
Deus versus Machina: How Much Health-supporting Technology Do
People Allow Depending on the Severity of the Disease?
Wiktoria Wilkowska
a
, Julia Offermann-van Heek
b
and Martina Ziefle
c
Human-Computer Interaction Center, RWTH Aachen University, Campus-Boulevard 57, 52074 Aachen, Germany
Keywords:
Technology Acceptance, Health-supporting Technology, Nursing Care, Disease.
Abstract:
Changes in demographic structures resulting in more and more overburdened healthcare systems require novel
solutions for modern societies. Members of aging populations are confronted with an ever increasing presence
of diseases and seniors frequently suffer from morbidity, which leads to a higher demand of nursing care on
the long run. Bottlenecks in this area can to some extent be relieved by the use of an assistive health-related
technology, but its acceptance and use is entirely dependent on the targeted users. This study considers the
perspective of severely ill persons regarding their nursing care and application of health-related technology
support. Using scenario-based empirical research, participants of an online-study (N = 585) were confronted
with three differently severe diseases and assessed aspects considered relevant for their nursing care and adop-
tion of assistive health-related technologies. Results show significantly differing opinions in dependency on
the severity of a disease. This study highlights several aspects that represent the perspective of diseased per-
sons and provides valuable insights into accepted use of health-enabling technologies and preferred models of
nursing care.
1 INTRODUCTION
While the growth of the world population on earth
continues to rise sharply, in many societies people
live now longer than some decades ago. The aver-
age age has been growing for many years, especially
in the industrialized countries, and the trend remains
unchanged for the time being. The declining number
of younger people and the simultaneously increasing
number of older people, however, continuously shift
the demographic structures. Also in Germany, the de-
mographic change has long since arrived (Statistische
¨
Amter des Bundes und der L
¨
ander, 2011).
The increasing proportion of aged individuals in
a population represents considerable challenges not
only to the economic sector, but it poses especially
challenging requirements to the feasibility and sus-
tainability of healthcare (Fleiszer et al., 2015). As the
probability of needing care increases with age, more
and more people are in need of care as society ages.
The result of this is that fewer and fewer young people
are forced to care for growing numbers of older indi-
a
https://orcid.org/0000-0002-7163-3492
b
https://orcid.org/0000-0003-1870-2775
c
https://orcid.org/0000-0002-6105-4729
viduals, in many ways (Nowossadeck, 2013). Such
a situation causes a rising burden of healthcare ex-
penditures and leads in its consequence to a shortage
of professionals trained to work with the aging part
of the population. The more the population ages, the
more it becomes an important issue of how we are
going to pay for, and deliver, a quality care for the
seniors (Rashidi and Mihailidis, 2012).
At the same time, rapid advances in the informa-
tion technology enable new solutions that can, at least
to some extent, alleviate the challenging situation of
aging societies. In recent years, several integrative ap-
proaches have been developed, focusing on assistance
of individuals – especially seniors, diseased, and im-
paired persons – in their natural home environments.
Paradigms like pervasive computing, ambient intelli-
gence, and ambient assisted living aim at empowering
capabilities of humans by the means of digital envi-
ronments that are unobtrusive, interconnected, sensi-
tive, adaptive, and responsive to their needs (Sadri,
2011). Therein, a multitude of sensors and activators,
applications, functions, single devices to whole sys-
tems are included. Smart homes which are equipped
with such complex technology have a great potential
to support their inhabitants and improve the quality of
the time spent at home. Such technology-enhanced
26
Wilkowska, W., Heek, J. and Ziefle, M.
Deus versus Machina: How Much Health-supporting Technology Do People Allow Depending on the Severity of the Disease?.
DOI: 10.5220/0009370900260037
In Proceedings of the 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2020), pages 26-37
ISBN: 978-989-758-420-6
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

environments are intended to provide greater levels
of independence for their inhabitants, and thus reduce
the need for institutionalized nursing facilities by ex-
tending the time that people can live in their familiar
surroundings.
In addition, information and communication tech-
nology (ICT) is increasingly being used in manage-
ment of (chronic) illnesses. Some common ICT-
applications, including home monitoring of vital pa-
rameters for chronically ill persons or communi-
cation via videophone consultations with medical
staff, facilitate the professional services (e.g., elec-
tronic health records) as well as knowledge man-
agement, such as care rules, protocols, or schedul-
ing (Celler et al., 2003). Jenssen et al. (2016) ar-
gue that there is a growing body of evidence that pa-
tient use of new technologies, enabling to communi-
cate with healthcare providers, can lead to a behavior
change and improved health outcomes. In this con-
text, telemedicine, eHealth, and telecare are key ap-
plications for ICT in healthcare delivery which aim at
specialist consultations and examinations of patients
health state through the use of telecommunication.
With all the available technical solutions, how-
ever, cooperative behavior and a largely accepted in-
teraction with the technology on the part of the per-
sons concerned is indispensable. There is a great
body of literature providing knowledge about applica-
tions for certain groups of diseases and, on the other
side, about the success or failure in their deployment.
In contrast, just a little is known about the willing-
ness to use technology depending on the varying de-
grees of severity of diseases. Therefore, the present
study focuses on the question how far persons suf-
fering from severe diseases allow the use of ambient
technologies which are meant to monitor their health
and support them in managing their day-to-day ne-
cessities associated with their illness. In a scenario-
based survey, we examined how the intention to use
such assistive health-related technology is connected
with emotional states of the persons concerned, who
is allowed to have a say in respect of their therapy and
rehabilitation, and what is the proportion of allowed
care support on the part of human and on the part of
technology.
2 RELATED WORK
In this section, the current research state on the accep-
tance of health-supporting technology innovations is
presented, taking a broad variety of technologies into
account. Also, the perspective of (chronically) ill per-
sons and the relevance of nursing care is stressed and
put in the context of the possibility to be supported by
appropriate technical applications. Finally, the under-
lying research questions are introduced.
2.1 (Health-supporting) Technology and
Its Acceptance
In view of the rapid development of technologies in
various fields, acceptance and use of innovations in
the area of information technology (IT) has been a
major concern for research and practice. Over the last
several decades, many theoretical models have been
proposed and validated in different contexts to exam-
ine the acceptance and to predict the use and long-
term adoption of particular innovations as reliable as
possible. The most prominent models were the Diffu-
sion of Innovation Theory (Rogers, 1983), Theory of
Planned Behavior (Ajzen, 1991), Technology Accep-
tance Model (TAM; Davis, 1989; Davis et al., 1989),
and Unified Theory of Acceptance and Use of Tech-
nology (UTAUT; Venkatesh et al., 2003, 2012), which
have been proposed, examined, and extended, provid-
ing factors which are able to explain to a great ex-
tent the acceptance and use of different technologies.
However, even though the most dominant theoretical
frameworks in the recent years – TAM and UTAUT
– are very robust technology acceptance models, they
have also received criticism for disregarding the pos-
sible fluctuation over time (Peek et al., 2014).
For the present study, especially the context of
health-related technologies, and therein mainly (am-
bient) assistive technologies and systems, are gaining
particular interest as their primary objectives are to
monitor the health of the residents – mostly elderly
and impaired persons – and ensure an appropriate data
exchange as well as communication with physicians,
caring staff, and families. To provide a smoothly op-
erating health-related technology that is able to detect
critical situations, such as falls, relevant changes in
the individuals’ behaviors, and/or sleeping patterns,
a high degree of technology acceptance as well as
consideration of the users’ privacy concerns and ex-
pectations is required (e.g., Kirchbuchner et al., 2015;
Schomakers and Ziefle, 2019).
