
Motivating Older Adults to Exercise at Home: Suitability of a
Humanoid Robot
Esther Ruf, Stephanie Lehmann
a
and Sabina Misoch
Institute for Ageing Research, FHS St. Gallen University of Applied Sciences, Rosenbergstrasse 59,
9001 St. Gallen, Switzerland
Keywords: Robot, Older Adults, Physical Activity, Exercise, Training.
Abstract: Regular physical activity is a central protective factor for health. The promotion of physical activity is an
important issue, especially for ageing societies, to achieve benefits of health and independence in old age.
However, motivation for physical activity decreases with age. Due to staff shortages and high cost of personal
exercise trainers, older adults living at home cannot be permanently motivated and instructed by health
personnel to engage in physical activity. Several studies investigated the use of a humanoid robot as an
exercise coach for older adults in nursing homes and laboratories, promising great potential. This explorative
user study investigated whether a robot is a practical solution for older adults living in their own home and
can motivate for regular physical activity in everyday life. Seven older adults participated in the study. In the
study period of 12-14 weeks, they completed three different training conditions (instructions by a robot, a
video instruction, and written instructions). Results showed that participants accepted and appreciated the
robot, but most participants would not recommend the robot, mainly because several technical and other
problems occurred. The present study showed that this humanoid robot is not suitable for autonomous exercise
training for older adults at home.
1 INTRODUCTION
Due to demographic change, the proportion of older
adults is rising in all industrialized nations (Vaupel,
2000). Health promotion and prevention are central
issues for our society, especially for the older
population, in order to be able to counteract the future
increase in health costs due to illness and care costs.
One of the most important fields of action is the
promotion of physical activity in old age (Weber et
al., 2016). Regular physical activity is regarded as a
central protective factor for health and is the measure
that shows the most stable evidence of benefits in
terms of health and independence in old age (Büla et
al., 2014). However, physical activity is age-
dependent and motivation for physical activity
decreases with age (Scholes and Mindell, 2012).
Therfore, many older adults don’t move enough
(Krug et al., 2013; Weber et al., 2016). The decrease
in physical activity with increasing age (Bornschlegl,
Fischer and Petermann, 2016) inevitably leads to a
reduction in (functional) everyday abilities
a
https://orcid.org/0000-0002-1086-3075
(Voelcker-Rehage, Godde and Staudinger, 2006), to
losses in health, self-confidence, self-efficacy,
participation in social life, cognitive abilities and to
loneliness (e.g. Bornschlegl et al., 2016; Füzéki and
Banzer, 2017; Gunzelmann, Brähler, Hessel and
Brähler, 1999). There are many studies that show that
targeted physical training can reduce frailty (e.g.
Löllgen and Leyk, 2012) and thus increase quality of
life and independence (e.g. Dorner and Schindler,
2017). Furthermore, regular physical activity reduces
the occurrence of falls (Müller, Lautenschläger and
Voigt-Radloff, 2016; Sherrington et al., 2016) and
has positive effects on other physical complaints
(Gadde, Kharrazi, Patel and MacDorman, 2011).
Therefore, there is a high need for healthcare systems
to develop effective solutions to ensure the physical
wellbeing of older adults (Čaić, Avelino, Mahr,
Odekerken-Schröder and Bernardino, 2019).
Although information campaigns try to make
older adults aware of the benefits of physical activity,
and various exercise programs promoting physical
activity specifically for older adults exist, it cannot be
Ruf, E., Lehmann, S. and Misoch, S.
Motivating Older Adults to Exercise at Home: Suitability of a Humanoid Robot.
DOI: 10.5220/0009341001130120
In Proceedings of the 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2020), pages 113-120
ISBN: 978-989-758-420-6
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
113

guaranteed that older adults integrate physical
activity into their daily lives. For this, it is helpful for
physical activities to be prompted and guided
regularly (Lebedeva et al., 2015). Regular guided
training is more effective than unguided training
(Gschwind and Pfenninger, 2016), and exercise
programmes are beneficial only when followed
regularly and over a long period of time (Gadde et al.,
2011).
Due to staff shortages (World Health
Organization, 2015) and the high cost of personal
exercise trainers, older adults living at home cannot
permanently be motivated and instructed by health
personnel. Robot-guided training could enable older
adults to exercise without a human coach and thus
alleviate this situation and increase the motivation of
older adults to carry out movement programmes in
everyday life.
