
IT-Governance in Integrated Care: A Risk-centred Examination in
Germany
Lena Otto
a
Chair of Wirtschaftsinformatik, esp. Systems Development, Technische Universität Dresden, Dresden, Germany
Keywords: IT Risk Management, Integrated Care Networks, IT Governance Frameworks, Evaluation, Information
Security.
Abstract: Health care systems face several challenges regarding costs and effectiveness. Integrated care networks and
usage of application systems (as automated part of information systems) are two approaches to overcome
these challenges. To fully reach their potential, a seamless process is mandatory. IT governance frameworks
help health care organisations to implement an integrative risk management. Nevertheless, a network-centred
approach, e.g. necessary for integrated care networks, is not in focus of existing frameworks, such as COBIT
or ITIL. Therefore, the following article evaluates how selected frameworks can be used for risk management.
A literature analysis and a case study of the German health care system are conducted focussing on
confidentiality, integrity, and availability in integrated care networks’ application systems. Findings suggest
that inter-organisational risk management is especially influenced by the increased need for coordination and
the autonomy of network partners. Finally, the main aspects necessary for using the evaluated frameworks
within an integrated care context are shown.
1 INTRODUCTION
The German health care system is one of the most
expensive worldwide while at the same time being
one with very high-quality standards. However, the
increasing effects of demographic change together
with comorbidities enforce a focus on integrated care,
where different actors are combined along the care
continuum (Gröne et al., 2001). To transfer and use
the highly sensitive data in the health care sector for
ensuring the cooperation of actors requires the
development of safe and secure application systems
(Henriksen et al., 2013) as well as high compatibility
of these systems to ensure available and sound data
(Zambon et al., 2011), i.e. to guarantee information
security. Information security as well as other
business objectives, e.g. integrated care cooperation,
rely on successful information technology (IT)
provision (Bannerman, 2008), which can be disturbed
by different risks. These risks include technical or
human failures as well as external events, e. g. fire.
To prevent and handle these risks (Agrawal, 2009),
risk management measures can be applied (Silva et
al., 2014). A clear guidance on how to implement and
a
https://orcid.org/0000-0003-3814-4088
execute risk management is, among others, provided
by IT governance frameworks (Alreemy et al., 2016).
However, they mainly address the internal
governance (Gaulke, 2014) and have rarely been
analysed in the context of networks, especially
integrated care networks. This leads to the following
research question:
How can existing IT governance frameworks be
adapted for the management of IT risks in integrated
care networks and what are possible weaknesses?
The aim of this paper is to improve the
understanding and use of IT governance frameworks
to implement an adequate risk management in
network organisations. Based on a literature study,
the feasibility for using existing frameworks in the
context of network organisations is examined for the
three frameworks COBIT, ITIL and ISO 27005. As
integrated care networks (especially in Germany)
involve a high degree of autonomy for participants, a
network’s risk management needs be seen within the
context of the risk management in each participating
individual organisation. To demonstrate this inter-
808
Otto, L.
IT-Governance in Integrated Care: A Risk-centred Examination in Germany.
DOI: 10.5220/0009376708080817
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 808-817
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

dependence, a case study is conducted, illustrating the
general measures incorporated in risk management
strategies. Furthermore, the transfer of results from
the exemplary case study to an integrated care setting
is explained. Based on the findings, requirements for
using IT governance frameworks for risk
management in integrated care settings will be
derived. Thereby, the paper contributes to the topic of
IT governance in integrated care.
2 METHOD
First, consistent criteria were defined against which
each framework could be evaluated. They were
derived from a narrative literature review covering
the topics integrated care and inter-organisation
application systems. After all criteria were defined,
the frameworks (AXELOS, 2013; ISACA, 2012;
ISO, 2011) were evaluated and compared, using
qualitative content analysis according to Mayring
(2000). Each framework was checked for covering
the criteria defined, which represent deductive
categories.
A case study was used to further illustrate the
process of risk management implementation. An
integrated care network with two participants is
displayed, showing hospital A as a maximum care
provider and hospital B as a smaller rural hospital. In
hospital A, risk management steps were conducted,
identify, analyse and assess existing risks. For the
initial risk identification and analysis, a focus group
was conducted to evaluate the BSI catalogue of
possible risks (BSI, 2011). Afterwards, the risk
assessment was performed by means of a risk matrix.
It was chosen as an evaluation tool as it shows very
clearly which risks need to be covered and which
risks can be neglected. Furthermore, the presentation
of risks is differentiated with concurrent manageable
complexity. The risk assessment was conducted
within the focus groups, i.e. as part of a Delphi study
(S. M. Smith et al., 2018). Different roles of the IT
management and hospital management participated
in these focus groups, e. g. the chief information
officer, leading IT project managers, administrators,
as well as representatives of the chief execution
officer. For hospital B, no risk management was
conducted but instead, the procedure of transferring
the results to an integrated care setting was described.
Based on the results from literature analysis,
qualitative content analysis and case study,
recommendations were derived for future research on
the topic of IT governance frameworks for risk
management in application systems of integrated care
networks.
3 FOUNDATIONS
3.1 IT Governance and IT Risk
Management
The goal of IT governance is to achieve business
objectives supported by IT processes while
generating value and minimising risks (Alreemy et
al., 2016). Nevertheless, different IT governance
frameworks exist. The three most widely used ones in
the context of risk management, i.e. COBIT, ITIL and
ISO 27005:2011 (Häfner & Felden, 2009), will be
analysed in detail in the following. While COBIT
presents a universal governance concept (Gaulke,
2014), ITIL focusses on IT service lifecycle
management with best practices (Sahibudin et al.,
2008). On the other hand, ISO 27005 provides a
generic frame for IT risk management and directly
addresses information security (Fenz et al., 2014).
