
Surgery Recording without Occlusions by Multi-view Surgical Videos
Tomohiro Shimizu
1
, Kei Oishi
1
, Ryo Hachiuma
1 a
, Hiroki Kajita
2
, Yoshihumi Takatsume
2
and Hideo Saito
1 b
1
Faculty of Science and Technology, Keio University, Yokohama, Kanagawa, Japan
2
School of Medicine, Keio University, Shinanomachi, Tokyo, Japan
Keywords:
Camera Scheduling, Dijkstra’s Algorithm, Multi-viewpoint Camera.
Abstract:
Recording surgery is important for sharing various operating techniques. In most surgical rooms, fixed surgical
cameras are already installed, but it is almost impossible to capture the surgical field because of occlusion by
the surgeon’s head and body. In order to capture the surgical field, we propose the installation of multiple
cameras in a surgical lamp system, so that at least one camera can capture the surgical field even when the
surgeon’s head and body occlude other cameras. In this paper, we present a method for automatic viewpoint
switching from multi-view surgical videos, so that the surgical field can always be recorded. We employ a
method for learning-based object detection from videos for automatic evaluation of the surgical field from
multi-view surgical videos. In general, frequent camera switching degrades the video quality of view (QoV).
Therefore, we apply Dijkstra’s algorithm, widely used in the shortest path problem, as an optimization method
for this problem. Our camera scheduling method works so that camera switching is not performed for the
minimum frame we specified, and therefore the surgical field observed in the entire video is maximized.
1 INTRODUCTION
Figure 1: The current surgery room.
Recording surgery is an indispensable task for a va-
riety of reasons, such as education, sharing surgery
technologies/techniques performing case studies of
diseases, and evaluation of the medical treatment, etc.
Video recording is one of the most important ways of
recording surgery, so a number of cameras have been
a
https://orcid.org/0000-0001-8274-3710
b
https://orcid.org/0000-0002-2421-9862
used for recording surgery.
The most important target of video recording is
the surgical field to which medical doctors operate
with medical tools and their hands, such as an abdom-
inal operation and an orthopedic surgery. However,
as shown in Figure 1, recording the surgical field with
the camera is often difficult because there are usually
several medical doctors around the surgical field.
We may be able to use cameras mounted on the
medical doctors head, but the videos captured with
such cameras are always affected by motion blur be-
cause of fast and wide head movements, so the video
is not always useful for recording purposes. It is as-
sumed that camera installed right above the surgical
field is suitable to record it. Therefore we might be
able to put a camera at the best position to capture
the target surgery field, but such cameras will pre-
vent the operation of medical doctor and cannot ac-
tually be installed since a surgical lamp is installed
right above the most surgical field. After all, there is
almost no position where such recording cameras can
be placed for the recording surgery target area in most
of surgery.
Even in such difficult situations regarding the
placement of recording cameras, we turn our attention
to surgical lighting systems, which have multiple light
Shimizu, T., Oishi, K., Hachiuma, R., Kajita, H., Takatsume, Y. and Saito, H.
Surgery Recording without Occlusions by Multi-view Surgical Videos.
DOI: 10.5220/0009158908370844
In Proceedings of the 15th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications (VISIGRAPP 2020) - Volume 5: VISAPP, pages
837-844
ISBN: 978-989-758-402-2; ISSN: 2184-4321
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
837

bulbs for illuminating the surgical field from multiple
directions, so that shadows are reduced. This implies
that at least one of the multiple light will always il-
luminate the surgical field. Therefore, in this study,
we first create a surgical lamp with a camera in which
multiple cameras are attached to the surgical lamp. At
that time, by attaching one camera to the light unit of
the surgical lamp, it is guaranteed that any camera al-
ways captures the surgical field as long as the surgical
field is illuminated. The created surgical lamp had
five light units, so five cameras were attached to the
surgical lamp.
We propose a method to automatically switch the
surgical video of multiple viewpoints taken using the
created surgical lamp. At that time, it is known that
frequent switching of the camera video will reduce
the quality of view (QoV) of the video. Switching
video creation is divided into two processes: scoring
and scheduling.
