
Simulation-based Business Process Evaluation in Home Health Care
Logistics Management
Fabian Lorig
1,2 a
, Colja A. Becker
3 b
, Daniel S. Lebherz
3 c
, Stephanie C. Rodermund
3 d
and Ingo J. Timm
3 e
1
Department of Computer Science and Media Technology, Malm
¨
o University, Sweden
2
Internet of Things and People Research Center, Malm
¨
o University, Sweden
3
Center for Informatics Research and Technology, Trier University, Germany
Keywords:
Home Health Care, Agent-based Social Simulation, Multiagent Systems, Dynamic Microsimulation, Artificial
Intelligence, Automated Planning and Scheduling, Logistics.
Abstract:
Home health care (HHC) providers face an increasing demand in care services, while the labor market only
offers a limited number of professionals. To cope with this challenge from a HHC provider’s perspective,
available resources must be deployed efficiently taking into account individual human needs and desires of
employees as well as customers. On the one hand, corresponding strategic management questions arise,
e.g., distribution or relocation of establishments or expansion of the vehicle fleet. On the other hand, logistical
challenges such as the flexible and robust planning and scheduling of HHC service provision must be addressed
by operational HHC management. This paper targets both perspectives by providing an integrated simulation-
based framework for the evaluation of different business processes. Methods from Agent-based Simulation,
Dynamic Microsimulation, and (Distributed) Artificial Intelligence are combined to investigate HHC service
provision and to support practical decision-making. The presented approach aims to facilitate the reasonable
development of the HHC provider’s organization to ensure the sustainable delivery of required medical care.
1 INTRODUCTION
Many countries face challenges in coping with in-
creasing demand for care services. In Germany, for
example, the number of people in need of care will
rise by approximately 32% by 2030, resulting in a
growing shortage of care personnel (Rothgang et al.,
2016). Besides stationary facilities and the support
of relatives, home health care (HHC) is one possibil-
ity to receive essential care services. Here, caregivers
are usually equipped with cars and render the required
services at the patients’ homes.
As the availability of qualified caregivers on the
labor market is very limited, it is not feasible to hire
additional caregivers for coping with the increasing
demand in HHC. Thus, logistical optimization and
managing of existing resources in HHC gains in rele-
a
https://orcid.org/0000-0002-8209-0921
b
https://orcid.org/0000-0003-1818-2079
c
https://orcid.org/0000-0003-0956-4841
d
https://orcid.org/0000-0002-5168-3564
e
https://orcid.org/0000-0002-3369-813X
vance to enable efficient service delivery. At the same
time, individual human needs and desires of employ-
ees as well as customers have to be taken into account.
On the one hand, flexible and robust planning and
scheduling of HHC service provision is a challenging
logistical task for operational HHC management. On
the other hand, corresponding strategic management
questions arise, like the distribution or relocation of
local establishments or the expansion the company’s
vehicle fleet. Testing and analyzing different strate-
gies during daily operation can be time consuming,
expensive, and thus economically harmful. To avoid
negative consequences from such real-world investi-
gations, the use of simulation is reasonable. Further,
methods from the field of Artificial Intelligence can
be applied to extend simulation technology and to in-
crease the efficiency of operations by applying auto-
mated processes.
This paper combines these techniques and pro-
poses a simulation-based framework for the evalua-
tion and comparison of business processes in HHC
logistics. It can serve as an assistance for HHC
providers to facilitate the development of their orga-
226
Lorig, F., Becker, C., Lebherz, D., Rodermund, S. and Timm, I.
Simulation-based Business Process Evaluation in Home Health Care Logistics Management.
DOI: 10.5220/0009348902260235
In Proceedings of the 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2020), pages 226-235
ISBN: 978-989-758-420-6
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

nization such that medical care can be ensured in the
long term.
This paper is structured as follows: In Chapter 2,
foundations of HHC and the state of the art in model-
ing, simulating, and assisting HHC processes are pre-
sented. In Chapter 3, the conceptual architecture of
the framework is explained and its application is sub-
ject of Chapter 4. Finally, in Chapter 5, conclusions
are drawn and an outlook on future work is provided.
2 BACKGROUND
This section terminologically introduces the domain
of HHC as a combination of medical and non-medical
care that is rendered by a mobile nursing service at the
patients’ homes. Additionally, this section presents
the state of the art of two research areas that contribute
to the development of the framework, i.e., forecast of
care demand and assistance of operational HHC man-
agement.
2.1 Home Health Care
The provision of HHC services is usually part of the
public health care system. There are national dif-
ferences in HHC systems, yet, they have a common
basis. Independent of a specific public health care
system, populations can be divided by their individ-
uals’ care status, i.e., care-dependent or not care-
dependent. Care-dependent individuals are referred
to as care recipients and can be classified by different
levels of care, e.g., depending on the required time
of support. These levels may change, if the con-
dition of the care recipient changes. Additionally,
care recipients can be differentiated by their choice
of care (type of care), that determines how they are
treated. Typical choices are family care, where the
care recipient will be taken care of at home by fam-
ily or friends, nursing care, where the care recipient
moves into a nursing facility, or HHC, where em-
ployees of an ambulatory care service provider (HHC
provider) execute requested care services (service re-
quests). In this work, HHC refers to “the provision of
health care services to people of any age at home or
in other noninstitutional settings” (Dieckmann, 2015,
p. 3). To distinguish skilled medical services and
non-skilled services (such as personal care routines,
household maintenance, and social services), the non-
skilled services are described using the term home
care, in contrast to HHC, which also includes medical
treatments, nursing services, and physical therapies
(Prieto, 2008). Typically, one HHC provider employs
several caregivers with different qualifications. Care-
givers are equipped with diverse vehicles and render
the service requests in the respective patients’ homes
according to their qualifications.