As research in this area has shown, acceptance
of medical assistance devices or systems, which pre-
dominantly address the senior part of the population,
is associated with a multitude of factors that play
a significant role. However, little is known about
whether or not older adults are ready to adopt and
use them (Jaschinski, 2014). In their review, Peek and
colleagues identified 27 factors influencing the accep-
tance of electronic technology for people who are ag-
ing in place and divided them into six clusters: i. con-
Deus versus Machina: How Much Health-supporting Technology Do People Allow Depending on the Severity of the Disease?
27

cerns regarding technology, ii. benefits of technology,
iii. need for technology, iv. alternatives to technol-
ogy, v. social influence, and vi. characteristics of
older adults (Peek et al., 2014). Nevertheless, a bulk
of these factors have not yet been tested in a quanti-
tative way. What has been substantiated by research,
however, is that acceptance of medical technologies
depends on perceptions of technology-related benefits
and barriers. Many studies in this context provided
evidence that assistive technologies were mostly as-
sessed favorably, whereas for elderly people and those
in need of care such benefits, like independent living,
feeling of safety, monitoring of health, and possibility
of staying at the own home, are especially appreciated
(Wilkowska, 2015; G
¨
overcin et al., 2016). Yet, per-
ceived obstacles can also cast a shadow over the moti-
vation for the use of assistive technologies. One of the
most decisive barriers are concerns referring to pri-
vacy (e.g., Yusif et al., 2016; Wilkowska et al., 2015),
which is a highly complex concept that involves dif-
ferent perspectives and dimensions (Little et al., 2007;
Schomakers and Ziefle, 2019). The desire for privacy
largely depends on the context and the individual at-
titudes (Bergstr
¨
om, 2015), but regarding the assistive
technology it has also been showed to vary between
different groups of individuals, like gender groups
or groups referring to the users’ health conditions
(Wilkowska and Ziefle, 2012), culture (Alag
¨
oz et al.,
2011), as well as social and physical environmental
factors (Himmel and Ziefle, 2016; Schomakers and
Ziefle, 2019). Other frequent barriers referring to the
acceptance of ambient technologies include, among
others, fears of surveillance and isolation from so-
cial contacts (van Heek et al., 2018), use of specific
types and placements of the technology (Himmel and
Ziefle, 2016; Kirchbuchner et al., 2015), perceived
control over the technology (van Heek et al., 2017),
trust, and the context of use (Montague et al., 2009;
van Heek et al., 2016; Wilkowska and Ziefle, 2018).
Given all the factors known to impact the health-
related technology acceptance and considering the
fact that in the given context the technology adop-
tion addresses especially the seniors, as they fre-
quently suffer from multi- and comorbidity, the ques-
tion arises if technology acceptance is significantly in-
fluenced by the severity of diseases.
2.2 Use of Health Information
Technologies for Diseases
Almost everyone wants to live as long as possible in-
dependently at home. However, age-related increase
of the probability for diseases and loss of functions in
persons aged 65 years and older frequently leads to an
ever greater loss of this autonomy (B
¨
ohm et al., 2009;
Barrett, 2011).
Older adults in this stage of life are likely to
suffer from one or more (chronic) diseases (Maren-
goni et al., 2011), experience changes of the im-
mune system and the endocrine system, which are
associated with disability, poorer health outcomes,
and lower quality of life (Fuchs et al., 2012). This
highly prevalent co-occurrence of chronic health con-
ditions among older individuals leads not only to the
need for preventive efforts, but a the same time to a
higher need for healthcare support, which can be, at
least partly, undertaken by the health-enabling tech-
nology equipment. Haux (2006) argued that with the
availability of health-enabling information technolo-
gies and the perspective of having adequate transin-
stitutional health information systems architectures,
a substantial improvement can be made to a better
patient-centered care, with possibilities ranging from
regional, national, to even global care. Applying ap-
proaches like AAL and ambient intelligence solutions
can even transfer such specific and to the individual
needs tailored care to private environments.
Such a development has the potential to contribute
to an efficient and affordable healthcare and would
support older and impaired persons to persevere an
independent life. However, in view of all the cur-
rent technological innovation little is known about the
willingness to use such assistive technology in the re-
lation to varying degrees of severity of disease by the
parties concerned. In this context, many ethical and
practical questions arise which refer not only to the
degree to which diseased persons wish to use such
technologies, but also to their emotional feelings con-
nected with their health condition and the associated
consequences. Also important are aspects, like how
should the patient’s care be structured and who may
decide on therapy and rehabilitation measures. In the
following, research questions of the present study are
described in more detail, attempting to empirically
elucidate these aspects, using a representative sample
of the German population.
2.3 Research Questions
Given the current demographic situation and the ex-
pected bottlenecks for the healthcare sector, on the
one side, and taking advantage of the sophisticated
health-supporting technologies, on the other, this
study focuses on questions referring to the individu-
als’ perceptions and acceptance of such innovations in
their lives and closer environments through the prism
of a serious illness.
In concrete terms, it is unclear how persons emo-
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
28

tionally sense when they are ill, which is probably sig-
nificantly associated with the given situations, states
of the disease, and not least people’s personalities. It
is worthwhile to examine whether certain profiles can
be assigned to certain disease-related situations, and
thus permit to develop meaningful strategies. More-
over, it is highly interesting to what extent such sen-
sations affect the decisions about the use of health-
supporting technologies. In this study, we therefore
ask (RQ1): Do emotional and ethical sensations ac-
companying ill persons differ in dependency of the
severity of the disease?
In this context, it is furthermore of interest how the
emotional state correlates with, or even significantly
affects, the motivation to be supported in case of ill-
ness. In terms of this study, we ask (RQ2): Does the
intention to use medical technology significantly vary
depending on the severity of the disease?
Moreover, in case of (severe) illnesses, people fre-
quently get in situations, which require decisions re-
garding their further/future treatment. In this context,
this study examines also (RQ3): To what extent other
important stakeholders (doctors, family members) are
allowed to make decisions about therapeutic and re-
habilitation measures associated with the disease?
Not least decisions about the use of health-
supporting technologies or applications are important
and in this context it is of interest, to what extent do
people affected by (severe) diseases allow technology
to support them in their convalescence? More specif-
ically, the question arises as to the extent to which
the use of health-supporting technologies may com-
pliment, (partially) take over the job, or even replace
caregivers. We therefore also examine in this study
(RQ4): To what extent do ill people allow the use of
medical technology next to the support of the human
caregiver(s)?
3 METHOD
In this section, the methodological approach, the op-
erationalization of the questions described are pre-
sented, and the study’s sample is introduced.
3.1 Quantitative Data Collection
This study used an online-survey as method for the
data collection and was structured as follows: At the
beginning, participants were asked for their socio-
demographic information regarding age, gender, pro-
fessional background, self-confidence in dealing with
technology (Beier, 1999) as well as general state of
health, subjective vitality (Ryan and Frederick, 1997),
and the general health condition coupled with the
presence or absence of chronic disease(s). In this part
of the survey, respondents also indicated their expe-
rience with health-supporting devices in their daily
lives.
