
CrowdHEALTH: An e-Health Big Data Driven Platform towards
Public Health Policies
Argyro Mavrogiorgou
1
, Athanasios Kiourtis
1
, Ilias Maglogiannis
1
, Dimosthenis Kyriazis
1
,
Antonio De Nigro
2
, Vicent Blanes-Selva
3
, Juan M. García-Gómez
3
, Andreas Menychtas
4
,
Maroje Sorić
5
, Gregor Jurak
5
, Mitja Luštrek
6
, Anton Gradišek
6
, Thanos Kosmidis
7
, Sokratis Nifakos
8
,
Konstantinos Perakis
9
, Dimitrios Miltiadou
9
and Parisis Gallos
10
1
Department of Digital Systems, University of Piraeus, Piraeus, Greece
2
Engineering Ingegneria Informatica SpA - R&D laboratory, Roma, Italy
3
Instituto de Tecnologías de la Información y Comunicaciones - BDSLab,
Universitat Politècnica de València, Valencia, Spain
4
BioAssist S.A., Athens, Greece
5
University of Ljubljana, Ljubljana, Slovenia
6
Department of Intelligent Systems, Jozef Stefan Institute, Ljubljana, Slovenia
7
Care Across Ltd, London, U.K.
8
Department Health Informatics Center, Karolinska Institutet, Stockholm, Sweden
9
Singular Logic EU projects department, Kifisia, Greece
10
European Federation for Medical informatics, Lausanne, Switzerland
amenychtas@bioassist.gr, {Maroje.Soric, Gregor.Jurak}@fsp.uni-lj.si, {mitja.lustrek, anton.gradisek}@ijs.si,
thanos.kosmidis@careacross.com, Sokratis.nifakos@ki.se, kperakis@ep.singularlogic.eu, dmiltiad@gmail.com,
parisgallos@yahoo.com
Keywords: CrowdHEALTH, e-Health Platform, Health Records, Health Policies, Health Analytics, Big Data.
Abstract: In today’s interconnected world, more health data is available than ever before, resulting into a rich digital
information environment that is characterized by the multitude of data sources providing information that has
not yet reached its full potential in eHealth. CrowdHEALTH introduces a new paradigm of Health Records,
the Holistic Health Records (HHRs), which offer the ability to include all this existing health data. To achieve
that, CrowdHEALTH seamlessly integrates big data technologies across the complete data path, providing its
results to the health ecosystem stakeholders, as well as to policy makers towards a “health in all policies”
approach. This paper describes the CrowdHEALTH architecture, summarizing all the mechanisms and tools
that have been developed and integrated in the context of CrowdHEALTH. The latter, along with the
experimentation with several use cases that provide diverse data from different sources, have provided useful
insights towards the successful and wide adaptation of the CrowdHEALTH platform in the healthcare domain.
1 INTRODUCTION
Information and data sharing across heterogeneous
healthcare systems, focusing on the management of
healthcare, nowadays have become the backbone of
modern delivery of sustainable healthcare services
and platforms (Ganguly, 2009). From routine patient
care to record keeping to requisite regulatory
compliance details, the healthcare industry generates
enormous amounts of directionless data, which on its
own does not hold any tangible value (Cohen, 2019).
At the same time, due to the explosion of all the
available information and communications
technology (ICT) services, there are several sensors
and applications supporting personalized care.
However, all these services and data are
heterogeneous and operate independently, resulting
into the limited exploitation of their emerging added-
value (The, 2019). Due to this inadequate integration
of the technology, as well as the large amount of data
being generated by the existing data sources, it is
getting increasingly common for important events to
be missed, such as the early identification of
development of diseases or the creation of inefficient
Mavrogiorgou, A., Kiourtis, A., Maglogiannis, I., Kyriazis, D., De Nigro, A., Blanes-Selva, V., García-Gómez, J., Menychtas, A., Sori
´
c, M., Jurak, G., Luštrek, M., Gradišek, A., Kosmidis, T.,
Nifakos, S., Perakis, K., Miltiadou, D. and Gallos, P.
CrowdHEALTH: An e-Health Big Data Driven Platform towards Public Health Policies.
