
Towards a Generic Framework for a Health Behaviour Change
Support Agent
Fawad Taj
a
, Michel CA Klein
b
and Aart Van Halteren
c
Social AI Group, Vrije Universiteit, Amsterdam, The Netherlands
Keywords: BDI-based Agent, Health Behavior Change Agent, Behavior Change Technique.
Abstract: Agent-oriented solutions form a useful paradigm to design intelligent systems. For health-related behaviour
change, this is also a promising approach. Designing an agent for lifestyle change interventions is a difficult
task because socio-ecological models are involved that represent many conflicting desires and goals. Different
types of cognitive architectures are available to design this type of health behavior agents but they are rarely
used. In this paper, we used the BDI model to design a health behavior agent that will execute behavior change
intervention for a better healthy lifestyle. We explain the working of the architecture by the example of an
agent which uses adaptive goals-setting and a percentile scheduling technique for increasing physical activity.
1 INTRODUCTION
One approach to build real-world complex systems is
using the agent-oriented paradigm. In this paradigm,
software components are tightly connected with one
another and they all function autonomously. Artificial
intelligence provides a major contribution to the agent
development paradigm due to the required properties
of autonomy, cognitive thinking, sociability and
learning (Girardi, 2001). Cognitive agents in artificial
intelligence are among the most developed and
studied topics, which explicitly maintains the model
of the environment perceive the external
environment, do rational thinking and make a plan to
act on the environment to fulfil one or more of its goal
(Wooldridge, 1995). Agent-based modelling is
common and brings significant advantages to systems
when the environment is complex, the interaction
between agents is nonlinear, discontinuous or the
population is heterogeneous (Bonabeau, 2002).
Health-related systems are complex, due to some
hard topics like patient life, data privacy, legal and
technical issues. For example delay or
misinterpretation between different entities/agents
could cost someone life (Datta et al., 2010)(Iqbal et
al., 2016). The use of agent systems in healthcare
setups has increased in the last decade and the usage
a
https://orcid.org/0000-0001-9049-1736
b
https://orcid.org/0000-0003-4119-1846
c
https://orcid.org/0000-0002-9631-0657
ranges from patient-centred applications to the
organizations-centred, multi-agent system (Isern &
Moreno, 2016). Drawing on (Datta et al., 2010)(Iqbal
et al., 2016), recent reviews about agents applied in
health-care, categorized the agents both on the basis
of intended users and functionality. The applications
are mainly patient-centered, staff-centered or
healthcare organization-centred and with respect to
functionality basis, they can be designed for planning
and resource management, decision support system,
data management, self-care systems and can be
multifunction systems that can integrate some of the
earlier describe systems to make a complete
healthcare system. Another subset of health-care
systems is behavior change support systems, which
could benefit from agent-based intelligent models to
facilitate rational and on-time decisions in a
heterogeneous environment.
An approximate 60% of the risks associated with
chronic diseases such as diabetes and cardiovascular
disease are associated with health habits and these
conditions account for 1.5%-3% of direct costs to the
UK National Health Service (NHS) (GC et al., 2016).
It is becoming critically important to question the
creation and implementation of effective methods to
improve healthy behavior. With a change in lifestyle
and prevention techniques, we can significantly
Taj, F., Klein, M. and Van Halteren, A.
Towards a Generic Framework for a Health Behaviour Change Support Agent.
DOI: 10.5220/0009173503110318
In Proceedings of the 12th International Conference on Agents and Artificial Intelligence (ICAART 2020) - Volume 1, pages 311-318
ISBN: 978-989-758-395-7; ISSN: 2184-433X
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
311

decrease the impact of non-communicable diseases,
which are some of the greatest challenges facing
modern society. Some of the key unhealth behaviors,
such as physical inactivity, unhealthy eating,
smoking, obesity, sexual behavior, and alcohol
misuse are among the most common causes of disease
and premature deaths in both developed countries
(Ding, Lawson, & Lancet, 2016).
While this prior research on improvements in
health behavior is critical in defining pragmatic
approaches that could lead to changes in health
behaviour, the theories developed in it are insufficient
to support the development of quantitative delivery
methods. Furthermore, the proposed theory-based
models consider health behavior as a function of
constructs such as motivation, attitude as opposed to
a product of a dynamic cognitive system that is
influenced by physiological, affective,
environmental, social, and experiential states (Riley
et al., 2011). Agent-based modelling, in contrast,
provides the opportunity to define simple reflexive
agent up to more complex cognitive learning agents.
When designing and developing agent-based
systems, an important question is to choose or
develop the decision-making process of agents. There
are around 15 famous decision-making models in the
literature, each based on different literature studies
(Balke & Gilbert, 2014). The main inspiration for
these decision-making systems are the human
psychological and neurological systems. A widely
used way to formalize the internal architecture of
such complex agents is the BDI (Belief-Desire-
Intention) paradigm. This paradigm allows to design
expressive and realistic agents, yet, it is rarely used as
an intelligent health behavior change agent. We argue
that health-behavior coaching – helping people to
develop helpful health-related behaviors and to
curtail harmful ones – is a challenging as well as a
fruitful domain to conduct human-aware AI research.
