
Smart Community Health: A Comprehensive Community Resource
Recommendation Platform
Mehdi Mekni
1
and David Haynes
2
1
Department of Computer Science & Information Technology, St. Cloud State University, St. Cloud, MN, U.S.A.
2
Institute for Health Informatics, University of Minnesota, Minneapolis, MN, U.S.A.
Keywords:
Social Determinants of Health, Informatics, Mobile Application Development, Software Engineering.
Abstract:
Health disparities and inequities are explained by the conditions of places where people live, learn, work and
play. In fact, the health of an individual is partially related to access and quality of health care and mainly
associated to his behaviours, socioeconomic conditions and other community related factors that are often
challenging to address by health care organizations. To meet the need for information about local social
services organizations and the ability to offer resource referrals, a number of platforms have been proposed
that provide electronic social resource directories and facilitate referrals to social service agencies. However,
these platforms show limitations with regards to their dependancy to health care organizations, application
portability, service availability, and user engaging interactions such as tracking, monitoring and notification.
Moreover, existing social resource referral platforms suffer from a fragmentation of services and a discon-
nection between individuals in need and service providers. In this paper, we introduce Smart Community
Health (SCH), a novel independent platform that prioritizes connecting people in need with local community
resources. SCH is a full-service, end-to-end community service provider recommendation platform designed
to help address pressing social, environmental, and health needs within our communities. The platform is
composed of a mobile application for individuals looking for services and a web application dashboard for the
management of community service providers and health care organizations.
1 INTRODUCTION
The Social Determinants of Health (SDOH), defined
as conditions of places where people live, learn, work
and play, are known to affect health. SDOH explain,
in part, why health disparities and health inequities
exist (McGowan et al., 2019). In fact, only 20 percent
of what influences the health of a group of patients
is related to access and quality of health care. The
other 80 percent—commonly known as the social de-
terminants of health—is found in patients’ behaviors,
socioeconomic conditions and other factors that are
often challenging to address in clinical visits (Smith
et al., 2019). For patients and families with complex
health issues (e.g., chronic disease, substance abuse,
mental health issues), effectively managing care is in-
creasingly complex (Koh et al., 2011).
Racial and ethnic minorities—populations who
are more likely to be poor, have lower educational lev-
els, or both—are fundamentally at greater risk of ill
health than their non-minority, non-poor, better edu-
cated peers (Smith et al., 2007). Multiple factors, both
within and outside the health care delivery system,
probably explain these disparities. Health care and so-
cial factors associated with such disparities relate di-
rectly to access to care, and access to care is important
because it is believed to lead to better health (Lurie
and Dubowitz, 2007). It is widely acknowledged that
addressing social risk factors is crucial when comes
the time to improve care quality and reduce costs, par-
ticularly for low-income patients.
The health care sector’s interest in addressing pa-
tients’ social and economic needs has grown dra-
matically over the past few years (Cartier et al.,
2019). For example, health care organizations are
interested in diminishing food insecurity to im-
prove outcomes for patients with diabetes and other
nutrition-related chronic diseases (Gundersen and Zil-
iak, 2015). Moreover, they are showing curiosity
in reducing housing insecurity and homelessness to
lower health care utilization among high-frequency
users of emergency health care services (Kushel et al.,
2006). In addition, they are engaging in improving
access to transportation as a way to reduce no-show
614
Mekni, M. and Haynes, D.
Smart Community Health: A Comprehensive Community Resource Recommendation Platform.
DOI: 10.5220/0009118306140624
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 614-624
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

rates and to improve specialty care access (Molfenter,
2013).
Health care organizations are also particularly in-
terested in referring their patients to local community-
based social service providers that can assist with
non-medical needs (Cartier et al., 2019).
For example, health care staff may want to refer
patients to food banks, benefits enrolment programs,
emergency housing services, or multi-need social ser-
vice agencies, depending on the patients’ social risks.
The health care sector have traditionally relied on in-
formal approaches such as hard-copy or electronic
lists of local or community service providers or the
experiential knowledge of social or community health
workers to determine where to refer patients for non-
medical needs. Community service providers’ listings
are rarely kept up-to-date and are not always available
organization-wide. Furthermore, ad hoc approaches
do not enable efficient tracking of referral outcomes,
which is increasingly a need as health care organiza-
tions seek to systematically address patients’ social
risk factors and assess the impacts of these activities.
As health care organizations’ interest in addressing
patients’ social risks has grown however, many have
found these informal approaches insufficient and in-
efficient to effectively facilitate systematic social risk
referrals.