First, in scoring, segmentation of the surgical field
was performed using the method of Li et al.(Li and
Kitani, 2013) and the ratio of the area other than the
surgical field of each frame was used as the frame
score. After that, in scheduling, we used a graph for
selecting best view, and Dijkstra’s algorithm, usually
used in the shortest path problem, was applied. In the
graph generation for scheduling, each frame is a node,
and we changed the edge connection between when
the camera sequence was switched and when it was
not switched. The obtained score was used as the edge
weight. By optimizing this graph using Dijkstra’s al-
gorithm, camera switching is not performed for the
minimum frame we specified, and camera scheduling
is performed to maximize the area of the surgical field
observed in the entire video.
In the experiment, the effectiveness of the pro-
posed method is verified by automatic switching
of multiple cameras. This system was installed at
Keio University School of Medicine and surgery was
recorded. A camera switching video was created from
the captured video and it is confirmed that the surgical
field can be observed throughout the surgery. After
that, we conducted a questionnaire on viewing qual-
ity to 14 active doctors using camera switching videos
and video shot with one camera, and verified the mini-
mum number of frames with the highest viewing qual-
ity.
Our contributions are as follows:
1. We present a novel surgery recording system in
which multiple cameras are attached to the surgi-
cal lamp.
2. We propose a method which switches multi-view
videos considering QoV using Dijkstra’ algo-
rithm.
3. Qualitative evaluation shows that the video cre-
ated by our method does not select the occluded
frame while keeping the QoV. Moreover, the user
test of the doctors on the quality of the switching
video quantitatively verify the effectiveness of our
proposed method.
The rest of the paper is organized as follows: we
first present related work in Section 2. Next, we
present details of surgical recording systems in Sec-
tion 3 and our proposed method in Section 4. We then
conduct experiments on creating switching video to
validate our method. At the School of Medicine in our
university, we recorded multi-view surgical videos
with multiple cameras mounted on the surgical lamp.
Then, we presented our experiment, results and dis-
cussions in Section 5. Last, we conclude this paper in
Section 6.
2 RELATED WORK
In this paper, we present a new surgery recording sys-
tem using multiple cameras attached to the surgical
lamp. In Section 2.1, we introduce the conventional
surgical recording systems. In addition, we proposed
a novel camera switching method to automatically se-
lect the best view. In Section 2.2, we introduce the
conventional camera switching method to clarify the
novelty of the proposed method.
2.1 Surgical Recording Systems
As doctors have a duty to teach their surgical skills
to future generations, it is important to record the
surgery and generate video for trainees. Moreover,
the usefulness of surgery recording has been recog-
nized in terms of reviewing. The surgery, such as la-
paroscopic surgery, which is performed through the
endoscope camera can be easily recorded. However,
the surgery that the doctor directly sees, such as the
surgery that involves dissection, it is difficult to record
due to the presence of the surgeon and spatial restric-
tions.
Kumar et al.(Kumar and Pal, 2004) designed a
camera arm system with a camera mounted on the arm
to record the surgery. The camera arm is set to the po-
sition that does not get occluded by the doctor and is
often set to the position far from the surgical field. In
addition, it is troublesome to position the camera ac-
cording to the surgical situation and the environment.
Therefore, Byrd et al.(Byrd et al., 2003) presented a
system of mounting a camera on the surgical lamp.
However, the view is occluded by the doctor’s head
VISAPP 2020 - 15th International Conference on Computer Vision Theory and Applications
838

or body and it is difficult to observe the surgical field
with a single camera constantly.
Other attempts have also been made to record
surgery with a surgical field camera placed between
the eyes of a doctor. The camera of such recording
systems were not high resolution and did not pro-
duce good video quality (Matsumoto et al., 2013;
Murala et al., 2010) because of the limited hardware
system. In addition, doctors had to perform surgery
with interference by the surgical camera itself and
its code. Nair et al.(Nair et al., 2015) recorded the
surgery by putting a high-resolution camera (GoPro
Hero 4) on the doctor’s head. The doctor’s head
moves greatly during the surgery, and camera cannot
always shoot the surgical fields, and video is always
shaking. Therefore, video recorded by it can be of-
fending for viewers.