The domain requires that a health coach understand
the cognitive, emotional, physical, situational, and
other aspects of a coaches’ health behaviors. The
possible interventions vary from providing
informational support, encouraging the practice of
helpful behaviors in different contexts, helping to
remember behaviors when the right context arises,
etc. To be impactful, these agents need to make a
more personalized decision and gradually adapted for
their specific circumstances. This paper presents a
generic framework for a health behavior support
agent, inspired by the BDI paradigm.
This article is structured as follows: section 2 will
discuss the concept of health behavior change and the
guidelines to define healthy behavior intervention.
Section 3 discusses agent architecture based on BDI.
Section 4 will define the components based on the
discussion in section 2. This section will discuss the
working of the model with the help of physical
activity scenario and discusses agent-based
programming algorithm. Finally, section 5 will
discuss future work and draw a conclusion on earlier
sections and will discuss the future directions.
2 BACKGROUND
In this section, we describe the theoretical
components of a health behaviour support agent.
Before defining the goals and plans for the agent, we
should determine the desired results of the agent in
detail. First, we have to decide the goal and plan
occurring in a different context. It is recognised that
any behavior that needs to be changed occurs in
several different contexts (e.g. at home, at work) and
have many different influences (e.g. personal,
interpersonal and environmental). Therefore,
different intervention results for each context and
level of influence were therefore defined. For this
purpose different taxonomies and planning guides
can be consulted (Kok, 2014). Using the steps defined
in these planning guides we can identify the context,
the performance outcome, and select the right
behavior change strategies.
Certain behaviors can be targeted with different
behavior change techniques (BCTs), which acts as an
active ingredient in any behavior change intervention.
Each BCT use a different mechanism of action to
target certain behavior (Michie & Johnston, 2012).
The interventions are usually delivered by expert
humans through a prolonged interaction with the
people they coach. According to (Taj, Klein, & van
Halteren, 2019), these BCTs are poorly reported and
the most used technique is the goal-setting
irrespective of target health domain. Each of these
behavior change techniques is differently modelled
and mathematically represented. For example, the
goal-setting technique is represented as the staircase
model to set an adaptive goal for coachee (Mohan,
Venkatakrishnan, 2017), whereas in another example
the adaptive goals are calculated with percentile
schedule method (Adams, 2009). Based on this
background knowledge we defined different
parameters for our physical activity agent in section
4.
ICAART 2020 - 12th International Conference on Agents and Artificial Intelligence
312
3 BDI ARCHITECTURE
3.1 Overview
The BDI approach in artificial intelligence represents
the way agents can do complex reasoning based on
folk psychology (Bratman, 1987). The three main
mental states around which the BDI model is centred
are belief, desire, and intentions. A typical BDI agent
represents all the information that it has about the
environment in the form of beliefs and these beliefs
can be represented by modal logic language. These
beliefs can be either true, false or outdated. The agent
has some desires that it wishes to accomplish. Not all
but for some desires that the agent actively wants to
achieve turns to become intentions and the agent is
equipped with a pre-defined set of plans which are
recipes for achieving its intentions (Visser et al.,
2016).
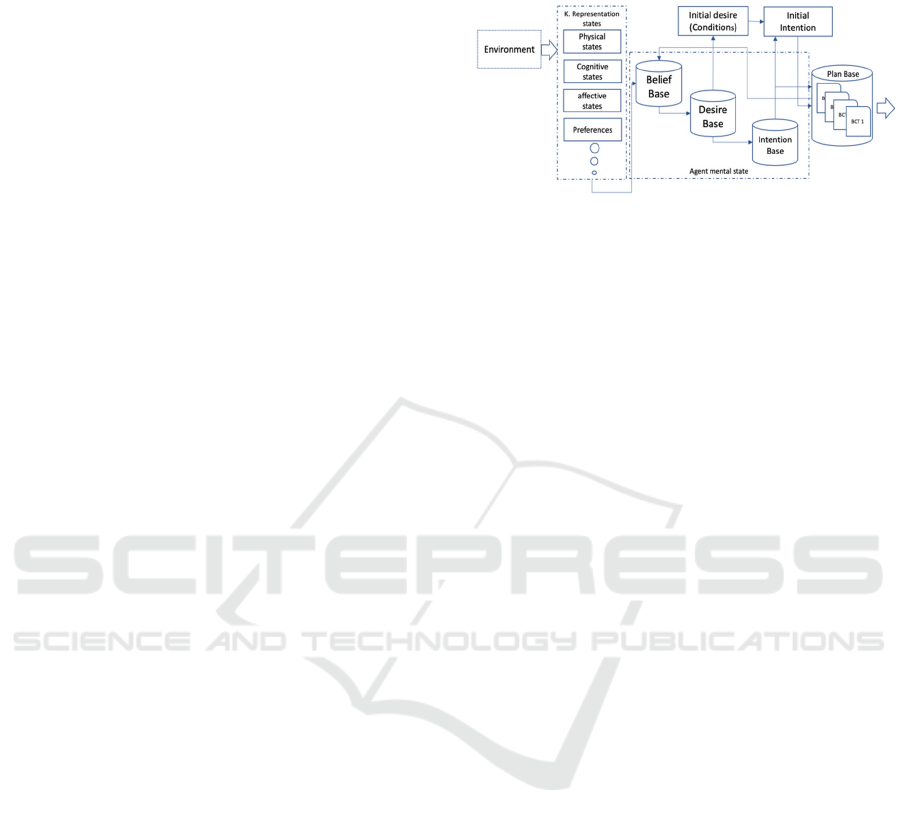
An agent architecture shown in figure 1 is a
software computational solution to a problem
showing how the component parts of a system
interact, thus providing an overview of the system
structure. It encodes its sensory perceptions into a
state representation of its environment. It also
represents the plans it can execute to manipulate its
sensors, effectors, and the environment in pursuit of
goals.