To meet the health care sector’s need for infor-
mation about local social services organizations and
the ability to make electronic referrals, a number
of new technology platforms that provide electronic
community resource directories and facilitate refer-
rals to social service agencies. However, these tech-
nology platforms show several critical limitations.
First, these platforms use web technology and do not
use the valuable advantages of mobile applications
(Han Rebekah Wong, 2012). These advantages in-
clude a better response time, a better service avail-
ability (off-line and on-line), a full exploitation of the
mobile device resources (i.e. camera and localization
services). Moreover, mobile applications enable push
notifications, instant updates and interactive engage-
ment to name a few. Second, these platforms rely on
key words or labels to search social service providers
directory ignoring two key factors: needs and loca-
tions. The social service referrals suggested by exist-
ing technology platforms suffer from a fragmentation
of services and a disconnect between individuals in
need and service providers. Finally, the coordination
between health care organizations or social services
agencies in one side and the patient in the other side
is systematically not supported in existing service re-
source referral platforms.
In this paper, we present Smart Community
Health (SCH), an end-to-end platform that exists out-
side the domain of any organization. SCH prioritizes
connecting people in need with local community re-
sources. Smart Community Health is a full-service,
end-to-end community service provider recommen-
dation platform designed to help address pressing so-
cial, environmental, and health needs within our com-
munities.
The paper is organized as follows. In Section 2,
we provide an overview of existing resource referral
systems. We highlight our motivations to use mo-
bile application technology and more precisely mo-
bile applications over web-based applications to em-
phasize the portability of our platform. We also of-
fer a comprehensive technical discussion of the intro-
duced existing resource referral systems from a soft-
ware functional and non-functional requirements per-
spective. Next, in Section 3, we detail the requirement
engineering, the software architecture along with an
overview of the two main components of our Smart
Community Health platform: the mobile application
and the web application dashboard. Finally, in Sec-
tion 4, we conclude this paper with a synthesis of the
main contributions and we share the key elements of
our future work.
2 RELATED WORK
In this section, we first provide a short overview on
existing local resource referral platforms. Second, we
highlight our motivations behind choosing mobile ap-
plication development over web technology. Finally,
we provide a discussion that summarizes the main
findings and outline the key functionalities that are
needed in a comprehensive, independent, end-to-end
community resource recommendation platform.
2.1 Overview on Community Resource
Referral Systems
Nine platforms currently dominate the field of com-
munity resource referral services; Aunt Bertha (Aunt,
2019), CharityTracker (Charity, 2019), CrossTx
(Cross, 2019), Healthify (Healthify, 2019), NowPow
(Now, 2019), One Degree (One Degree, 2019), Pieces
Iris (Pieces Iris, 2019), TAVConnect (TAVHealth)
(TAVHealth, 2019) and Unite Us (Unite Us, 2019).
Cartier et al. studied the existing resource referral
technology platforms and provided a comprehensive
guide for health care organizations (Cartier et al.,
2019). Authors in (Cartier et al., 2019) have iden-
tified four groups of such technology platforms; (1)
Smart Community Health: A Comprehensive Community Resource Recommendation Platform
615

Platforms designed for health care-centred social ser-
vice referrals; (2) Platforms designed for health care-
coordination; (3) Platforms designed for individual
social service referrals; and (4) Platforms designed
for health care professionals.
Healthify, NowPow, and Pieces Iris were devel-
oped specifically for health care sector users for
the purpose of fostering referrals to social services
organizations as part of efforts to improve health
by addressing patients’ social needs. As a result,
they have a strong focus on providing comprehen-
sive community-wide resource directories and refer-
ral management. CrossTx and TAVConnect were also
originally developed specifically for health care users
but with a greater focus on care coordination and less
on the resource directory, though TAV- Connect has
recently shifted its focus to become a tool primarily
for social service organizations.
In contrast, Aunt Bertha, CharityTracker, One De-
gree, and Unite Us were not originally developed for
health care users. Therefore, they tend to emphasize
a community collaboration or patient-focused model
of platform implementation rather than a health-care
centric approach. Aunt Bertha and One Degree are
the only platforms developed to be used by individ-
uals seeking help for themselves; they are the only
two that offer a free public-facing online community
resource directory that is accessible without logging
in. CharityTracker and Unite Us were both originally
developed for use by social service organizations and
approach referral management more from a commu-
nity perspective than from a health-care organization
perspective. For instance, CharityTracker is the only
platform that provides the ability to have unstructured
back and forth conversations with a number of orga-
nizations through its bulletin board feature. Unite Us
stresses in its pitch to users that it approaches imple-
mentation from a community wide perspective, rather
than only from a health care organization perspective.