Risk management supports the handling of
potential risks and includes the steps “definition of
risk strategy”, “identification and analysis”,
“assessment”, “control” and “monitoring” of risks
(Agrawal, 2009). Furthermore, information and their
security, including confidentiality, integrity and
availability (Zambon et al., 2011), are an important
aspect in application systems. Different events in
daily business can be a direct risk to these security
goals: Fire can harm availability and malware can
threaten integrity or confidentiality of data, followed
by economic and legal risks. When speaking of IT
risks the automated part of an information system, the
application system (Ferstl & Sinz, 2013), is
addressed. This is also true for inter-organisational
application systems which are the automated part of
an inter-organisational information system. Main risk
categories on this operational perspective are risks
which are related to involved persons, processes and
systems as well as external risks that consider the
surrounding (Bistarelli et al., 2012). The BSI
catalogue of possible risks provides a good starting
point for identifying possible risks, especially for
critical infrastructures. BSI (Bundesamt für
Sicherheit in der Informationstechnik) is the German
Federal Office for Information Security. The BSI
catalogues provide a wide range of possible risks
related to information technology and were
developed by different experts in that field, which
makes them reliable.
IT-Governance in Integrated Care: A Risk-centred Examination in Germany
809
3.2 Characteristics of Integrated Care
and Related Information Systems
Similar to most of the western health care systems,
the health care system in Germany is separated into
different sectors, with own budgets and planning
structures (Koch, 2005). Connections within and
between these sectors are insufficient and lacking
(Amelung et al., 2012). A possible solution to
overcome the related problems is seen in integrated
care as it supports the patient-centred treatment across
all sectors. However, integrated care is a widely used
term that arose from a tendency towards cooperative
care years ago (D. L. Smith & Bryant, 1988).
Nevertheless, the focus in this research paper is on
integrated care in Germany as its special characteristics
are important for the later evaluation of frameworks.
Digital tools are important to improve existing health
services and integrated care solutions (Seventy-first
World Health Assembly, 2018), e.g. information
systems to share existing data. Information systems
which are commonly used by different organisations
are called inter-organisational information system. In
inter-organisational information systems, information
is processed beyond organisation’s borders (Johnston
& Vitale, 1988). Data retention is thereby possible in a
centralised as well as decentralised manner.
In the following, characteristics of network
structures generally and in integrated care settings
and of application systems within these structures are
introduced.
Organisational Structures. Challenges regarding
the organisational structure occur due to the
collaboration of different organisations in one
network. Such networks have complex, relatively
stable temporary relations with contractual
commitment between legally independent but
economically dependent participants for a specific
purpose (Schüppler, 1998). The management has no
direct authority, which is why all attendees get
involved in leadership (Bogenstahl, 2012). Further
challenges arise from the beneficiary involvement of
every organisation and the following organisational
structure of a network. Networks can range in
multiple dimensions between market and hierarchy,
competition and cooperation, autonomy and
dependency, flexibility and specificity, variability
and unity, trust and control, stability and fragility,
formality and informality as well as economical
action and safeguarding of power (Sydow, 2006).
Every network has its own position within the
different areas of tension. For integrated care
networks in Germany, this position is as follows: In
accordance with §140a SGB V special care contracts
are possible between health insurance companies and
different service providers. Integrated care is
therefore market-related and service providers are
cooperating even though they can compete when
being on the same service level. Every service
provider acts autonomously, specifically and variable
as the network is built to separate tasks depending on
specification. A supervisory authority does not exist in
a narrower sense and therefore enormous trust between
all participants is necessary. Furthermore, contractual
commitment with a health insurance company
guarantees a stable cooperation, high formality
between service providers and economical action.
Inter-organisational Application Systems. Infor-
mation processing beyond organisation’s borders
results in differences between inter-organisational
application systems and such within a single
organisation. These differences are displayed in table
1. Systems and processes in integrated care are
developed differently in comparison to systems and
processes in a single institution. Characteristics of
inter-organisational application systems in an
integrated care setting in Germany are also depicted
in table 1, column 3.
Table 1: Characteristics of inter-organisational application
systems and typical characteristics in Germany.
