
The Effects of a Nursing Care Plan Incorporated with a Decision
Support System on Ventilator Associated Pneumonia: A Case Study
Ozgur Bolat
1a
, Nalan Gulenc
1b
, Elife Ozkan
1c
, Nuran Aydin
2d
and Ilker Kose
3e
1
Izmir Tire Public Hospital, Izmir, Turkey
2
Department of Midwifery, Istanbul Medipol University, Istanbul, Turkey
3
Department of Health System Engineering, Istanbul Medipol University, Istanbul, Turkey
Keywords: Ventilator Associated Pneumonia, Nursing Care, Decision Support System, Intensive Care Unit.
Abstract: The risk of pneumonia is high in patients who are ventilated in intensive care units (ICUs). Without proper
and adequate care, this risk and the mortality rate increases. In a study conducted by the infection committee
of our hospital (İzmir Tire State Hospital, the first digital (Stage 7) hospital in Turkey in 2016), it was found
that the rate of ventilator-associated pneumonia (VAP) cases increased had increased over three years (2015-
17) and was well above the national average. In this study, VAP prevalence in our ICU and the associated
extra medication costs were calculated. Furthermore, nursing care plans related to VAP were reviewed and
improvements were made according to international standards. The care plan was triggered by criteria defined
in a clinical decision support system (CDSS) on the hospital information management system (HIS), and
monitorization was conducted to ensure that nurses implement the care plan in a comprehensive and timely
manner. As a result of the change, the rate of VAP cases, which had risen to 4.5% in 2017, was reduced to
0.5% in 2018. Similarly, we achieved cost reductions of 90.87% for VAP-based extra medications. Based on
these results, it can be suggested that CDSS-supported nursing care can significantly reduce the risk of VAP
and increase patient safety in the ICU.
1 INTRODUCTION
Ventilator-associated pneumonia (VAP), defined as
pneumonia between 48 and 72 hours following
endotracheal aspiration, is the most common
infection among intensive care unit patients receiving
mechanical ventilatory support (Kapucu & Ozden,
2014). In a study conducted at the national level in the
USA, it was estimated that a significant 10% of
patients who are connected to mechanical ventilators
are diagnosed with VAP (Wang et al., 2014). Other
studies found that mortality rates of 20-50% in
patients connected to ventilators in intensive care
units may be reduced by 13% (Klompas & Li, 2013;
Melsen et al., 2013; Sara, Phillips, Kaur, & Isaac,
2015).
a
https://orcid.org/0000-0003-4411-1696
b
https://orcid.org/0000-0003-1696-9943
c
https://orcid.org/0000-0002-8805-9338
d
https://orcid.org/0000-0003-0582-1484
e
https://orcid.org/0000-0002-5549-5579
According to a recently published systematic
review of VAP, the aims of several studies to identify,
prevent, and treat VAP epidemiology were related to
the prevention of associated mortality and morbidity,
to reduce costs, and to improve the quality of care
(Gutiérrez et al., 2019). Studies in different countries
indicate that the development of VAP in patients
increases the duration of ventilator utilization and
hospital stay and increases patient care and treatment
costs (Kalil et al., 2016), (Başyiğit, 2017; Hayashi et
al., 2013; Luckraz et al., 2018; S et al., 2017).
There are many approaches to preventing the
development of VAP, such as infection control
measures, minimum possible intubation, re-training
of health personnel, and using care guidelines
(Gutiérrez et al., 2019). Alternative VAP care
management plans are prepared and recommended by
Bolat, O., Gulenc, N., Ozkan, E., Aydin, N. and Kose, I.
The Effects of a Nursing Care Plan Incorporated with a Decision Support System on Ventilator Associated Pneumonia: A Case Study.
DOI: 10.5220/0009164706930698
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 693-698
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
693

recognized organizations, such as the European
Respiratory Society (ERS), the European Society of
Intensive Care Medicine (ESICM), and the European
Society of Clinical Microbiology and Infectious
Diseases (ESCMID) (Torres et al., 2018). The use of
care plans has consistently been found to decrease the
duration of VAP-related length of stay, reduce
complications, decrease antibiotic usage, and
decrease antibiotic resistance; all of which reduce the
amount of time and money lost due to VAP. The
move from handwritten care plans to digital plans is
effective in improving VAP control and reducing
VAP-associated length of stay, useful in decreasing
antibiotic use, and effective in reducing loss of time
and money (Kalil et al., 2016), (Wang et al., 2014),
(Klouwenberg et al., 2014), (Liao et al., 2019).