Further, the survey focused on perceptions of cri-
teria related to aging, like a high quality of life in old
age (e.g., self-supply in daily life, competent medical
care, consistent social network, etc.) as well as as-
pects referring to positive and negative effects of ag-
ing [for details see Wilkowska et al. (2019)]. Another
part of the survey evaluated general attitudes towards
the use of medical technology (e.g., ”I can imagine
the use of medical technology.”) as well as the par-
ticipants’ (intended) use and assessments of health-
supporting technologies in the form of benefits and
barriers. Participants expressed their (dis-)agreement
to the respective items on a 6-point Likert-scale rang-
ing from 1 (”I do not agree at all”) to 6 (”I fully
agree”).
The last part of the questionnaire represents the
central content of this paper. Here, three different
scenarios were introduced, varying the severity of a
disease. The intention was to make the participants to
envision and, as far as possible, empathize with the ill
persons in the situations presented in the scenarios (S
I-III). In the following, the scenarios are presented in
their respective wordings:
Scenario I: ”After a serious car accident, you are
hospitalized. You have suffered various bone frac-
tures and your stay at the hospital will probably last
about 2 weeks. Afterwards, you have to expect many
weeks of healing (including a splint on your leg).
This situation implies also other consequences which
means that you are professionally absent for a few
months and need some nursing support at home (at
least for the time when you are bedridden and wear
plaster splints). However, according to doctors, a
complete recovery can be expected in the long term.”
Scenario II: ”After two heart attacks, you now suf-
fer from chronic heart failure in stage three. This
means that even slight physical exertion can cause
you to become exhausted, suffer from arrhythmias or
breathlessness. According to this, you need an inten-
sive (nursing) care and a lot of support in your every-
day life. In addition, you need to visit a doctor and
undergo rehabilitation measures on a regular basis.
The insurance experts classify you as no longer fit for
work due to your state of health and they force you
to take early retirement. The therapy of the disease is
possible to a certain extent, but it is also very com-
plex (i.e., drug therapy, rhythmological therapy with
pacemaker devices, targeted body training, appropri-
ate diet, etc.). By treating the causes and thanks to
Deus versus Machina: How Much Health-supporting Technology Do People Allow Depending on the Severity of the Disease?
29

the complex treatment measures, the prognosis is im-
proved, but unfortunately a high mortality rate is a
sad reality.”
Scenario III:”Please put yourself in the difficult sit-
uation in which you suffer from colorectal carcinoma
and your body is very severely impaired and weak-
ened as a result of a chemotherapy and the following
radiation therapy. You can manage your everyday life
only with the intensive support of a trained nursing
staff. You need support in terms of personal hygiene
and daily meals as well as regarding your mobility
needs. In this respect, you will be supported by both
professional carers and your family members. The
chances of recovery through surgery and chemother-
apy depend decisively on the stage and course of the
disease (on average the five-year survival rate is 40-
60%). Unfortunately, the near future is uncertain.”
The order of the scenarios was randomized. After
each scenario, participants worked through four ques-
tion blocks, referring to topics that are relevant for a
disease and the associated consequences. The first re-
ferred to the question who, and to what extent, may
have a say in decisions regarding a further medical
treatment. The possible stakeholders were ’myself’,
’the doctor’ and the ’nuclear family’, and the possible
answer alternatives were ’not at all’ (0%), ’a little’
(25%), ’partly’ (50%), ’for the most part’ (75%), ’en-
tirely’ (100%). The second block of questions used
the psychological method of the semantic differential
(Osgood et al., 1957), in which respondents’ judg-
ments had to be placed on a 10-step scale between two
poles of a dimension described by a pair of two ad-
jectives (e.g., threatening—conforming, hopeless—
hopeful, vulnerable—protected). With these, the state
of people’s emotional sensations and ethical percep-
tions was examined after each scenario. The third
group of questions referred to the intention to use
health-supporting medical equipment. We used the
three following items: ”In the context of the scenario,
...
• ...I can imagine the use of medical supportive
technology.”
• ...I consider the use of medical technology use-
ful.”
• ...I do not want to use medical technology at all.”
The respondents could express their (dis-)agreement
regarding these statements on a 6-point Likert-scale.
After re-coding of the negatively poled item, scales
for the intention to use the medical assistive technol-
ogy were built and reached sufficient internal validi-
ties (S I: α=.78, S II: α=.80, S III: α=.81); the par-
ticipants could reach in this regard 3 (=low intention)
to 18 points (=high intention). In the fourth block of
questions, the survey collected the participants’ opin-
ions about which caring/nursing model they would
ideally prefer with regard to the particular scenario.
Four alternatives were presented, and the respondents
had to choose the most preferred one: i. only nurs-
ing persons/caring staff (100% human), ii. for the
most part nursing staff and partly intelligent technol-
ogy (70% human and 30% medical technology), iii.
half intelligent technology and half nursing staff (50%
medical technology and 50% human), and iv. entirely
intelligent technology (100% medical technology).
Eventually, two last questions were asked to the
survey participant: “If you had the choice to decide:
may technology prolong life?” and “. . . may technol-
ogy delay dying?” In this case, only yes/no-answers
were possible.
3.2 Research Approach
The empirical study aimed at an investigation of opin-
ions regarding the support of individuals with frail
health conditions by medical technology (e.g., mon-
itoring technologies). For this purpose, respondents
assessed aspects related to decisions about handling
of situations of (severe) diseases and the associated
consequences in an online-survey.
Using a scenario-based method, participants were
introduced to three different situations referring to
varying severity of a medical condition. After each
scenario, which is treated in this study as an inde-
pendent variable, data on the following aspects, i.e.,
dependent variables, were collected:
• Ethical, emotional, and social sensations,
• Intention to use health-supporting technologies,
• Permission for others to participate in the deci-
sions on the future medical treatment,
• Desired proportion of the support from humans
(i.e., caregivers) vs. health-supporting technol-
ogy.
This study intended to provide an overview of the
above aspects depending on the severity of a disease
and the associated consequences (three scenarios as
described in Section 3.1), taking the German popu-
lation as an example. Figure 1 shows the schematic
outline of the examined variables.
3.3 Description of the Sample
A total of N=585 respondents completed the online
survey and were taken into consideration for statisti-
cal analyses in this study. A possibly broadest spec-
trum of the German population was addressed, in-
cluding differently aged male and female individuals,
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
30

Figure 1: Research Design of the Study.
with different professional backgrounds, life experi-
ences, and socio-economic statuses. The sample cov-
ered different professions, including individuals from
engineering and IT-sectors, education and economy
as well as health professionals and employers from
the social sector.
The participants were German adults, ranging in
age between 16 and 84 years (M=47.2; SD=16.6) and
the sample was quite balanced with 48% female and
52% male respondents. As the highest educational
levels, 21.5% of the participants reported to hold an
academic degree and 35.7% completed an apprentice-
ship. A further 19.1% of the sample stated to hold
a university entrance diploma, and 23.6% reported a
secondary school certificate as an educational gradu-
ation. The resulting know-how connected to the tech-
nology use and the general level of self-confidence in
this regard was for this sample quite high (M=18.2;
SD=4.4, from a maximum of 25 points).
Since health played a central role in the study, ad-
ditional information regarding health status and ex-
perience with the use of health-supporting technical
equipment was also asked for in the questionnaire.