General characteristics
Typical
integrated care
characteristics
in Germany
I
Exchange/corporate usage of
data and applications (Raupp,
2002; Schüppler, 1998)
Loosely coupled
application
systems
II
Risk of heterogeneous
security concepts (Raupp,
2002)
Focus on
internal security
concepts
III
Centralised/decentralised data
retention (Raupp, 2002;
Schüppler, 1998)
Decentralised
data retention
IV
Supervision by multiple
participants (Suomi, 1992)
Supervision by
respective
network
partners
V
Interface management
necessary (can lead to
system/media disruption and
data inconsistencies) (Raupp,
2002; Schüppler, 1998)
No
standardised
interfaces
VI
(unilateral) interdependencies
possible (Raupp, 2002)
Low
dependencies
Scale-IT-up 2020 - Workshop on Best Practices for Scaling-Up Digital Innovations in Healthcare
810
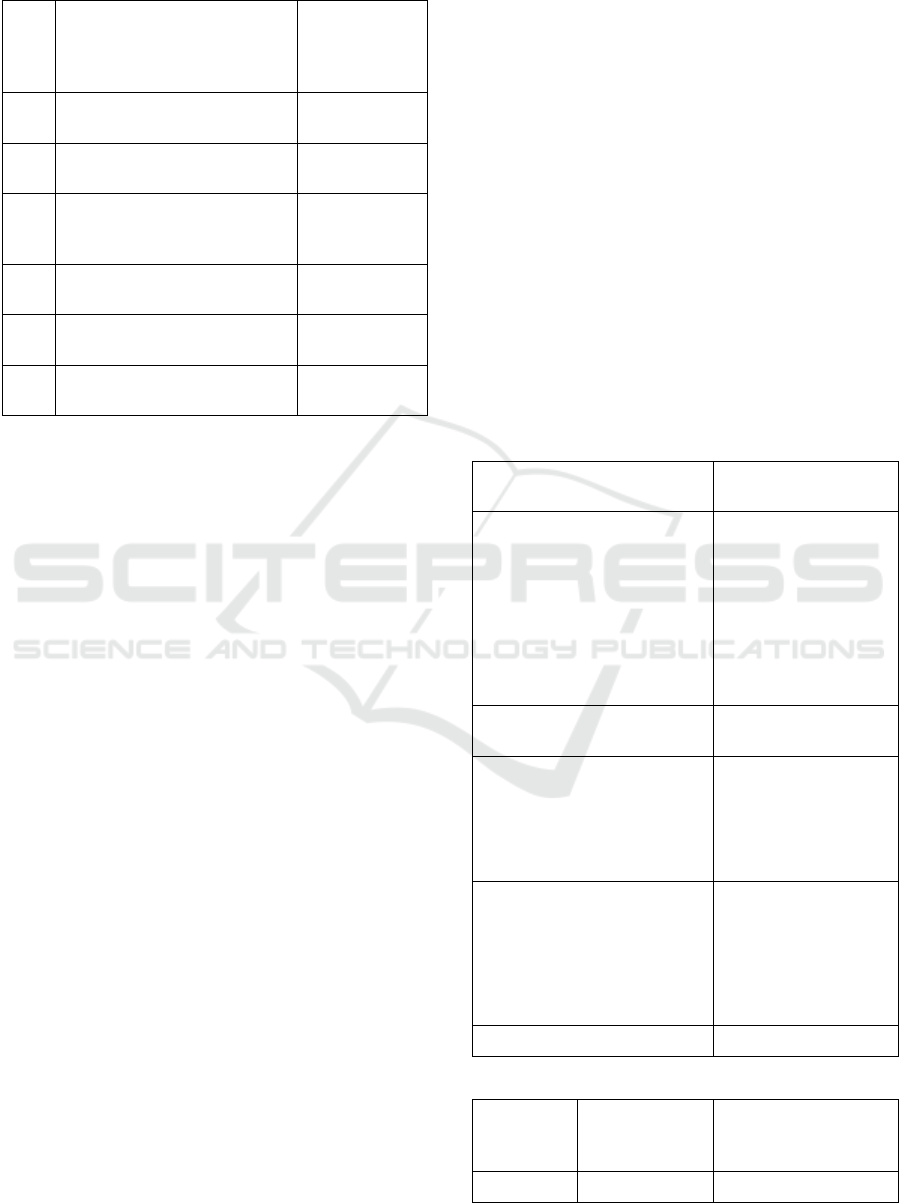
Table 2: Characteristics of inter-organisational application
systems and typical characteristics in Germany (cont.).
General characteristics
Typical
integrated care
characteristics
in Germany
VII
Mostly standardised systems
(Raupp, 2002)
Low
standardisation
VIII
Centralised/decentralised rights
of disposal (Raupp, 2002)
Centralised or
decentralised
IX
High system security for data
and transaction (Raupp, 2002)
System security
is highly
important
X
Flexible number of participants
possible (Raupp, 2002)
Flexible number
of participants
XI
Spatial distribution of network
participants (Raupp, 2002)
Regional
distribution
XII
Level of intensity in
collaboration (Schüppler, 1998)
Low intensity
Another aspect, which is specific in inter-
organisational application systems are the larger
numbers of components (hard- and software) and
involved persons (users and administrators) as well as
the necessary secure connections between several
application systems (Johnston & Vitale, 1988).
3.3 Evaluation of IT Governance
Frameworks
To evaluate and compare the three chosen
frameworks (COBIT, ITIL and ISO 27005) consistent
comparison criteria are necessary. Important for risk
management is its integration into business processes
(see section foundations). Therefore, IT governance
frameworks should provide recommendations for
conducting the whole IT risk management process. In
general, this involves the following steps: definition
of risk strategy (1), identification and analysis (2),
assessment (3), control (4) and monitoring (5) of risks
(Agrawal, 2009). Furthermore, the goals of
information security, i.e. confidentiality, integrity and
availability (6), need to be considered (Zambon et al.,
2011). Focussing on application systems, the
components involved, i.e. hard- (7) and software (8),
as well as involved individuals (9) need to be addressed
within the frameworks (Johnston & Vitale, 1988).
Further evaluation criteria are the risk categories
person- (10), process- (11) and system-related (12) as
well as external risks (13) (Bistarelli et al., 2012) and
the appropriateness due to the general characteristics
of the frameworks analysed (14).
Based on the selected criteria the three frame-
works can be evaluated and compared regarding the
suitability for risk management of (general) intra-
organisational application systems, i.e. application
systems within a single institution. Afterwards, the
transfer of results to inter-organisational application
systems in integrated care can be examined, consi-
dering the specific characteristics of integrated care.
3.3.1 Intra-Organisational Context
The results of analysing the three models are
displayed in Table 2. As can be seen, COBIT is one
of the most extensive IT governance frameworks,
addressing all criteria and providing detailed
explanation for risk management steps and system
components (Gaulke, 2014). However, its complexity
(14) threatens its applicability (De Haes et al., 2013).