The basic logic components of a BDI agent are
belief, desire and intention. In our model we follow
the conventions adopted in the GAMA-platform- a
control architecture, which in turn are based on PRS
(Procedural Reasoning System). The vocabulary of
the key terms of the architecture can be summarized
as follows.
3.2 Vocabulary
3.2.1 Knowledge States
The agent must represent the environment by
capturing information that is necessary to not only
formulate a beneficial goal state but also to decide
over its action space. All the information about the
environment is represented in the different
representation states. For example, the affective states
can be represented as a different scale, whereas the
preference value can be represented as logical
predicates. These states will not only be used to
update the belief of the agent but also will help in
defining the algorithm of behavior change techniques.
In figure 1 a few of possible knowledge states are
mentioned; however, any number and types of states
can be considered depending on the behavior the
agent is targeting.
Figure 1: Conceptual diagram of BDI behavior change
agent.
3.2.2 Beliefs
Belief is the agent knowledge about the world. The
belief base always gets updated with the new
information in representation states. The beliefs of the
BDI is usually represented as predicates for example,
Step_count (Monday, 3000)- a person steps count for
Monday is 3000 steps. Belief can either be true or
false.
3.2.3 Desire
Desires are all the objectives that the agent wants to
achieve and often called the goal of the agent. It can
have hierarchical links (sub/super desires) or each
desire can be defined with a dynamic priority value.
For example, the agent can have different conflicting
desires which can be ordered according to some
priority values according to the intervention. For
example, for “set goal” desire will be having higher
priority than giving a reward.
3.2.4 Intentions
Among the desires that an agent wants to achieve it
select one having high priority. The intention will
determine the selected plan. That is the reason that
BDI based agents are usually called intention systems
(Balke & Gilbert, 2014).
3.2.5 Plan
The agent plan base consists of actions that the agent
would carry to fulfil its selected intention. In our
architecture shown in Figure 1, most of the plans are
the delivery or implementation of behavior change
techniques. Now to define a plan for certain desire
regarding behavior change the plan needs to have
some pre and post conditions and the body which in
our case can raise to the question that which behavior
Towards a Generic Framework for a Health Behaviour Change Support Agent
313
change techniques are best for which kind of health-
related problem. There are a lot of randomized control
trials available that can help us define our plan. For
example, to implement goal-setting intention, the most
used behavior change technique is the goal setting.