DOI: 10.5220/0009388802410249
In Proceedings of the 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2020), pages 241-249
ISBN: 978-989-758-420-6
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
241

policies. On top of all these, today’s health records
(i.e. electronic - EHRs and personal - PHRs) are far
from being what the citizens consider as of value to
their health. This is consistent with the beliefs of 80%
of the public regarding health as more than being
disease-free (Edelman, 2011) and includes a variety
of everyday living aspects, such as the environment,
the active and fit lifestyle, the nutrition, the mental
and emotional health. Capturing this information, as
well as linking it with other data in EHRs and PHRs
would be of benefit for learning about outcomes of
prevention strategies and health policies, diseases,
and efficiency of patient pathway management. All
these highlight the opportunity of exploiting all the
existing amounts of healthcare data for achieving
effective and targeted policy making, development of
personalized medicine, and health promotion.
All these confirm the fact that nowadays there
exist a plethora of independent and heterogeneous
services, while health records are of limited value
since their data exploitation is limited as well. This
has resulted into ineffective and untargeted health
policies, fragmented health strategies and inefficient
personalized healthcare, highlighting the need for a
holistic approach to enable public health policies and
strategies and efficient medicine, health support and
disease prevention. In order to address this gap,
CrowdHEALTH platform (CrowdHEALTH, 2019)
envisions to incorporate technologies for a paradigm
shift from independent and heterogeneous services
and data sources, from limited data exploitation and
from health records that partially address the policy
domain, to complete integrated data views through
the Holistic Health Records (HHRs) (Kiourtis,
2019a). This is achieved based on the actual data
exploitation emerging from collective knowledge
(from HHRs clusters), and effective and targeted
health policies based on a set of health analytics tools.
Therefore, CrowdHEALTH explores mechanisms
that can be clustered across the main areas of the
holistic data services exploiting user knowledge, and
the efficient policy making across domains.
The rest of this paper is organized as follows.
Section 2 describes the overall CrowdHEALTH
architecture capturing all its components, in
combination with the interactions among them, so as
to achieve the integration of all the heterogeneous
existing health data towards the creation of successful
public health policies and strategies. Section 3
outlines the chosen use cases for evaluating the
applicability of the CrowdHEALTH platform in
different eHealth scenarios, while Section 4 depicts
all the users that are involved in the platform. Finally,
Section 5 states the conclusions and future work.
2 CrowdHEALTH
ARCHITECTURE
The CrowdHEALTH platform aims to deliver an
integrated ICT platform that provides decision
support to public health authorities for policy
creation, co-creation, and evaluation, through the
exploitation of collective knowledge that emerges
from multiple information sources and its
combination with situational awareness artefacts. The
platform incorporates big data management
mechanisms addressing the complete data path: from
acquisition, and cleaning, to data integration,
modelling, analysis, information extraction and
interpretation. What is more, CrowdHEALTH
provides various services to policy makers, enabling
them to utilize causal and risk stratification
mechanisms - combined with forecasting and
simulation tools, in order to develop multi-modal
targeted policies in terms of time scales (i.e. long- /
short- term), location properties (i.e. area, regional,
national, international), population segmentation (e.g.
patients of a specific disease, overnight workers, etc.),
and evolving risks (e.g. epidemics).
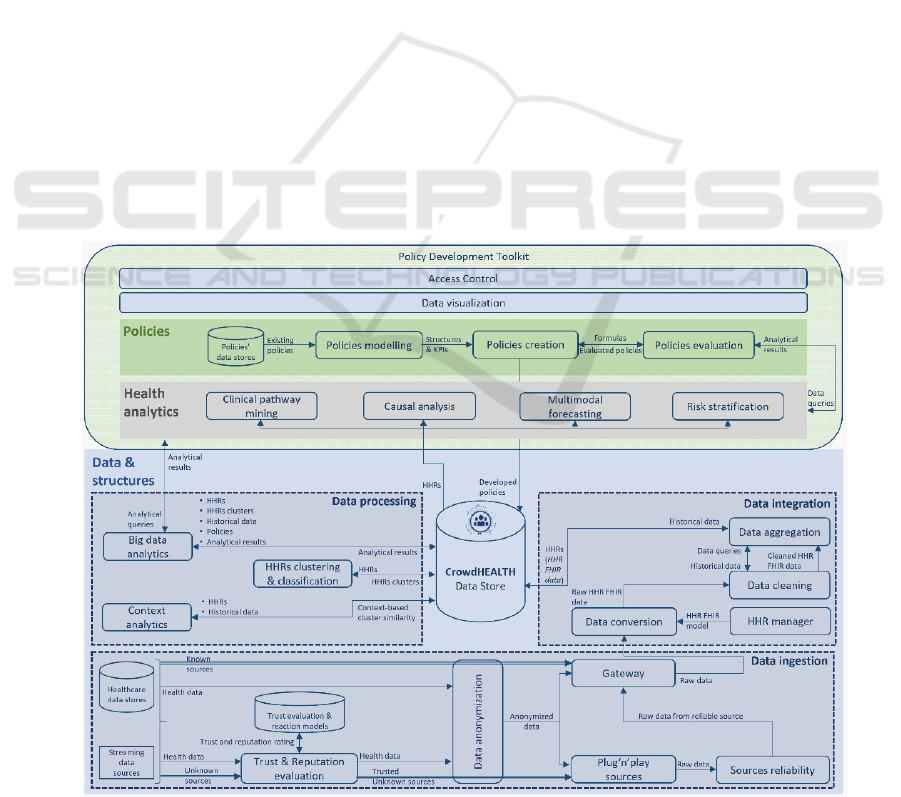
In order to offer all the aforementioned
capabilities, the overall architecture of the
CrowdHEALTH platform consists of three (3) main