ITIL’s focus on IT service lifecycle management
leads to a lack in considering risk manage-
ment as a continuous cyclical process (1, 5, 14)
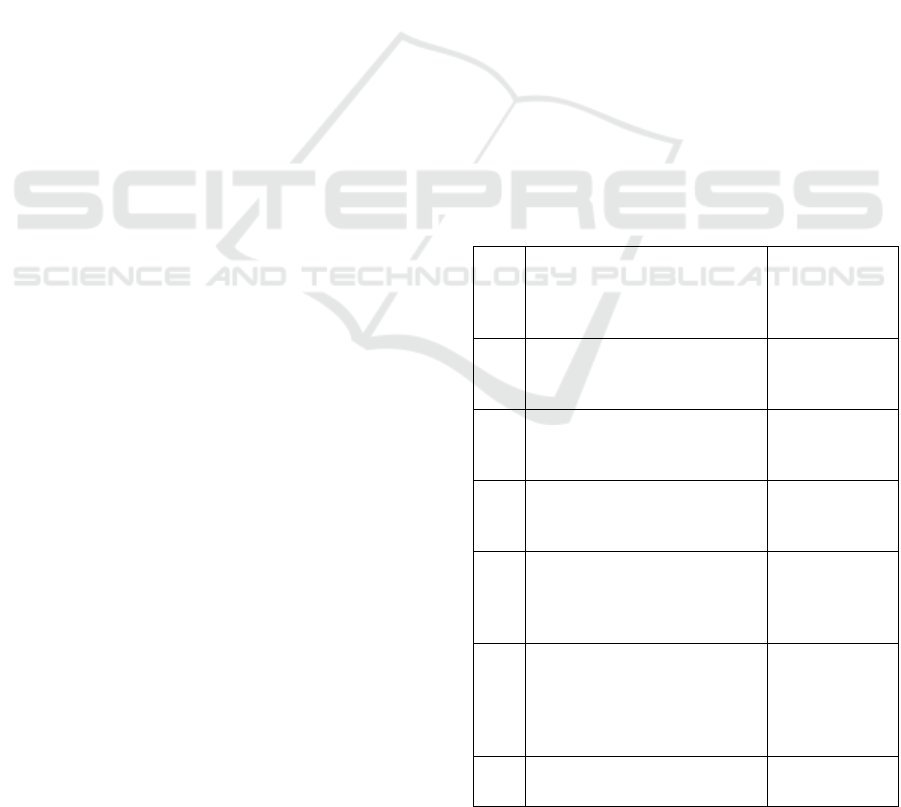
Table 3: Evaluation criteria fulfilled per framework.
Category COBIT ITIL
ISO
27005
Covering of risk management
process:
(1) Definition of risk strategy
(2) Identification and analysis
(3) Assessment
(4) Control
(5) Monitoring
(6) Focus on confidentiality,
integrity and availability
Consideration of components:
(7) Hardware
(8) Software
(9) Individuals
Considered risk categories:
(10) Person-related risks
(11) Process-related risks
(12) System-related risks
(13) External risks
(14) General characteristics
Legend:
Fully
complies
with criteria
Partly complies
with criteria
Does not comply with
criteria
IT-Governance in Integrated Care: A Risk-centred Examination in Germany
811

(Vilarinho & da Silva, 2011). Furthermore, most of
the specific risk categories (11-13) are not in focus.
In contrast, ISO 27005 fully complies with the
evaluation criteria.
As it can be seen from the comparison, the
examined frameworks mostly support the
implementation of risk management for application
systems within a single organisation. ITIL is the
framework which fits least as the definition of risk
strategy as well as process-, system-related and
external risks are only partly considered.
3.3.2 Inter-Organisational Application
Systems in Integrated Care
To check the transfer of results to risk management in
integrated care networks, the identified
characteristics of inter-organisational application
systems (I-XII) will be considered additionally. In
addition to the presented evaluation categories (fully,
partly, not complying), another one will be used in
table 3, for differentiating the results. If a criterion is
evaluated with ““, the framework addresses the
criteria abstractly, but does not specify its prospective
usage for inter-organisational networks.
The frameworks still consider the risk
management process steps (see table 2), but do not
take specific characteristics (see section foundations)
of integrated care networks into account. For every
step, finding a consensus between all network
participants is at least partly necessary as they are,
despite legally independent, economically dependent
from each other. The risk strategy needs to be uniform
for the whole network and risks evolving through a
connection between participants have to be identified
and analysed generally. A consistent assessment,
control and monitoring also needs to be based on joint
agreements, especially as integrated care networks
are characterised by low dependencies (VI) and
intensity in collaboration (XII) as well as high
regional distribution of participants (XI).
Additionally, risk assessment, in particular
probability of occurrence, can change. For example,
mistrust between the network participants can
increase person-related risks, while the loosely
coupled application systems (I) with non-
standardised interfaces (VII) constitute a high risk of
inconsistent data within process-related risks in
integrated care networks.
None of the frameworks selected considers the
specific characteristics explicitly. COBIT takes
requirements of status groups into account (ISACA,
2012), but does not particularly address corporate
networks. ITIL was not fully appropriate for intra-
organisational application systems already. In ISO
27005, its usage for all kinds of organisations is
mentioned (ISO, 2011), although characteristics of
corporate networks are also not considered.
Implementation guidance supported through
examples for risk management steps is still provided,
esp. in COBIT and ISO. Nevertheless, required
integrated management processes and consultations
are not yet included. Furthermore, solutions are
lacking for problems of missing management
authority and supervision (IV), low dependencies
between participants (also regarding security
concepts – VI/II), flexible number of participants (X)
and additional interface management (V). These
problems would require an adjusted risk management
which leads to a reduced validation (1-5).
The criteria confidentiality, integrity and
availability (6) are addressed for inter-organisational
as well as for intra-organisational application
systems. Integrated care networks do not require any
additional aspects for these criteria. Therefore, the
validation remains. Nevertheless, challenges can
arise due to the operational assurance of these criteria.
