
Individualized Computer-based Training for Elderly in Nursing
Homes: A Pilot Study
Katja Orlowski, Gina Maria Gräfe, Laura Tetzlaff, Thomas Schrader and Eberhard Beck
Department of Computer Science and Media, University of Applied Sciences Brandenburg,
Magdeburger Str. 50, 14770 Brandenburg, Germany
Keywords: Balance Training, Computer-based Training, Mobility.
Abstract: In older ages, the people are affected by limitations referring to physical and cognitive functions of the body.
These limitations can lead to falls, which can be prevented by different types of physical training. Some
studies showed that different kinds of physical activity have a positive effect on the equilibrium as well as on
cognitive function. During a project an individualized computer-based training was developed. The developed
application was examined during a pilot study in a local nursing home. The results indicate that the training
intervention based on the computer-based training has a positive effect on different parameters (balance, TUG
test). The limitation of the pilot study is the small sample size, which is additionally reduced due to dropouts.
In further studies the effect of a balance training with the computer-based training will be done in other nursing
homes.
1 INTRODUCTION
The ability to keep the human body balanced is a very
complex interaction of different components: the or-
gan of equilibrium of the inner ear, the visual system
as well as the proprioceptors within the joints and
muscles ensure that the body stays upright and bal-
anced. In older ages, limitations of the sensorimotor
functions can lead to dizziness and falls (Buchner et
al., van Doorn et al.) whereby persons affected are en-
dangered to loose the ability to lead a self-determined
and thus independent life. Different studies show that
physical training has a positive effect on the general
fitness, the static and dynamic equilibrium (gait pa-
rameters) (Boa Sorte Silva et al., Hortobágy et al,
Heath et al.) as well as an impact on cognitive perfor-
mance (Huxhold et al., 2008, Didczuneit-Sandhop,
2018).
Persons aged 70 years or older have an increased
risk of getting problems with dizziness. Sixty percent
of women and 50 % of men in that age group suffer
from dizziness (Schaaf et al., 2009). In that those
cases, Schaaf et al. (2009) recommend a periodically
conducted balance training, which has a positive in-
fluence on the equilibrium and leads to prevention of
50 % of the falls.
In this paper, the pilot study including an inven-
tion utilizing an individualized computer-based ba-
lance training is presented. This paper focuses on the
impact of the balance training on the ability to keep
up or even improve the individual balance, which is
considered as static and dynamic balance.
2 MATERIALS & METHODS
The pilot study was conducted in a nursing home in
Brandenburg/Havel, which provides an accommoda-
tion for 14 elderly persons. At the starting point only
12 residents could have participated in the pilot study,
however, two of whom were not able to walk or to
stand independently since they were wheelchair us-
ers. From the remaining ten subjects six (2 m, 4 f,
mean age: 85.3 (± 5.96) years, Karnovski Index 60-
70 %, level of dizziness: 5 no, 1 light to moderate)
were willing to participate in the intervention with the
individualized computer-based training. The remain-
ing four elderly persons (1 m, 3 f, mean age: 88.3
(± 8.49) years, Karnovski Index 60 %, level of dizzi-
ness: 4 no) could be motivated to serve as control
group participating in the pre- and post-intervention
test setting. All participants or their legal representa-
tives gave written consent to participate in this study
after having been informed about the procedure, its
purpose and possible risks related to the participation.
The study was approved by the local ethics committee
664
Orlowski, K., Gräfe, G., Tetzlaff, L., Schrader, T. and Beck, E.
Individualized Computer-based Training for Elderly in Nursing Homes: A Pilot Study.
DOI: 10.5220/0009162106640669
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 664-669
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

of the Brandenburg Medical School Theodor Fontane
and was carried out in line with the Declaration of
Helsinki (no. E-01-20181030).
The training intervention with the computer-based
balance training was planned to last for six weeks
with three training sessions per week. Each training
session was conducted in the same environment of the
nursing home at approximately the same time of the
day. The computer-based balance training requests
the user to move his/her center of gravity (COG)
throughout the training with the result that step by
step a hidden image becomes visible. Additionally,
music plays as long as the user moves his/her center
of pressure. Both factors, utilizing visual and auditive
stimuli, were intended to increase the test persons’
motivation, since it was shown, that the application of
socioemotionally relevant aspects result in an in-
creased effect of the respective intervention (Carsten-
sen, 2003, Mather & Carstensen, 2005).