2.2 Mobile Application Development
Most of the existing community resource referral sys-
tems we introduced in sub-section 2.1 use web tech-
nology (desktop or mobile websites) to enable user
interactions. However, we believe that web technol-
ogy is not enough to power user engagement or to
optimize users’ interaction with community resource
referral platforms. In 2018, 51% of the time spent on-
line in the US is on mobile devices. Moreover, 90%
of the time people spend on mobile devices is spent
in apps (BroadBandSearch, 2018). Mobile apps have
higher engagement rates than mobile-optimized web-
sites or desktop web viewing.
Existing community resource referral will soon
need to consider mobile app development to meet
users’ needs and expectations. The key question here
is; why should community resource referral platforms
be built as mobile apps? And what are the key ben-
efits of mobile applications over mobile websites? In
the following, we present the key advantages mobile
apps have over web technology (desktop or mobile
websites) that motivated the software architecture of
our Smart Community Health platform.
Response Time. Mobile applications are usually
1.5 times faster than mobile websites and they per-
form actions much faster too. Mobile applications
store data locally on the mobile device. In web tech-
nology, data needs to be fetched from web servers
which can can be a time consuming task depending
upon the network speed and data size (Baby, 2019).
Personalized Content. With respect to the user ’s
interest, location, preferences, mobile apps make it
easy to personalize content and enable a user-centred
experiences (Pinpin et al., 2019).
Instant Online & Offline Access. All mobile apps
offer instant access by a tap. They allow users to con-
sume their content quickly offering seamless experi-
ence via storing vital data that can be accessed of-
fline too. Web technology rely on pre-defined URLs
that need to be typed in a web browser (Cupala et al.,
2019).
Leveraging Mobile Devices’ Capabilities. Mobile
apps have a unique advantage where access and uti-
lize features from the mobile device such as camera,
NFC, GPS, fingerprint scanner for authentication and
other apps such as calendar, payment, or QR reader,
etc (Sen et al., 2019).
Push Notifications. Push notifications are received
on mobile devices regardless a user opens an app or
not. Notifications are valuable to maintain an open
reliable communication channels with users. These
notifications could express updates, reminders, warn-
ings, etc (Pang and Teh, 2019).
Usability. Unlike web technology that relies on web
browsers to support functions, mobile applications
support a wide range of functions enabling various in-
teractions and swipe gestures like a drag, pinch, hold,
tap, double tap and more, each performing a certain
action that increases user friendliness (Kaya et al.,
2019).
HEALTHINF 2020 - 13th International Conference on Health Informatics
616
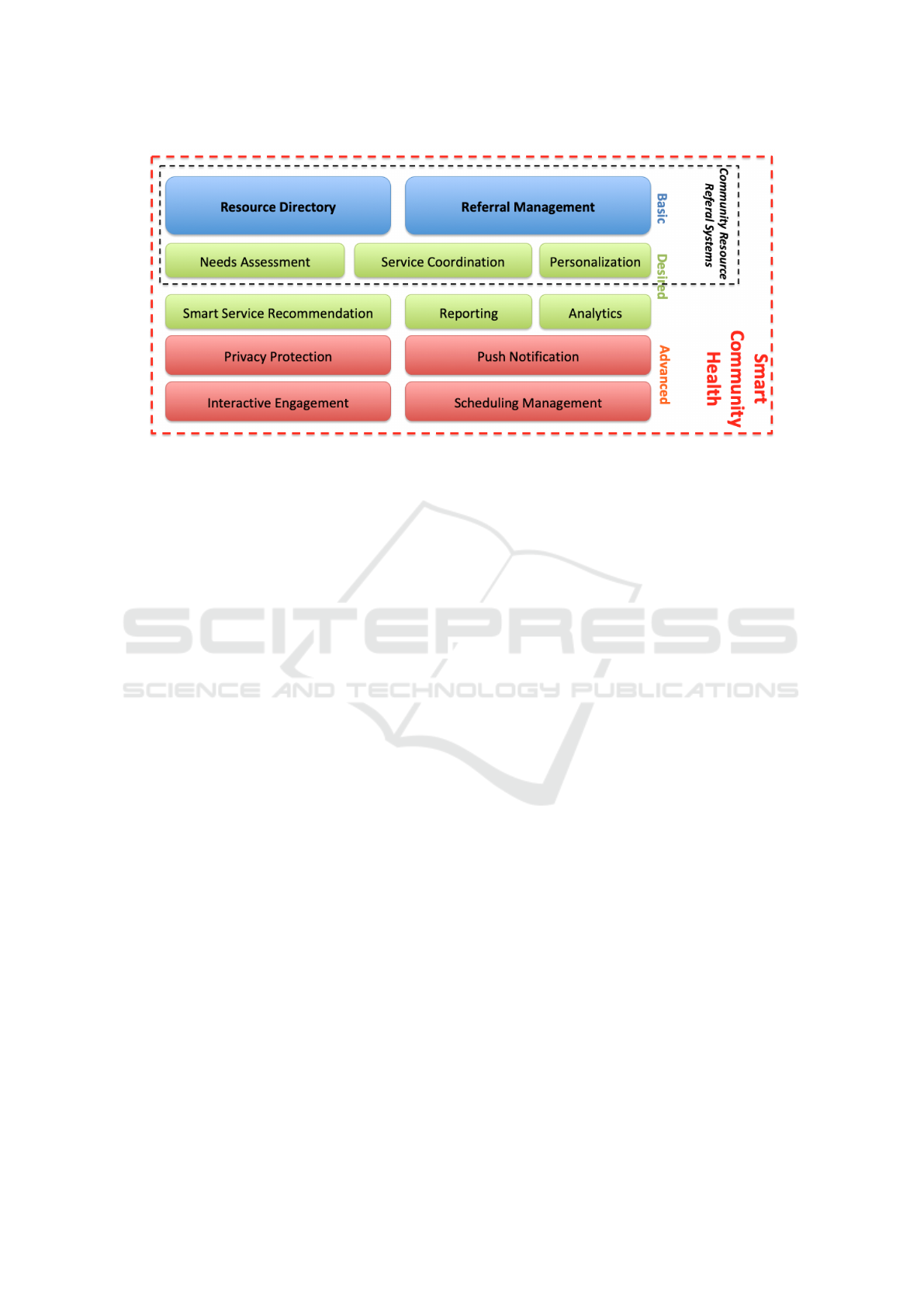
Figure 1: An overview of basic, desired and advanced functionalities of a community resource referral system. Smart Com-