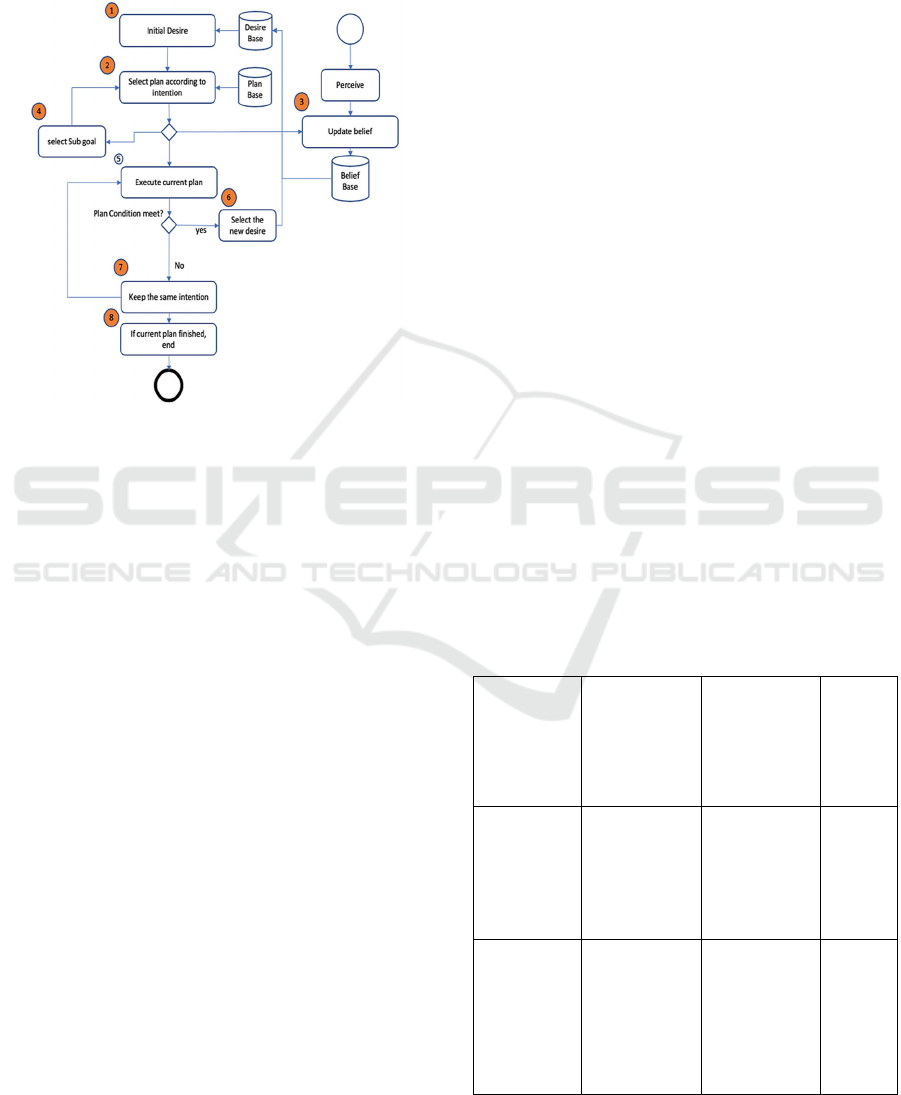
Figure 2: The flow chart of behavior change agent.
3.2.6 Behavior Change Techniques
Algorithms
The plan base in architecture shown in Figure 1
contains behavior change techniques algorithms where
all the relevant BCTs can be placed so that the agent
can reason about it and select one that is relevant and
feasible to the scenario. In health behavior change
literature several constructs such as goal-setting, self-
efficacy, reward shaping and incentives are defined
and extensively studied to positively influence health
behavior. The well-known hierarchy taxonomy by
Susan can be considered to properly report and define
the intended construct (Michie et al., 2013).
The algorithm for each of the BCT will explain post
and pre-conditions, and intensity of the BCT. Currently
the efficacy of different kind of BCTs are not
established with regard to different behavior. Different
people define each type of BCT with their unique
algorithm. This is why the algorithm for BCT is shown
separate than simple plans.
3.3 Workflow
In the BDI practical reasoning, the agent is equipped
with a library of pre-compiled plans. These plans are
manually constructed, in advance, by the agent
programmer. Hence in Table 1 we define performance
outcomes as the goal of the agent and defined the plan
as the execution of relevant BCT.
The flow of the process depicted in Figure 2 is as
follow:
1. Set initial goal: The initial goal will be the
behavioral outcomes that we want to achieve.
2. Plan execution: execute the relevant plan which
can be either to select the sub-goal or update the
belief base.
3. Perceptions are updated: For each behavioral
goal, the second step is to perceive the relevant
information from the environment and update
agent belief base.
4. If the current goal contains a sub-goal it would
hold the current goal on hold and will select the
sub-goal and will select the relevant plan for it.
5. If the current goal doesn’t have any sub goals and
don’t need to update the belief base the current
plan would be executed.
6. After successful completion of the plan, the new
desire with the highest priority would be selected.
7. Until the successful completion of the current
plan, the current intention would still in hold and
will execute until get finished.
8. The reasoning end if there is no plan and desire
available for execution.
4 SCENARIO
Using the planning guidelines discussed in section 2,
Table 1: The behavior change performance objectives and
selected methods.
Target
population:
individual
Target
behavior:
Physical
activity
Determinant:1
Intention
Determinant:2
Motivation
Selected
BCT
Performance
outcome:
increase
number of
daily steps
count
A resolve to act
on certain way
Goal
Setting
(behavior)
Performance
outcome:
Keep
motivation
for behavior
outcome
Arrange reward
if and only if
there is an
effort to
achieve the
targeted
behaviour
Rewards
ICAART 2020 - 12th International Conference on Agents and Artificial Intelligence
314

we will choose some specific components for our
example. Table 1 shows the performance outcomes
and the mechanism of action (determinants)-through
which we will achieve our target in our example
scenario that is presented below. The last column
shows the selected BCTs that are considered best in
literature for these kinds of targets. We considered
adaptive goal-setting techniques for the daily
recommended steps. The mathematical formulation
and algorithm are defined in section 4.1.