2.2 Modeling and Simulation of Care
Demand
The combination of Dynamic Microsimulation (DM)
and Agent-based Social Simulation (ABSS) has been
proposed as a hybrid approach for forecasting indi-
vidual care demand (Lebherz et al., 2018). Seen indi-
vidually, DM and ABSS are well known in the field
of care demand analysis or for simulating care deci-
sions. DM allows for simulating the developments
of micro-units, e.g., persons or households, over time
(Li and O’Donoghue, 2013). Here, statistical data and
derived probabilities are used for the estimation of
each micro-unit’s potential future (Rutter et al., 2011).
Decision-making analysis originated in Operations
Research (OR). Usually, the target of OR approaches
is the optimization of decision behavior, e.g., with
multiple objectives (Azc
´
arate et al., 2008). However,
when reconstructing human decision-making, there is
no need for such optimizations. Instead, sophisticated
methods that include psychological and sociological
theories are required for a realistic reconstruction of
human decision behavior. ABSS enables the inclu-
sion of such methods and thus seems more promising
(Davidsson, 2002; Lorig et al., 2018).
Most ABSS approaches in health care pursue dif-
ferent goals and are suitable for strategic decision
support (Liu and Wu, 2016) or process optimiza-
tion (Moore et al., 2012), e.g., by simulating roles
and activities in health care systems (Mustapha and
Frayret, 2016). Yet, there are also approaches that
focus on the forecast of care demand, e.g., Ma et al.
(Ma et al., 2016). Other approaches combine exist-
ing methods in hybrid simulations, e.g., Bae et al.
(Bae et al., 2016), who combine Agent-based Model-
ing and Microsimulation for studying population dy-
namics. However, for the forecast of individual care
demand, there is no approach that combines meth-
ods for population forecasting, e.g., DM, with so-
phisticated methods for simulating individual human
decision-making, e.g., ABSS. Yet, the combination of
both methods seems promising to take individual de-
cision behavior into account when forecasting future
care demand.
2.3 Supporting Operational HHC
Management
The support of operational management ranges from
basic technologies for carrying out daily tasks to com-
Simulation-based Business Process Evaluation in Home Health Care Logistics Management
227
HHC Provider Care Recipients
Modern HHC
Provision
Prediction of
Individual
Care Demand
KPI
Validation of
Simulation
Models
Data
Empirical
Studies
Care
Statistics
Census
HHC
Provider
DEMAND
INPUT
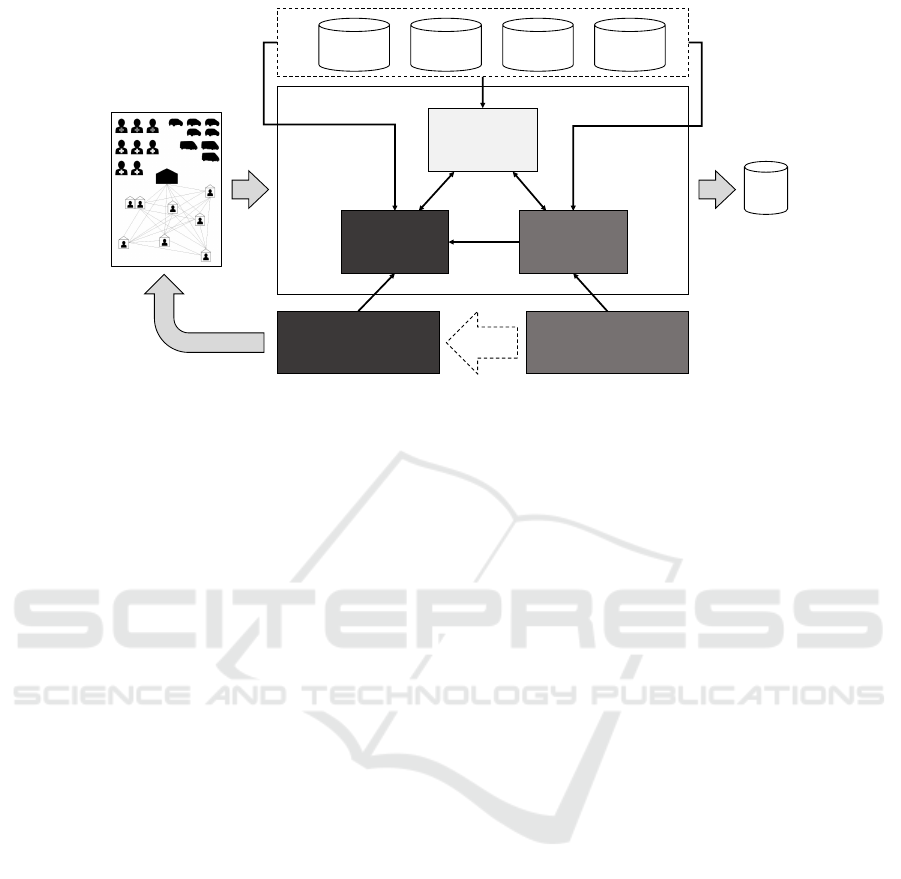
Figure 1: Conceptual Architecture of the Framework.
prehensive support for difficult decisions using so-
phisticated Decision Support Systems (DSS). Emil-
iano et al. (Emiliano et al., 2017) identified logis-
tics problems in the domain of HHC and proposed
a framework, which structures management tasks for
the development of a DSS. An especially complex
and recurring management task that is important for
cost reduction is the scheduling and routing of avail-
able resources. Suitable methods for HHC scheduling
and routing include Variable Neighborhood Search
by means of a Mixed-Integer Linear Programming
model (Mankowska et al., 2014) or the use of fuzzy
models for more uncertain scenarios (Shi et al., 2017).
A comprehensive overview on existing approaches
is provided by Fikar and Hirsch (Fikar and Hirsch,
2017).
To make such approaches usable for the opera-
tions manager, Begur et al. (Begur et al., 1997), for
instance, developed a tool to support scheduling and
routing decisions of caregivers. To facilitate capac-
ity planning, Zhang et al. (Zhang et al., 2012) de-
veloped a DSS using optimization and Discrete Event
Simulation with demographic data. Besides this, the
use of methods from the field of Artificial Intelli-
gence is an increasing trend in practical applications.