More than one third of the sample (35.7%) reported
to be in very good health and further 18.8% stated to
suffer from a chronic condition, but to manage it very
well in the everyday life. Another considerable part
of the participants (41.9%) indicated to be somewhat
limited due to a chronic illness and 3.6% reported to
be dependent on the support of others (relatives / nurs-
ing care professionals). Moreover, less than half of
the sample (44.3%) reported experience with health-
supporting devices, like heart rate monitors, blood
pressure meters, activity monitors, or blood sugar me-
ters.
Participants were recruited for this study through
a professional survey panel platform, which enabled
to gather a representative sample of the German soci-
ety. They were paid for the participation by the survey
panel’s institute. The composition and the character-
istics of the sample are described further below.
4 RESULTS
For the statistical analyses of perceptions referring
to an accepted use of health-supporting technologies
in case of (severe) illness, repeated measures analy-
ses of variance (rmANOVA) were applied in order to
compare three different scenarios. As non-parametric
alternative the Friedman Test was used. For effect
size measures, the parameter partial eta squared (η
2
)
is reported according to (Cohen, 1988) and the sig-
nificance value in the multivariate tests was taken
from Wilks’ Lambda. If the assumption of sphericity
was violated (Mauchly’s Test < 0.05), Greenhouse-
Geisser correction was used. In the following, means
(M) and standard deviations (SD) are reported for de-
scriptive analyses and the level of statistical signifi-
cance (p) is set at the conventional level of 5%.
4.1 Emotional State of the Persons
Concerned
After each scenario, participants were asked to pos-
sibly realistically envision the outlined situation and
to rank their emotional states on scales, lying be-
tween two adjectives that refer to particular dimen-
sions. Figure 2 depicts the resulting means for the
three scenarios.
Figure 2: Ethical and Emotional Sensations for the Three
Illness-Scenarios (S I-III).
Evidently, the sensations significantly differed de-
pending on the scenario and this result is also reflected
in the statistical calculations. Only the polarity pro-
file of scenario I showed in part positive judgements:
Those affected felt in such a situation worthy, opti-
mistic, and hopeful, they were able to accept the dis-
ease to some extent, and regarded it as temporary. As
opposed to this, in the situation of scenario III, partic-
ipants felt threatened and vulnerable, and felt a certain
finality of their state. Repeated measures analyses of
Deus versus Machina: How Much Health-supporting Technology Do People Allow Depending on the Severity of the Disease?
31

variance with a Greenhouse-Geisser correction deter-
mined statistically significant differences between all
adjective pairs between the three degrees of severity
of a disease. The relevant statistical parameters de-
picting this effect are summarized in Table 1, provid-
ing evidence that the emotional and ethical sensations
sharply worsen the more severe the disease.
4.2 Intention to Use Medical
Technology
Given the different emotional states, it can be as-
sumed that these are associated with the willingness
to use medical supportive technologies. In this sec-
tion, it is therefore interesting (1) whether this will-
ingness changes significantly depending on the sever-
ity of the disease, and (2) to what extent this willing-
ness significantly correlates with the frames of mind
in each scenario.
A rmANOVA comparing the intention to use
health-supporting technology in dependency of the
severity of the disease revealed statistically significant
differences (F(1.9,1005.8)=7.3, p6.001, η
2
=.01).
Even though, according to the effect size the differ-
ences were small, the intention to use assistive tech-
nologies diminished the more severe was the illness.
Figure 3 depicts these differences.
Figure 3: Intention to Use Health-Supporting Technology
Depending on the Severity of an Illness.
In the next step, correlative relationships to the
previously collected emotional and ethical concerns
were analysed, relating these to the respective scales
for intention to use assistive technology in each sce-
nario. The resulting coefficients are summarized in
Table 2. For statistical purposes, the adjective pairs
were coded in such a way that the ”negative” expres-
sions show low numbers (adjectives on the left side,
e.g., lonely = 1) and the ”positive” expressions show
high values of the scale (adjectives on the right side,
e.g., social = 10).
The resulting coefficients generally display rather
weak correlations. It is striking that the associa-
tions are almost consistently significant in the sce-
nario with the most optimistic healing prospects (S
I). The mostly positive directions of the values sug-
gest that an affirmative attitude to the current state
of health goes along with a higher acceptance of the
use of health-supporting technology. Especially, the
confidence about the temporary and not stigmatizing
character of the health status as well as the hopeful ex-
pectation of healing indicate stronger correlative rela-
tions with the intention to use technological support.
Moreover, the clarity of correlative relationships
decreases in disease scenarios with more severe states
of health and less positive prospects for the future (S
II, S III). There, statistically significant associations
are less pronounced, but the alignment of the result-
ing coefficients is the same in both scenarios. The
results indicate that there is less willingness to use
the assistive technology equipment, the more threat-
ening and depending people perceive their health sta-
tus. In contrast, the more they accept their situation
and have a hopeful and socially oriented attitude, the
more the tendency for an open-minded use of techno-
logical support for their health.
Summing up, the results show that the emotional
state of the persons concerned is significantly corre-
lated to the intention to use health-supporting tech-
nology.
4.3 Who Is Allowed to Decide?
Closely linked to these considerations is also the
question of who can have a say in the various ther-
apeutic measures and thus in the shared use of infor-
mation technology for health purposes in the event of
a more or less serious illness. In the questionnaire, we
therefore asked the participants to quote the extent to
which they would allow – besides themselves – peo-
ple, like the doctor in charge and family members, to
have a say in decisions regarding their further treat-
ment (again depending on the severity of the disease
in the three scenarios). In order to ease the visibility
and comprehensibility of the results, only the results
of the answers relating to 100% decisions (”may fully
decide”) are presented below (Figure 4).
Interestingly, the resulting percentages did not dif-
fer considerably in the scenarios. This finding leads
to the conclusion that independently from the severity
of the disease individuals mostly wish to decide about
their medical treatment by themselves. With regard to
the ’other people’ who might have a say in the mat-
ter of the therapeutic treatment in case of illness, the
preferences are distributed between the treating physi-
cians and family members, although the proportion is
slightly higher for the physicians.