Digital care plans have been shown to have an impact
on decreasing VAP-related complications and the
number of ventilator-associated tracheobronchitis
(VAT) events (Neuville, Mourvillier, Bouadma, &
Timsit, 2017).
Completing VAP checklists on paper is not
efficient due to errors and omissions. Missing data in
manually generated records may cause insufficient
evaluations. Studies have shown that the transfer of
checklists to digital media helps to reduce these
problems (Liao et al., 2019), (De Bie et al., 2017),
(Klompas, Kleinman, & Platt, 2008).
Although it is controversial whether the
development of VAP and VAP-related complications
should be used to measure the quality of patient care
(Kalil et al., 2016), (Klompas & Berra, 2016),
particularly in developing countries, there are
significant costs associated with VAP (Alp et al.,
2012). The results of studies conducted in Turkey are
consistent with other studies in the literature.
According to 2017 data from the business intelligence
application of the Ministry of Health, the average rate
of VAP in Level 2 ICUs in Turkey was 3.8%, while
İzmir Tire State Hospital had a VAP rate of 4.5%,
which is 18.42% higher than the national average
(Kapucu & Ozden, 2014), (Alp et al., 2012; Grassie
& Gevrek, 2016; Karaoglan et al., 2010; Torres et al.,
2017).
In 2016, İzmir Tire State Hospital was designated
as the first digital hospital (Stage 7) according to
Healthcare Information and Management Systems
Society (HIMSS) Electronic Medical Record
Adoption Model (EMRAM) reguirements (HIMSS
Analytics, 2018). This study examines the effects of
incorporating VAP care plans and patient monitoring
with a clinical decision support system (CDSS)
application within the hospital information
management systems (HIS).
2 METHODS
In the first stage of the study, the incidence of VAP,
the number of patients diagnosed with VAP, and the
cost of extra medications associated with VAP were
tracked between 1 January and 31 December, 2018.
The Level 2 intensive care unit at İzmir Tire State
Hospital has 15 ventilators and 17 beds. All nursing
forms and nursing care plans related to VAP
prevention and care that were used in the hospital
were reviewed. The hospital's infection control
committee reviewed patient monitoring charts and
nursing care plans completed manually by nurses on
paper. The committee then developed a single nursing
care plan based on the recommendations of
international guidelines (Torres et al., 2018). The new
care plan and related forms were transfered to the
hospital’s HIS so that medical records related to VAP
prevention and care would be digital instead of paper-
based.
During our review of current practice, we found
that some VAP prevention and care activities were
not performed in the unit even though they were