Several studies investigated the use of a robot as
an exercise coach for older adults. Besides
counteracting the future lack of healthcare staff, a
robotic fitness coach could comply with the
preferences of older adults. It has been shown that
socially assistive robots can positively influence
motivation (Torta, Oberzaucher, Werner, Cuijpers
and Juola, 2013) and that a robot can be very
motivating for seniors to perform physical activity
and might be less boring for seniors than just
performing an exercise session on their own (Werner,
Werner and Oberzaucher, 2013b). In their study,
Shen and Wu (2016) found a strong preference for a
robotic instructor for physical exercise over a human
instructor. Regarding motivation, it was shown that a
humanoid robot instructor was experienced as very
motivating and more motivating than a standard
training plan, but not more motivating than a human
trainer (Werner, Krainer, Oberzaucher and Werner,
2013a). For example, older adults of a day care centre
were able to exercise successfully with the help of a
robot (Görer, Salah and Akın, 2017). It was shown
that a humanoid robot assisting in a demonstration,
attracts onlookers and encourages them to participate
in health exercises (Matsusaka, Fujii, Okano and
Hara, 2009). Lewis, Metzler and Cook (2019)
investigated a humanoid robot in a senior living
community with older adults, caregivers and
administrative staff. They focused on technical
components as well as on affective reactions and
opinions recorded in focus groups. Fasola and
Mataric (2013) found that older adults prefer a
physically embodied robot and a robot which creates
a relation for example through praise (2012).
Inpatients in an assisted living facility adjusted their
movements to a humanoid robot used in geriatric
physiotherapy rehabilitation (López Recio, Márquez
Segura, Márquez Segura and Waern, 2013). Although
technical malfunctions can influence acceptance
parameters (Werner et al., 2013b), even incomplete
prototype systems generated very positive responses
(Gadde et al., 2011). It has been shown that
performing exercises with a humanoid robotic partner
exercising along with the participant boosted the
effort compared to performing these exercises alone
(Schneider and Kümmert, 2016).
Taken together, several studies indicate the great
potential of humanoid robots as instructors and
motivators for physical exercise for older adults.
However, the question of the use of a humanoid robot
as a fitness coach in the private households, where
older adults must perform physical exercises
independently with the robot, is still pending.
Our explorative user study investigated whether
the implementation of a robotic training coach is a
practical and motivating solution to promote regular
physical activity of older adults living at home. The
results show problems and motivating effects. This
research can help to determine ways to support
physical activity amongst older adults.
2 METHODS
2.1 Material
For this study, an exercise program was compiled
based on "Walk safely, stand safely", a program
recommended by Pro Senectute Switzerland for older
adults (www.sichergehen.ch). Three strength
exercises and three balance exercises were selected.
The six exercises were presented in three versions
based on the official video of the Swiss campaign.
Firstly, a booklet with written instructions and
pictures of the exercises, secondly, a video tutorial,
and thirdly, a programmed humanoid robot (NAO
V6, 6
th
version) acting as an autonomous exercise
coach. The duration of the exercise program
including an introduction and six exercises with
verbal instructions was 36 minutes (for details on the
selection process, programming, and pretest see
Brack, 2019).
A self-developed questionnaire was used.
Sociodemographic data collected were age, gender,
marital status, type of housing, former professional
activities, level of education, and residential area.
Health status was measured with a single item “In
general, would you say your health is… (ranging
from “excellent” to “poor”) from the Short Form
Health Survey (SF-36) (Ware, 2000). To collect the
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
114

current physical activity of the participants three self-
developed questions were asked “How often a week
do you exercise?”, “How long does such a session
usually last?”, “Do you do the activities in a group or
alone?”.
To measure self-efficacy, the “Allgemeine
Selbstwirksamkeit Kurzskala” (ASKU) (Beierlein,
Kovaleva, Kemper and Rammstedt, 2012) was used
with three items, and a five-point Likert scale from
“not true at all” to “absolutely true”. Participant’s
technical affinity was measured with two adopted
questions (Seifert and Meidert, 2018) to be
comparable within the Swiss population.
To evaluate the suitability of the robot NAO as an
exercise coach in older adults’ homes, eight questions
(see table 2) based on studies that equally evaluated a
robot as an exercise coach (Fasola and Mataric, 2011,
2012, 2013; Torta et al., 2013; Werner et al., 2013a,
2013b), were compiled using an answer format of a
five-point Likert scale from 1 “not at all” to 5 “very
much”. Because of the explorative character of the
study and the limited number of participants,
qualitative methods were used. They make it possible
to identify important issues and help understand
subjective opinions of participants more in-depth
(Misoch, 2015). A qualitative semi-structured
interview was conducted with the following questions
at the end of the study: (1) Were you able to train
regularly (3 times a week) with the robot NAO? (2)
Were there any difficulties during training? What
didn't work? (3) Was it fun to train with the robot? (4)
Was it motivating for you to train with the robot
NAO? (5) How was the operation of the robot for
you? Were there any difficulties? (6) If you look at
your own experiences, do you think the use of NAO
for older adults to activate movement is generally
possible? (7) Would you like to tell us anything else
about your experience with the robot?