Thus, according to the results, in case of ill-
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
32
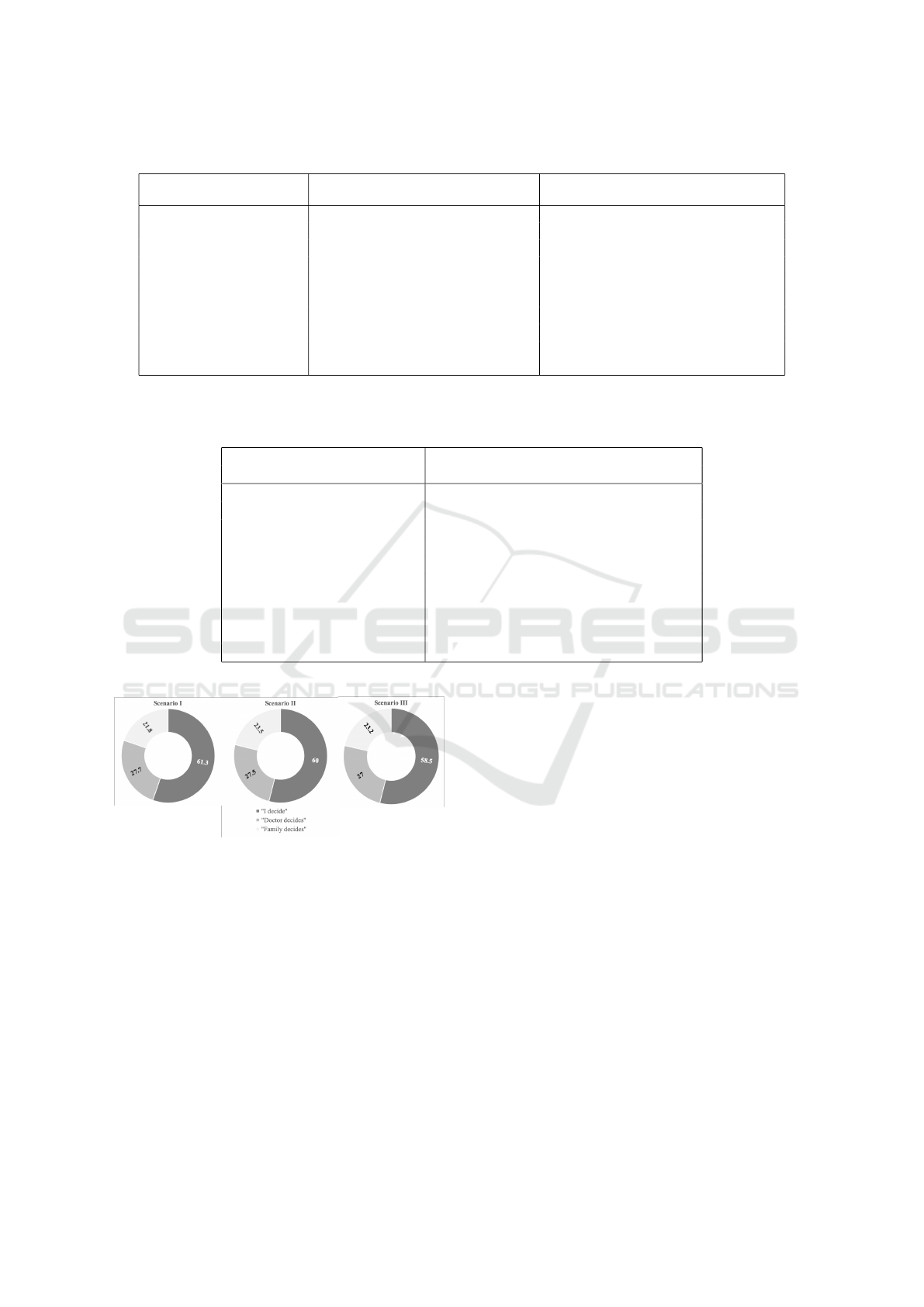
Table 1: Effect of the Severity of a Disease on Emotional and Ethical Sensations in Persons Concerned.
Pairs of adjectives Within-Subjects Effects Means (SD)
Scenario I Scenario II Scenario III
threatening vs. comforting F(1.8,969.3)=275.7, p6.001, η
2
=.34 5.3 (2.4) 3.2 (2.4) 2.9 (2.6)
unworthy vs. worthy F(1.9,982.8)=156.5, p6.001, η
2
=.14 5.0 (2.3) 4.3 (2.2) 3.6 (2.2)
uncontrol. vs. controllable F(1.9,1032.8)=223.3, p6.001, η
2
=.29 6.2 (2.4) 4.4 (2.5) 3.7 (2.7)
depending vs. autonomous F(1.9,999.8)=84.1, p6.001, η
2
=.14 5.0 (2.2) 4.3 (2.2) 3.6 (2.2)
lonely vs. social F(1.9,1054.7)=105.8, p6.001, η
2
=.16 5.4 (2.3) 4.3 (2.3) 4.0 (2.4)
pessimistic vs. optimistic F(1.9,882.7)=215.9, p6.001, η
2
=.31 6.8 (2.3) 5.0 (2.3) 4.4 (2.3)
vulnerable vs. protected F(1.8,983.6)=197, p6.001, η
2
=.27 5.2 (2.3) 3.6 (2.4) 3.2 (2.5)
stigmatizing vs. acceptable F(1.9,947.7)=123.2, p6.001, η
2
=.20 6.8 (2.0) 5.6 (2.1) 5.2 (2.2)
final vs. temporary F(1.7,927.3)=396.4, p6.001, η
2
=.42 6.9 (2.4) 3.7 (2.2) 3.6 (2.4)
hopeless vs. hopeful F(1.8,991.1)=339.5, p6.001, η
2
=.38 7.0 (2.3) 4.5 (2.5) 4.0 (2.5)
Table 2: Pearson’s Correlation Coefficients between the Intention to Use (ItU) Health-Supportive Technologies and the Emo-
tional States Based on Pairs of Adjectives in the Three Scenarios (Significant Values Are Bold; Level of Significance: *p6.05,
**p6.01).
Pairs of adjectives ItU
Scenario I Scenario II Scenario III
threatening vs. comforting r = .04 r = −.17** r = −.16**
unworthy vs. worthy r = .18** r = .09* r < .01
uncontrolable vs. controllable r = .18** r = .08 r = −.08
depending vs. autonomous r = − .11** r = −.10* r = −.17**
lonely vs. social r = .12** r = .13** r = .10*
pessimistic vs. optimistic r = .18** r = .04 r = .02
vulnerable vs. protected r = .09* r = −.02 r = −.08
stigmatizing vs. acceptable r = .21** r = .16** r = .12**
final vs. temporary r = .30** r = −.06 r = .01
hopeless vs. hopeful r = .38** r = .13** r = .11**
Figure 4: Percentage Rates Presenting Decisions about
Who May Fully Decide about the Further Therapeutic
Treatment Depending on the Severity of the Disease.
ness people predominantly wanted to decide by them-
selves, even when their state of illness was very se-
vere.
4.4 Human vs. Technology in the
Nursing Care?
Finally, one of the research questions referred to the
extent to which ill people would allow the use of med-
ical technology next to the support of human care-
giver(s).
To examine this question, after each scenario re-
spondents had to choose one preferred caring model
among the following four alternatives: i. 100% hu-
man care (coded as 1), ii. mainly professional hu-
man carers (70%) and partly medical assistive tech-
nology (30%; coded as 2), iii. partly assistive tech-
nology (50%) and partly human care (50%; coded as
3) and iv. 100% technology (coded as 4). In order
to determine statistically significant differences be-
tween the preference models, Friedman test was ap-
plied. Results of this non-parametric measure suggest
that there are significant differences in the preferences
of the nursing care models depending on the sever-
ity of the disease (χ
2
(2)=7.6, p=.022, n=543). Fig-
ure 5 summarizes the preferences for all caring mod-
els, depicting the three scenarios which refer to the
severity of the disease. It can be seen that the partici-
pants mostly preferred the mixed models (ii. and iii.),
where in case of illness a combined support of hu-
man and technology is offered. The percentage rates
resulting for the three scenarios do not vary signifi-
cantly within the different caring models. Overall, the
highest percentage rates resulted for the caring model,
where technology (50%) and human support (50%)
are balanced (iii.). It is noteworthy, however, that per-
Deus versus Machina: How Much Health-supporting Technology Do People Allow Depending on the Severity of the Disease?