4.1 Adaptive Goals and a Percentile
Schedule of Reinforcement
Adaptive goals that often and uniquely adjust to the
recent performance of an individual may be a more
realistic approach to developing flexible yet
challenging and achievable goals. The goal-setting
and feedback algorithm was based on a rank-order
percentile algorithm derived from recent
developments in basic science around schedules of
reinforcement (Adams, 2009). The percentile
algorithm requires continuous and repeated
measurements of daily steps count and then the
algorithm work as follow:
1. The ranking of a sample of behavior (steps/day)
from lowest to highest and calculation of a new goal
based on a pth percentile criterion. For example, for
one participant, the steps count each day for their last
9 days (ranked from lowest to highest) was 1000,
1500, 2600, 4500, 5000, 5700, 6300, 8000, 11,000.
2. The 60th percentile represents a goal of 5700
steps, which becomes the 10th day's goal. Based on
(Adams, 2009), the best window to consider is of 9
window and the pth percentile 60% of the last 9
reading which is calculated with
=((p/100) * no_day). (1)
To achieve customized targets, percentile shaping
capitalizes on the normal behavioral variability.
Percentile shaping also generates specific,
measurable goals inherently that can be explicitly
rewarded. Only a handful of studies have evaluated
the use of a percentile shaping strategy by changing
goals to increase physical activity, and none have
compared percentile shaping goals orthogonally
(Adams, 2009).
In our example, the aim is to develop an intelligent
agent that can provide counselling in a manner similar
to a human coach. There is a need for computational
methods that can not only model and predict the
changes in the human physiological and cognitive
system, but also for methods that can coach this
human system toward a beneficial goal (Shiwali
Mohan & Venkatakrishnan, 2017). The working of
the agent for the given scenario below is depicted in
Figure 3.
The BDI health behavior agent model function as
follows: our agent aims to assist in delivering the best
available BCT for increasing physical activity and
keep the motivation high to maintain the behavior. To
make it simple we considered simple physical activity
guidelines of 10000 steps per day by the National
Heart Association of Australia (Tudor-Locke et al.,
2011). To achieve this goal, a number of behavior
change techniques can be applied but according to the
literature, the mostly applied BCT for physical
activity behavior is goal-setting. The goal-setting
theory by Locke and Latham (Locke & Latham,
2012) provides evidence that to be maximally
effective, the goals should be difficult yet attainable.
Therefore, for adherence purpose, the agent will set a
new adaptive goal for the coachee each day if the
coachee didn’t meet the standard guidelines.
Moreover, for motivation and reinforcement purpose,
if the coachee meeting the guidelines the coachee will
be awarded rewards. To make it short, the main goal
is to assist user to maintain 10000 steps count daily
and sub goals to achieve this main goal is goal setting
and reward.
According to the flow diagram discussed in Figure
2 the flow of the process of our scenario is as follows:
1. Initial goal of increasing physical activity is
depicted as initial desire: Keep_Fit
2. To fulfil this desire the plan is to start monitoring
daily steps count and update the belief base
accordingly. For example, step_count(Monday,
3000)- a person steps count for Monday is 3000
steps.
3. while executing the monitoring plan and adding
new belief about daily step count. A rule is
introduced which add new sub-goal of goal setting
by applying the following rule.
Rule: with each belief: Steps_count add
New_desire: goal_setting
4. For this new desire of goal setting the plan is to
call the adapting goal setting algorithm. Which is
explained in section 4.1.
5. The execution of the plan will also update the
belief base of the agent.
6. Whenever the step counts would be more than
1000 per day the goal setting plan would generate
a new sub-goal of reward.