mentioned in the nursing care plan. As such, the
following elements were added to the nursing care
plan: correct hand washing and use of aseptic
technique, continuous control of tracheal cuff
pressure, postural drainage, and endotracheal tube
direction change and level control. Then, the HIS
vendor developed a CDSS application for the HIS
system. The new CDSS was rule-based and triggered
when relevant conditions are met, such as entering
predefined diagnoses or interventions. Our CDSS
was triggered when a nurse indicated on the
respiratory system evaluation screen that a patient had
an endotracheal tube (intubated) placed. The CDSS
responds to this trigger by automatically adding the
necessary care, follow-up, and nursing interventions
to the care plan at appropriate frequencies. The HIS
then prompts the nurses to follow the ventilator care
plan scheduled by the CDSS. The CDSS generated
plan includes the following tasks:
Ventilator Care Plan
1. Deep venous thrombosis and peptic ulcer
prophylaxis
2. Raising the head of the bed
3. Subglottic secretion drainage
4. Cleaning ventilator circuits and preventing
fluid build-up
5. Oral care
6. Extubation readiness assessment
7. Aspiration with aseptic technique
8. Cuff pressure monitorizition
HEALTHINF 2020 - 13th International Conference on Health Informatics
694
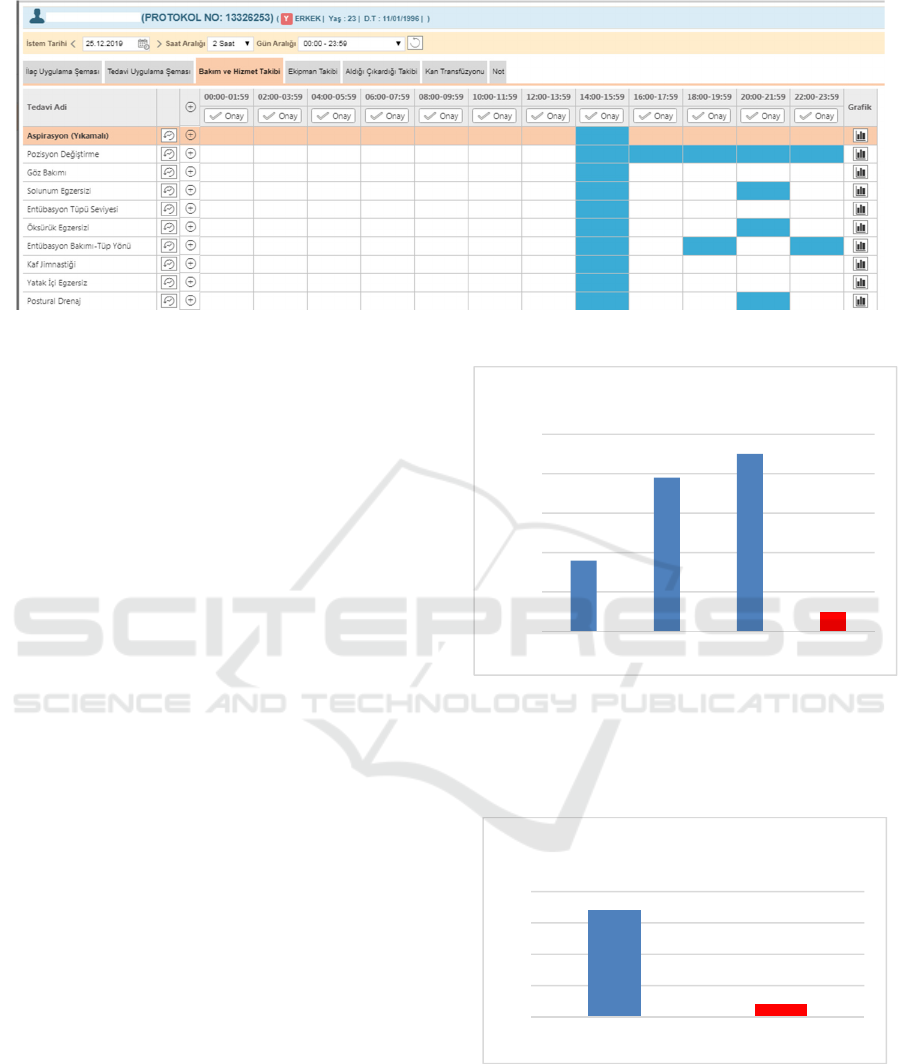
Figure 1: VAP Care scheduling screen on HIS.
Figure 1 shows these tasks added to the nursing
care plan in the HIS work schedule.
In addition to the improvements in nursing care
plans (Klompas et al., 2014), (Resetar et al., 2014), it
is essential to train nurses on the new practices
(Mogyoródi, Dunai, Gál, & Iványi, 2016),
(Pneumonia, 2005). Once the improvement work was
finalized on the HIS, 24 nurses working in the Level
2 ICU received training on the new care plan. After
the nurses were trained and had used the new system
for one complete year (2018), the incidence of VAP,
the number of patients diagnosed with VAP, and the
cost of extra medications related to VAP for 2018
were calculated and compared with the previous
period (2015-17). When calculating the number of
VAP cases, only patients who developed VAP after
admission to the intensive care unit were taken into
account (including the ppatients who were already on
a ventilator when they arrived at the hospital (without
pneumonia), and patients who were already
diagnosed with pneumonia during hospitalization
were excluded. In the calculation of medication costs,
the costs of extra medications (antibiotics, etc.)
administred to the patient due to a VAP diagnosis
were taken into consideration. Costs were extracted
from the hospital’s HIS which is integrated with the
claims submission portal of the national health
insurance system.