pillars: (i) the Data & Structures, (ii) the Health
Analytics, and (iii) the Policies. Fig.1 illustrates the
final version of the CrowdHEALTH platform that is
an updated version of the architecture proposed in
(kBioAssist, 2017), reflecting all the components that
have been implemented in the context of the
CrowdHEALTH platform.
2.1 Data & Structures
In the context of Data & Structures, the whole pillar
is divided into three (3) sub-pillars: (i) Data ingestion,
(ii) Data integration, (iii) Data processing (Fig. 1).
Data Ingestion: The CrowdHEALTH platform is
able to take as an input either live data coming from
streaming data sources (i.e. unknown sources) or data
at rest that are already in diverse healthcare data
stores (i.e. known sources). For the known sources,
since these sources are fully trustful and reliable, the
nature of their data does not have to be checked.
However, with regards to the unknown sources, since
their nature and as a result their derived data may be
anomalous either from a technical point of view (e.g.
malfunctioning of a component) or from a security
point of view (e.g. malicious), these sources in
combination with their produced data are given as an
input into the Trust & Reputation evaluation
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
242
component. The latter retrieves by the existing trust
evaluation and reaction models’ datastore the
required trust and reputation ratings, in order to rank
the input unknown data sources into the trustfulness
list that finally decides whether these sources can be
connected into the CrowdHEALTH platform or not.
In sequel, for both the input known and unknown
sources, in order for their data to be anonymized, the
Data anonymization component takes as an input this
data so as to completely anonymize it, achieving the
required data disclosure and privacy requirements. It
should be noted that there exist cases that the part of
data anonymization may take place either within or
outside the different organizations of the healthcare
data providers, in order to enable and achieve data
protection and privacy policy. Depending on the type
of the data source that the anonymized data has been
derived from (i.e. either unknown or known sources),
the flow of the data has two (2) different options. In
the first option of the unknown sources, the
anonymized data is being sent into the Plug’n’play
sources component. In this component, different
technologies are being provided for easing the
connection between the new streaming data sources
and the CrowdHEALTH platform, identifying the
sources’ Application Programming Interfaces (APIs),
and finally gathering all their data. Sequentially, all
this data is being sent to the Sources reliability
component that combines and evaluates (i) the
reliability of the collected data, and (ii) the reliability
of the data sources that produced all the collected
data, so as to estimate the reliability levels of each
connected data source, and keep only the reliable data
that comes from exclusively reliable sources. Thus,
all this data is sent to the Gateway component so as
to be transferred into the remaining flow of the
architecture. In the second option of the known
sources, the anonymized data is sent immediately to
the Gateway component, where both connectivity and
communication issues are solved at the same time, so
as to gather the data from the connected sources.
Data Integration: In order for the collected data to
be firstly managed and transformed into an
interoperable format, the Gateway sends the collected
data in the form of raw data to the Data conversion
component. The latter implements different
functionalities in order to make it interoperable both
structure and terminology wised, translating finally
the collected data of the Gateway into the HHR FHIR
format (Kiourtis, 2019a) that has been decided to be
used for the interoperability purposes, based on a
relevant research that was conducted in the past
(Kiourtis, 2019b). In more details, the Data
conversion component initially transforms the raw
data into HHR format using the HHR model
(Kiourtis, 2019a) that is being produced by the HHR
Figure 1: CrowdHEALTH architecture.
