtig ist den
schweizern eine spitalzusatz- versicherung? . Retrieved
from www.comparis.ch/»/media/files/medien-corner/
studies/2006/krankenkassen/spitalzusatzversicherunge
n_studie.pdf.
Finkelstein, E. A., Haaland, B. A., Bilger, M.,
Sahasranaman, A., Sloan, R. A., Nang, E. E. K., &
Evenson, K. R. (2016). Effectiveness of activity
trackers with and without incentives to increase
physical activity (TRIPPA): a randomised controlled
trial. The Lancet Diabetes & Endocrinology, 4(12),
983-995. doi:10.1016/S2213-8587(16)30284-4
Gollwitzer, P. M. (1999). Implementation intentions: strong
effects of simple plans. American psychologist, 54(7),
493.
Guertler, D., Vandelanotte, C., Kirwan, M., & Duncan, M.
J. (2015). Engagement and Nonusage Attrition With a
Free Physical Activity Promotion Program: The Case
of 10,000 Steps Australia. Journal of Medical Internet
Research, 17(7), e176. doi:10.2196/jmir.4339
Harkins, K. A., Kullgren, J. T., Bellamy, S. L., Karlawish,
J., & Glanz, K. (2017). A Trial of Financial and Social
Incentives to Increase Older Adults’ Walking.
American Journal of Preventive Medicine, 52(5), e123-
e130. doi:10.1016/j.amepre.2016.11.011
Harris, T., Limb, E. S., Hosking, F., Carey, I., Dewilde, S.,
Furness, C., Cook, D. G. (2019). Effect of pedometer-
based walking interventions on long-term health
outcomes: Prospective 4-year follow-up of two
randomised controlled trials using routine primary care
data. PLOS Medicine, 16(6), e1002836.
doi:10.1371/journal.pmed.1002836
Kowatsch, T., Otto, L., Harperink, S., Cotti, A., & Schlieter,
H. (2019). A design and evaluation framework for digital
health interventions. it - Information Technology, 61(5-
6), 253-263. doi:10.1515/itit-2019-0019
Kramer, J. N., Tinschert, P., Scholz, U., Fleisch, E., &
Kowatsch, T. (2019). A Cluster-Randomized Trial on
Small Incentives to Promote Physical Activity. Am J
Prev Med, 56(2), e45-e54. doi:10.1016/j.amepre.
2018.09.018
Kyu, H. H., Bachman, V. F., Alexander, L. T., Mumford, J.
E., Afshin, A., Estep, K., Forouzanfar, M. H. (2016).
Physical activity and risk of breast cancer, colon cancer,
diabetes, ischemic heart disease, and ischemic stroke
events: systematic review and dose-response meta-
analysis for the Global Burden of Disease Study 2013.
BMJ, i3857. doi:10.1136/bmj.i3857
Lear, S. A., Hu, W., Rangarajan, S., Gasevic, D., Leong, D.,
Iqbal, R., Yusuf, S. (2017). The effect of physical
activity on mortality and cardiovascular disease in
130 000 people from 17 high-income, middle-income,
and low-income countries: the PURE study. The
Lancet, 390(10113), 2643-2654. doi:10.1016/s0140-
6736(17)31634-3
Lee, I. M., Shiroma, E. J., Lobelo, F., Puska, P., Blair, S.
N., & Katzmarzyk, P. T. (2012). Effect of physical
inactivity on major non-communicable diseases
worldwide: an analysis of burden of disease and life
expectancy. The Lancet, 380(9838), 219-229.
doi:10.1016/s0140-6736(12)61031-9
Mitchell, M. S., Goodman, J. M., Alter, D. A., John, L. K.,
Oh, P. I., Pakosh, M. T., & Faulkner, G. E. (2013).
Financial Incentives for Exercise Adherence in Adults.
American Journal of Preventive Medicine, 45(5), 658-
667. doi:10.1016/j.amepre.2013.06.017
Patel, M. S., Asch, D. A., Rosin, R., Small, D. S., Bellamy,
S. L., Eberbach, K., Volpp, K. G. (2016). Individual
Versus Team-Based Financial Incentives to Increase
Physical Activity: A Randomized, Controlled Trial.
Journal of General Internal Medicine, 31(7), 746-754.
doi:10.1007/s11606-016-3627-0
Patel, M. S., Asch, D. A., Rosin, R., Small, D. S., Bellamy,
S. L., Heuer, J., Volpp, K. G. (2016). Framing Financial
Incentives to Increase Physical Activity Among
Overweight and Obese Adults: A Randomized,
Controlled Trial. Annals of Internal Medicine, 164(6),
385-394. doi:10.7326/m15-1635
Patel, M. S., Volpp, K. G., Rosin, R., Bellamy, S. L., Small,
D. S., Heuer, J., Asch, D. A. (2018). A Randomized,
Controlled Trial of Lottery-Based Financial Incentives
to Increase Physical Activity Among Overweight and
Obese Adults. American Journal of Health Promotion,
32(7), 1568-1575. doi:10.1177/0890117118758932
Sallis, J. F., Bull, F., Guthold, R., Heath, G. W., Inoue, S.,
Kelly, P., Hallal, P. C. (2016). Progress in physical
activity over the Olympic quadrennium. The Lancet,
388(10051), 1325-1336. doi:10.1016/s0140-6736(16)
30581-5
Shin, D. W., Yun, J. M., Shin, J.-H., Kwon, H., Min, H. Y.,
Joh, H.-K., Cho, B. (2017). Enhancing physical activity
and reducing obesity through smartcare and financial
incentives: A pilot randomized trial. Obesity, 25(2),
302-310. doi:10.1002/oby.21731
Steinhubl, S. R., Muse, E. D., & Topol, E. J. (2015). The
emerging field of mobile health. Science Translational
Medicine, 7(283), 283rv283-283rv283. doi:10.1126/
scitranslmed.aaa3487
Strohacker, K., Galárraga, O., Emerson, J., Fricchione, S.,
Lohse, M., & Williams, D. (2015). Impact of Small
Monetary Incentives on Exercise in University
Students. American Journal of Health Behavior, 39.
doi:10.5993/AJHB.39.6.5
Strohacker, K., Galarraga, O., & Williams, D. M. (2014).
The Impact of Incentives on Exercise Behavior: A
Systematic Review of Randomized Controlled Trials.
Annals of Behavioral Medicine, 48(1), 92-99.
doi:10.1007/s12160-013-9577-4
Scale-IT-up 2020 - Workshop on Best Practices for Scaling-Up Digital Innovations in Healthcare
832

Troiano, R. P., Berrigan, D., Dodd, K. W., Masse, L. C.,
Tilert, T., & McDowell, M. (2008). Physical activity in
the United States measured by accelerometer. Med Sci
Sports Exerc, 40(1), 181-188. doi:10.1249/mss.0b013e
31815a51b3
Swiss Francs Seem to Make Insured Move: Comparing Daily and Monthly Financial Incentives of a Scalable Digital Health Intervention
833