Additionally, securing interoperability on all
layers (legal, organisational, semantical, technical)
without creating further risks is important (European
Commission, 2017). Also, the components of inter-
organisational application systems (hard- and
software systems) are the same as for intra-
organisational ones. However, the number of
involved hard- and software systems is increasing in
inter-organisational settings, which results in the need
for appropriate interfaces (V). This is especially
important due to the prevalence of loosely coupled
application systems (I) and lack of standardised
interfaces and systems (V/VII). Furthermore, the
number of involved individuals (users and
administrators) increases as well compared with an
intra-organisational application system. All
additional individuals need to be included in the risk
management, especially when engaged on interfaces.
Nevertheless, none of the selected frameworks takes
one of these requirements into account. On the
contrary, individual organisations and their holistic
view are especially focussed on (Gaulke, 2014).
Despite a high independence of network participants
(VI), the network perspective and thus the “gaps”
between single institutions are important to be
considered. As this is not the case in all of the
frameworks analysed, the assessment needs to be
reduced (7-9).
The consideration of the four risk categories
in the frameworks was already positively evaluated
for intra-organisational application systems.
Scale-IT-up 2020 - Workshop on Best Practices for Scaling-Up Digital Innovations in Healthcare
812
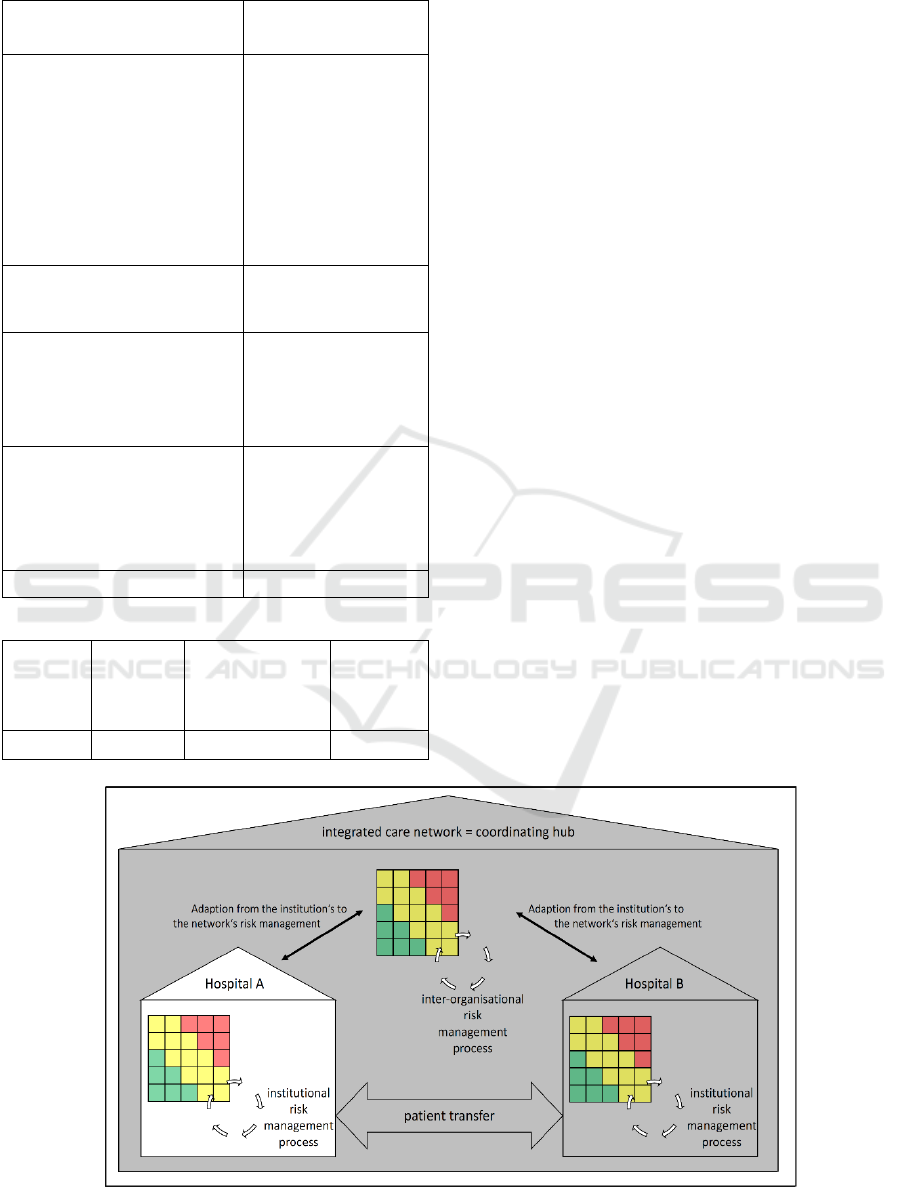
Table 4: Applicability of strategic fit for integrated care.
Category COBIT ITIL ISO
27005
Covering of risk management
process:
(1) Definition of risk
strategy
(2) Identification and
analysis
(3) Assessment
(4) Control
(5) Monitoring
(6) Focus on
confidentiality, integrity and
availability
Consideration of components:
(7) Hardware
(8) Software
(9) Individuals
Considered risk categories:
(10) Person-related risks
(11) Process-related risks
(12) System-related risks
(13) External risks
(14) General characteristics
Legend:
Fully
complies
with
criteria
Partly
complies
with
criteria
Complies with
criteria (no focus
on networks)
Does not
comply
with
criteria
Still, required consultations may be harmed due to
complex relationships, regional distribution (XI) of
partners collaborating with low intensity (XII) and the
resulting low dependency (VI). None of these
characteristics is included in the frameworks, what
leads to a reduction in the assessment of
corresponding criteria (10-13) as well.
Irrespective of the aforementioned lack of
consideration of company network specifics, the
evaluation of the fundamental characteristics (14)
does not change. The overall assessment is shown in
Table 3.