33
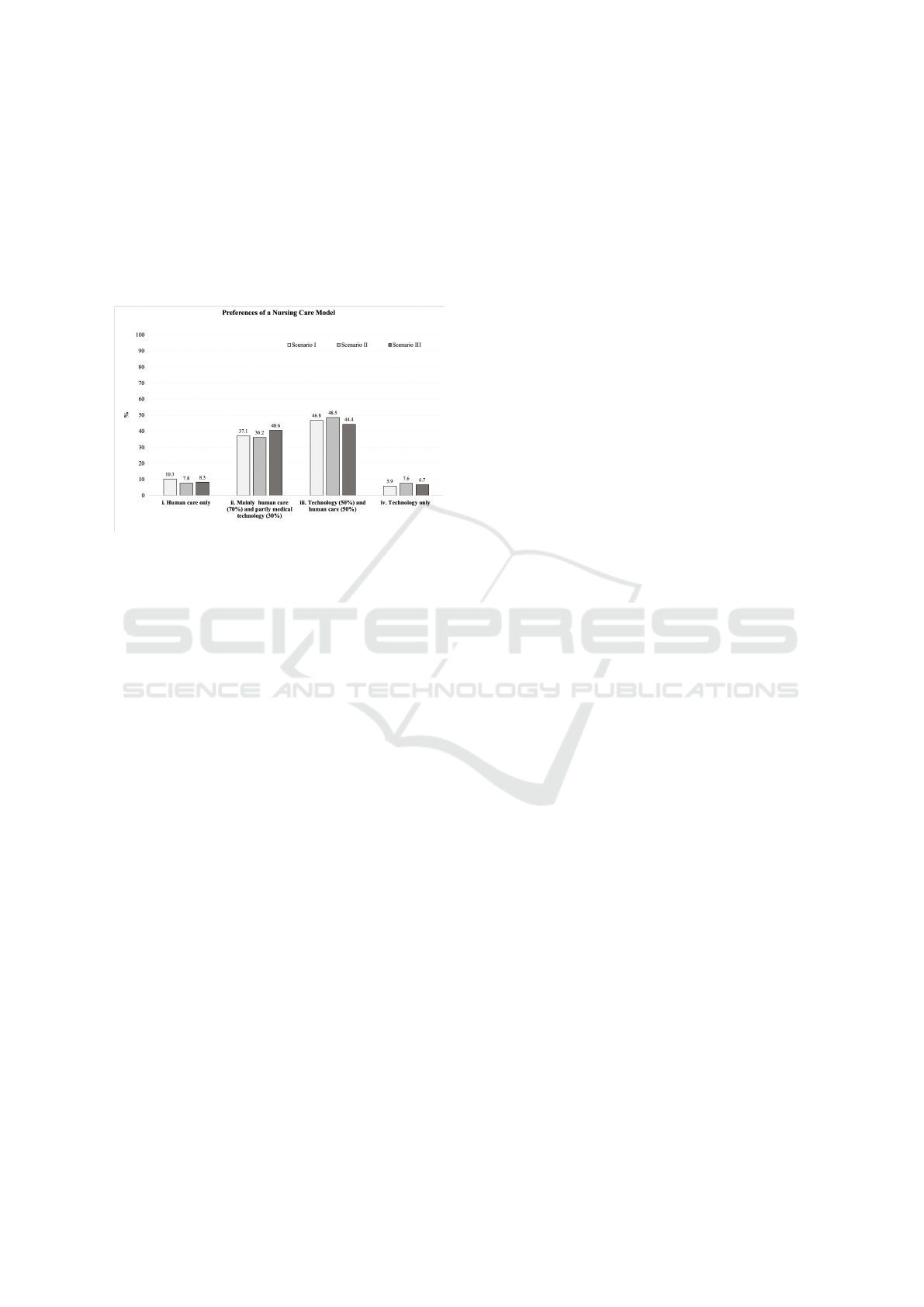
sons suffering from a serious illness, like the colorec-
tal cancer in our example (S III), rather prefer the al-
ternative of ”mainly human (70%) and partly technol-
ogy care (30%)” (ii.), while this caring model in the
less fatal health conditions (S I, S II) was slightly less
preferred. On the contrary, the alternatives of ’100%
human care’ (i.) and ’100% technology’ (iv.) were
chosen only by small proportions of the sample.
Figure 5: Percentage Rates in Preferences of Nursing Care
Models Depending on the Severity of the Disease.
These outcomes let conclude that regardless of the
severity of the disease the preferred models of care
allow for both human carers and technology to take
care for, and support, their health.
5 DISCUSSION
Aging in place in a familiar environment and as close
as possible to the own family is one of the most as-
pired ways of life for seniors. However, with increas-
ing age people are often tormented by (multiple) ill-
nesses, which thwart these plans or make this wish
even impossible due to the needs of care and support
for their everyday lives. Today’s technology develop-
ment has great potential in the area of healthcare, to
support people who need clear therapy for the conva-
lescence process or rehabilitation measures, and also
for those who need just some support in mastering of
their everyday tasks. This can happen, at least partly,
in their own home environments, using the merits
of the ambient technologies or systems, sensor-based
networks for activity monitoring, fall detection, and
various other health-supporting applications.
But how do the elderly ”tick”? A lot of research
has been done to develop, evaluate, and optimize
current technical applications, but relatively little is
known about what the potential users – in this case
the elderly, impaired, and chronically ill ones – want,
how they feel about their particular state of health, and
what they are willing to allow regarding these techni-
cal solutions in their individual situations. There are
some facts which one must not lose sight of: First,
the today’s old people are mostly technologically so-
cialized in different matter (Sackmann and Winkler,
2013) than the so-called generation X or Y, and they
have completely different relations to the use of tech-
nologies. Second, in an acute state of illness, the pri-
orities lie in the recovery and may be completely dif-
ferent from those in a normal or stable state of health:
It is thus quite conceivable that in such a state one no
longer has the capacity to use, or learn to use, tech-
nologies even when these are very supportive. Third,
according to studies (e.g., Loft et al., 2019) and from
the psychological point of view, human contact is of
the utmost importance for recovery and mental stabil-
ity, especially for the elderly, who are often socially
isolated or neglected. It may therefore be the case
that diseased persons turn generally more to people
than to technology.
5.1 Perceptions of the Diseased Persons
The presented study examined such considerations
and can answer the research questions asked at the
beginning on the basis of empirical data. Findings
revealed that the emotional and ethical sensations
sharply worsen, the more severe is the disease. Even
if this result is not particularly surprising in itself, in
the context studied here this is an important insight.
As opposed to health conditions which have
prospects of a secure recovery, seriously ill people
feel threatened, vulnerable, and dependent. These in-
dividuals experience a certain sense of finality and un-
controlled state of their health, and they find it diffi-
cult to show a hopeful attitude. In addition, the emo-
tional states have been shown to be essentially related
to the willingness of using health-enabling technolo-
gies. Statistical calculations provided evidence that
the intention to use the health-assisting technology di-
minishes with the severity of the disease; even though
the here provided effect was not very strong. Corre-
lating the intention to use the health-enabling equip-
ment with the emotional states of persons suffering
from differently severe diseases suggests that an affir-
mative attitude due to an optimistic health prospects
goes along with a higher technology acceptance. On
the other side, there is also less willingness to use the
assistive technology, the more threatening and depen-
dent individuals perceive their health situation.