add_sub_intention(reward)
Towards a Generic Framework for a Health Behaviour Change Support Agent
315
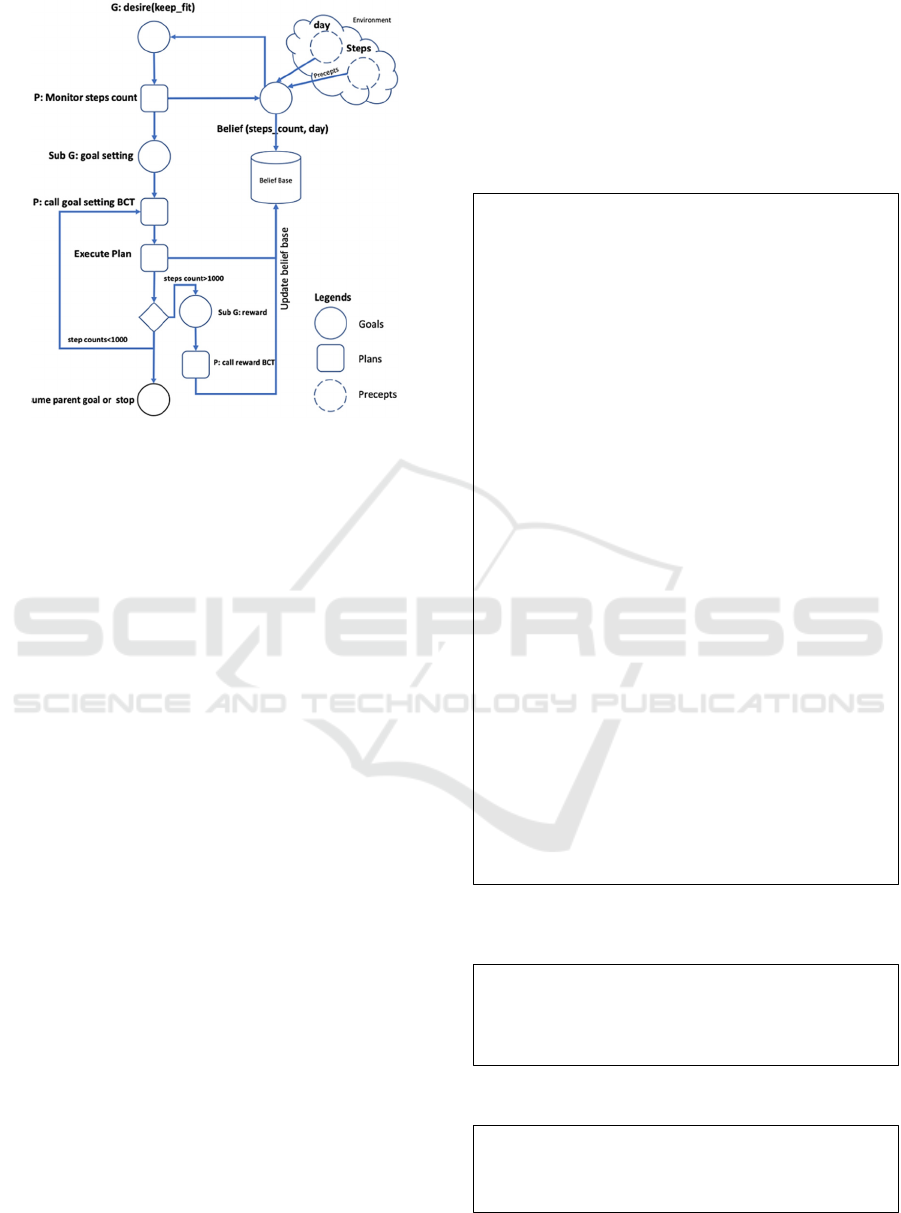
Figure 3: Flow chart of the scenario.
4.2 ABMS Platforms and Languages
for Simulating BDI Agents
The design of its internal architecture is an important
decision when developing a software agent. Several
models of deliberative, reactive, and hybrid
architectures have already been proposed. BDI
architecture is one of the most popular agent decision-
making models in the community of agents. BDI
architectures have been introduced in several agent-
based modelling and simulation (ABMS) platforms.
For example, the BDI paradigm integrated into the
GAMA modelling platform and its GAML modelling
language to manipulate BDI concepts in a simple
language (Taillandier, Bourgais, Caillou, Adam, &
Gaudou, 2017). There also exists some middleware to
connect the famous ABMS platform to BDI
frameworks e.g. JACK (Busetta, Rönnquist,
Hodgson, & Lucas, 1999) and Jadex (Pokahr,
Braubach, & Lamersdorf, 2005).
A programming language is an essential
component of agent-based technology and agent-
based systems implementation. Such a language,
called an agent-oriented programming language,
should provide high-level abstractions and constructs
for developers to implement and use agent-related
concepts directly. Some of the famous languages
Agent-oriented languages that support BDI
architecture are AgentSpeak(L), Jason, Af-APL,
2APL, JACK(L), JADEX, GOAL etc.
We will illustrate our scenario using a
programming language. Algorithm 1 is developed
with the close syntax to GAML modelling language
but it can be modelled in any agent-oriented language.
Algorithm 2 shows the goal-setting algorithm and
algorithm 3 keep track of the reward for achieving the
goal. The algorithm uses an existing constraint solver
and does not need to modify or enforce the
vocabulary of the BDI.
Algorithm 1: BDI based goal-setting agent.
Algorithm 2: Adaptive goal based on Percentile schedule
algorithm.
Algorithm 3: Reward algorithm.