3 RESULTS
Following a full year of implementation of the new
nursing care plans triggered by the CDSS, the rate of
new cases diagnosed with VAP decreased from 4.5%
in 2017 to 0.5% in 2018 (Figure 2).
Figure 2: Comparison of VAP Ratio in ICU.
Similarly, the total number of patients diagnosed
with VAP, dropped from 17 in 2017 to 2 in 2018
(Figure 3).
Figure 3: Comparison of the number of VAP incidence.
In our hospital, the cost of extra medication
(antibiotics, etc.) administrered to the patient due to
VAP decreased significantly (90.87%). Accordingly,
the cost of extra medications, which was 855,412
Turkish Lira (≈189,250€) in 2017, decreased to only
78,044 TL (≈12,900€) in 2018 (Figure 4).
1,80%
3,90%
4,50%
0,50%
0,00%
1,00%
2,00%
3,00%
4,00%
5,00%
2015 2016 2017 2018
VAP Ratio
17
2
0
5
10
15
20
2017 2018
#ofVAPIncidence
The Effects of a Nursing Care Plan Incorporated with a Decision Support System on Ventilator Associated Pneumonia: A Case Study
695
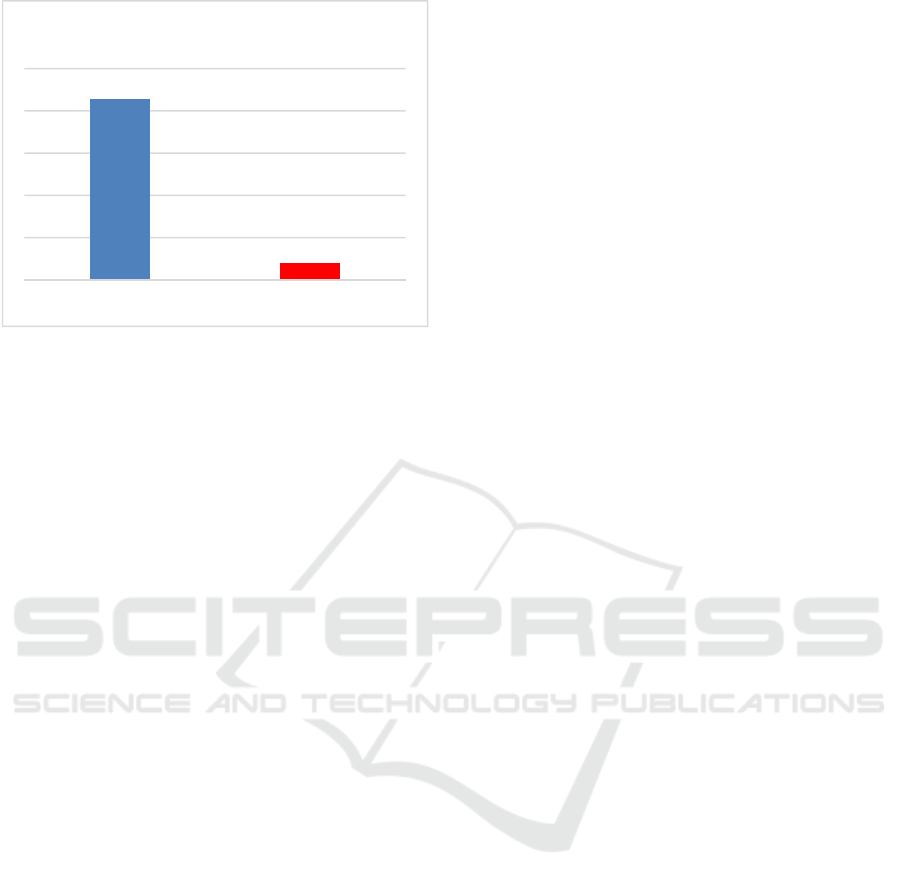
Figure 4: Comparison of extra medication costs related to
VAP.