If the extend of the motion was too small, the
music softens away before it finally stops. In that
case, the user was asked to move his/her COG again.
Figure 1: Setting of the training sessions. The elderly stands
on the force plate, which is surrounded with a safety con-
struction. A coach, nurse or caregiver supervised the elderly
during the training. During playing the elderly sees the
changes made by moving the center of gravity on the screen
and step-by-step the hidden image becomes visible.
As shown in figure 1 the elderly persons were
supervised during the training sessions by a coach
(or a nurse/caregiver).
In order to assess the impact of the balance train-
ing using the individualized computer-based training,
different tests were exerted before and after the inter-
vention. In the pretest scenario all ten test persons
took part and completed the Timed-Up-and-Go (TUG
(Podsiadlo & Richardson, 1991) test and a balance
test. Additionally, different cognitive test, such as the
Mini-Mental-State-Test (MMST (Folstein et al.,
1975)) or Trail-Making-Test (TMT, (Reitan, 1992))
were performed (results not presented).
During the TUG, the time for standing up from the
chair, walking a three meters distance, turning 180°,
going back to the chair and sitting down was regis-
tered using a stop watch. In addition, the performance
of the subject was captured with a video camera in
order to be able to evaluate the gait (dynamic balance)
of the subject.
The static balance test was conducted using a
PLUX force plate (PLUX-Wireless Biosignals S.A,
Lisbon, Portugal (Plux, 2019)) and an in-house devel-
oped software called BALANCE. The balance was
examined under four different conditions:
(1) standing on both feet with a defined distance be-
tween the feet and eyes opened,
(2) standing on both feet with a defined distance be-
tween the feet and eyes closed,
(3) semi-tandem stand with right foot in front, and
(4) semi-tandem stand with left foot in front.
Each standing position was captured for 20 seconds
and the maximum variations of the center of gravity
in the left-right (medio-lateral) as well as theback-
/forwards (anterior-posterior) direction was regis-
tered with the BALANCE software. During the bal-
ance test, a safety construction and if necessary an ex-
aminer supported the test persons in order to avoid
falls (see figure 1). Complementary to the objective
values of the COP variations, the examiners docu-
mented the level of support by using a subjective
scale: without, little, medium or large (great, major)
support.
Due to the small size of the groups (experimental
and control group), the parameters of the tests were
only considered with descriptive methods of statis-
tics. The difference of the values from pre- and post-
test settings were compared.
3 RESULTS
Training Sessions
During the six-week intervention, 18 training ses-
sions were conducted. Table 1 gives an overview on
how many sessions each subject participated in and
Individualized Computer-based Training for Elderly in Nursing Homes: A Pilot Study
665
how long the mean training sessions lasted. While
two subjects took part in almost all training sessions,
one subject missed five training sessions and three
subjects were absent for seven to eight training ses-
sions. Considering the mean time per training session,
three groups were apparent: Three subjects had a
mean session time of twelve or thirteen minutes,
while one subject played the game for seven minutes
on average while the remaining two subjects with the
lowest number of training sessions were also having
the lowest mean session times of one or two minutes.
Consequently, only three subjects were to be consid-
ered as forming the experimental group during the
further analysis.
Table 1: Number of training sessions conducted from the
six subjects during the six-week intervention. Additionally,
the mean session time in minutes is given for each subject.
Subject
Number of training
sessions
Mean session time
(min)
S01 16 13
S02 10 2
S03 11 1
S04 17 12
S05 13 12
S06 10 7
User Feedback
All the participants of the EG were motivated during
the whole intervention and gave a positive oral feed-
back to the caregiver or examiner. Surprisingly the
motivation was maintained and even increased by
changing the music and/or the images weekly as well
as choosing music and images suited to seasonal or
special events during the intervention period. The in-
itial scepticism of the participants regarding the new
and unknown technology changed to a pleasant antic-
ipation of the next training.
Balance Test
For the static balance test two different aspects had to
be considered: On the one hand, the objective meas-
urement of the variations of the COG by means of the
force platform and, on the other hand, the level of in-
dividual support documented subjectively by the ex-
aminer, which provides insight into the (potential)
improvement of physical function during the inter-
vention.