Becker et al. (Becker et al., 2019) surveyed the use
of multiagent systems and agent-based simulations to
support automated planning and scheduling in oper-
ational HHC logistics management. Discovered ap-
proaches mostly focus on the evaluation of specific
aspects of HHC logistics management systems, yet,
the study revealed shortcomings in end user provi-
sion, evaluation of developed concepts, and in deal-
ing with a shortage of qualified workers. Comprehen-
sive approaches that include both demand and supply
modeling were not identified.
3 EVALUATION FRAMEWORK
FOR HHC BUSINESS
PROCESSES
The framework proposed in this paper conceptualizes
and enables the evaluation of different business pro-
cesses in HHC logistics by means of simulation. It
allows for the long-term evaluation of strategies for
potential future scenarios while taking the possible
influences of the customers into account. The frame-
work consists of two components: a simulation that
predicts the care demand of individuals and an ap-
proach for the planning and provision of HHC ser-
vices. This section presents a conceptual architecture
in which all required components as well as their in-
teractions are introduced. Moreover, it outlines how
the simulation-based prediction of individual care de-
mand and the approach for modern HHC provision
facilitate the evaluation of business processes of HHC
providers.
3.1 Conceptual Architecture of the
Framework
To evaluate whether or not a specific business pro-
cess for the delivery of HHC services is economically
viable and satisfactory for care recipients and care-
givers, its present and future suitability must be sys-
tematically assessed under a variety of potential cir-
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
228
Census
Care
Statistics
Empirical
Studies
Artificial
Population
Forecast of
population
development
Individual
Care
Decision
Individual Care-Dependency
Order
Data
Individual
Care
Demand
Statistics on
provided
care services
Probabilities
of demand
for specific
care services
HHC
Provider
Data
Forecast of
required
care services
Demand for Specific Care Services
Dynamic
Microsimulation
Agent-Based
Social Simulation
Quantitative
Forecasting
Methods
Probability
Distribution
Fitting
Commissioning
of Care Services
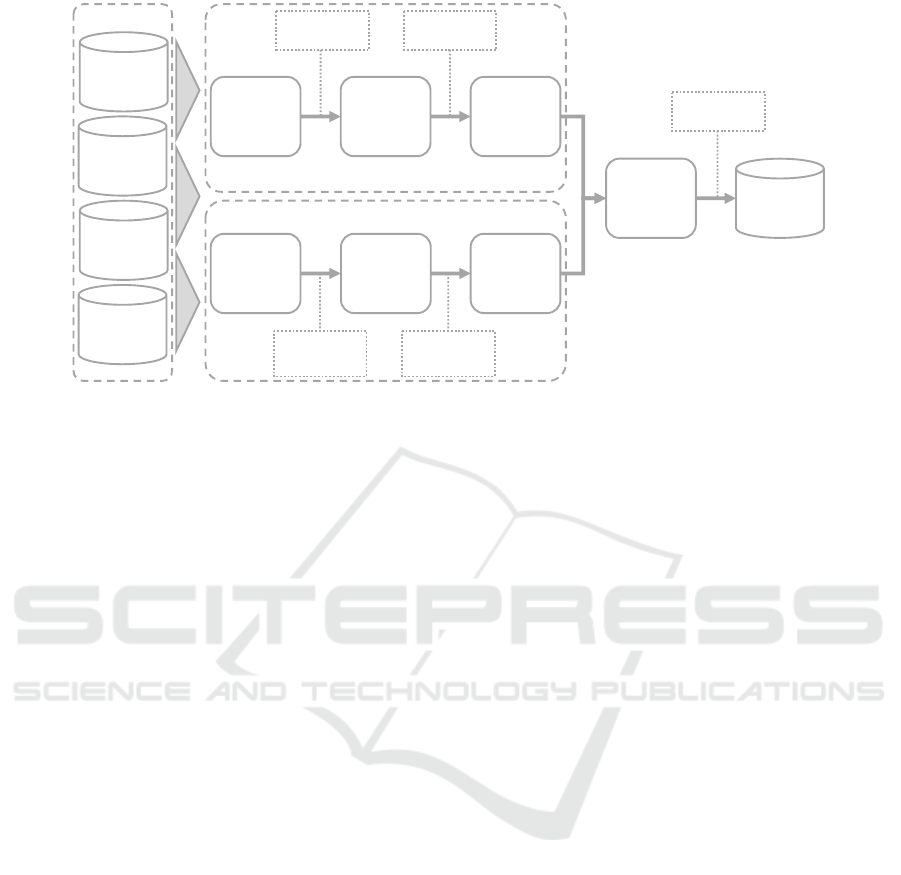
Figure 2: Forecasting Individual Care Demand.
cumstances. To achieve this, the presented framework
(cf. Figure 1) models real-world care recipients, their
demand for care services, and HHC providers that ful-
fill such services. This enables the simulation-based
evaluation of care provision approaches and serves as
an assistance system for HHC providers.
To allow for the investigation and comparison of
different business processes that serve as input of
the proposed framework, their performance must be
quantified. For this purpose, the framework returns
KPIs, e.g., adherence to schedules or the ratio be-
tween travel and service provision times. By this
means, a more profound decision-making basis is cre-
ated for the management. Yet, more advanced KPIs
such as customer satisfaction must be gathered and
evaluated after implementing the business process in
the real-world system.
Business processes of HHC providers may be dis-
criminated into three hierarchical layers depending on
the goal they pursue and how they define and struc-
ture the process. On the highest level, the strategic
layer defines business process based on future de-
velopments. Such strategic decisions might include
investment decisions such as the recruitment of new
staff. The practical implementation of such strategies
is achieved by the tactical layer. Here, the achieve-
ment of the business goal is addressed by algorithms
that, e.g., solve problems of staff allocation. Finally,
the lowest layer can be defined as operational layer
where the business process specifies the short-term
operational control. Such processes, for example, de-
fine weekly schedules that assign each caregiver to
render specific services for multiple care recipients.