Therefore, in order to actually make use of the
support offered by medical technology at this point
in people’s lives, a special sure instinct is needed.
Because no one can expect that seriously ill people
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
34

leave the decision about the necessary treatment in the
hands of others (e.g., medical professionals). On the
contrary, the current study showed that regardless of
the severity of the disease people want to decide pri-
marily by themselves about measures regarding their
therapy and/or rehabilitation. Although they grant
doctors – in particular – but also family members a
say in decisions about their health, according to the
above findings they want to keep the final word, even
if they are terminally ill.
In addition, there were only few of those who pre-
fer a nursing care based only on the technology or
coming only from the human. The majority of respon-
dents preferred models combining the sensitivity of a
human carer and the efficiency of the smart assistive
technologies. In this regard, individuals with rather
positive chances for recovery tend to permit more sup-
port from the technology side (50%), whereas the se-
riously ill persons would rather choose the care alter-
native with a higher proportion of human care (70%)
and less proportion of technology care (30%). In any
case, it seems to be an unanimous opinion that the use
of health-related technology should always be a free
choice of the persons concerned. This result corrob-
orates previous findings (e.g., Hofstede et al., 2014)
and shows that there is a fine line in decisions between
human (’deus’) vs. machine in disease situations and
this quite complex process cannot be unambiguously
determined beforehand.
Returning to the research questions formulated at
the beginning, the following findings can be summa-
rized on the basis of the presented results:
• Emotional and ethical sensations accompanying
ill persons significantly differ depending on the
severity of a disease and are significantly re-
lated to the intention to use assistive technology
for health purposes. The intention itself differs
slightly between the scenarios, decreasing with
the increasing severity of an illness.
• Other persons, considered important in the course
of a disease (e.g., doctors, family members), are
allowed to support decisions about the associated
therapeutic and rehabilitation measures. Yet, a
majority of respondents wishes to make such de-
cisions by themselves, regardless of the severity
of their illness.
• Ill people allow the use of medical technology,
but they would rarely rely only on the technology
as caregiver/support in case of severe diseases.
Much more, the more severe is the health status of
the person concerned the more mixed caring mod-
els are desired with the tendency to prefer more
nursing care from professional staff (70%) than
from technology (30%).
On a final note, it is valuable to take a closer look
at one of the last questions of the survey, asking if
technology is allowed to prolong life. Almost 76%
of the participants responded with ”yes”, but still one
out of four persons (24%) does not allow technology
to extend his or her greatest good. At this point, it is
not clear – yet of great interest – who are the persons
which decide against the support brought by techni-
cal innovations, but the result itself represents an im-
portant ethical question, which cannot be disregarded
in the context of using assistive technology to deliver
healthcare.
5.2 Limitations and Directions for
Future Research
Especially the last described result makes the impor-
tance of further, deepening research in this area par-
ticularly plausible. In addition, there are still some
limitations of the present research to be addressed in
future studies.
In the first place, it should not be disregarded that
this study only depicts the perceptions and opinions
of people who have envisioned particular health states
on the basis of disease scenarios, and are not based
on real experiences of ill persons with acutely or in
the past experienced disease states. This can lead to
considerable distortions and should thus be validated
in the future to get even more informative results.
Another limitation applies to the fact that the pre-
sented results are very general. Yet, the interesting
questions are hidden in the particular participants’
characteristics, which are considered important for
the issues presented, like age groups, different lev-
els of technical confidence, and preparedness to use
technology solutions for health matters. Further stud-
ies should thus focus more on these aspects.
In addition, to enrich understanding of peo-
ple’s assessments and their intended use of health-
supporting equipment in case of illness, examinations
of their personality as well as compliance would pre-
sumably add value to the current research. Insights in
this regard could enable to evolve appropriate strate-
gies to the therapy and rehabilitation measurements
for people with different illness and personality pro-
files.
Overall, this study gives first insights into the rel-
evant topic of the perspective of ill persons for whom
the use of assistive health-related technologies repre-
sents an important alternative enabling to live an au-
tonomous life. Further studies are necessary from the
perspective of those affected to deepen this knowl-
edge and to apply it in the practice in an optimized
way.
Deus versus Machina: How Much Health-supporting Technology Do People Allow Depending on the Severity of the Disease?
35

6 CONCLUSIONS
User perceptions of, and their willingness to use, elec-
tronic health-related technology are important deter-
minants of its successful implementation. The knowl-
edge about how to provide an accepted technology-
enhanced assistance is, however, multifaceted and
requires especially the perspective of persons con-
cerned. This study highlights several aspects that rep-
resent the perspective of the diseased and provides
valuable hints on preferred models of nursing care.
ACKNOWLEDGEMENTS
Authors thank all respondents for the participation
and sharing their opinions on aspects referring to the
acceptance of assisting technologies in health-related
context. This work resulted from the project PAAL
(Privacy Aware and Acceptable Lifelogging services
for older and frail people) and was funded by the
German Federal Ministry of Education and Research
(16SV7955).
REFERENCES
Ajzen, I. (1991). The theory of planned behavior. Or-
ganizational behavior and human decision processes,
50(2):179–211.
Alag
¨
oz, F., Ziefle, M., Wilkowska, W., and Valdez, A. C.
(2011). Openness to accept medical technology-a cul-
tural view. In Symposium of the Austrian HCI and Us-
ability Engineering Group, pages 151–170. Springer.
Barrett, L. L. (2011). Healthy@ home 2.0. AARP Research
& Strategic Analysis.
Beier, G. (1999). Kontroll
¨
uberzeugungen im Umgang mit
Technik [Locus of control when interacting with tech-
nology]. Report Psychologie, 24(9):684–693.
Bergstr
¨
om, A. (2015). Online privacy concerns: A broad
approach to understanding the concerns of different
groups for different uses. Computers in Human Be-
havior, 53:419–426.
B
¨
ohm, K., Mardorf, S., N
¨
othen, M., Schelhase, T., Hoff-
mann, E., Hokema, A., Menning, S., Sch
¨
uz, B., Sul-
mann, D., Tesch-R
¨
omer, C., et al. (2009). Gesundheit
und krankheit im alter [health and disease in old age].
Celler, B. G., Lovell, N. H., and Basilakis, J. (2003). Us-
ing information technology to improve the manage-
ment of chronic disease. Medical Journal of Australia,
179(5):242–246.
Cohen, J. (1988). Statistical power analysis for the behav-
ioral sciences. 2nd.
Davis, F. D. (1989). Perceived usefulness, perceived ease of
use, and user acceptance of information technology.
MIS quarterly, pages 319–340.
Davis, F. D., Bagozzi, R. P., and Warshaw, P. R. (1989).
User acceptance of computer technology: a compari-
son of two theoretical models. Management science,
35(8):982–1003.
Fleiszer, A. R., Semenic, S. E., Ritchie, J. A., Richer, M.-C.,
and Denis, J.-L. (2015). The sustainability of health-
care innovations: a concept analysis. Journal of ad-
vanced nursing, 71(7):1484–1498.
Fuchs, J., Busch, M., Lange, C., and Scheidt-Nave,
C. (2012). Prevalence and patterns of morbidity
among adults in germany. Bundesgesundheitsblatt-
Gesundheitsforschung-Gesundheitsschutz,
55(4):576–586.