In our proposed system, multiple cameras are at-
tached to multiple lights mounted the surgical lamp,
and the surgery is recorded by them. While one of the
lights illuminates the surgical field, we assume that
the surgical field can be observed one of the attached
cameras. Therefore, the surgical field is recorded
without disturbing the surgery.
2.2 Multiple Camera Switching
In recent years, multiple cameras are introduced in
any place, such as office environments, sports stadi-
ums, and downtown areas. Instead of its convenience,
it is difficult to extract only the necessary information
from the huge amount of video sequences from a lot
of cameras. Therefore, camera self-control technol-
ogy, such as the automatic viewpoint switching video
generation, and highlight video generation technol-
ogy, are regarded as important issues (Chen and Carr,
2014).
Liu et al.(Liu et al., 2001) interviewed pro editors
to gain knowledge of video editing, and implemented
the camera switching rules. Based on the rules, they
switched the viewpoint of three cameras shooting the
speaker, the audience, and the entire in conference
video. Doubek et al.(Doubek et al., 2004) observed
moving objects using multiple fixed cameras in an
office environment. Selection of a camera was per-
formed based on the score of each camera, and the re-
sistance coefficient was introduced so that the switch-
ing of a camera may be performed only when the
score changed significantly. However, such camera
switching strategies may occur frequently if cameras
with competing scores existed, which may reduce the
overall QoV.
In order to suppress camera switching frequency,
Jiang et al.(Jiang et al., 2008) proposed a cost func-
tion calculated based on the size, posture, orientation,
etc. of the target, and controlled the frequency of the
camera switching while considering QoV. Daniyal et
al.(Daniyal and Cavallaro, 2011) calculated the visi-
bility score of an object using a multivariate Gaussian
distribution model, and used the partial observation
Markov decision process for the camera switching to
maximize the visibility score while suppressing the
camera switching frequency. Although these methods
selected the optimal view using past sequential infor-
mation, the switching should be conducted using not
only past but also future information. Compared to
the conventional switching method, our method uses
both past and future frames to switch cameras so that
a higher QoV can be generated.
Also, QoV and user-specified weights for camera
switching may change depending on the target scene,
because they detected the event for calculating QoV.
For that reason, the hyper-parameter of the method
which determines camera switching depends on the
surgical scene, and it is difficult for non experts to de-
termine. On the other hand, in the proposed method,
since the minimum frame during that camera switch-
ing does not perform is specified and optimization is
performed for the entire frame, the camera switching
frequency does not change depending on the target
surgery scene.
3 MULTI-CAMERA RECORDING
As shown in Figure 2, we attached multiple cam-
eras to multiple lights mounted the surgical lamp.
Thereby, as long as the surgical field is illuminated
by one of the lights, our proposed camera recording
system shoots the surgical field. Compared to the
previous camera recording system (Matsumoto et al.,
2013) which attached cameras to the doctor’s head,
our system does not bother the doctors during surgery
while maintaining visibility of the surgical field.
4 PROPOSED METHOD
Figure 3 shows the overview of the proposed method
which consists of two components: camera scoring
and camera switching. The multiple surgical videos
are captured from the our capturing system (Section
3). To switch between camera sequences to generate
the best video quality, the frame in each sequence has
to be scored. The score represents how the surgical
field can be seen in the image. In our methods, first,
the score is estimated against each frame in each se-
quence. Next, the frame is selected sequentially using
the score.
Surgery Recording without Occlusions by Multi-view Surgical Videos
839

Figure 2: Multiple cameras mounted the surgical lamp.
Figure 3: The overview of the proposed method.
4.1 Camera Scoring
To generate a single video from videos recorded by
multiple cameras, the frame captured from each cam-
era sequence is scored which represents how the sur-
gical field can be seen. The score is used as the
switching criterion. In the proposed method, after
segmenting the surgical field, the camera is scored
based on the number of pixels of the segmentation
mask. The segmentator F that performs segmentation
of the surgical field is defined as follows:
F(I(i, j)) =
(
1 surgical f ield
0 otherwise
(1)
Here, I denotes the input RGB image, and (i, j) is the
pixel coordinate in I.