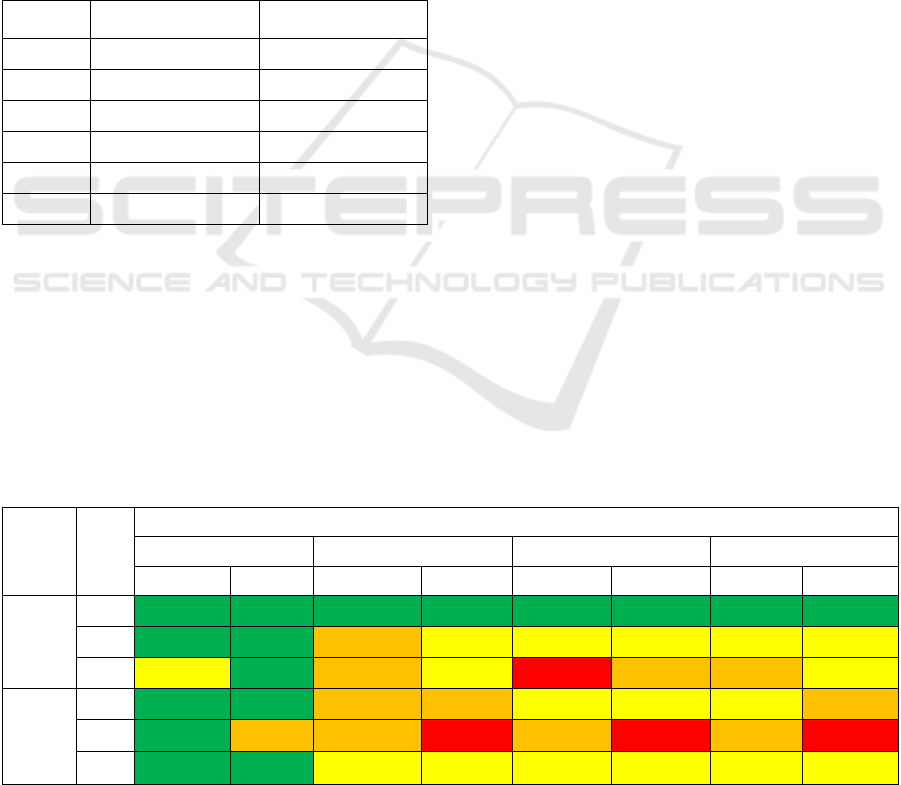
Table 2 shows the level of support of the exam-
ined subjects. The examiner used a scale of four items
to document the level of support. As it is clearly visi-
ble, there is only one subject (S01), who was able to
conduct all test settings without any help and was
standing during all test positions upright and free in
the pre- and post-intervention tests. A second subject
(S03), who could not take part in the post-intervention
test due to general health reasons, also did not need
any support during the pretest. The subjects (S04,
S05) of the EG showed a reduced level of support in
the post-intervention test in one or even all settings.
In all of the other subjects the level of support was
unchanged (S06, S09) or even increased (S07, S08)
in the post-test scenario. Furthermore, it has to be
noted that the subject S08 had to be supported
throughout the three standing positions “closed eyes”,
“tandem left” and “tandem right”. We therefore de-
cided that the data of S08 could not be considered for
further analysis, especially since the TUG test could
also not be conducted.
Table 2: Level of Support (subjective assessment of the examiner) during the static balance test conducted on the force plate
for the four standing positions. The * means that the subject have to cancel the trial before the end of the measurement was
reached.
Group Subject
Level of support
Opened Eyes Closed Eyes Tandem left Tandem right
Pre Post Pre Post Pre Post Pre Post
EG
S01
without without without without without without without without
S04 without without medium little little little little little
S05 little without medium little large medium medium little
CG
S07
without without medium medium little little little medium
S08 without medium medium large medium large medium large*
S09 without without little little little little little little
HEALTHINF 2020 - 13th International Conference on Health Informatics
666

Table 3: Variations of COP in anterior-posterior direction and medio-lateral direction considered as area (in mm) and given
as relative difference between pre- and posttest (in %).
Group Subject
Opened Eyes
Change of the area (%)
Closed Eyes
Change of the area (%)
Tandem left
Change of the area (%)
Tandem right
Change of the area (%)
EG
S01 -41.0 63.3 45.8 49.5
S04 -34.7 -39.9 -85.5 -74.0
S05 -29.4 9.7 4.6 22.9
CG
S07 -11.8 32.4 65.1 51.7
S09 -43.9 12.0 17.1 26.8
Table 4: Time needed for the task of the TUG test presented in time format (mm:ss.msms) for pretest and posttest and as
relative change between pre- and posttest (in %). Additionally, the kind of support used by the subject is given.