2.2 Study Population
Eight older adults were enrolled in the study.
Inclusion criteria were age over 65 years, no physical
or cognitive restrictions which could impair the
movement training, living in Switzerland and
German-speaking, living in private homes. The older
adults were recruited via the network of senior
citizens of the institute.
2.3 Design and Procedure
The entire study period of this explorative user study
was June 2019 to December 2019. In this period, the
individual participants remained under study
condition for 12-14 weeks.
The study started with an individual appointment
for each participant at the study center (I): After
informed consent and a pre-survey (T0), the
participants were extensively introduced to all three
conditions, and participated in a one-time training
with the robot to get used to the handling, commands,
etc. (see figure 1). The participants were instructed
not to place the robot on a table or other elevation due
to its instability in order to avoid a fall and thus
damage to the robot. After this, the participants were
interviewed using a questionnaire and semi-
structured interview questions (T1).
Figure 1: Older adult trains with robot in the study center.
Image source: Brack, 2019.
Independently at home, each participant then
carried out a training including the three versions of
instruction (written (Condition Booklet; C
B
), video
(Condition Video; C
V
), robot (Condition Robot; C
R
))
according to a predetermined schedule. In each
condition, the participants remained one week and
had to perform the six movement exercises three
times under the respective guidance during this
period. For each condition, they fulfilled a study
protocol. Between each training week there was a
break (B) of two weeks in which the participants were
encouraged not to carry out the study exercises (see
figure 2). After training with the robot, a face-to-face
interview was conducted with the participants at
home (T2). Two weeks after finishing the last
training, a final telephone interview was conducted
with each participant (T3) (see table 1).
In order to avoid effects that could occur due to
the order of the three conditions, the sequence in
which the study participants went through the three
conditions varied. As only one robot was available for
the
study,
the
participants
did
not
all
go
through
the
conditions in parallel but staggered in time. Due to a
technical failure of the robot it was not possible to
realize the same distance between the conditions for
all participants, the repair lasting longer than three
weeks.
Motivating Older Adults to Exercise at Home: Suitability of a Humanoid Robot
115
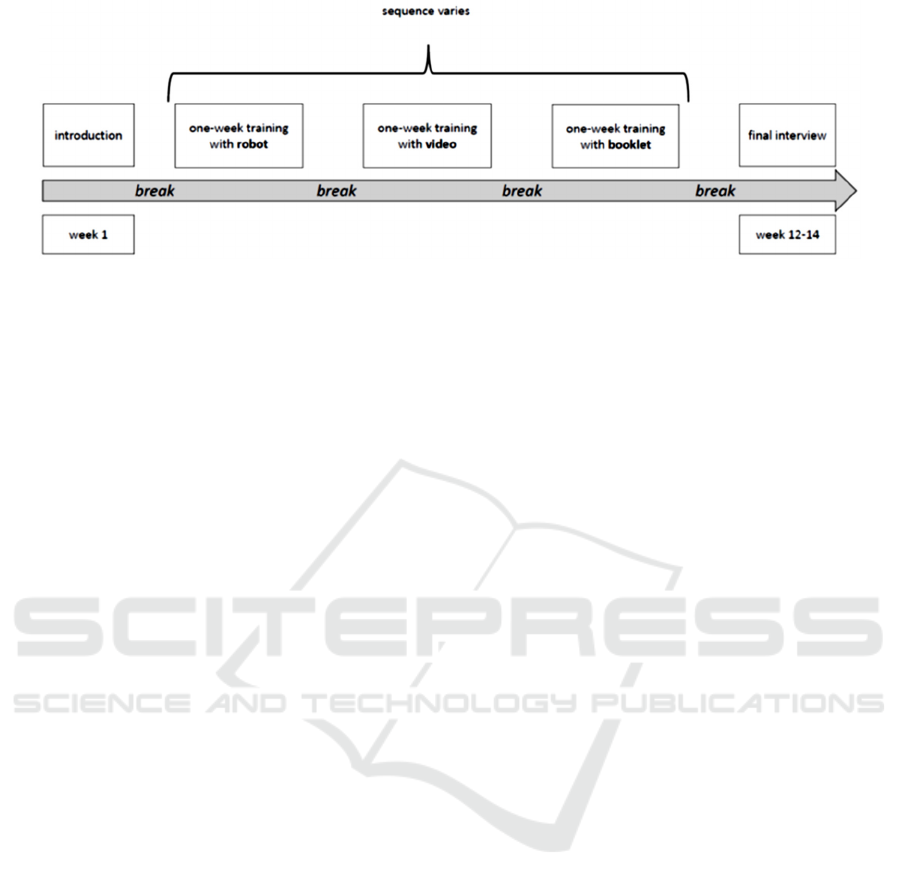
Figure 2: Course of the study conditions.