All in all, none of the three evaluated frameworks
fully complies with all criteria. ITIL and COBIT did
not or only partly fit for intra-organisational
application system’s risk management and the rating
is further reduced due to special characteristics of
integrated care. Also, ISO 27005 can only partly meet
the adapted requirements.
2.3.3 Exemplary Demonstration: Risk
Management in a Hospital Network
To illustrate the procedure of implementing risk
management within a single institution and show how
integrated care scenarios change this process, a case
study was conducted. As case scenario, a real-world
case of two hospitals (hospital A and B) is used,
where the risk management process is exemplary
executed for hospital A. Both hospitals are in a
strategic partnership to organise the patient transfer in
an integrated care network (see Figure 1). This means
defined processes in integrated care pathways, shared
electronic health records as well as shared
management processes and responsibilities. Hospital
Figure 1: Integrated care network scenario.
IT-Governance in Integrated Care: A Risk-centred Examination in Germany
813
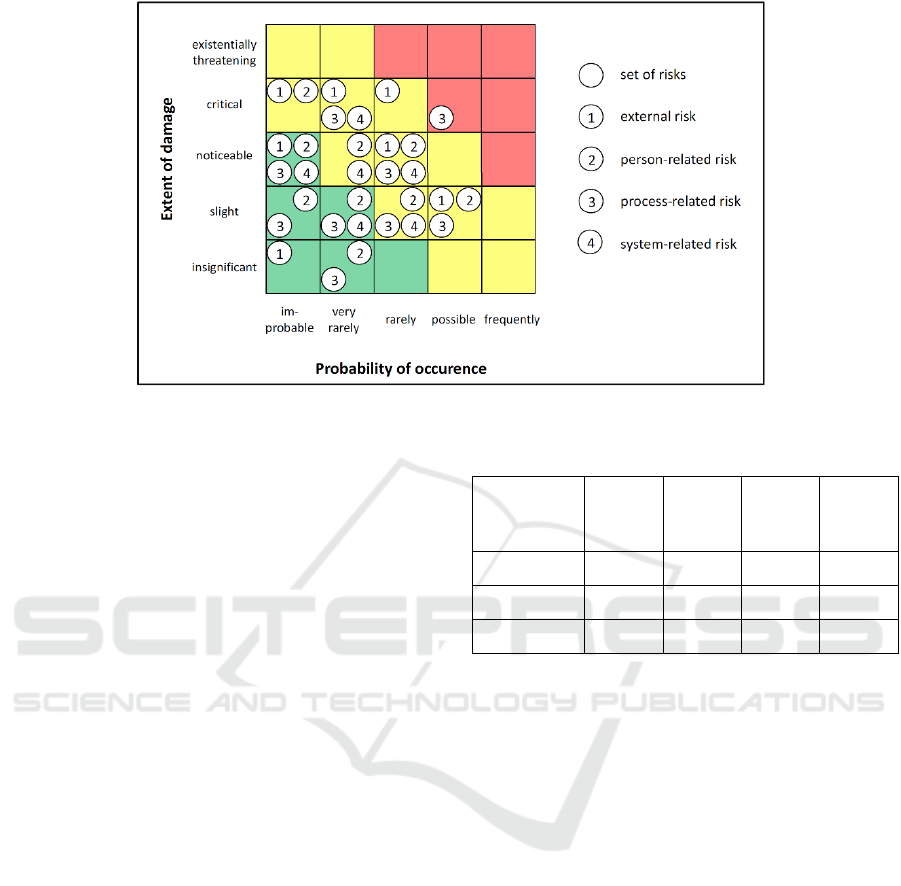
Figure 2: Accumulated risk matrix for assessing risks related to the application system of hospital A.
A is a maximum care provider with over 1,200 beds
capacity. Contrary, hospital B is a hospital in a rural
area focussing on basic care with 160 beds. The
network and the inter-organisational application
system are characterised by the typical features
described above.
As first step, the risk assessment (identification and
evaluation) was done on institutional level for
hospital A. As initial set of relevant risks, the 660
risks in the six categories elementary threats, force
majeure, organisational deficiencies, human errors,
technical failures and intentional acts from BSI (BSI,
2011) were used.
Out of the 660 risks, 182 risks were defined as
relevant by the focus group for hospital A. They were
categorized into four groups: external (50), person-
(75), process- (23), and system-related (34) risks. In
the next step, all risks were evaluated with a 5x5 risk
matrix regarding their probability of occurrence and
the extent of damage they might have. Each risk was
assessed by all experts, disagreement was solved
through discussion until consensus was reached.
Depending on this classification, the risks vary
widely in criticality. Some are intolerable (red area),
some undesirable (yellow area) and some negligible
(green area) (see Figure 2). Depending on the rating,
the following risk control is defined (the more a risk
is placed in the upper right corner of the matrix, the
more is a control action required). Each circle in
Figure 2 represents a set of risks. Since the matrix
does not reflect the number of risks in each section,
table 4 summarizes this information additionally.
Table 5: Summary of criticality per category.
Person-
related
risks
Process-
related
risks
System-
related
risks
External
risks
In-tolerable - 1 - -
Un-desirable 24 17 13 46
Negligible 51 5 21 4
The results of the risk assessment show that the
biggest proportion of the risks are assessed as
undesirable (yellow area – 100 risks). Since the
hospital A has a big IT department, only one system-
related risk could be identified as intolerable (red
area) and must be considered for further
countermeasures. The other 81 negligible risks (green
area) are existent but do not necessarily need further
consideration. However, the reason for this result is
not a missing importance of most risks. It is rather the
low expected probability of occurrence that lead to an
undesirable or negligible risk assessment. The focus
group assessed the probability relatively low for most
of the risks as the information system is already
highly mature. However, some risks to be controlled
further remain.