CrowdHEALTH: An e-Health Big Data Driven Platform towards Public Health Policies
243

manager component. In short, the HHR model has
been constructed in the context of the
CrowdHEALTH platform, for representing in a
consistent way all the data required by the underlying
data sources. It implements an XML language,
specifically designed for the HHR model, which
allows to specify in a machine-interpretable way the
structure of HHR types and map them to the structure
of the corresponding FHIR resources (HL7 FHIR,
2018). As soon as all the acquired data is transformed
into HHR FHIR format, since it is important to have
a certain confidence about the created information
“fresh-ness” and appropriateness, the generated HHR
FHIR data is sent to the Data cleaning component so
as to be cleaned. To achieve that, the latter performs
specific data queries to the Data aggregation
component. This component, in turn, submits these
queries into the CrowdHEALTH Data Store, so as to
retrieve historical data and send it back to the Data
cleaning component for performing data cleaning
actions based on the defined cleaning rules and the
patterns created by the acquired historical data. Thus,
all the gathered data is fully cleaned, being sent in the
form of cleaned HHR FHIR data to the Data
aggregation component. In sequel, this component
aggregates all the input HHR FHIR data into the
corresponding HHRs, storing them finally into the
CrowdHEALTH Data Store. It should be noted that
the HHRs are not stored as raw HHR documents into
the Data Store, but instead, they are translated into
tuples that are stored in the data tables of the relational
schema of the Data Store, which was designed with
respect to the E-R definition of the HHR model.
Data Processing: Having constructed and stored
into the CrowdHEALTH Data Store all the
aforementioned information, the HHRs clustering &
classification component is triggered taking as an
input the stored HHRs, in order to capture the
correlations among the similar HHRs that are
identified, and produce the corresponding HHRs
clusters. These clusters are then stored into the
CrowdHEALTH Data Store. On top of this, the
Context analytics component retrieves both the HHRs
and the historical data that is stored into the
CrowdHEALTH Data Store so as to identify cluster
similarities based on the health contexts obtained
from this data. Again, this information is stored into
the CrowdHEALTH Data Store for future usage.
Thus, upon all this stored data (i.e. HHRs, HHRs
clusters, historical data), the Big data analytics
component performs real-time big data analytics,
enabling correlations and extraction of situational
factors between biosignals, physical activities,
medical data patterns, clinical assessment, and
laboratory exams. This component is able to process
millions of events per second allowing the
exploitation of (often-critical) medical data from
different sources as things happen.
2.2 Health Analytics
Since the data from the underlying sources have been
successfully imported, transformed, and stored into
the CrowdHEALTH HHR-compatible format
through the Data & Structures pillar, all this data can
then be exploited by the Health Analytics pillar of the
CrowdHEALTH platform. In more detail, in the
context of Health Analytics, analytical techniques are
utilized for carrying out Clinical pathway mining,
Causal analysis, Multimodal forecasting, as well as
Risk stratification upon all the gathered data. Each
one of these components works independently,
acquiring as an input from the CrowdHEALTH Data
Store all the stored information that they need, which
was originally arrived in the platform in the form of
constructed HHRs. Additionally, each one of these
components exploits the Big data analytics
component so as to perform its queries upon the
required data and retrieve the corresponding health
analytical results. In short, Causal analysis allows the
identification of the properties that affect the
performance of policies and care plans, while Clinical
pathway mining supports data analysis so as to
identify similarities or differences in treatment among
groups of patients, indicating major effective factors
that affect several treatments and establishing a
supporting framework for improving the treatment of
patients with different diseases. Multimodal
forecasting estimates the applicability and
effectiveness of health policies, their variations and
combinations to particular population segments,
considering social information and spatiotemporal
properties. Finally, the Risk stratification informs
about population-level health risk, identifying what
proportions are of low, medium and high risk.
2.3 Policies
On top of the Data & Structures and Health Analytics
pillars, there exists the Policies pillar that is mainly
responsible for exploiting the results by using the
developed Policy Development Toolkit. The latter
represents the component that integrates several sub-
components to enable policy makers to create, update
and validate policy models. In this context, initially
the Policies modelling component is triggered, which
collects as an input all the existing policy models,
formulates new policy models’ structures based on
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
244

the policy makers’ inputs, and sends the constructed
structures and key performance indicators (KPIs) to
the Policies creation component in order to create the
corresponding policies. In sequel, as soon as the
policies have been created, their evaluation takes
place through the Policies evaluation component,
which takes as an input (i) the constructed formulas
of the created policies from the Policies creation
component, and (ii) the analytical results from the
corresponding Health analytics tool (i.e. Clinical
pathway mining, Causal analysis, Multimodal
forecasting, Risk stratification) that it was decided to
be used by the user. Based on this input, the Policies
evaluation component outputs to the Policies creation
component the evaluated policies so as to conclude to
the final context of its created policies and store them
into the CrowdHEALTH Data Store.