4 CONCLUSIONS
VAP is associated with high mortality and morbidity
rates and high treatment costs. Managers of intensive
care units can improve the quality and cost of care
through prevention of VAP. This study produced
results consistent with previous studies showing that
the implementation of a comprehensive, evidence-
based, and safe care plan to prevent VAP can
significantly reduce the cost of care. This study also
confirmed that findings of other research showing the
economic benefits of using electronic systems in
patient monitoring and evaluation, early diagnosis,
and documentation are also valid for VAP (Prgomet,
Li, Niazkhani, Georgiou, & Westbrook, 2017),
(Schurink et al., 2007). Many studies reporting the
benefits of CDSSs on improving performance on
healthcare quality indicators (Johnston, Langton,
Haynes, & Mathieu, 1994; Kawamoto, Houlihan,
Balas, & Lobach, 2005). It can be suggested that
instead of implementing nursing interventions
individually, even if they are scientifically proven,
incorporating comprehensive care plans with CDSS
and following the activity plan can contribute to
preventing or reducing infections more efficiently.
Following this study, hospital managers decided to
develop new care plan packages using CDSS for
other care processes.
ACKNOWLEDGMENTS
The authors wish to thank the Chief Medical Officer
of İzmir Tire State Hospital, Dr. Fatih Hayali, for his
valuable support and encouragement during this
study. Care plans are routinely integrated with HIS
programs and used in hospitals throughout Turkey.
No permission was required from any individual or
institution. This research was carried out within the
scope of digital transformation in our hospital and no
financial support was received.
REFERENCES
Alp, E., Kalin, G., Coskun, R., Sungur, M., Guven, M., &
Doganay, M. (2012). Economic burden of ventilator-
associated pneumonia in a developing country. Journal
of Hospital Infection, Vol. 81, pp. 128–130.
https://doi.org/10.1016/j.jhin.2012.03.006
Başyiğit, S. (2017). Clinical pulmonary infection score
(CPIS) as a screening tool in ventilatory associated
pneumonia (VAP). The Medical Bulletin of Sisli
Hospital, 51(2), 133–141. https://doi.org/10.5350/
semb.20170208030528
De Bie, A. J. R., Nan, S., Vermeulen, L. R. E., Van Gorp,
P. M. E., Bouwman, R. A., Bindels, A. J. G. H., &
Korsten, H. H. M. (2017). Intelligent dynamic clinical
checklists improved checklist compliance in the
intensive care unit. British Journal of Anaesthesia,
119(2), 231–238. https://doi.org/10.1093/bja/aex129
Grassie, S. S., & Gevrek, S. Ç. (2016). In our intensive care
unit the experience of the checklist use to prevent
ventilator associated pneumonia. Journal of the Turkish
Society of Intensive Care, 14(April), 13–17.
https://doi.org/10.4274/tybdd.63644
Gutiérrez, J. M. M., Borromeo, A. R., Dueño, A. L.,
Paragas, E. D., Ellasus, R. O., Abalos-Fabia, R. S., …
Domantay, J. A. A. (2019). Clinical epidemiology and
outcomes of ventilator-associated pneumonia in
critically ill adult patients: protocol for a large-scale
systematic review and planned meta-analysis.
Systematic Reviews, 8(1), 1–12. https://doi.org/10.
1186/s13643-019-1080-y
Hayashi, Y., Morisawa, K., Klompas, M., Jones, M.,
Bandeshe, H., Boots, R., … Paterson, D. L. (2013).
Toward improved surveillance: The impact of
ventilator-associated complications on length of stay
and antibiotic use in patients in intensive care units.
Clinical Infectious Diseases, 56(4), 471–477.
https://doi.org/10.1093/cid/cis926
HIMSS Analytics. (2018). Electronic Medical Record
Adoption Model. Retrieved January 2, 2019, from
HIMSS Analytics website:
https://www.himssanalytics.org/emram
Johnston, M. E., Langton, K. B., Haynes, R. B., & Mathieu,
A. (1994). Effects of Computer-based Clinical Decision
Support Systems on Clinician Performance and Patient
Outcome: A Critical Appraisal of Research. Annals of
Internal Medicine, 120(2), 135. https://doi.org/10.