In this paper, we chose the method proposed by Li
et al.(Li and Kitani, 2013) as the segmentator F. They
used hand color and texture information for learning,
and performed hand segmentation from the learning
model. The surgical field changes shape over time,
and it is difficult to keep detecting it. However, the
area other than the surgical field is covered with cloth
and the color contrast between the surgical field and
other parts is large. Moreover, although their method
is often difficult to detect the target due to environ-
mental changes and high contrast shadows, the sur-
Figure 4: The segmentation result of the surgical field;
(left): input; (right): output.
gical field is always illuminated, and the surgery is
always performed in the surgical room. Therefore,
their method, which was performed only from color
and texture information, is well suited to detect surgi-
cal fields. Figure 4 shows the segmentation result of
the surgical field.
In the proposed method, the score is a ratio of
non segmented pixels in the image I. A score s
c
t
at
timestep t of a camera c is defined as follows:
s
c
t
= 1 −
∑
w
i
∑
h
j
F(I
c
t
(i, j))
wh
, (2)
where w and h are the width and height of the image
I
c
t
. The point is, the larger the area of the surgical field
is, the smaller the score is.
4.2 Camera Switching
The simple approach to achieve camera switching is
taking the minimum score at every timestep. How-
ever, this approach does not consider the scores at the
previous/next frames so that the selected camera may
change over and over during the sequence; the QoV
of video will be decreased.
Hence, the camera switching should be considered
using previous/next frames. In the proposed method,
the scores of all camera sequence were calculated in
advance. Then, the switching video is generated so
that the sum of the scores of the selected sequences
was minimized. However, as above, frequent cam-
era switching occurs in this approach. For this rea-
son, video sequence is selected by using a graph so
that camera switching is suppressed. We changed the
edge connection between when the camera sequence
was switched and when it was not switched. Then, by
optimizing so that the score is minimized throughout
the graph, we created the video sequence in which
camera switching is suppressed. Therefore, we pro-
pose a combined optimization method that applies to
Dijkstra’s algorithm (Ahuja et al., 1990).
4.2.1 Graph Generation
In the proposed method, the edge connection was
changed between when the camera sequences was
VISAPP 2020 - 15th International Conference on Computer Vision Theory and Applications
840
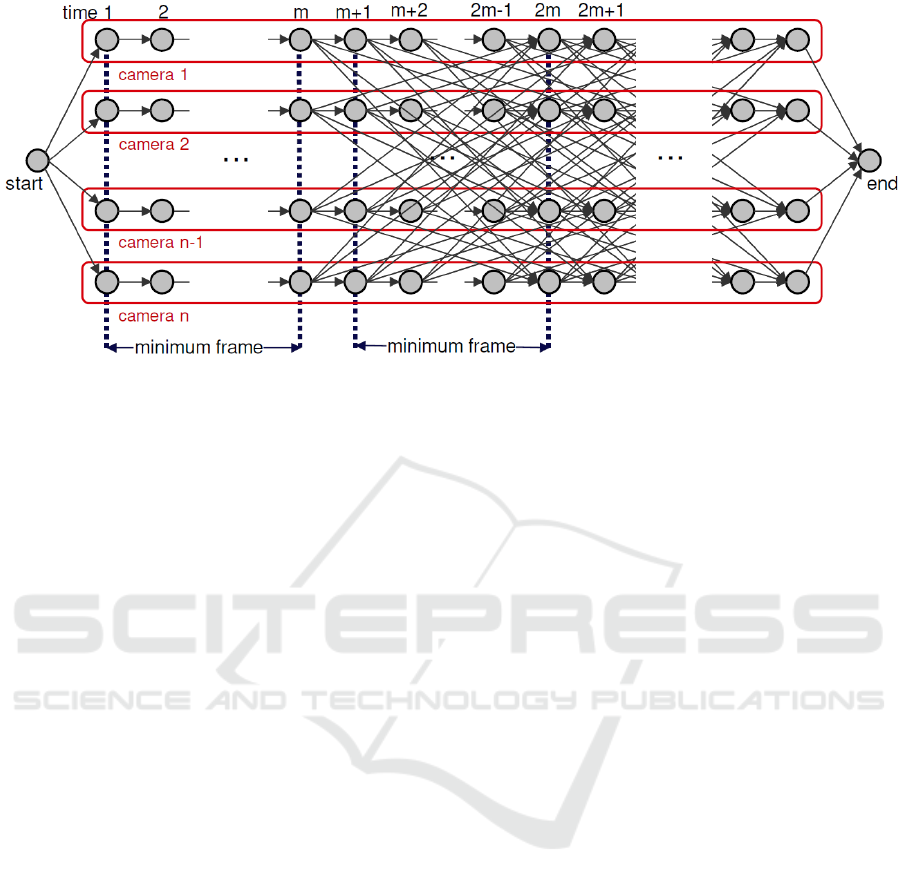
Figure 5: The expected result of generating graph.