2.4 Analyses
Quantitative data from questionnaires were entered in
IBM SPSS 26. Descriptive statistics (mean, standard
deviation, frequencies) were used to characterize the
sample and evaluate frequencies of the questionnaire
answers. The Wilcoxon signed-rank test (Higgins,
2004) was used to compare motivation to train with
the robot at the introduction and after a one-week
training, as non-parametric tests do not require a
normal distribution of data and are applicable to small
sample sizes.
The statements of the participants in the semi-
structured interviews (T2, T3), were collected based
on written protocols and are summarized and
reported. Due to small sample size and the explorative
character of the study, no further qualitative content
analysis (Mayring, 2000) was worked out.
3 RESULTS
3.1 Participants
Seven older adults participated in the study (P1-P4,
P6-P8), five men and two women. One study
participant could not participate in the study due to
acute physical impairments (P5). The average age of
the participants was 74 years (SD=5.63, Range 67-
84). All participants were Swiss coming from three
different cantons. Five participants described their
current residential area as more rural, two as more
urban. One participant described his general state of
health as excellent, four as very good and two as
good. Five participants had received up to tertiary
level education and five participants lived in a
household consisting of two persons. All participants
said that they were very interested in new technical
objects, and four participants considered themselves
to be very interested, three as interested in
technology. Two participants already had contact
with a robot before at home, one at work, one
somewhere else, and three participants never had
contact with a robot before.
3.2 The Robot as a Training Coach
3.2.1 Experiences
• The participants could all perform the exercises
with the robot.
• The appearance of the robot was perceived as
pleasant.
• The joy of technology and the experience of
something interesting and new was emphasized.
3.2.2 Barriers and Difficulties
Several difficulties in using the robot were reported
by the participants:
Technical:
• It took a long time for the robot to get started.
• The participants had to wait too long to
communicate with the robot, as it takes a long
time for the robot to be operational, and the
robot didn’t react to instructions immediately.
• The older adults had to bend down towards the
robot because the robot didn’t recognize them.
• The robot didn't recognize the face of the older
adults very well and was therefore not ready to
take orders.
• The robot fell backwards while showing the
exercises with six participants.
Acoustic communication problems:
• Computer voice was not optimally
understandable.
• Sometimes the voice was perceived as
strenuous.
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
116
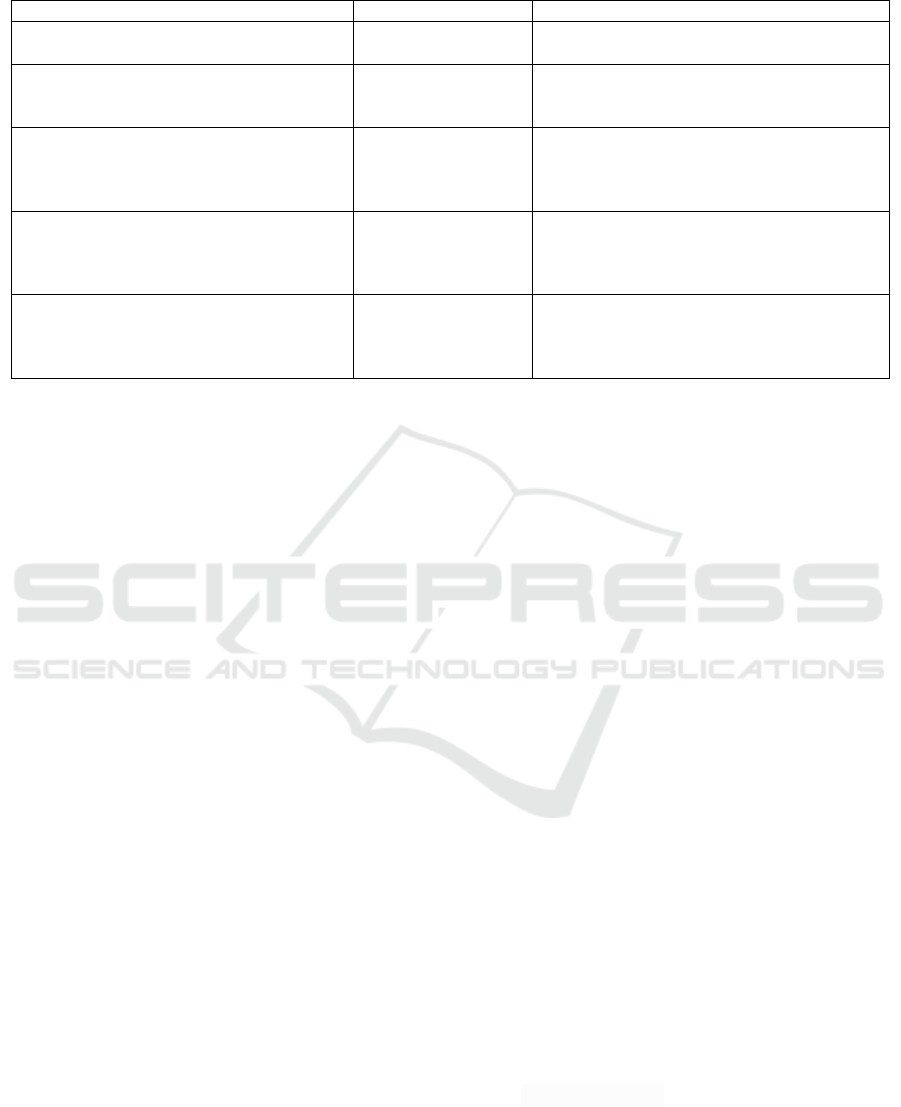
Table 1: Survey dates and instruments.