The hierarchical order of these layers also repre-
sents the stepwise implementation and evaluation of
business processes. Management decisions take place
of the strategic layer. Here, the structured and thor-
ough investigation of such processes might for in-
stance require the top-down application of different
scheduling algorithms as well as the simulation-based
analysis of multiple schedules by the framework.
The presented framework pursues an approach
where the individual care demand of a specific pop-
ulation is predicted by DM and ABSS. Based on this
demand, specific order data is generated that serves as
input for the provision of the requested services. The
fulfillment of the services is then simulated and dif-
ferent KPIs are gathered. As both components require
real-world data, sociodemographic and empirical data
sources are integrated by the framework, e.g., cen-
sus data and operational data from the care provider.
To ensure the generation of reproducible and credible
simulation results, a data-based validation of the sim-
ulation models is also an inherent part of the proposed
framework.
3.2 Prediction of Individual Care
Demand
The prediction of individual care demand, as imple-
mented by the framework, includes the determination
of recent care demand as well as the realistic predic-
tion of future care demand for reliable and sustain-
able planning (cf. Figure 2). This includes the fore-
cast of the number of care-dependent individuals as
well as information about their location and the re-
quested type of care. In previous work, Agent-Based
Microsimulation (ABMS) has been proposed for pre-
dicting future care demand (Lebherz et al., 2018).
Simulation-based Business Process Evaluation in Home Health Care Logistics Management
229

This approach can be used to generate synthetic in-
formation on the amount of HHC-demanding peo-
ple and potential service requests (order data) and al-
lows for the transformation of individual care demand
into specific service requests for HHC providers. For
the prediction of care demand, two perspectives need
to be considered: The forecast of individual care-
dependency, i.e., the prediction of the amount and lo-
cation of all HHC-demanding people in the investi-
gated area, and forecasts of the demand for specific
care services, i.e., the prediction of potentially re-
quested services. The combination of both perspec-
tives allows for the determination of the individual
care demand.
Forecasting Individual Care-dependency. This per-
spective allows for determining the number of care
recipients that choose HHC services for their care
support at an arbitrary (future) point in time. Here,
ABMS generates location, level of care, and further
information about the care recipient’s family situa-
tion. ABMS is an iterative approach and consists
of three steps. The first step is the generation of
an artificial population. Sociodemographic and care
statistic data are used to generate an artificial popu-
lation that matches all required structural characteris-
tics of the real population, e.g., age structure. Further-
more, the combination of map data, census data, and
geo-referencing approaches allows for the allocation
of the artificial population to real-world households
(Lebherz et al., 2018). In the second step, DM is used
to predict the stepwise development of this popula-
tion into the future (Li and O’Donoghue, 2013). This
allows for the investigation of the demographic de-
velopment as well as of each individuals’ care status,
level of care, and family situation. In the third step,
ABSS is used to simulate individual care decisions
and the preferred type of care for every care depen-
dent person. A simulative decision-making process
based on objective and subjective criteria is used for
analyzing care decisions. Influences that potentially
affect this decision are implemented as different func-
tions, e.g., saving of cost or social steadiness, which
are objectively interpreted depending on each individ-
uals’ situation. By this means, data about the individ-
ual care level or living situation can be integrated into
the decision-making process. Finally, an individual
subjective assessment of these results allows for de-
riving unique decisions based on the individual per-
son’s characteristics (Lebherz et al., 2018). After a
determined number of iterations, the output is a set
containing information on every care recipient, its de-
mographic characteristics, and its choice of care. For
the application in the presented framework only those
recipients choosing HHC are considered.
Forecasting the Demand for Specific Care Ser-
vices. The second perspective pursues two different
goals. The first one is a realistic assessment of spe-
cific services that are offered by HHC providers based
on the care recipient’s level of care. To this end, data
of service providers is required about the types of ser-
vices that are requested by care recipients depending
on their level of care. In a following step, quantitative
forecasting methods are used for the prediction of fu-
ture service requests. Based on this forecast, methods
for probability distribution fitting can be used to cal-
culate probabilities of the demand for every specific
care service (n) combined with every possible level
of care (m). Hence, the first result is a n × m matrix
consisting of probabilities for requesting a service.
The second goal is to determine which services
are usually provided by family members or friends
based on the assumption that even if a care recipi-
ent chooses HHC, some tasks are performed by fam-
ily members or friends. Such information must be
gathered through empirical studies, e.g., interviews.
Hence, as a second result of this perspective, prob-
abilities about the professional and non-professional
provision of services must be collected. In summary,
this perspective provides two different results, which
can be combined as probability matrices.
Forecasting Individual Care Demand and Order
Data. The set of HHC recipients combined with
the calculated probability matrices enables the fore-
cast of individual care demands. A random process
is used to assign possible services to the recipients
based on the provided probabilities. The probabilities
regarding the professional or non-professional provi-
sion of services are used in a second random process,
which transforms the demand forecast into realistic
order data for potential HHC providers. Here, ran-
domly chosen services are requested from the service
provider. Final order data consists of a list of HHC re-
cipients with all data provided by ABMS and two in-
dividual sets of services: HHC provider requests and
services provided by family or friends.
3.3 Modern Home Health Care
Logistics Management
Some management tasks in HHC are highly com-
plex or require great coordination effort. The idea of
modern HHC logistics management is to reduce the
range of such tasks by means of innovative informa-
tion systems, to create more space for social-related
tasks concerning customers and employees, like sen-
sitive human-to-human interaction in leading a team.