switched and when it was not switched. Figure 5
shows the expected graph generation results. Each
node V
c,t
has information on camera number c and
the timestep t. It determines whether or not to con-
nect edges between nodes, and its weight. Between
each node, if the edge E is connected to the node of
the same camera sequence, it is connected to the next
node. On the other hand, if it is connected to the node
of the different camera sequence, it is connected to the
node ahead of the minimum number of frames. Each
edge E is defined as follows:
E(V
c1,t1
, V
c2,t2
) =
1 (V
c1,t1
= start)
∪((c
1
= c
2
) ∩ (t
1
+ 1 = t
2
))
∪((c
1
6= c
2
) ∩ (t
1
+ m = t
2
)
∩(t
2
≤ 2m))
∪(V
c2,t2
= end)
0 otherwise
(3)
m is the minimum number of frames specified by
the user, and E(V
c1,t1
, V
c2,t2
) denotes the edge that
connects between node V
c1,t1
and node V
c1,t1
. Edges
are connected when E = 1.
At this time, the weight W of edge E is defined as
follows:
W (E(V
c1,t1
, V
c2,t2
)) =
1 (V
c1,t1
= start)
∪((c
1
= c
2
)
∩((t
1
+ 1 = t
2
)
∑
i=t
2
i=t
1
+1
s
c
2
i
((c
1
6= c
2
) ∩ (t
1
+ m = t
2
)
∪(t
2
≤ 2m))
0 V
c2,t2
= end
(4)
4.2.2 Optimization
We apply Dijkstra’s algorithm to the graph generated
in Section 4.2.1. Dijkstra’s algorithm is the search
algorithm for solving the single-source shortest path
problem when the weight of the edge in graph is non-
negative.
In the proposed method, the camera number ar-
ray is obtained by acquiring the information of the
nodes, excluding the start and end nodes, after op-
timization by Dijkstra’s algorithm. However, since
there are edges connected to the node ahead of the
minimum number of frames, the array is smaller than
the number of frames of the actual video. Therefore,
at the position where the camera number in the array
has changed, the skipped camera number is added to
the array.
5 EXPERIMENTS
In this section, we describe the details of the experi-
ments we conducted to verify the effectiveness of the
proposed method. At the School of Medicine in our
university, we verified the effectiveness of the pro-
posed method using multi-view surgical videos shot
with multiple cameras mounted on the surgical lamp.
We introduced our surgical lamp system in the actual
surgery of jaws, and we recorded surgery by using it.
5.1 Example Result of Automatic
Camera Switching
We set five cameras on the surgical lamp and per-
formed experiments using a surgical image of the jaw.