Survey date
Duration (approx.)
Instruments, data
I: Introduction at the study centre 60-90 minutes Informed consent, detailed introduction to the
three conditions (booklet, video,
robot
)
(Part of introduction) T0: face-to face
interview and questionnaire at the study
centre
be
f
or
e
introduction to the conditions
15 minutes Sociodemographic, question about physical
training, state of health, self-efficacy
(Part of introduction) T1: face-to face
interview and questionnaire at the study
centre after introduction and first training
with
the humanoid robot
15 minutes Self-developed scale robot as fitness coach
T2: face-to face interview at participant’s
home after the one-week training with the
robot
30 minutes Self-developed scale NAO as fitness coach,
semi structured interview including questions
of operation of the robot, problems during
training, motivation
T3: final interview by telephone at least two
weeks after the end of all three conditions
15 minutes Semi-structured interview: state of health,
suitability of the robot, problems, questions
about motivation, experience,
recommendations
General:
• There were too many and too long breaks in
between exercises and the older adults didn’t
know whether the robot was not working, or if
it was an intended break.
3.2.3 Motivational Ability
• The older adults found the training interesting,
exercises attractive and the robot motivating for
physical activity.
• Participants suspect that habituation effects occur
when using the robot for a longer time.
• The vocal instructions were too long and should
be individually controllable because it was boring
for the older adults when the robot always gave
the exact same instructions.
A significant influence of the one-week training
with the robot on the evaluation of the robot as an
exercise coach could not be proven using the self-
developed scale. Wilcoxon-tests show no significant
results (see table 2).
3.2.4 Recommendations of the Participants
• After the study the participants recommended the
robot to be individually adaptable and
personalizable.
• It has been mentioned that the social aspect of
activities is missing, and this is very important
especially for older adults.
• Participants wished for a robot bigger in size, so
bending down to talk to it would not be necessary.
• A memory function, and variation in the
programme and sentence structures was also
requested.
• Announcing break durations and correcting false
movements like a gym teacher were also
suggested.
• In addition, the participants wished for the
instructions of the robot to be compatible with
hearing aids of older adults and requested the
communication with the robot be easier and fully
functional.
4 DISCUSSION
The older adults who trained with the robot
considered the use of a robot at home to motivate
them to do more physical activity. However, the used
robot was judged as not suitable because of its
abilities and the strict sequence of the programmed
movement exercises. Further, the participants thought
robot instructed training could be useful for people
who are not yet physically active, but not for already
active people.
Overall, after the study, the participants would not
recommend the robot for exercise for older adults at
home as they tested it, due to the problems mentioned
above. A possible assignment for the robot was rather
seen as the accompaniment of a human coach. In their
study Čaić et al. (2019) conclude that a robotic coach
can be used to motivate seniors to be more active, but
human caregivers should make sure the elderly users
perform the exercises correctly and assist them if
necessary.