The vision comprises an Intelligent Assistance Sys-
tem for decision support and a Multiagent Control
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
230
Wirtschaftsinformatik I
(Prof. Dr. Timm)
- 1 -
Universität Trier
The Vision: Modern Home Health Care Logistics Management
Model
Simulation-based
Intelligent
Assistance System
Multiagent Control
System
Forecast of
Order Data
HHC
Provider
Input Data
Operations
Manager
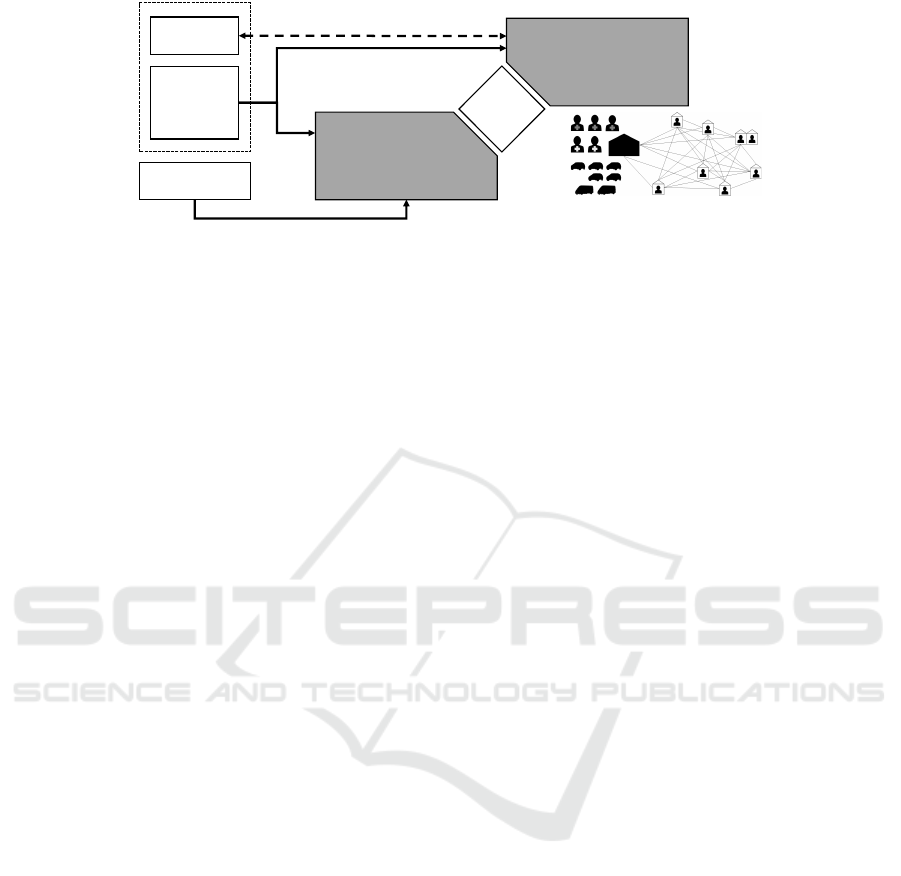
Figure 3: Modern HHC Logistics Management.
System for managing employees’ operational activi-
ties during execution. Both parts can be understood
as a mutual complement in practice (cf. Figure 3).
First, the intelligent assistance system is applied for
defining and planning the execution of HHC services.
Afterwards, the multiagent system is used to control
the execution of the planned activities and to adapt the
execution if necessary.
Intelligent Assistance System. The system focuses
on adapting the current way of providing HHC ser-
vices to increase efficiency. It can be described as a
comprehensive model-driven DSS with an Intelligent
User Interface. According to Power (Power, 2008),
a model-driven DSS has access to a financial, opti-
mization, or simulation model, is able to manipulate
this model, and to analyze the new situation to sup-
port decision makers. The system presented in this
work is based on an agent-based simulation and pro-
vides support by the means of automated simulation
studies. The suggested simulation model consists of
care recipients in their homes and caregivers perform-
ing HHC services using vehicles in an abstract envi-
ronment. To describe individual entities, the model
is capable of representing individual behavior of em-
ployees and customers.
Through manipulation of the modeled (artificial)
world, different scenarios can be evaluated and the
gained knowledge can be applied to improve real-
world processes. Examined scenarios include differ-
ent possibilities for performing services and the con-
sideration of potential future circumstances, which
are realized by using forecast order data. To manage
data and to control the DSS, an intelligent user inter-
face is applied. Here, the model’s input data and the
higher-level system are administered by a software
agent, which is able to communicate with the oper-
ations manager (user) via different channels. Since
not all employees are familiar with information tech-
nology, this interface is to be understood as an intu-
itive connection to a virtual employee. Accordingly,
the core computational application of the intelligent
assistance system is controlled and conducted by the
software agent. It comprises the design and con-
ducting of simulation experiments as well as output
data analysis as defined in Hypothesis-Driven Simu-
lation Studies (Lorig et al., 2017). Based on the fore-
casted order data and the available resources as input
data, multiple simulation experiments are systemati-
cally designed and executed to identify the most ef-
ficient provision of HHC services. To this end, the
simulation model is modified accordingly and sev-
eral alternatives of service provision are evaluated.
For instance, specific combinations of skilled and
non-skilled workers that form a set of teams can be
tested in the artificial world and KPIs can be measured
to assess their suitability. Furthermore, correspond-
ing planning data for order fulfillment and routing is
generated, aggregated, and structured in a schedule,
which can be treated as a separate output of the sys-
tem. Besides the generation of daily schedules, real-
world processes can benefit from using insights from
simulation output data analysis to adapt schedule pat-
terns or adjust involved long-term resources. The lat-
ter, for instance, can be realized by hiring profession-
als with specific skills according to the analysis re-
sults.