munity Health outperforms the traditional platforms and offers advanced innovative features including push notification,
interactive user engagement and scheduling functionalities.
2.3 Synthesis
In most existing platforms, users can either browse
for services or search based on keywords, usually
based on a program, organization, service, need, or
geographic area. Another limitation that character-
ize most of existing platforms is preventing users to
search for multiple needs simultaneously. All plat-
forms, except CrossTx, offer the possibility to initi-
ate a community resource referral. This referral is
either directly to the community service provider or
through the individual. With CrossTx, users cannot
provide referrals to the individual, instead all referrals
are made directly to the community service provider.
In addition, all the existing platforms enable refer-
ral information to be sent directly to a social service
organization. These platforms do not offer commu-
nity service providers to securely access a dedicate
platform in order to view and act on referrals, to com-
municate with the individual, and potentially the abil-
ity to accept or decline a referral.
Moreover, a critical functionality that is missing
in most of existing platforms is closed-loop referral
tracking. The goal of closed-loop referral tracking is
to find out what happened after a referral is made.
Notifications about services are an important part of
a community resource referral system. For exam-
ple, when information about a service is entered by
a community service provider, it should ideally trig-
ger a notification to individuals who are expressing
needs that match that service. Similarly, a notifi-
cation would ideally be sent to the community ser-
vice provider is an individual is seeking help with a
certain need. Other useful features to facilitate re-
ferrals included appointment scheduling and built-in
web forms that enable patients to apply for specific
services at the time of the referral.
Finally, most of existing platforms do not match
the assessment results with community service
providers. In fact, assessment results should automat-
ically trigger platform actions, for example, recom-
mendation of a list of service providers that address
identified needs filtered with respect to criteria such as
distance, business hours, service quality rating, sup-
ported languages and ethnicities.
3 SMART COMMUNITY HEALTH
The main purpose of the Smart Community Health
is to provide an end-to-end platform that exists out-
side the domain of any organization that prioritizes
connecting people in need with community resources
in their area. Smart Community Health (SCH) is a
full-service, end-to-end community service provider
recommendation platform designed to help address
pressing social, environmental, and health needs
within our communities. The platform is composed of
a mobile application for individuals looking for ser-
vices and a web application for service providers to
register and list their services and relavant informa-
tion about their respective organizations.