Motivating Older Adults to Exercise at Home: Suitability of a Humanoid Robot
117
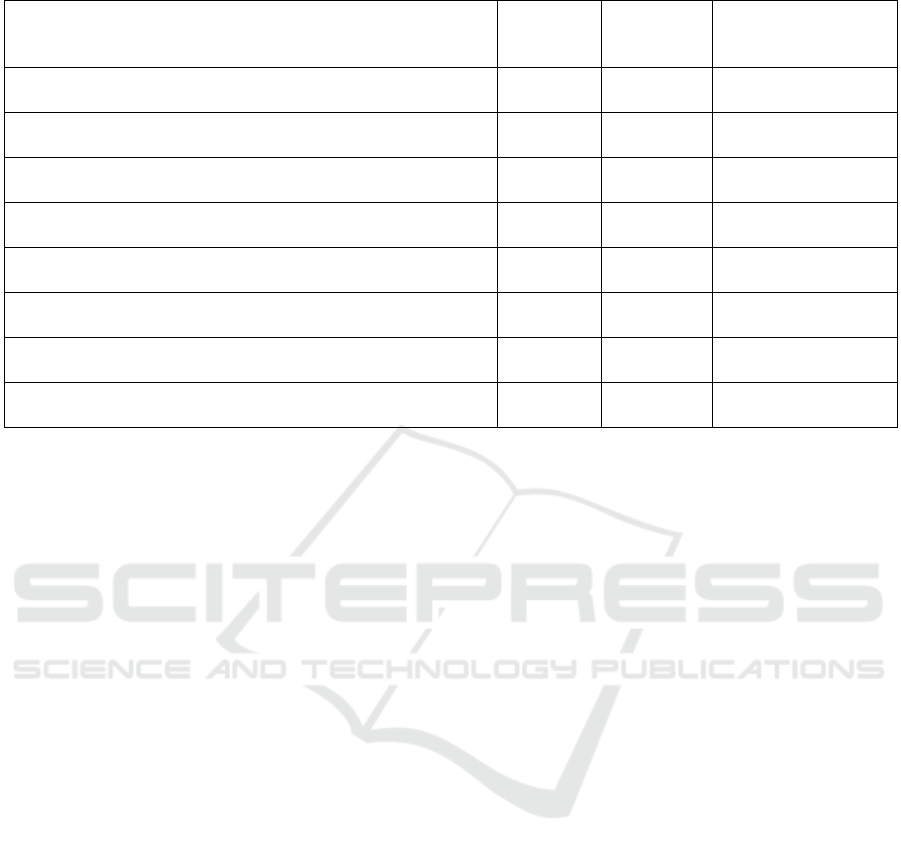
Table 2: Change in the assessment of the robot.
Question T1
M (SD)
T2
M (SD)
Wilcoxon-test, exact
significance, one-
sided
How much did you enjoy training with NAO? 4.0 (0.82) 4.43 (0.98) Z = -.828, p = .281,
n = 7
Would you recommend NAO as a training coach to your friends? 2.17 (1.60) 2.50 (1.64) Z = .000, p = .750,
n = 6
How much would you like to train with NAO in the future? 3.14 (1.46) 2.29 (1.38) Z = -1.857, p = .063,
n = 7
Do you find NAO a good training coach? 3.43 (1.40) 2.71 (1.60) Z = -1.089, p = .188,
n = 7
How well could NAO motivate you for the training? 4.00 (1.41) 4.00 (1.73) Z = -.378, p = .500,
n = 7
Do you think NAO is more motivating than a human training
coach?
1.43 (0.79) 1.29 (0.49) Z = -1.000, p = .500,
n = 7
Do you think NAO is more motivating than a training plan with
video instructions?
3.57 (1.27) 2.57 (1.40) Z = -1.382, p = .109,
n = 7
Do you think NAO is more motivating than a written training
plan?
4.71 (0.49) 3.57 (1.62) Z = -1.857, p = .063,
n = 7
The written instructions based on the booklet were
by all participants considered to be the least
motivating. The video condition was judged best.
During the one-week training, the participants
experienced the limitations of the robot (technical
problems, inflexibility, rigidity in repetitions, no
personal approach to the participants) as an obstacle
for further use. The participants would not
recommend the robot to other older adults, and if,
then with restrictions. Much would have to be
technically changed and adapted, and the question of
cost-benefit arises.
As stated in the semi-structured interviews, the
robot's motivational factor quickly diminished when
the novelty effect was exhausted. The effect that users
engage easily in interactions with new technologies,
but their interest in continuous usage decreases
rapidly after a novelty effect vanishes is widely
observed (Rosenthal-von der Pütten et al., 2014).
5 CONCLUSIONS
The programmed humanoid robot was accepted and
was appreciated by the study participants. However,
most of the participants would not recommend the
robot for use for older adults at home, and if so, only
with limitations. The pilot study showed that the
programmed robot is not suitable for autonomous
exercise training for older adults at home. These
statements given by older participants who were
highly motivated and interested in technology should
be taken very seriously.
Some limitations of the study should be noted.
The study was explorative in order to find out what
problems can occur when implementing a robot as a
motivator for training. It was not examined whether
the physical fitness of the participants changed. Due
to the high demands on the participants (12-14 weeks
in study condition, several visits at home, etc.) and the
fact that only one robot was available, only seven
participants were included in the study. The sample is
small and therefore has a limited representativeness,
especially the meaningfulness of statistical
evaluations of quantitative data gathered in this study
is restricted.
Real life testing had some challenges: due to
technical problems of the robot and personal
appointments of the participants, not all of them went
through the study in the same time, and variation of
the three conditions could not be balanced in this
group.
It should also be stated that humans, not robots,
were depicted in the booklet and the video
instructions. In addition, the robot praised the
participants at irregular intervals during the training.