G
¨
overcin, M., Meyer, S., Schellenbach, M., Steinhagen-
Thiessen, E., Weiss, B., and Haesner, M. (2016).
Smartsenior@ home: Acceptance of an integrated am-
bient assisted living system. results of a clinical field
trial in 35 households. Informatics for health and so-
cial care, 41(4):430–447.
Haux, R. (2006). Individualization, globalization and
health–about sustainable information technologies
and the aim of medical informatics. International
journal of medical informatics, 75(12):795–808.
Himmel, S. and Ziefle, M. (2016). Smart home medical
technologies: users’ requirements for conditional ac-
ceptance. i-com, 15(1):39–50.
Hofstede, J., de Bie, J., Van Wijngaarden, B., and Heij-
mans, M. (2014). Knowledge, use and attitude to-
ward ehealth among patients with chronic lung dis-
eases. International journal of medical informatics,
83(12):967–974.
Jaschinski, C. (2014). Ambient assisted living: towards a
model of technology adoption and use among elderly
users. In Proceedings of the 2014 ACM International
Joint Conference on Pervasive and Ubiquitous Com-
puting: Adjunct Publication, pages 319–324. ACM.
Jenssen, B. P., Mitra, N., Shah, A., Wan, F., and Grande, D.
(2016). Using digital technology to engage and com-
municate with patients: a survey of patient attitudes.
Journal of general internal medicine, 31(1):85–92.
Kirchbuchner, F., Grosse-Puppendahl, T., Hastall, M. R.,
Distler, M., and Kuijper, A. (2015). Ambient intelli-
gence from senior citizens’ perspectives: Understand-
ing privacy concerns, technology acceptance, and ex-
pectations. In European Conference on Ambient Intel-
ligence, pages 48–59. Springer.
Little, L., Marsh, S., and Briggs, P. (2007). Trust and pri-
vacy permissions for an ambient world. In Trust in
e-services: Technologies, Practices and Challenges,
pages 259–292. IGI Global.
Loft, M. I., Martinsen, B., Esbensen, B. A., Mathiesen,
L. L., Iversen, H. K., and Poulsen, I. (2019). Call
for human contact and support: an interview study ex-
ploring patients’ experiences with inpatient stroke re-
habilitation and their perception of nurses’ and nurse
assistants’ roles and functions. Disability and rehabil-
itation, 41(4):396–404.
Marengoni, A., Angleman, S., Melis, R., Mangialasche, F.,
Karp, A., Garmen, A., Meinow, B., and Fratiglioni,
L. (2011). Aging with multimorbidity: a system-
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
36

atic review of the literature. Ageing research reviews,
10(4):430–439.
Montague, E. N., Kleiner, B. M., and Winchester III, W. W.
(2009). Empirically understanding trust in medical
technology. International Journal of Industrial Er-
gonomics, 39(4):628–634.
Nowossadeck, S. (2013). Demografischer wandel,
pflegebed
¨
urftige und der k
¨
unftige bedarf an
pflegekr
¨
aften. Bundesgesundheitsblatt - Gesundheits-
forschung - Gesundheitsschutz, 56(8):1040–1047.
Osgood, C. E., Suci, G. J., and Tannenbaum, P. H. (1957).
The measurement of meaning. Number 47. Urbana:
University of Illinois Press.
Peek, S. T., Wouters, E. J., Van Hoof, J., Luijkx, K. G.,
Boeije, H. R., and Vrijhoef, H. J. (2014). Factors in-
fluencing acceptance of technology for aging in place:
a systematic review. International journal of medical
informatics, 83(4):235–248.
Rashidi, P. and Mihailidis, A. (2012). A survey on ambient-
assisted living tools for older adults. IEEE journal of
biomedical and health informatics, 17(3):579–590.
Rogers, E. M. (1983). Diffusion of innovations. New York,
The free press.
Ryan, R. M. and Frederick, C. (1997). On energy, personal-
ity, and health: Subjective vitality as a dynamic reflec-
tion of well-being. Journal of personality, 65(3):529–
565.
Sackmann, R. and Winkler, O. (2013). Technology gener-
ations revisited: The internet generation. Gerontech-
nology, 11(4):493–503.
Sadri, F. (2011). Ambient intelligence: A survey. ACM
Computing Surveys (CSUR), 43(4):36.
Schomakers, E.-M. and Ziefle, M. (2019). Privacy percep-
tions in ambient assisted living. In Proceedings of
the 5th International Conference on Information and
Communication Technologies for Ageing Well and e-
Health (ICT4AWE 2019), pages 205–215.
Statistische
¨
Amter des Bundes und der L
¨
ander, S. A. d. B. u.
d. L. (2011). Demografischer wandel in deutschland–
bev
¨
olkerungs- und haushaltsentwicklung im bund und
in den l
¨
andern (heft 1). Wiesbaden: Statistisches Bun-
desamt.
van Heek, J., Arning, K., and Ziefle, M. (2016). The
surveillance society: Which factors form public ac-
ceptance of surveillance technologies? In Smart
Cities, Green Technologies, and Intelligent Transport
Systems, pages 170–191. Springer.
van Heek, J., Himmel, S., and Ziefle, M. (2017). Helpful but
spooky? acceptance of aal-systems contrasting user
groups with focus on disabilities and care needs. In
ICT4AgeingWell, pages 78–90.
van Heek, J., Ziefle, M., and Himmel, S. (2018). Care-
givers’ perspectives on ambient assisted living tech-
nologies in professional care contexts. In ICT4AWE,
pages 37–48.
Venkatesh, V., Morris, M. G., Davis, G. B., and Davis, F. D.
(2003). User acceptance of information technology:
Toward a unified view. MIS quarterly, pages 425–478.
Venkatesh, V., Thong, J. Y., and Xu, X. (2012). Consumer
acceptance and use of information technology: ex-
tending the unified theory of acceptance and use of
technology. MIS quarterly, 36(1):157–178.
Wilkowska, W. (2015). Acceptance of eHealth technology
in home environments: Advanced studies on user di-
versity in ambient assisted living. Apprimus Verlag.
Wilkowska, W., Offermann-van Heek, J., Brauner, P., and
Ziefle, M. (2019). Wind of change? attitudes towards
aging and use of medical technology.
Wilkowska, W. and Ziefle, M. (2012). Privacy and data se-
curity in e-health: Requirements from the user’s per-
spective. Health informatics journal, 18(3):191–201.
Wilkowska, W. and Ziefle, M. (2018). Determinants of trust
in acceptance of medical assistive technologies. In In-
ternational Conference on Information and Commu-
nication Technologies for Ageing Well and e-Health,
pages 45–65. Springer.
Wilkowska, W., Ziefle, M., and Himmel, S. (2015). Percep-
tions of personal privacy in smart home technologies:
Do user assessments vary depending on the research
method? In International Conference on Human
Aspects of Information Security, Privacy, and Trust,
pages 592–603. Springer.
Yusif, S., Soar, J., and Hafeez-Baig, A. (2016). Older peo-
ple, assistive technologies, and the barriers to adop-
tion: A systematic review. International journal of
medical informatics, 94:112–116.
Deus versus Machina: How Much Health-supporting Technology Do People Allow Depending on the Severity of the Disease?
37