In the following section, we detail the fol-
lowed steps to support the Software Development
Life-Cycle (SDLC). (Mahalakshmi and Sundararajan,
2013). First, we present the requirement engineering
Smart Community Health: A Comprehensive Community Resource Recommendation Platform
617
process and highlight the key system requirements.
Next, we provide an overview on the system design
and architecture.
3.1 System Requirements Engineering
Smart Community Health has been designed to meet
specific requirements that aim to to help address
pressing social, environmental, and health needs
within our communities. Therefore, three key actors
have been identified; (1) Community Service Provider
User, (2) Individual User and (3) Health Care Pro-
fessional User. Moreover, with respect to the size
and scale of community service organizations, sev-
eral units or entities of such an organization need to
independently and autonomously set up and control
their instance of the community dashboard by manag-
ing its users and associated credentials and resources.
Hence a third actor has been added ton the list; (3)
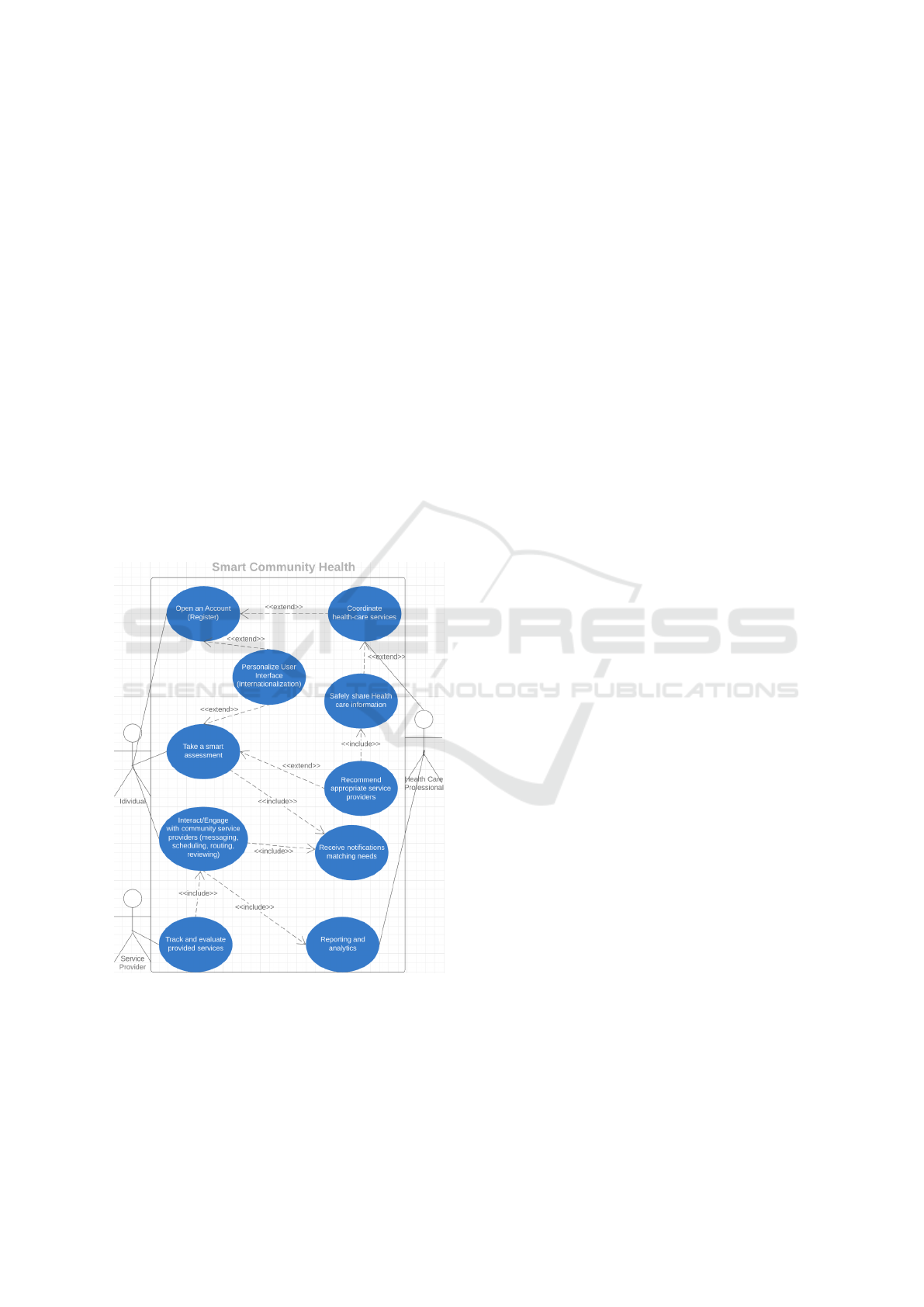
Community Service Provider Administrator. Figure 2
presents the use case diagram of the Smart Commu-
nity Health platform.