Group Subject
TUG time pre
(mm:ss.msms)
TUG time post
(mm:ss.msms)
Relative Change
(%)
Support during
Pre-/Posttest
EG
S01 00:16.33 00:11.27 -31.3 No / No
S04 00:25.00 00:37.53 48.0 Walker / Crutches
S05 01:00.12 00:46.31 -21.7 Walker / Walker
CG
S07 00:35.19 00:32.02 -8.6 Walker / Walker
S09 00:12.45 00:10.15 -15.4 No / No
In table 3 the relative changes between the results
of the pre- and post-intervention tests are given for
the area calculated from the maximum variations of
the COG in anterior-posterior and medio-lateral di-
rection. All analyzed subjects (EG: 3; CG: 2) im-
proved their balance during normal standing with
opened eyes, whereby the balance test rather deterio-
rated in subject S07 (-11.8 %) (range: -43.9 to -29.4
%).
Timed-up and Go Test
For the TUG test the individual time needed is pre-
sented in the table 4. Besides the raw time each sub-
ject needed during the pre- and post-intervention test,
the relative change in time was calculated. The calcu-
lation was based on the rounded time values and is
given as percentage. Additionally, the kind of sup-
port, which was used by each subject, is listed for the
pre- and posttest scenarios. As shown in the column
“relative change”, an improvement can be seen in
four of five subjects (EG: 2 (-31.3% to -21.7 %), CG:
2 (-15.4 % to -8.6 %)). Only the subject S04 needed a
longer time (38 vs 25 sec, deterioration: 48 %) for the
TUG test post-interventional compared to the pretest.
It has to be noted, that with exception of subject S04
all the other subjects used the same means of support
in the pre- and posttest setting.
4 DISCUSSION
As our preliminary results show no generalized con-
clusion can be drawn based on the intervention utiliz-
ing the individualized computer-based training. At
the beginning of the six-week intervention, the exper-
imental group consisted of six subjects. Due to the
fact, that three of these six subjects only attended a
small number of the training session and had a very
low mean training time, they could not be considered
as part of the experimental group in the data analysis
(balance test, TUG test). Consequently, at the end of
the pilot study only the data of three subjects who had
a considerable number of training sessions and mean
duration of the training where analyzed as experi-
mental group. Initially, four subjects were considered
as control group, only two of whom could be included
in the final analysis.
One of the most striking positive effects of the in-
tervention we would attribute to the level of support
provided by the coaches while investigating the bal-
ance. While the level of support given to the subjects
of the EG during the post-intervention test is the same
or even lower compared to the pretest setting, the sub-
jects of the control group needed at least partly more
support in the post-intervention test as compared to
the pretest.
Balance Test
Concerning the results of the balance investigations
(table 3), it can be seen that all subjects show im-
provements in the setting “eyes open”. However, only
one subject of the EG showed also a reduction in the
variation area in all the other settings (“eyes closed”,
“tandem left”, “tandem right”). Small changes in the
Individualized Computer-based Training for Elderly in Nursing Homes: A Pilot Study
667

variation area in the setting “eyes closed” and “tan-
dem left” and a moderate decline (22.9 %) can be ob-
served for a second subject of the EG. Almost the
same results were found in one other subject of the
CG with a moderate decline in the three settings “eyes
closed”, “tandem left”, “tandem right”. All of the
other subjects showed greater declines. Based on the
data of the two subjects of the EG, it has to be at least
considered that the intervention may have a positive
effect on the equilibrium of the subject, which, how-
ever, has to be proven in a larger prospective random-
ized trial.
Timed-up and Go Test
Improvements in the time needed for the TUG test
can be noticed for both groups (EG, CG). For one sub-
ject of the EG a deterioration were registered, which
can be explained with the changed walking support.
While the subject used a walker during the TUG test,
he chose crutches as support during the posttest. It is
assumed that the process of standing up from a chair
is much easier using a walker than using crutches.
Methodological Critique
The main critique is the small group of subjects in-
cluded in the study. The second problem refers to the
kind of support (wheeler, crutches) used by the sub-
ject during the TUG test. In further examinations it
should be noted, that the subject uses the same kind
of support in pre- and posttest. However, in the case
a subject used no support and walks freely in the TUG
test, and needs crutches or a walker in posttest, it
should be realized due to safety aspects.