The images are shown in Figure 6. Each row shows
Surgery Recording without Occlusions by Multi-view Surgical Videos
841
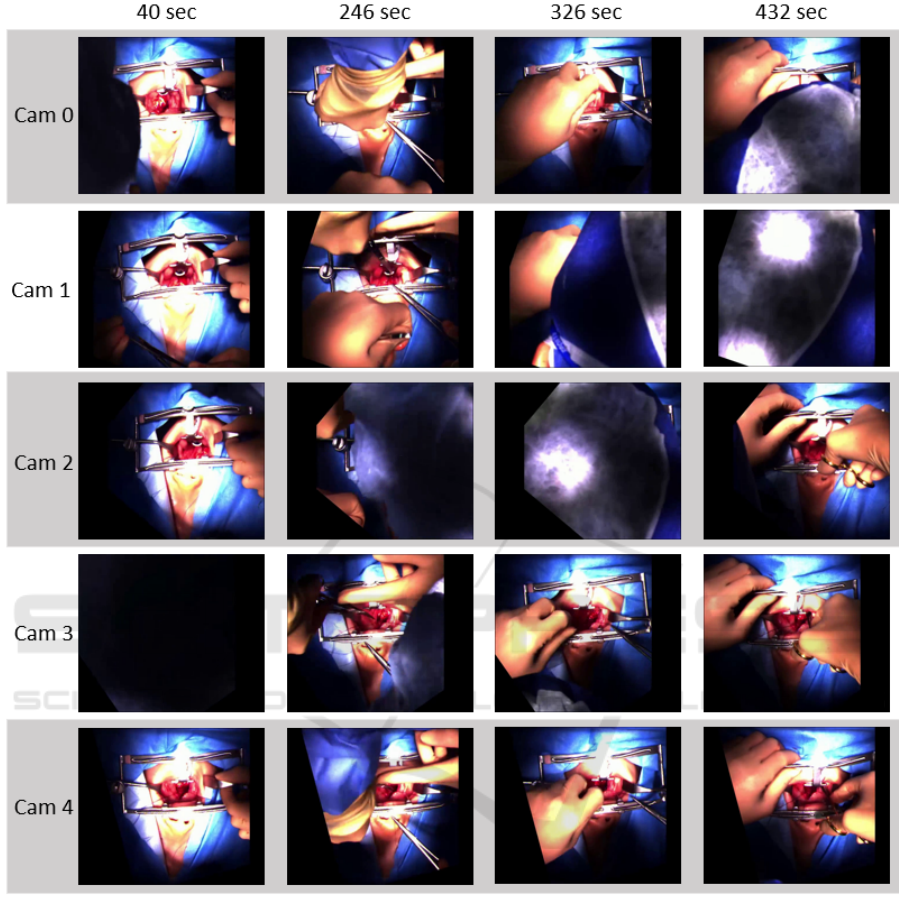
Figure 6: Images recorded by the multiple cameras mounted the surgical lamp.
the images captured by each camera, each column
shows the timestamp.
In Figure 6, it can be seen that at least one cam-
era always captures the surgical field. The segmen-
tator was trained using about 100 images randomly
extracted from the videos. We manually annotate the
surgical field. In the experiment, we set the minimum
frame to one second.
The generated videos are shown in Figure 7. In
Figure 7 (a), the surgical field cannot be observed due
to the occlusion of the head, etc., in the image ob-
tained from one camera. On the other hand, in Figure
7 (b), the video created by our proposed method was
the video with diminishing occlusion.
As seen from the upper graph in Figure 8, when
the camera switching is not scheduled, it is frequently
performed. However, when the proposed method is
applied, it can be seen that the camera switching is
suppressed.
As shown in the lower graph, even when cam-
era switching is suppressed, the score of the selected
camera is almost the same as before the suppression.
Therefore, we can say that QoV was improved while
the observation of the surgery was maintained.