Multiagent Control System. To link the described
model with the real world, the multiagent control sys-
tem uses the model to create a cyber-physical rela-
tion: real-world entities (like employees) are repre-
sented by virtual surrogates in the simulation model
and communication is directed in both ways. Similar
to the application of the model by the intelligent as-
sistance system, the control system creates a virtual
world in a non-terminating simulation run represent-
ing the real world. Defined properties (like geograph-
ical location) of the modeled entities are continuously
synchronized with the values of the real world. Based
on the current simulation state, unavoidable devia-
tions from the schedule can be handled by comput-
ing several opportunities in parallel simulation runs.
These start from the current simulation state, and by
selecting the best alternative to change the current
schedule for the remaining tasks. Because of infor-
Simulation-based Business Process Evaluation in Home Health Care Logistics Management
231

mation exchange and coordination on the virtual level
between the representatives, the respective real-world
participants can reduce communication efforts and are
provided with necessary data and instructions. While
the operations manager is the user of the intelligent
assistance system in the first step, he or she is now
part of the multiagent control system itself and repre-
sented by a virtual surrogate, which initiates coordi-
nation tasks like auctions and votes.
This also enables, for instance, the real-time pro-
cessing of urgent customer service requests, which re-
quire the coordination of the consultation with care-
givers. Moreover, customers with an affinity for tech-
nology can be connected to the system by using per-
sonal devices, which eases the sending of such re-
quests. Wearable technologies on the customer side
allow for emergency requests, which can be han-
dled automatically by the multiagent control system.
Changing preferences of the employees (caregivers)
can also trigger coordination processes in a similar
way. In summary, the multiagent control system of-
fers two main functions regarding disturbances of the
previously planned execution of HHC services: On
the one hand, the current real-world status is trans-
ferred to the simulation and can be used for (short-
term) experiments to compute a well-suited solution
to change the current schedule. On the other hand,
coordination and communication between the real-
world participants is carried out by virtual representa-
tives and reduces time and effort among the employ-
ees of the HHC provider.
4 APPLICATION AND
VALIDATION OF THE
FRAMEWORK
To demonstrate the feasibility of the proposed frame-
work, its application is presented in this section. This
includes the identification and acquisition of a data
basis, the application of the introduced models for
care demand and decision support, as well as the pre-
sentation of a frame for validating the models.
4.1 Data Basis
Data required for the model application and validation
comes from four sources. Census data represents so-
ciodemographic data and contains information, e.g.,
about financial aspects or residential situations. Care
statistics of the respective regions include information
on, e.g., the number of care recipients and their level
of care. To produce reliable results, we use empiri-
cal studies to generate and validate the model behav-
ior. A first study is concerned with care recipients
and contains information about different motives to
choose a specific type of care as well as subjectively
perceived individual conditions. A second study fo-
cuses on care recipients that make use of HHC and
the services they request. HHC provider data con-
tains information such as average duration of differ-
ent services, travel times, and demand for various ser-
vices depending on the level of care. Since the created
population is projected into the future, collected data
must be updated using validated statistical methods
and trend analyses.
4.2 Application of the Care Demand
Model
The care demand model starts with the generation of
an artificial population. For this purpose, all available
data (e.g., census, land register, or map data) is used to
create a population that matches the real-world popu-
lation on all required characteristics (e.g., care status
and level of care). The iterative ABMS process is ini-
tialized with this population. First, DM projects the
population one year into the future. During this step,
the care level of individuals might change so it is nec-
essary to adapt their type of care. ABSS is then used
to simulate a new care decision for each individual.
First, the given situational context is evaluated and
all objective decisive factors (e.g., monetary or so-
cial criteria) are determined with rating functions for
each potential decision. Following this, an assessment
is performed to derive a reasonable decision depend-
ing on each care recipients objective situation accord-
ing to census data. Income or family members liv-
ing in the same household can influence the decision.
Here, the same objective situation leads to the same
decision. Hereafter, a subjective assessment is made
based on the care recipient’s individual constitution.
Every care recipient is characterized by an individual
configuration of four motives, represented by social
actor types, i.e., homo economicus, homo sociologi-
cus, identity keeper, emotional man. This allows for
different preferences and interests in decisive factors
(Lorig et al., 2018). For instance, homo economicus
tries to save money and to reduce efforts, while homo
sociologicus lays emphasize on a steady social envi-
ronment and cares less about money.
At the end of this phase, an individual assessment
is made that interprets the objective assessment based
on the recipient’s individual constitution and gener-
ates an updated population. After a predefined num-
ber of iterations, a subset consisting of all care recip-
ients that have HHC as type of care is used for fur-
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
232

ther process. Now, every person of this set is assessed
regarding different HHC services, based on a random
process and explored probabilities. A subsequent sec-
ond random process is used for choosing a subset of
these services that will be requested at a professional
HHC provider. Finally, each person of the artificial
population who choses HHC demands a set of ser-
vices as a set of order data.
4.3 Application of the HHC Model
The order data determines which customer requests
which service during which time interval. The HHC
provider has the option to read in a duty roster for the
considered period of time, so further planning algo-
rithms can use information of employees’ availability.
Both serve as input data for the intelligent assistance
system. Furthermore, overtime hours of employees,
customer geolocation data, and type and quantity of
available vehicles are also required. Before using a
state of the art algorithm for temporal planning, the
system retrieves current or predicted traffic data. As a
first step, the algorithm creates a schedule and related
routing data on the basis of the input data. After that,
a simulation run is executed for evaluation using the
agent-based simulation model.
Depending on the HHC provider’s questions, the
design of experiments is conducted which includes
planning of further simulation runs to answer what-if
questions. In addition, experiments can be conducted
to find efficient solutions of service delivery. For ex-
ample, an HHC provider wants to examine the impact
of buying an additional vehicle. Another example is
that the operational manager wants to know if cur-
rent processes of service provision are able to cope
with an increasing demand in 5 years, and if not what
are possible adaptions to handle the situation. Finally,
methods of output data analysis are applied to provide
knowledge on a significant level. Key performance
indicators can be defined and measured data is aggre-
gated accordingly. If the simulation model represents
the real world with sufficient accuracy, conclusions
for real processes can be drawn.