Conclusively, all four risk categories (person-,
process-, system-related and external) are relevant for
risk control and monitoring in hospital A. The usage
of frameworks in this internal context would be
helpful and can be realised e. g. with ISO 27005
which serves as a good framework for intra-
organisational risk management as shown above (see
Table 2). Furthermore, the BSI catalogues and their
approaches are compliant with ISO 27001 (to which
Scale-IT-up 2020 - Workshop on Best Practices for Scaling-Up Digital Innovations in Healthcare
814

ISO 27005 belongs) what supports the applicability
of this framework for hospital A even more.
Outlining the transition to a common risk
management within the integrated care setting
described, the risk assessment of hospital B needs to
be carried out as well, covering the individual
application systems’ risks of this second hospital.
However, to fully cover the whole network within the
risk management strategy, the network itself and its
application system need to be considered. This is due
to the fact that inter-organisational risk management
is more than the sum of risk managements within each
individual institution.
Some implications can be inferred from the
maximum care provider’s results. Following the
results of framework evaluation, the assessment of
risks, especially probability of occurrence, is likely to
increase when considering the perspective of
integrated care networks. The focus group workshop
already came to the same conclusion by
acknowledging that a modified assessment for some
risks would be required within a network scenario.
This applies to all risk categories and can lead to a
higher criticality and more necessary control.
Furthermore, an overall guideline or framework is
needed for coordination in an integrated care
network, especially as participants in integrated care
networks act highly independent from each other and
no common supervision exists.
Due to the lacking applicability of the frameworks
included, the need for a new domain-specific
framework could be identified. Summarising the
identified deficits, the following requirements need to
be considered for such a framework:
Req. 1 - Cross-company Management
Processes: An explicit reference to the
increased need for consultation in most
risk management steps is necessary.
Req. 2 – Assignment of Responsibility:
Instructions for defining responsibilities
regarding a holistic control of all shared
processes needs to be included in such a
framework.
Req. 3 – Rules in the Event of Changing
Participants: Responsibilities need to be
ensured, also in case of changing
participants. This can be ensured by means
of a sufficient number of defined deputies
or the implementation of process steps that
come into effect when responsible persons
leave the network.
Req. 4 – Interoperability: An explicit reference to
the different levels of interoperability and
the need to ensure it is needed.
Req. 5 – Holistic Management Processes: An
explicit reference to the necessity of a
holistic interface management (possibly by
defining responsible persons) is necessary.
4 DISCUSSION & CONCLUSION
The three most widely used IT governance
frameworks considering risk management (COBIT,
ITIL and ISO 27005) were evaluated. Focus of
evaluation was their use for application systems in
integrated care networks. The results show that the
selected IT governance frameworks are not
applicable for risk management in integrated care
networks, especially in Germany. Furthermore, a
stronger analysis of institutionalisation for integrated
care networks is necessary to enable a more powerful
legitimation of the network itself and to subordinate
the independence of participants under the processes
of the network. Additionally, coordination of
individual services or risk management could be a
joint task. The organisation-centred approach, which
is currently applied, possibly needs a shift to a
network perspective, especially in Germany.
To gain further insights on understanding the
coordination process for management, additional
research is needed to transfer intra-organisational
results to an integrated care network. However, the
case example is limited to German and integrated care
characteristics. Additional case studies need to be
conducted to understand the transferability of results
to other countries and to other kinds of networks.
Nevertheless, the literature study has shown that the
problems regarding the framework usage for
networks are fundamental.
All in all, it has been shown that an application of
the frameworks considered is always accompanied by
a large number of restrictions, especially since an
explicit consideration of networks as an
organisational form is not intended. Missing aspects
in this area are, in particular, consideration of
additional consultations, lack of authority and control
(management), incorporation of a flexible number of
participants as well as necessary interoperability and
interface management, resulting from the network
characteristics itself. Nevertheless, risk management
steps, a focus on confidentiality, integrity and
availability as well as operational risks (person-,
process-, system-related and external) are considered
IT-Governance in Integrated Care: A Risk-centred Examination in Germany
815

in all of the frameworks. On the one hand, it can be
said that the evaluated frameworks cannot support the
risk management of application systems in integrated
care networks. However, on the other hand, a transfer
to a network view would be worthwhile due to the
high autonomy of participants in these networks, for
which e. g. ISO 27005 is an adequate guideline.
Further research needs to focus on two aspects:
Firstly, the scenario presented should be completed
by investigating the risk management of the second
hospital and the network itself as well as matching
this with the presented results. Secondly, the findings
of this paper could improve the design process to
develop a risk management framework focussing on
(integrated care) networks. Therefore, strengths of
established frameworks need to be combined and
extended by the requirements provided. A
combination of ISO’s clear structure supplemented
by detailed explanations from COBIT and ITIL’s best
practices could be a good basis.
As a fully integrated IT enables integrated care
concepts, a helpful framework for inter-
organisational care networks can lead to improved
care supply, not only in Germany.
ACKNOWLEDGEMENTS
I thank Hannes Schlieter for his feedback on the topic
and Jeannette Stark for helping me improving the
paper.
REFERENCES
Agrawal, R. C. (2009). Risk Management. ABD Publishers.
Alreemy, Z., Chang, V., Walters, R., & Wills, G. (2016).
Critical success factors (CSFs) for information
technology governance (ITG). International Journal of
Information Management, 36(6), 907–916.
Amelung, V., Hildebrandt, H., & Wolf, S. (2012).
Integrated care in Germany—A stony but necessary
road! International Journal of Integrated Care, 12(1),
1–5.
AXELOS. (2013). ITIL Service Design. The Stationery
Office, London.