VISAPP 2020 - 15th International Conference on Computer Vision Theory and Applications
842
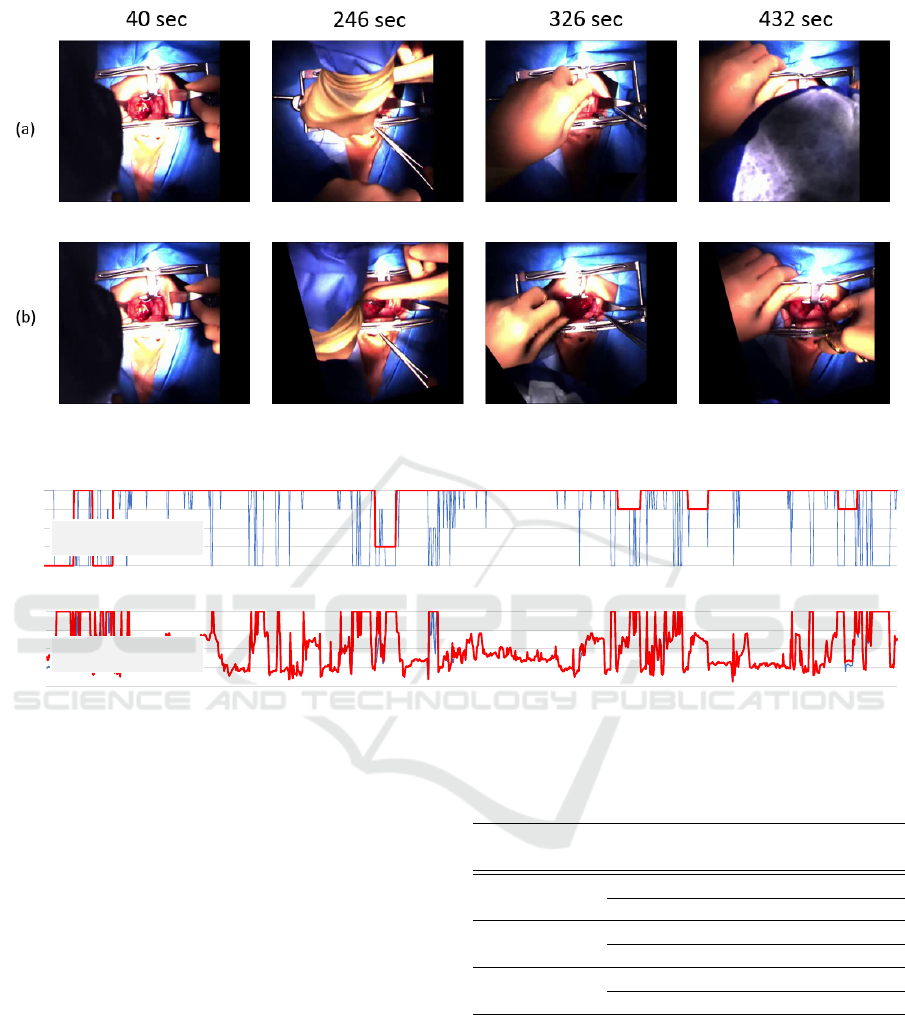
Figure 7: Comparison between a video taken with one camera and a video created by the proposed method; a: images of each
time of the video taken with one camera; b: images of each time of the video created by the proposed method.
0.96
0.97
0.98
0.99
1
236 240 243 246 250 253 256 260 263 266 270 273 276 280
Negative Region
time [sec]
0
1
2
3
4
236 240 243 246 250 253 256 260 263 266 270 273 276 280
camera num
time [sec]
- No scheduling
- Minimum time 1 sec
- No scheduling
- Minimum time 1 sec
Figure 8: Camera switching and scoring results; (upper graph): the result of the camera switching; (lower graph): the result
of camera scoring.
5.2 Assessment of Switching Video by
Medical Doctors
We asked 13 doctors about the usefulness of the cre-
ated video. Three videos of one camera, no schedule,
and the proposed method were shown, and we asked
two questions (Q1: whether switching cameras is not
bothersome, Q2: whether it is possible to recognize
the surgical operation.). Their responses were col-
lected on a five-stage scale. (1: Strongly disagree, 2:
Disagree, 3: Neither agree nor disagree, 4: Agree, 5:
Strongly agree). Responses of Q1 and Q2 are shown
in Table 1.
As a result, it can be seen that the recognition rate
of the surgical operation is improved compared to us-
ing one camera from the result of Q2, and the QoV is
improved compared to the video without scheduling
from the result of Q1.