Procedure Main()
Create agent
goal_setting_agent
name of
the agent
Target_steps:1000#day
Reward:0 Percentile:
p
Agent goal_agent Control::BDI
Procedure init() {
add Desire
keep_fit }
Perceive target:no_of setps var:day
Add belief: Steps_count var: day
i
Do remove_intention(keep_fit, false)
Rules belief: Steps_count New_desire: goal_setting
Plan record_steps_count where intention: keep_fit
Do read_daily_steps_count
Plan set_goal where intention: goal_setting
If current_step_count < Target_steps
Do add_sub_intention(get_current_intention(),
find_adaptive_goal, true )
Do current_intention_on_hold();
Else
Do add_sub_intention(reward)
Plan adaptive_goal where intention:
find_adaptive_goal_perc
Call Adaptive_percentile_goal (days
,
,p)
Goal
setting algorithm
do remove_intention(find_adaptive_goal_perc,
true)
Plan calculate_reward where intention: reward
Call reward()
reward algorithm
do remove_intention(reward, true)
Procedure Adaptive_percentile_goal (no_days, p
th
)
Do arrange daily_steps_count in ascending order
Compute the position of p
th
percentile /60
th
Return ((p/100)*no_day)
Procedure reward ()
Do add reward=reward+1
make sure
reinforcement
ICAART 2020 - 12th International Conference on Agents and Artificial Intelligence
316

5 FUTURE WORK
In this article, we explore ways that an agent system
can specify the goal for the coachee according to his
previous performance which is incorporated into the
BDI execution process and used to guide the choices
made.
The future direction would be to implement this
algorithm with any agent base modelling
environment and will simulate it. The agent
technology is rarely adopted in health behavior
domain so there is so much opportunity to include
knowledge from behavior sciences. For example,
adding more personalization aspect to agent e.g. a
value-based planning approach which takes into
account social and ethical values that affect decision-
making (Cranefield, Winikoff, Dignum Delft
MVDignum, & Frank Dignum, 2017).
The health behavior agent needs to consider the
causal model which can assess the failure or success
of the intervention, this can be achieved by
considering a causal model within the BDI
architecture. The coachee may not have enough
expertise or resources to conduct the behavior, may
not believe they can execute the behavior effectively
(low self-efficacy), may not have the right emotional
state or having some social norms etc. (Shiwali
Mohan & Venkatakrishnan, 2017). This kind of
model is already available which can initially do
reasoning about unwanted behavior (Klein, Mogles,
& Van Wissen, 2011), which can likely be modelled
according to BDI architecture.
Furthermore, a promising direction to equip the
health change agent with a functionality that allow it
to reason about the reasoning of the coachee. This
topic has received significant research attention and
can be explored with the help of implementing
Theory of Mind (ToM). Theory of mind provides an
important understanding of how human reason about
other mental states (Baron-Cohen, Leslie, & Frith,
1985). There is some research which introduces a
formal BDI-based agent model for Theory of Mind,
which can be used or modified to reason about the
coachee health-related constructs (Bosse, Memon, &
Treur, 2007).
6 CONCLUSION
In this paper, we proposed a design of a BDI based
health behavior agent model that can monitor and
reason about the different psychological and
physiology constructs of its user. The knowledge
about the environment is represented in the form of beliefs
and the intentions are fulfilled in the form of delivering the
right kind of behavior change technique. The model is
illustrated with the help of an example of physical activity
coach which records the daily steps count of the coachee
and according to the adopted goal-setting technique, the
agent selects goals that are appropriate for a coachee given
the past history of performance. The agent’s other goal is to
keep the motivation high for which the agent uses the
reward-based behavior change technique.
REFERENCES
Adams, M. A. (2009). A pedometer-based intervention to
increase physical activity: Applying frequent, adaptive
goals and a percentile schedule of reinforcement. UC
San Diego.
Balke, T., & Gilbert, N. (2014). How do agents make
decisions? A survey. Journal of Artificial Societies and
Social Simulation, 17(4), 13.
Baron-Cohen, S., Leslie, A. M., & Frith, U. (1985). Does
the autistic child have a “theory of mind” ? Cognition,
21(1), 37–46. https://doi.org/10.1016/0010-
0277(85)90022-8
Bonabeau, E. (2002). Agent-based modeling: Methods and
techniques for simulating human systems. Proceedings
of the National Academy of Sciences, 99(suppl 3),
7280–7287.
Bosse, T., Memon, Z. A., & Treur, J. (2007). A two-level
BDI-agent model for theory of mind and its use in social
manipulation. In Proceedings of the AISB 2007
Workshop on Mindful Environments (Vol. 4, pp. 335–
342).
Bratman, M. (1987). Intention, plans, and practical reason.
Busetta, P., Rönnquist, R., Hodgson, A., & Lucas, A.
(1999). Jack intelligent agents-components for
intelligent agents in java. AgentLink News Letter, 2(1),
2–5.
Cranefield, S., Winikoff, M., Dignum Delft MVDignum, V.
T., & Frank Dignum, tudelftnl. (2017). No Pizza for
You: Value-based Plan Selection in BDI Agents.
Datta, A., Dave, N., Mitchell, J. C., Nissenbaum, H.,
Sharma, D., & others. (2010). Privacy Challenges in
Patient-centric Health Information Systems. In
HealthSec.