Bannerman, P. L. (2008). Risk and risk management in
software projects: A reassessment. Journal of Systems
and Software, 81(12), 2118–2133. https://doi.org/
10.1016/j.jss.2008.03.059
Bistarelli, S., Fioravanti, F., Peretti, P., & Santini, F. (2012).
Evaluation of complex security scenatios using defence
trees and economic indexes. Journal of Experimental &
Theroretical Artificial Intelligence, 24(2), 161–192.
Bogenstahl, C. (2012). Management von Netzwerken: Eine
Analyse der Gestaltung interorganisationaler
Leistungsaustauschbeziehungen. Gabler.
BSI. (2011). IT-Grundschutz: Gefährdungskataloge.
Bundesamt Für Sicherheit in Der Informationstechnik.
https://www.bsi.bund.de/DE/Themen/ITGrundschutz/I
TGrundschutzKataloge/Inhalt/_content/g/g00/g00.htm
l
De Haes, S., Van Grembergen, W., & Debreceny, R. S.
(2013). COBIT 5 and Enterprise Governance of
Information Technology: Building Blocks and
Research Opportunities. Journal of Information
Systems, 27(1), 307–324. https://doi.org/10.2308/isys-
50422
European Commission. (2017). ANNEX to the European
Interoperability Framework—Implementation Strategy
COM (2017) 134 final.
Fenz, S., Heurix, J., Neubauer, T., & Pechstein, F. (2014).
Current challenges in information security risk
management. Information Management & Computer
Security, 22(5), 410–430.
Ferstl, O. K., & Sinz, E. J. (2013). Grundlagen der
Wirtschaftsinformatik. Oldenbourg Verlag.
Gaulke, M. (2014). Praxiswissen COBIT - Grundlagen und
praktische Anwendung in der Unternehmens-IT.
dpunkt. Verlag.
Gröne, O., Garcia-Barbero, M., & WHO European Office
for Integrated Health Care Services. (2001). Integrated
care: A position paper of the WHO European Office for
Integrated Health Care Services. International Journal
of Integrated Care
, 1, e21–e21. PubMed.
Häfner, C., & Felden, C. (2009). Building a framework for
an efficient IT governance (Vol. 231). Techn. Univ.
Berakademie.
Henriksen, E., Burkow, T., Johnsen, E., & Vognild, L.
(2013). Privacy and information security risks in a
technology platform for home-based chronic desease
rehabilitation and education. BMC Medical Informatics
and Decision Making, 13(85), 1–13.
ISACA. (2012). COBIT 5—A Business Framework for the
Governance and Management of Enterprise IT.
ISO. (2011). International Standard ISO/IEC
27005:2011(E)—Information technology; Security
techniques; Information security risk management.
Johnston, R. H., & Vitale, M. R. (1988). Creating
Competitive Advantage With Interorganizational
Information Systems. MIS Quarterly, 12(2), 153–165.
Koch, O. (2005). Unterstützung von einrichtungsüber-
greifenden Kommunikationsprozessen in der
integrierten Gesundheitsversorgung. In
Telemedizinführer Deutschland (pp. 106–109).
Mayring, P. (2000). Qualitative Content Analysis. Forum:
Qualitative Social Research, 2(1), 1–10.
Raupp, M. (2002). Informationsmanagement und
strategische Unternehmensführung. Lang.
Sahibudin, S., Sharifi, M., & Ayat, M. (2008). Combining
ITIL, COBIT and ISO/IEC 27002 in Order to Design a
Comprehensive IT Framework in Organizations. 749–
753.
Scale-IT-up 2020 - Workshop on Best Practices for Scaling-Up Digital Innovations in Healthcare
816

Schüppler, D. (1998). Informationsmodelle für
überbetriebliche Prozesse: Ein Ansatz zur Gestaltung
von Interorganisationssystemen (Vol. 2357). Lang.
Seventy-first World Health Assembly. (2018). Agenda item
12.4—Digital health (WHA71.7; pp. 1–4). World
Health Organization. http://apps.who.int/gb/ebwha/
pdf_files/WHA71/A71_R7-en.pdf
Silva, M. M., Gusmão, A. P. H. de, Poleto, T., Silva, L. C.
e, & Costa, A. P. C. S. (2014). A multidimensional
approach to information security risk management
using FMEA and fuzzy theory. International Journal of
Information Management, 34(6), 733–740.
https://doi.org/10.1016/j.ijinfomgt.2014.07.005
Smith, D. L., & Bryant, J. H. (1988). Building the
Infrastructure for Primary Health Care: An Overview of
Vertical and Integrated Approaches. Social Science &
Medicine, 26, 909–917.
Smith, S. M., Wallace, E., Salisbury, C., Sasseville, M.,
Bayliss, E., & Fortin, M. (2018). A Core Outcome Set
for Multimorbidity Research (COSmm). Annals of
Family Medicine, 16(2), 132–138. Embase.
https://doi.org/10.1370/afm.2178
Suomi, R. (1992). On the Concept of Inter-organizational
Information Systems. Journal of Strategic Information
Systems, 2, 93–100.
Sydow, J. (2006). Netzwerkberatung—Aufgaben, Ansätze,
Instrumente. In J. Sydow & S. Manning (Eds.),
Netzwerke beraten. Gabler.
Vilarinho, S., & da Silva, M. M. (2011). Risk Management
Model in ITIL. In M. M. Cruz-Cunha, J. Varajão, P.
Powell, & R. Martinho (Eds.), ENTERprise
Information Systems (pp. 306–314). Springer Berlin
Heidelberg.
Zambon, E., Etalle, S., Wieringa, R. J., & Hartel, P. (2011).
Model-based qualitative risk assessment for availability
of IT infrastructures. Software Systems Modeling,
10(4), 553–580.
IT-Governance in Integrated Care: A Risk-centred Examination in Germany
817