It should be mentioned, that all this information
can be provided to different user groups in the
ecosystem (e.g. healthcare providers, policy makers,
healthcare professionals, nutrition experts, etc.)
through the Data visualization component. In short,
this component enables the interaction of all the users
with the platform through analytical queries, while
processing the results and visualizing them in an
adaptive way. The Data visualization component is
integrated into the Policy Development Toolkit in
order to provide the required enhanced visualizations
towards the end users. What is more, the Access
control component is also integrated into the Policy
Development Toolkit in order to give access to
authorised members, providing them with different
capabilities based on their privileges and rights. Thus,
all the members are allowed to interact and exploit the
corresponding capabilities of the Policy Development
Toolkit and the Data visualization component.
3 CrowdHEALTH USE CASES
Based on the architecture described in Section 2,
CrowdHEALTH aims to design, develop and
showcase a novel data integration and health analytics
framework for exploiting heterogeneous health data,
which leverages the proper understanding for
successfully creating and evaluating public health
policies. Thus, CrowdHEALTH aggregates
healthcare data aiming to track the same patients in
different sources, and create a holistic overview of
their health conditions, leveraging it to population-
based analysis. For that purpose, in this Section six
(6) different representative use case scenarios of the
CrowdHEALTH platform are described, which
consist of both private and public healthcare
stakeholders that have a different health scope across
Europe. More specifically, these use cases refer to the
organizations of University Hospital of La Fe
(HULAFE) (HULAFE, 2019), Karolinska Institutet
(KI) (Karolinska Institutet, 2019), University of
Ljubljana (ULJ) (University of Ljubljana, 2019),
CareAcross (CRA) (CareAcross, 2019), BioAssist
(BIO) (BioAssist, 2019), and German Research
Centre for Artificial Intelligence (DFKI) (DFKI,
2019). Through these use cases, the main scope is to
integrate the research and development work of the
CrowdHEALTH platform, verifying its purposes, and
collecting useful feedback about its developed
concepts and technologies. Since the use cases aim to
verify the applicability of the whole CrowdHEALTH
platform, their collected data has followed all the
steps and mechanisms provided by the Data &
Structures and Policies pillars, whereas depending on
each different use case’s scope and requirements, the
corresponding health analytical technique was
implemented. All this information is described for
each different use case in the following paragraphs.
HULAFE use Case: This use case has been
chosen for the identification of overweight and obese
patients in the Health Department Valencia-La Fe
through the implementation of CrowdHEALTH. In
more detail, HULAFE offers data that is related to
patients’ demographic information, hospitalization
episodes, emergency room episodes, hospital at home
episodes, and morbidity. By implementing the whole
CrowdHEALTH data and policies process upon the
HULAFE collected data, as well as the clinical
pathway mining and risk stratification techniques, it
has become feasible to understand and characterize
Figure 2: CrowdHEALTH use case scenarios.
CrowdHEALTH: An e-Health Big Data Driven Platform towards Public Health Policies
245

which data is crucial to drive effective policies in
obesity and overweight fields, whilst improving
accuracy of the identification of overweight and
obese patients. In the same notion, it has been
achieved the improvement of the management and the
detection of obesity, including the systematic
detection of obese and overweight people and the
detection of bad nutrition and activity habits to
promote better habits on these citizens. What is more,
it has been achieved the detection of groups of
citizens with greater propensity for obesity to guide
public health policies, whereas broaden the
knowledge of health professionals through a catalog
of physical activity resources and professionals in
order to improve the prescribing of physical activity.