In addition to the assessment by doctors, we eval-
uated the performance of the automatic switching
Table 1: The result of questionnaire.
video question average
standard
deviation
one camera
Q1 4.23 0.80
Q2 1.69 0.91
without
scheduling
Q1 1.38 0.49
Q2 3.08 1.00
proposed
method
Q1 3.77 0.80
Q2 4.15 0.77
video by checking if each selected frame captures the
target surgery region or not by actually watching the
video. According to the visual examination, we have
confirmed that the ratio of missing the target region is
less than 5 %.
Surgery Recording without Occlusions by Multi-view Surgical Videos
843

6 CONCLUSION
In the proposed method, multiple cameras were in-
stalled corresponding to the multiple light sources
provided for the surgical lamp, and it became possi-
ble to switch the camera and record the operation au-
tomatically while diminishing the doctor’s head and
body. As a result, doctors can record surgery with-
out being aware of the presence of a camera during
surgery. In addition, we experimented with the pro-
posed method and evaluated its usefulness. In the fu-
ture, we would like to switch the multi-view videos
without determining the minimum frame manually,
and to generate camera switching video more in ac-
cordance with the preference of the doctor.
ACKNOWLEDGEMENT
This research was funded by AMED research
expenses (task number JP18he1902002h0001),
JSTCREST (JPMJCR14E1, JPMJCR14E3), and
Saitama Prefecture Leading-edge Industry Design
Project.
REFERENCES
Ahuja, R. K., Mehlhorn, K., Orlin, J., and Tarjan, R. E.
(1990). Faster algorithms for the shortest path prob-
lem. Journal of the ACM (JACM), 37(2):213–223.
Byrd, R. J., Ujjin, V. M., Kongchan, S. S., and Reed, H. D.
(2003). Surgical lighting system with integrated digi-
tal video camera. US Patent 6,633,328.
Chen, J. and Carr, P. (2014). Autonomous camera systems:
A survey. In Workshops at the Twenty-Eighth AAAI
Conference on Artificial Intelligence.
Daniyal, F. and Cavallaro, A. (2011). Multi-camera
scheduling for video production. In 2011 Conference
for Visual Media Production, pages 11–20. IEEE.
Doubek, P., Geys, I., Svoboda, T., and Van Gool, L.
(2004). Cinematographic rules applied to a camera
network. In Omnivis2004: The fifth Workshop on
Omnidirectional Vision, Camera Networks and Non-
Classical Cameras, pages 17–29. Prague, Czech Re-
public: Czech Technical University.
Jiang, H., Fels, S., and Little, J. J. (2008). Optimizing mul-
tiple object tracking and best view video synthesis.
IEEE Transactions on Multimedia, 10(6):997–1012.
Kumar, A. S. and Pal, H. (2004). Digital video recording of
cardiac surgical procedures. The Annals of thoracic
surgery, 77(3):1063–1065.
Li, C. and Kitani, K. M. (2013). Pixel-level hand detec-
tion in ego-centric videos. In Proceedings of the IEEE
Conference on Computer Vision and Pattern Recogni-
tion, pages 3570–3577.
Liu, Q., Rui, Y., Gupta, A., and Cadiz, J. J. (2001). Au-
tomating camera management for lecture room envi-
ronments. In Proceedings of the SIGCHI conference
on Human factors in computing systems, pages 442–
449. ACM.
Matsumoto, S., Sekine, K., Yamazaki, M., Funabiki, T.,
Orita, T., Shimizu, M., and Kitano, M. (2013). Digital
video recording in trauma surgery using commercially
available equipment. Scandinavian journal of trauma,
resuscitation and emergency medicine, 21(1):27.
Murala, J. S., Singappuli, K., Swain, S. K., and Nunn, G. R.
(2010). Digital video recording of congenital heart
operations with surgical eye. The Annals of thoracic
surgery, 90(4):1377–1378.
Nair, A. G., Kamal, S., Dave, T. V., Mishra, K., Reddy,
H. S., Della Rocca, D., Della Rocca, R. C., Andron,
A., and Jain, V. (2015). Surgeon point-of-view record-
ing: using a high-definition head-mounted video cam-
era in the operating room. Indian journal of ophthal-
mology, 63(10):771.
VISAPP 2020 - 15th International Conference on Computer Vision Theory and Applications
844