7326/0003-4819-120-2-199401150-00007
Kalil, A. C., Metersky, M. L., Klompas, M., Muscedere, J.,
Sweeney, D. A., Palmer, L. B., … Brozek, J. L. (2016).
IDSA guidelines pneumonias nosocomiais. Clinical
₺855,412
₺78,044
2017 2018
Medication Costs
HEALTHINF 2020 - 13th International Conference on Health Informatics
696

Infectious Diseases, 63(5), 61–111. https://doi.org/10.
1093/cid/ciw353
Kapucu, S., & Ozden, G. (2014). Ventilator associated
pneumonia and nursing care. Journal of Hacettepe
University Faculty of Nursing, 99–110.
Karaoglan, H., Yalcin, A. N., Cengiz, M., Ramazanoglu,
A., Ogunc, D., Erbay, R. H., … Mamikoglu, L. (2010).
Cost analysis of ventilator-associated pneumonia in
Turkish medical-surgical intensive care units. Infez
Med, 18(4), 248–255.
Kawamoto, K., Houlihan, C. a, Balas, E. A., & Lobach, D.
F. (2005). Improving clinical practice using clinical
decision support systems: a systematic review of trials
to identify features critical to success. BMJ (Clinical
Research Ed.), 330(765), 765. https://doi.org/10.1136/
bmj.38398.500764.8F
Klompas, M., & Berra, L. (2016). Should ventilator-
associated events become a quality indicator for ICUs?
Respiratory Care, 61(6), 723–736. https://doi.org/10.
4187/respcare.04548
Klompas, M., Kleinman, K., & Platt, R. (2008).
Development of an algorithm for surveillance of
ventilator-associated pneumonia with electronic data
and comparison of algorithm results with clinician
diagnoses. Infection Control & Hospital Epidemiology,
29(1), 31–37. https://doi.org/10.1086/524332
Klompas, M., & Li, L. (2013). Beyond pneumonia:
Improving care for ventilated patients. The Lancet
Infectious Diseases, Vol. 13, pp. 640–641.
https://doi.org/10.1016/S1473-3099(13)70111-7
Klompas, M., Rrt, R. B., Eichenwald, E. C., Greene, L. R.,
Mps, R. N., Mph, M. D. H., … Eichenwald, E. C.
(2014). Strategies to prevent ventilator-associated
pneumonia in acute care hospitals : 2014 Update.
Infection Control and Hospital Epidemiology, 35(8),
915–936. https://doi.org/10.1086/677144
Klouwenberg, P. M. C. K., Van Mourik, M. S. M., Ong, D.
S. Y., Horn, J., Schultz, M. J., Cremer, O. L., & Bonten,
M. J. M. (2014). Electronic implementation of a novel
surveillance paradigm for ventilator-associated events
feasibility and validation. American Journal of
Respiratory and Critical Care Medicine, 189(8), 947–
955. https://doi.org/10.1164/rccm.201307-1376OC
Liao, Y. H., Wang, Z. C., Zhang, F. G., Abbod, M. F., Shih,
C. H., & Shieh, J. S. (2019). Machine learning methods
applied to predict ventilator-associated pneumonia with
pseudomonas aeruginosa infection via sensor array of
electronic nose in intensive care unit. Sensors
(Switzerland), 19(8), 1–15. https://doi.org/10.3390/
s19081866
Luckraz, H., Manga, N., Senanayake, E. L., Abdelaziz, M.,
Gopal, S., Charman, S. C., … Andronis, L. (2018). Cost
of treating ventilator-associated pneumonia post
cardiac surgery in the National Health Service: Results
from a propensity-matched cohort study. Journal of the
Intensive Care Society, 19(2), 94–100. https://doi.org/
10.1177/1751143717740804
Melsen, W. G., Rovers, M. M., Groenwold, R. H. H.,
Bergmans, D. C. J. J., Camus, C., Bauer, T. T., …
Bonten, M. J. M. (2013). Attributable mortality of
ventilator-associated pneumonia: A meta-analysis of
individual patient data from randomised prevention
studies. The Lancet Infectious Diseases, Vol. 13, pp.