BIO use Case: This use case has been chosen for
monitoring disease progression and healthcare
expenditure for improved chronic disease
management of patients that have enrolled in the
BioAssist platform. More specifically, BIO offers
data related to biosignals relevant to patients’
conditions, being acquired from pulse oximeters,
blood pressure meters, glucometers, spirometers,
weighing scales, and physical activity trackers. By
implementing the whole CrowdHEALTH data and
policies process upon the BIO collected data, as well
as the risk stratification technique, CrowdHEALTH
bestows added value to patient monitoring
technologies, transforming these into tools that
support evaluation assessment with regards to
attributes of a population that are currently difficult to
examine, and providing a link between public health
authorities and patients. By applying the
CrowdHEALTH technologies within this use case, it
is achieved to enhance patients’ quality of life,
encourage proactive care, and offer efficient support
in potentially dangerous situations. Extending this
scenario by exploiting the data analysis capabilities
provided by CrowdHEALTH, collected data has the
potential to equip policy makers with a tool that
allows them to measure the impact of relevant
policies, in terms of actual results on populations
health and quality of life.
CRA use Case: This use case has been chosen for
evaluating the impact of online coaching and medical
education on cancer patient behavior that have
enrolled in the CareAcross web platform. More
specifically, CRA offers data related to patients’
diagnosis, treatment, comorbidities, health behaviors
and side-effects. By implementing the whole
CrowdHEALTH data and policies process upon the
CRA collected data, as well as the causal analysis
technique, all this data is analyzed in order to identify
potential causal relationships between specific data
points. Furthermore, it enables predictions of future
behaviors since a patient with specific diagnosis is
less likely to report a specific side-effect. Such
analyses are very important for patients, for
healthcare professionals, but also for public policy
makers. This is because the nature of oncology and
cancer care services is mostly confined to the clinic.
On the other hand, patients have increased and
prolonged support needs. This means that, while there
are no specific policies established for the provision
of medical information and online coaching, such an
approach may be quite helpful. This is not restricted
only to the benefit of individual patients, but it may
also be fruitful towards the improvement of resource
allocation in the healthcare system.
ULJ use case: This use case has been chosen for
analysing the current state of physical fitness and
weight status of children, analysing its development
over time, predicting future levels of fitness and
somatic development, through the implementation of
CrowdHEALTH. More particularly, ULJ offers data
related to cohort, physical activity, sedentariness,
sleep, resting heart-rate, socio-economic status, and
parental physical activity of school children. Thus, it
provides data on physical fitness and physical activity
to supplement the data on nutritional status of
children and enable the construction of obesity risk
assessment and developmental prediction models of
somatic and physical fitness development. By
implementing the whole CrowdHEALTH data and
policies process upon the ULJ collected data, as well
as the clinical pathway mining, risk stratification, and
causal analysis techniques, ULJ use case obtains a
basis for the implementation of policies that enable
linking school and health data for early interventions
monitoring and evaluation. What is more, the
individual growth trends, physical fitness and
nutritional development trends, adult stature
prediction, adult weight prediction, adult physical
fitness prediction, adult obesity-related health risks
prediction for all the students are visualized, for
easing the monitoring of the physical fitness, physical
activity and obesity among school children.
DFKI use Case: This use case has been chosen for
understanding and characterizing influences of
people’s nutritional habits, and differences in
physical activity upon their overall health and quality
of life, through the implementation of
CrowdHEALTH. More particularly, DFKI offers
citizens’ physical and activity data provided by their
personal activity trackers. By implementing the
whole CrowdHEALTH data and policies process
upon the DFKI collected data, all this data can be
clustered based upon their common nutritional and
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
246
physical habits, thus finding relevant correlations
among it, and among the habits of the citizens.
KI use Case: This use case has been chosen for
monitoring patients with chronic kidney diseases
(CKD) and cardiovascular diseases through the
implementation of CrowdHEALTH. In more detail,
KI offers patients’ demographical data, drug usage
data, and practitioners’ consultation data with regards
to these diseases. By implementing the whole
CrowdHEALTH data and policies process upon the
KI collected data, as well as the clinical pathway
mining, risk stratification, and causal analysis
techniques, all this data can be combined in order to
determine the prevalence of CKD, and ascertain its
clinical consequences in terms of comorbid
complications and healthcare resource utilization, to
determine healthcare- and socioeconomic-related risk
factors for progression of CKD, and finally to
establish the safety and effectiveness of common
drugs in individuals with CKD and the connection to
cardiovascular diseases.