5 CONCLUSION
Based on the very preliminary results of this pilot
study, we nonetheless feel encouraged to further in-
vestigate the effects of a computer-based balance
training on the physical and cognitive function in el-
derly people with beginning dementia. Due to the low
number of subjects included in the study and the high
rate of dropouts, the informative value remains very
low. Nevertheless, we could gain a lot of experience
conducting the test scenarios with elderly and par-
tially handicapped persons. These experiences will be
integrated in the further development and improve-
ment of the computer-based training. Furthermore,
the tests conducted in the pre- and post-intervention
test settings, will be revised critically and adjusted to
the abilities of the test persons.
ACKNOWLEDGEMENT
The authors thanks the nursing home “Geschwister
Pape GmbH” in Brandenburg/Havel for the possibil-
ity to conduct the pilot study and for all the support
given before, during and after the pilot study. Special
thanks go to the participants of the pilot study taking
part in the weekly training intervention and the other
elderly persons being part of the pilot study as mem-
bers of the control group.
Furthermore, the authors want to thank the bach-
elor student Anne Biermann, who helped to conduct
the study in the nursing home and took very good care
of the residents.
REFERENCES
Boa Sorte Silva NC, Gill DP, Gregory MA, Bocti J (2018).
Multiple-modality exercise and mind-motor training to
improve mobility in older adults: A randomized con-
trolled trial. Experimental Gerontology 103: 17-26.
Buchner DM, Larson EB. (1987). Falls and fractures in pa-
tients with Alzheimer-type dementia. Jama, 257(11),
1492-1495.
Carstensen LL, Fung HH, Charles ST: Socioemotional se-
lectivity theory and the regulation of emotion in the sec-
ond half of life. Motivation an Emotion. (2003), 27 (2),
103-123.
Didczuneit-Sandhop B (2018). Ethikantrag: Entwicklung
eines statischen und dynamischen
Gleichgewichtstrainings zur Verbesserung der
kognitiven Leistungsfähigkeit von Menschen mit
leichter und mittelschwerer Demenz.
Folstein MF, Folstein SE, Mc Mugh PR. "Mini-mental
state": a practical method for grading the cognitive state
of patients for the clinician. J Psychiatr Res (1975)
12:189-198.
Heath M, Shellington E, Titheridge S, Gill DP, Petrella RJ.
(2017). A 24-week multi-modality exercise program
improves executive control in older adults with a self-
reported cognitive complaint: Evidence from the Anti-
saccade Task. J Alzheimers Dis 56: 167-183.
Hortobágyi T, Lesinski M, Gäbler M, VanSweartingen JM,
Malatesta D, Granacher U. (2015). Effects of three
types of exercise interventions on healthy old adults’
gait speed: A systematic review and Meta-Analysis.
Sports Med 45: 1627-1643.
Huxhold O, Schäfer S, Lindenberger U. (2008).
Wechselwirkungen zwischen Sensomotorik und
Kognition im Alter. Zeitschrift für Gerontologie und
Geriatrie. doi:10.1007/s00391_008_0566_3.
Mather M, Carstensen LL: Ageing and motivated cogni-
tion: The positivity effect in attention and memory.
Trends in cognitive sciences. (2005) 9(10), 496-502.
PLUX-Wireless Biosignals, S.A. (2019). Force Platform
Data Sheet. Retrieved August 23, 2019, from
HEALTHINF 2020 - 13th International Conference on Health Informatics
668

https://plux.info/sensors/288-force-platform-8202025
04.html.
Podsiadlo D, Richardson S. The Timed Up & Go": a test of
basic functional mobility for frail elderly person. J Am
Geriatr Soc (1991) 39:142-148.
Reitan, R.M. Trail Making Test. Tucson, AZ: Reitan Neu-
ropsychology Laboratory. (1992).
Schaaf H, Walther LE, Hesse, G.: Was das Gleichgewicht
im Alter verschwinden lassen kann: Betrachtungen
über den klassischen HNO Bereich hinaus. In: HNO
kompakt (2009). http://www.drhschaaf.de/Schaaf-
SchwindelimAlterHNOcompact42009.pdf
Van Doorn C, Gruber‐Baldini A L, Zimmerman S, Richard
Hebel J, Port C L, Baumgarten M, Quinn CC, Taler G,
May C, Magaziner J. and the Epidemiology of Demen-
tia in Nursing Homes Research Group. Dementia as a
risk factor for falls and fall injuries among nursing
home residents. Journal of the American geriatrics so-
ciety. (2003) 51(9), 1213-1218.
Individualized Computer-based Training for Elderly in Nursing Homes: A Pilot Study
669