The influence of this reinforcer was not examined.
Regarding the positive evaluations, it must be
considered that the participants are a highly selective
group. They were quite interested in technical
solutions and willing to participate in such a study.
Therefore, it must be assumed that it is very likely to
generate positive evaluations. These should not be
transferred to other groups or the general population.
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
118

ACKNOWLEDGEMENTS
We thank all study participants who were willing to
try out the robot at home and gave us their feedback.
Especially, we thank Zoe Brack, who programmed
the robot as part of her master thesis.
REFERENCES
Beierlein, C., Kovaleva, A., Kemper, C. and Rammstedt,
B., 2012. Ein Messinstrument zur Erfassung subjektiver
Kompetenzerwartungen: Allgemeine Selbstwirksamkeit
Kurzskala (ASKU). Mannheim: GESIS - Leibniz-
Institut für Sozialwissenschaften.
Bornschlegl, M., Fischer, R. and Petermann, F., 2016.
Erfolgreiches kognitives Altern: Zusammenhang der
kognitiven Leistungen mit Aktivität und Zufriedenheit.
Zeitschrift für Neuropsychologie, 27, 173-187.
Brack, Z. (2019). Programming and evaluating a robotic
exercise coach to promote physical activity among
elderly people. Master Thesis. ETH, Zurich.
Büla, C., Jotterand, S., Martin, B. W., Bize, R., Lenoble-
Hoskovec, C. and Seematter-Bagnoud, L., (2014.
Bewegung im Alter: Dafür ist es nie zu spät! Swiss
Medical Forum, 14, 836–841.
Čaić, M., Avelino, J., Mahr, D., Odekerken-Schröder, G.
and Bernardino, A., 2019. Robotic Versus Human
Coaches for Active Aging: An Automated Social
Presence Perspective. International Journal of Social
Robotics, 1-16. doi:10.1007/s12369-018-0507-2
Dorner, T. E. and Schindler, K., 2017. Gesundheit im Alter:
Selbständigkeit erhalten, Gebrechlichkeit vorbeugen.
Wien: MANZ'sche Verlags- und
Universitätsbuchhandlung GmbH.
Fasola, J. and Mataric, M. J., 2013. A socially assistive
robot exercise coach for the elderly. Journal of Human
Robot Interaction, 2(2), 3-32.
Fasola, J. and Mataric, M. J., 2011. Comparing physical and
virtual embodiment in a socially assistive robot exercise
coach for the elderly. Center for Robotics and
Embedded Systems.
Fasola, J. and Mataric, M. J., 2012. Using socially assistive
human–robot interaction to motivate physical exercise
for older adults. Proceedings of the IEEE, 100(8), 2512-
2526.
Füzéki, E. and Banzer, W. (2017). Bewegung und
Gesundheit im Alter. In Banzer, W. (Ed.), Körperliche
Aktivität und Gesundheit. Präventive und
therapeutische Ansätze der Bewegungs- und
Sportmedizin (pp. 139-155). Berlin: Springer.
Gadde, P., Kharrazi, H., Patel, H. and MacDorman, K. F.,
2011. Toward Monitoring and Increasing Exercise
Adherence in Older Adults by Robotic Intervention: A
Proof of Concept Study. Journal of Robotics.
doi:10.1155/2011/438514
Görer, B., Salah, A. A. and Akın, H. L., 2017., An
autonomous robotic exercise tutor for elderly people.
Autonomous Robots, 41, 657-678.
Gschwind, Y.J. and Pfenninger, B., 2016. Training zur
Sturzprävention. Bfu-Fachdokumentation 2.104. Bern:
Beratungsstelle für Unfallverhütung.
Gunzelmann, T., Brähler, C., Hessel, A. and Brähler, E.,
1999. Körpererleben im Alter. Zeitschrift für
Gerontopsychologie & -psychiatrie, 12(1), 40-54.
Higgins, J. J., 2004. An introduction to modern
nonparametric statistics. Pacific Grove, CA:
Brooks/Cole.
Krug, S., Jordan, S., Mensink, G. B. M., Müters, S., Finger,
J. D. and Lampert, T., 2013. Körperliche Aktivität.
Ergebnisse der Studie zur Gesundheit Erwachsener in
Deutschland (DEGS1). Bundesgesundheitsblatt, 56,
765-771.
Lebedeva, A., Steinert, A., Buchem, I., Merceron, A.,
Kreutel, J. and Haesner, M., 2015. Trainingskonzepte
seniorengerecht und motivational entwickeln –
Handlungsempfehlungen aus Wissenschaft und Praxis.