4.4 Empirical Validation of the Models
Finally, the validity of the simulation framework must
be ensured. Since the models are developed and eval-
uated independently of each other, verification and
internal validation are not considered here. To en-
sure credible results, the validity of the models and
some respective results have to be determined. There-
fore, this paper examines the individual components
of the framework, i.e., the decision-making model and
the HHC model, and investigate them for validity us-
ing empirical data. The used data basis consists of
the conducted empirical studies and HHC data as de-
scribed in Section 4.1.
The validity of models can be ensured in vari-
ous ways. For example, face validation is a method
in which experts evaluate the model (Sargent, 2013).
They determine whether the assumptions made dur-
ing concept development are correct and whether the
model is suitable for solving the problem. Further-
more, the model output is checked for appropriateness
for the application area. These methods are subjec-
tive, since the assessment of the model depends on an
expert and his domain knowledge. Objective valida-
tion includes, for example, sensitivity analysis, which
tests the effects of changes in the values of the input
variables on the model output. The framework valida-
tion presented here focuses on comparing the model
output with data of the real world in order to approx-
imate the model output to it and validate the model
(empirical or historical validation). The system out-
put is compared with the test data to determine dif-
ferences, e.g. using statistical methods. This type of
validation is independent of experts or assessments by
third parties and therefore objective (Sargent, 2013).
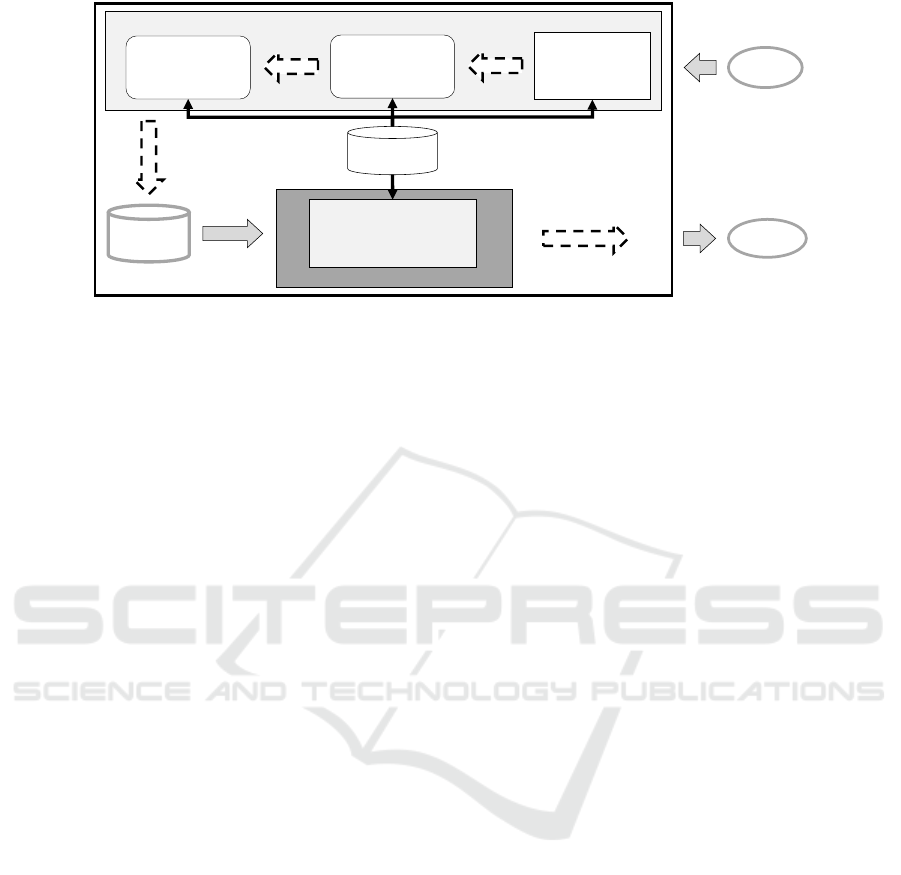
The arrows from the empirical data basis in Fig-
ure 4 point to the components of the framework to
be validated. First, the decision-making model and
the results that require empirical validation are exam-
ined. Therefore, Section 4.1 presents two empirical
studies. The generation of the initial population and
its projection one year into the future are based on
valid inputs (e.g., census data) and models (cf. Sec-
tion 3.2). Therefore, the decision-making model is the
first starting point of an empirical validation. A de-
cision is made using objective and subjective factors
of the agents regarding the type of care. Objective
factors are derived from census data. The subjective
factors are compared with empirical data, so that the
effect of motivations defined in the model can be vali-
dated against reality through target-oriented question-
ing. Furthermore, the waiting functions, whose valid-
ity cannot be guaranteed by statistical methods alone,
have to be validated against empirical data. This con-
cerns functions that work upon subjective perceptions
of care recipients, such as social pressure based on the
experience of the individual. The resulting updated
population can be validated by comparison with esti-
mation models of health statistics.
The next step of the model that has to be valid is
the mapping of services to the agents on the list of
HHC recipients. Here, the second empirical study,
which contains information about services requested
by care recipients, is used. The same applies to the
Simulation-based Business Process Evaluation in Home Health Care Logistics Management
233
Prediction of Individual Care Demand
List of agents with
care level and care
decision
Decision-Making
Model
Input
Output
Empirical Data
Basis
Order Data
HHC Model
List of agents with
home care
Modern HHC Provision
Figure 4: Empirical Validation of the Framework.
next step in the framework which reduces the list of
services which are not rendered by family members
but requested at HHC providers. For these two lists,
both their generation and validation are based on the
same data of the empirical study. This means that
the data is divided into a training set for generation
and a test set for validation. The final output of the
model is the order data, which is transferred to the
HHC simulation model. Here, the model itself has
to be validated, in order to produce a reliable output.