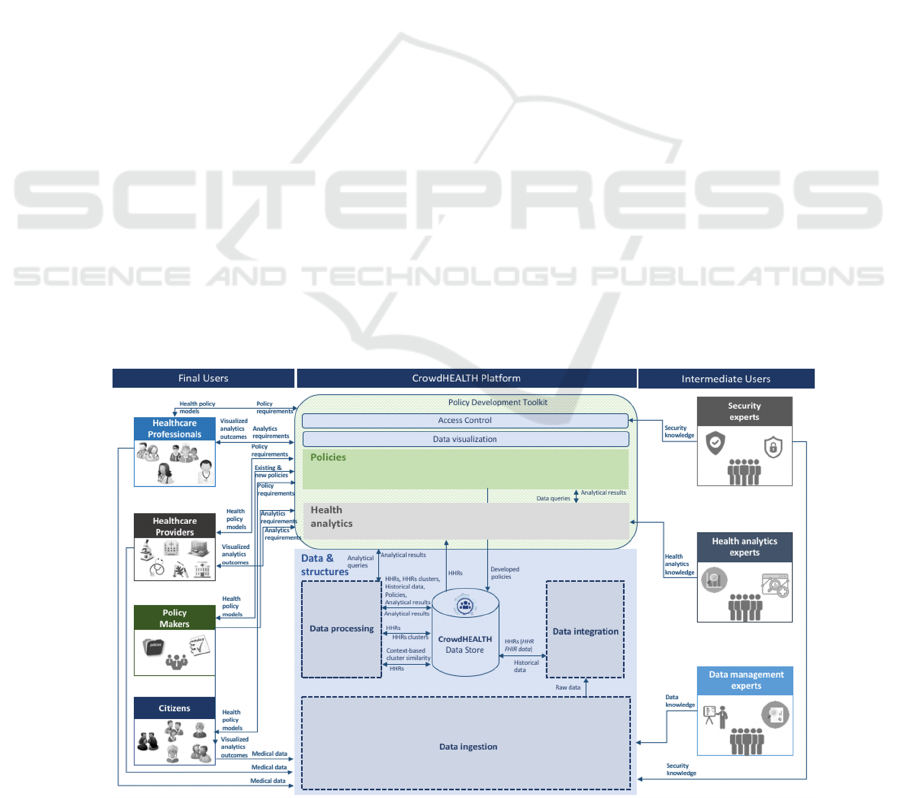
4 CrowdHEALTH USERS
Based on the use cases described in Section 3, various
users can offer their data and exploit the results of the
CrowdHEALTH platform. Thus, all the information
provided by the CrowdHEALTH platform can be
exploited by different types of user groups that may
exist in a healthcare ecosystem. These users may
represent either final or intermediate users, depending
on whether they have access to the final output
information of the platform or they have access to all
the information that is being produced, exchanged,
and managed through the whole data flow of the
platform. All the types of users that are getting
involved into the CrowdHEALTH platform and the
interactions that they have with the platform’s (3)
main pillars are depicted in Fig. 3, including both
final and intermediate users.
With regards to the final users, these include the
healthcare professionals, the healthcare providers, the
policy makers, and the citizens. The most crucial and
central stakeholder among them is the citizens, since
the whole CrowdHEALTH architecture, both
initiation and existence are based upon the medical
data that is provided by them. Apart from this, the
citizens may provide to the platform their
experimentation results based upon the policies that
were exported by the platform and given to them.
Apart from the citizens, a major role in the platform
is played by the policy makers. The latter are able to
provide to the platform their existing policies - not
only the existing health policy models that they
currently aim to create, but also the health policies
that other policy makers have modelled and created.
As a result, they contribute to the successful
completion of the policies creation process, being
able to get as an output from the platform the final
developed policies. Furthermore, another major role
in the platform is played by healthcare providers that
can offer the citizens’ medical data into the platform,
whilst they are offering the ability to receive the
developed health policies based upon their requested
policy requirements. Finally, another major role in
Figure 3: User groups’ interaction with CrowdHEALTH architecture.
CrowdHEALTH: An e-Health Big Data Driven Platform towards Public Health Policies
247

the, platform refers to the healthcare professionals
that, as in the case of the healthcare providers, can
enter the citizens’ medical data into the platform.
Moreover they are able to view analytics outcomes
that they have requested based on their analytics
requirements through the visualization component of
the platform and receive the developed health policies
based upon their requested policy requirements.