8. AAL-Kongress in Frankfurt am Main.
Lewis, L., Metzler, T. and Cook, L., 2019. An Autonomous
Robot-to-Group Exercise Coach at a Senior Living
Community: A Study in Human-Robot Interaction. In
Rapid Automation: Concepts, Methodologies, Tools,
and Applications (pp. 1145-1163). IGI Global.
Löllgen, H. and Leyk, D., 2012. Prävention durch
Bewegung. Bedeutung der körperlichen
Leistungsfähigkeit. Der Internist, 53(6), 663-670.
López Recio, D., Márquez Segura, E., Márquez Segura, L.
and Waern, A., 2013. The NAO models for the elderly.
Proceedings of the 8th ACM/IEEE international
conference on Human-robot interaction, 187-188.
Matsusaka, Y., Fujii, H., Okano, T. and Hara, I., 2009.
Health exercise demonstration robot TAIZO and effects
of using voice command in robot-human collaborative
demonstration. 18th IEEE International Symposium on
Robot and Human Interactive Communication, 472-
477.
Mayring, P., 2000. Qualitative Content Analysis. Forum
Qualitative Sozialforschung / Forum: Qualitative
Social Research, 1(2), Art. 20.
Misoch, S., 2015. Qualitative Interviews. Berlin: Walter de
Gruyter GmbH.
Müller, C., Lautenschläger, S. and Voigt-Radloff, S., 2016.
Potential analysis for research on occupational therapy-
led physical exercise programmes and home
environment adaptation programmes to prevent falls for
elderly people living at home. International Journal of
Health Professions, 3, 85- 106.
Rosenthal-von der Pütten, A. M., Schulte, F. P., Eimler, S.
C., Sobieraj, S., Hoffmann, L., Maderwald, S., Brand,
M. and Krämer, N. C., 2014. Investigations on empathy
towards humans and robots using fMRI. Computers in
Human Behavior. 33, 201–212.
Schneider, S. and Kümmert, F., 2016. Exercising with a
humanoid companion is more effective than exercising
alone. 16th IEEE International Conference on
Humanoid Robots, 495-501.
Motivating Older Adults to Exercise at Home: Suitability of a Humanoid Robot
119

Scholes, S. and Mindell, J., 2012. Physical activity in
adults. Health Survey for England, 1(2), 1-49.
Seifert, A. and Meidert, U., 2018. Quantified seniors.
Prävention und Gesundheitsförderung, 13, 353-360.
Shen, Z. and Wu, Y., 2016. Investigation of practical use of
humanoid robots in elderly care centres. Proceedings of
the 4th International Conference on Human Agent
Interaction, 63-66.
Sherrington, C., Michaleff, Z. A., Fairhall, N., Paul, S. S.,
Tiedemann, A., Whitney, J., Cumming, R. G., Herbert,
R. D., Close, J. C. T. and Lord, S. R., 2016. Exercise to
prevent falls in older adults: an updated systematic
review and meta-analysis. British Journal of Sports
Medicine, 51, 1750-1758.
Torta, E., Oberzaucher, J., Werner, F., Cuijpers, R. H.,
Juola, J. F., 2013. Attitudes towards socially assistive
robots in intelligent homes: results from laboratory
studies and field trials. Journal of Human-Robot
Interaction, 1(2), 76-99.
Vaupel, J., 2000. Setting the stage: a generation of
centenarians? The Washington Quarterly, 23(3), 197-
200.
Voelcker-Rehage, C., Godde, B. and Staudinger, U. M.,
2006. Bewegung, körperliche und geistige Mobilität im
Alter. Gesundheitsschutz, 49, 558-566.
Ware, J. E., 2000. SF-36 health survey update. Spine, 25,
3130-3139.
Weber, D., Abel, B., Ackermann, G., Biedermann, A.,
Bürgi, F., Kessler, C., Schneider, J., Steinmann, R. M.
and Widmer Howald, F., 2016. Gesundheit und
Lebensqualität im Alter. Grundlagen für kantonale
Aktionsprogramme «Gesundheitsförderung im Alter»
(Bericht 5) Bern: Gesundheitsförderung Schweiz.
Werner, F., Krainer, D., Oberzaucher,J. and Werner, K.,
2013a. Evaluation of the acceptance of a social assistive
robot for physical training support together with older
users and domain experts. Assistive Technology: From
Research to Practice: AAATE, 33, 137-142. doi:
10.3233/978-1-61499-304-9-137
Werner, F., Werner, K. and Oberzaucher, J., 2013b.
Evaluation of the acceptance of a socially assistive
robot by older users within the project KSERA.
Proceedings: Lebensqualität im Wandel von
Demografie und Technik. Deutscher AAL-Kongress.
World Health Organization, 2015. World report on ageing
and health. Geneva: World Health Organization.
ICT4AWE 2020 - 6th International Conference on Information and Communication Technologies for Ageing Well and e-Health
120