Therefore, internal documentation data of the HHC
provider is used. Caregivers use hand-sized devices
to enable electronic documentation while executing
daily tasks. The corresponding data is stored in the
HHC providers’ database. In addition to this, the cor-
responding order data, and the used schedule serve as
model input in order to compare the model output and
the real world documentation data. According to this,
the corresponding time recording is defined as mea-
suring points in the simulation run. If the artificial
output data matches the gathered real data, the model
is considered to be sufficiently valid.
5 CONCLUSIONS AND
OUTLOOK
In this paper, we introduced a framework that allows
HHC agencies to systematically analyze and optimize
business processes with respect to current and future
care demand. To this end, methods from the fields of
Agent-based Simulation, Dynamic Microsimulation,
and (Distributed) Artificial Intelligence were com-
bined. Questions ranging from strategic to opera-
tional logistics management were addressed and the
approach’s results can help to increase the efficiency
of HHC business processes while at the same time
taking human needs into account.
In future work, we will extend the modeling and
simulation of service provision to IoT-, robotics-, and
qualification-based innovations to allow for preinvest-
ment analysis. In long term research, we are working
on combining micro- and agent-based simulation for
validated care demand prognosis. Also, we will fur-
ther elaborate on aspects of AI planning for the practi-
cal application in a multiagent setting as well as on re-
fining knowledge generation and processing. This in-
cludes the development of a system for the automated
design and conducting of simulation experiments of
HHC scenarios.
REFERENCES
Azc
´
arate, C., Mallor, F., and Gafaro, A. (2008). Multiob-
jective Optimization in Health Care Management. Al-
gorithmic Operations Research, 3(2).
Bae, J. W., Paik, E., Kim, K., Singh, K., and Sajjad, M.
(2016). Combining microsimulation and agent-based
model for micro-level population dynamics. Procedia
Computer Science, 80:507–517.
Becker, C. A., Lorig, F., and Timm, I. J. (2019). Multiagent
systems to support planning and scheduling in home
health care management: A literature review. In Arti-
ficial Intelligence in Health, pages 13–28. Springer.
Begur, S. V., Miller, D. M., and Weaver, J. R. (1997). An in-
tegrated spatial dss for scheduling and routing home-
health-care nurses. Interfaces, 27(4):35–48.
Davidsson, P. (2002). Agent based social simulation: A
computer science view. Journal of artificial societies
and social simulation, 5(1).
Dieckmann, J. L. (2015). Home health care: A historical
perspective and overview. Handbook of home health
care administration, pages 9–26.
Emiliano, W., Telhada, J., and do Sameiro Carvalho, M.
(2017). Home health care logistics planning: a review
and framework. Procedia Manufacturing, 13:948–
955.
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
234

Fikar, C. and Hirsch, P. (2017). Home health care routing
and scheduling: A review. Computers & Operations
Research, 77:86–95.
Lebherz, D. S., Lorig, F., and Timm, I. J. (2018). Agent-
based modeling and simulation of individual elderly
care decision-making. In 2018 Winter Simulation
Conference, pages 1025–1036. IEEE.
Li, J. and O’Donoghue, C. (2013). A survey of dy-
namic microsimulation models: uses, model structure
and methodology. Int. Journal of Microsimulation,
6(2):3–55.
Liu, P. and Wu, S. (2016). An agent-based simulation model
to study accountable care organizations. Health care
management science, 19(1):89–101.
Lorig, F., Lebherz, D. S., Berndt, J. O., and Timm, I. J.
(2017). Hypothesis-Driven Experiment Design in
Computer Simulation Studies. In 2017 Winter Simu-
lation Conference, pages 1360–1371, Las Vegas, NV.
IEEE.
Lorig, F., Rodermund, S. C., Berndt, J. O., and Timm,
I. J. (2018). Modeling and Simulation of Complex
Agents for Analyzing Communication Behavior in
Social Media. International Journal On Advances in
Internet Technology, 10(1&2):57–69.
Ma, Y., Shen, Z., and Nguyen, D. T. (2016). Agent-based
simulation to inform planning strategies for welfare
facilities for the elderly. JASSS, 19(4).
Mankowska, D. S., Meisel, F., and Bierwirth, C. (2014).
The home health care routing and scheduling problem
with interdependent services. Health care manage-
ment science, 17(1):15–30.
Moore, D., McCabe, G., and Craig, B. (2012). Introduction
to the practice of statistics.
Mustapha, K. and Frayret, J.-M. (2016). Agent-based mod-
eling and simulation software architecture for health
care. In 2016 6th International Conference on Simula-
tion and Modeling Methodologies, Technologies and
Applications (SIMULTECH), pages 1–12. IEEE.
Power, D. J. (2008). Decision support systems: a historical
overview. In Handbook on decision support systems
1, pages 121–140. Springer.
Prieto, E. (2008). Home health care provider: a guide to
essential skills. Springer.
Rothgang, H., Kalwitzki, T., Unger, R., and Ams-
beck, H. (2016). Pflege in Deutschland im Jahr
2030 - regionale Verteilung und Herausforderungen
LebensWerte Kommune. G
¨
utersloh: Bertelsmann
Stiftung.
Rutter, C. M., Zaslavsky, A. M., and Feuer, E. J. (2011). Dy-
namic microsimulation models for health outcomes: a
review. Medical Decision Making, 31(1):10–18.
Sargent, R. G. (2013). Verification and validation of simu-
lation models. Journal of simulation, 7(1):12–24.
Shi, Y., Boudouh, T., and Grunder, O. (2017). A fuzzy
chance-constraint programming model for a home
health care routing problem with fuzzy demand. In
International Conference on Operations Research
and Enterprise Systems, volume 2, pages 369–376.
SCITEPRESS.
Zhang, Y., Puterman, M. L., Nelson, M., and Atkins, D.
(2012). A simulation optimization approach to long-
term care capacity planning. Operations research,
60(2):249–261.
Simulation-based Business Process Evaluation in Home Health Care Logistics Management
235