665–671. https://doi.org/10.1016/S1473-3099(13)
70081-1
Mogyoródi, B., Dunai, E., Gál, J., & Iványi, Z. (2016).
Ventilator-associated pneumonia and the importance of
education of ICU nurses on prevention - Preliminary
results. Interventional Medicine and Applied Science,
8(4), 147–151. https://doi.org/10.1556/1646.8.2016.4.9
Neuville, M., Mourvillier, B., Bouadma, L., & Timsit, J.
(2017). Bundle of care decreased ventilator-associated
events — implications for ventilator-associated
pneumonia prevention. Journal of Thoracic Disease,
9(3), 430–433. https://doi.org/10.21037/jtd.2017.02.72
Pneumonia, H. (2005). Guidelines for the Management of
Adults with Hospital-acquired, Ventilator-associated,
and Healthcare-associated Pneumonia. American
Journal of Respiratory and Critical Care Medicine,
171(4), 388–416. https://doi.org/10.1164/rccm.200405
-644ST
Prgomet, M., Li, L., Niazkhani, Z., Georgiou, A., &
Westbrook, J. I. (2017). Impact of commercial
computerized provider order entry (CPOE) and clinical
decision support systems (CDSSs) on medication
errors, length of stay, and mortality in intensive care
units: A systematic review and meta-analysis. Journal
of the American Medical Informatics Association,
24(2), 413–422. https://doi.org/10.1093/jamia/ocw145
Resetar, E., McMullen, K. M., Russo, A. J., Doherty, J. A.,
Gase, K. A., & Woeltje, K. F. (2014). Development,
implementation and use of electronic surveillance for
ventilator-associated events (VAE) in adults. AMIA ...
Annual Symposium Proceedings / AMIA Symposium.
AMIA Symposium, 2014, 1010–1017.
S, Z., H, A., F, Z., AE, B., AA, S., S, N., … A, T. (2017).
Ventilator-associated pneumonia (VAP): Clinical
strategies, treatment challenges and economic
concerns. Journal of Bioequivalence & Bioavailability,
09(04), 432–436. https://doi.org/10.4172/jbb.1000338
Sara, A., Phillips, A., Kaur, P., & Isaac, R. (2015).
Incidence and attributable costs of ventilator-associated
pneumonia ( VAP ) in a tertiary-level intensive care unit
( ICU ) in northern India. Journal of Infection and
Public Health, 8(2), 127–135. https://doi.org/10.1016/j.
jiph.2014.07.005
Schurink, C. A. M., Visscher, S., Lucas, P. J. F., Van
Leeuwen, H. J., Buskens, E., Hoff, R. G., … Bonten,
M. J. M. (2007). A Bayesian decision-support system
for diagnosing ventilator-associated pneumonia.
Intensive Care Medicine, 33(8), 1379–1386.
https://doi.org/10.1007/s00134-007-0728-6
Torres, A., Niederman, M. S., Chastre, J., Ewig, S.,
Fernandez-Vandellos, P., Hanberger, H., …
Wunderink, R. (2017). International ERS/ESICM/
ESCMID/ALAT guidelines for the management of
hospital-acquired pneumonia and ventilator-associated
pneumonia. European Respiratory Journal, 50(3).
https://doi.org/10.1183/ 13993003.00582-2017
The Effects of a Nursing Care Plan Incorporated with a Decision Support System on Ventilator Associated Pneumonia: A Case Study
697

Torres, A., Niederman, M. S., Chastre, J., Ewig, S.,
Fernandez-Vandellos, P., Hanberger, H., …
Wunderink, R. (2018). Summary of the international
clinical guidelines for the management of hospital-
acquired and ventilator-acquired pneumonia. ERJ Open
Research, 4(2), 2–10. https://doi.org/10.1183/
23120541.00028-2018
Wang, Y., Eldridge, N., Metersky, M. L., Verzier, N. R.,
Meehan, T. P., Pandolfi, M. M., … Battles, J. (2014).
National trends in patient safety for four common
conditions, 2005-2011. New England Journal of
Medicine, 370(4), 341–351. https://doi.org/10.
1056/NEJMsa1300991
HEALTHINF 2020 - 13th International Conference on Health Informatics
698