Regarding the intermediate users, these include
the security experts, the health analytics experts, and
the data management experts. The security experts
provide their expertise upon all the security aspects
that are developed into the CrowdHEALTH platform
of the Policies and the Data & Structures pillars, and
are of crucial importance. Apart from the security
experts, the health analytics experts are highly
involved into the platform, providing their health
analytics knowledge upon all the developed health
analytical tools of the Health Analytics pillar. In the
same notion, the data management experts are
responsible for providing their data knowledge upon
all the data management procedures that occur within
the Data & Structures pillar of the platform.
5 CONCLUSIONS
Patients’ data coming from multiple information
sources constitutes a computable collection of fine-
grained longitudinal phenotypic profiles that may
facilitate cohort-wide investigations and knowledge
discovery on an unprecedented scale, which is the
prerequisite for patient-centered care (Chawla, 2013).
To this end, in this paper a complete patient-centered
eHealth platform was presented, the CrowdHEALTH
platform, being able to capture all the existing health
determinants in new structures, the HHRs, while
creating groupings of them (i.e. clusters). As a result,
it provided the ground for the discovery of deep
knowledge about population segments and provision
of insight for different segments and users according
to various criteria (e.g. location, medication status,
emerging risks, etc.), by creating and evaluating the
corresponding health policies. This opens the
opportunities for successfully achieving personalised
medicine, and disease prevention (Chawla, 2013),
(Cirillo, 2019).
The applicability of the proposed platform was
evaluated through different use case scenarios in
terms of collecting and processing data from real-
world data sources, being heterogeneous, and having
various data formats, analysis needs, information to
be included in the HHRs, target groups (e.g. people
suffering from chronic diseases, children and youth),
and environments (e.g. care centers, social networks,
public environments, and living labs). Thus, by
currently exploiting the 2 million records and 700.000
streams of lifestyle activities and nutrition data, as
well as engaging more than 200.000 users that come
from these use case scenarios, the platform is
expected to be able to exploit more than 7.5 million
measurements from 1 million people across Europe.
ACKNOWLEDGEMENTS
The research leading to this result has received
funding from the European Union’s Horizon 2020
research and innovation programmes under grant
agreement No 727560 (CrowdHEALTH project).
REFERENCES
BioAssist (2019). BioAssist platform,
https://bioassist.gr/?lang=en
CareAcross (2019). CareAcross platform,
https://www.careacross.com/
Chawla, N. V., et al. (2013). Bringing big data to
personalized healthcare: a patient-centered framework.
Journal of general internal medicine, 28(3), 660-665.
Cirillo, D., et al (2019). Big data analytics for personalized
medicine. Current opinion in biotechnology, 58, 161-
167.
Cohen, L. (2019). More, More, More: Removing data
inefficiencies will remove healthcare roadblocks,
https://www.medicaleconomics.com/news/more-more-
more-removing-data-inefficiencies-will-remove-
healthcare-roadblocks
CrowdHEALTH (2019). CrowdHEALTH EU project,
https://crowdhealth.eu/
DFKI (2019). DFKI, https://www.dfki.de/en/web/
Edelman (2011). Health Barometer 2011: Global Findings,
http://healthbarometer.edelman.com/2011/10/health-
barometer-2011-global-findings
Ganguly, S., et al., (2009). Sharing information and data
across heterogeneous e-health systems. Telemedicine
and e-Health, 15(5), 454-464.
HL7 FHIR (2018). Resource Index,
https://www.hl7.org/fhir/resourcelist.html
HULAFE (2019). Health Department of Valencia-La Fe,
http://www.lafe.san.gva.es/home
Karolinska Institutet (2019). Karolinska Institutet,
https://ki.se/
kBioAssist, S. (2017). CrowdHEALTH: Holistic Health
Records and Big Data Analytics for Health Policy
Making and Personalized Health. Informatics
Empowers Healthcare Transformation, 238, 19.
Kiourtis, A., et. al (2019a). Holistic Health Records towards
Personalized Healthcare. IEEE International
Symposium on Circuits and Systems. (under review)
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
248

Kiourtis, A., et. al (2019b). Aggregating the syntactic and
semantic similarity of healthcare data towards their
transformation to HL7 FHIR through ontology
matching. International Journal of Medical Informatics
132 (2019): 104002.
LeanXcale (2019). Any load & scale database,
https://www.leanxcale.com/
The, L. P. H. (2019). Next generation public health: towards
precision and fairness. Public health, 4(5), e209.
University of Ljubljana (2019). University of Ljubljana,
https://www.uni-lj.si/eng/
CrowdHEALTH: An e-Health Big Data Driven Platform towards Public Health Policies
249