Ding, D., Lawson, K., Lancet, T. K.-A.-T., & 2016,
undefined. (n.d.). The economic burden of physical
inactivity: a global analysis of major non-
communicable diseases. Elsevier. Retrieved from
https://www.sciencedirect.com/science/article/pii/S014
067361630383X
GC, V., Wilson, E. C. F., Suhrcke, M., Hardeman, W., &
Sutton, S. (2016, April 1). Are brief interventions to
increase physical activity cost-effective? A systematic
review. British Journal of Sports Medicine. BMJ
Publishing Group. https://doi.org/10.1136/bjsports-
2015-094655
Towards a Generic Framework for a Health Behaviour Change Support Agent
317

Girardi, R. (2001). An analysis of the contributions of the
agent paradigm for the development of complex systems
1.
Iqbal, S., Altaf, W., Aslam, M., Mahmood, W., & Khan, M.
U. G. (2016). Application of intelligent agents in
health-care: review. Artificial Intelligence Review,
46(1), 83–112. https://doi.org/10.1007/s10462-016-
9457-y
Isern, D., & Moreno, A. (2016). A Systematic Literature
Review of Agents Applied in Healthcare. Journal of
Medical Systems, 40(2), 1–14. https://doi.org/10.1007/
s10916-015-0376-2
Klein, M., Mogles, N., & Van Wissen, A. (2011). Why
won’t you do what’s good for you? Using intelligent
support for behavior change. In International Workshop
on Human Behavior Understanding (pp. 104–115).
Kok, G. (2014). A practical guide to effective behavior
change How to apply theory- and evidence-based
behavior change methods in an intervention. The
European Health Psychologist, 16(5), 156–170.
Retrieved from https://www.ehps.net/ehp/index.php/
contents/article/viewFile/ehp.v16.i5.p156/8
Locke, E. A., & Latham, G. P. (2012). Goal setting theory.
In Motivation: Theory and research (pp. 23–40).
Routledge.
Michie, S., & Johnston, M. (2012). Theories and techniques
of behaviour change: Developing a cumulative science
of behaviour change. Health Psychology Review, 6(1),
1–6. https://doi.org/10.1080/17437199.2012.654964
Michie, S., Richardson, M., Johnston, M., Abraham, C.,
Francis, J., Hardeman, W., … Wood, C. E. (2013). The
behavior change technique taxonomy (v1) of 93
hierarchically clustered techniques: building an
international consensus for the reporting of behavior
change interventions. Annals of Behavioral Medicine,
46(1), 81–95.
Mohan, S, Venkatakrishnan, A., … M. S.-T.-N. I., & 2017,
defined. (n.d.). On designing a social coach to promote
regular aerobic exercise. Aaai.Org. Retrieved from
https://www.aaai.org/ocs/index.php/IAAI/IAAI17/pap
er/viewPaper/14963
Mohan, Shiwali, & Venkatakrishnan, A. (2017). Health
Behavior Coaching: A Motivating Domain for Human-
Aware Artificial Intelligence Research Advanced
Cognitive Learning for Embodied Language (AILEEN)
View project Interactive Task Learning View project.
Retrieved from www.aaai.org
Pokahr, A., Braubach, L., & Lamersdorf, W. (2005). Jadex:
A BDI Reasoning Engine (pp. 149–174).
https://doi.org/10.1007/0-387-26350-0_6
Riley, W. T., Rivera, D. E., Atienza, A. A., Nilsen, W.,
Allison, S. M., & Mermelstein, R. (2011). Health
behavior models in the age of mobile interventions: are
our theories up to the task? Translational Behavioral
Medicine, 1(1), 53–71.
Taillandier, P., Bourgais, M., Caillou, P., Adam, C., &
Gaudou, B. (2017). A BDI agent architecture for the
GAMA modeling and simulation platform. In Lecture
Notes in Computer Science (including subseries
Lecture Notes in Artificial Intelligence and Lecture
Notes in Bioinformatics) (Vol. 10399 LNAI, pp. 3–23).
Springer Verlag. https://doi.org/10.1007/978-3-319-
67477-3_1
Taj, F., Klein, M. C. A., & van Halteren, A. (2019). Digital
Health Behavior Change Technology: Bibliometric and
Scoping Review of Two Decades of Research. JMIR
MHealth and UHealth, 7(12), e13311.
Tudor-Locke, C., Craig, C. L., Brown, W. J., Clemes, S. A.,
De Cocker, K., Giles-Corti, B., … others. (2011). How
many steps/day are enough? For adults. International
Journal of Behavioral Nutrition and Physical Activity,
8(1), 79.
Visser, S., Thangarajah, J., Harland, J., & Dignum, F.
(2016). Preference-based reasoning in BDI agent
systems. Autonomous Agents and Multi-Agent Systems,
30(2), 291–330. https://doi.org/10.1007/s10458-015-
9288-2
Wooldridge, M., review, N. J.-T. knowledge engineering,
& 1995, undefined. (n.d.). Intelligent agents: Theory
and practice. Cambridge.Org. Retrieved from
https://www.cambridge.org/core/journals/knowledge-
engineering-review/article/intelligent-agents-theory-
and-practice/CF2A6AAEEA1DBD486EF019F6217F1
597
ICAART 2020 - 12th International Conference on Agents and Artificial Intelligence
318