Figure 2: Use Case Diagram of the Smart Community
Health platform.
Requirements describe the characteristics that a
system must have to meet the needs of the stakehold-
ers. These requirements are typically divided into
functional and non-functional requirements. Func-
tional Requirements [FR] describe how a software
must behave and what are its features and functions
(Shah and Rogers, 1988). Non-Functional Require-
ments [NFR] describe the general characteristics of a
system (Glinz, 2007) They are also known as software
quality attributes (Kim and Kim, 2019).
The following is a selection of functional require-
ments:
• [FR1] The system shall allow Community Service
Provider User, Community Service Provider Ad-
ministrator and Health Care Professional User to
create (register), view and edit accounts to be al-
lowed secure access to the platform;
• [FR2] The system shall allow to Health Care Pro-
fessional User to list and coordinate health care
services;
• [FR3] The system shall allow users to support
multiple languages (Internationalization);
• [FR4] The system shall allow Health Care Pro-
fessional User to safely share Health care infor-
mation;
• [FR4] The system shall allow Individual User to
take a smart assessment;
• [FR5] The system shall provide Individual
User with recommended and appropriate service
providers with respect to multiple criteria (i.e. lo-
cation, review, health network, etc.);
• [FR6] The system shall allow actors to inter-
act through reliable and synchronous communica-
tion channels such as instant messaging, internal
emails, routing services, appointment scheduling,
and review of services;
• [FR7] The system shall allow Individual User
to subscribe for a notification service matching
needs of interest;
• [FR8] The system shall allow to track and evalu-
ate provided services;
• [FR9] The system shall allow to provide Commu-
nity Service Provider User, Community Service
Provider Administrator and Health Care Profes-
sional users with reporting and analytics;
The above listed functional requirements have
been analyzed and validated with stakeholders and the
following set of quality attributes (non-functional re-
quirement) has been derived:
• [NFR1] Availability: the system shall be available
24/7/365;
• [NFR2] Scalability: the system shall be capable
to scale in order to address large number of users
connecting and interacting with the platform.
HEALTHINF 2020 - 13th International Conference on Health Informatics
618

Figure 3: The Smart Community Health architecture.
• [NFR3] Portability: the system shall support
common iOS and Android-based mobile devices.
• [NFR4] Security: user access and access control
as well as data management and sharing must sup-
port security best practices and techniques and
comply with standard protocols;
3.2 System Architecture
The Smart Community Health platform architecture
is a the cloud-based architecture detailed in Figure 3.
The architecture uses the well-established infrastruc-
ture offered by Amazon Web Services (AWS) (Ko-
valcik and Altman, 2019). The main motivation be-
hind the use of AWS is the non-functional require-
ments validated with our stakeholders with regards to
availability (NFR1), scalability (NFR2) and security
(NFR4).
The Smart Community Health platform architec-
ture is composed of three layers; the mobile appli-
cation, the web application and the back-end cloud-
based modules hosted by AWS. The use of mobile
and web applications aims to address the portability
quality attribute supported by the non-functional re-
quirement NFR3.
The platform also heavily rely on Application Pro-
gram Interface (API). In fact, traditional web applica-
tion design, centred on client server architecture and
scripting languages to ensure dynamic rendering, has
delivered significant improvements in web develop-
ment. But when facing the advanced characteristics of
interactive content with multiple channels such as the
Smart Community Health platform, the client-server
request-driven model alone hits its limits. Applica-
tions become harder to scale and the web application
harder to manage, leading to ever-more tightly cou-
pled systems. To move beyond the client server archi-
tecture, and to enable more scalable, contextual and
responsive systems, we integrated and implemented a
fully event-driven architecture (EDA) within the core
of our SCH platform and design capabilities.
3.3 SCH Mobile Application
The SCH mobile application supports the common
iOs and Android mobile operating systems. It aims to
target a large panel of mobile devices and hence reach
out to a large community of potential users (see Fig-
ure 4a). The SCH mobile application allows users to
securely register or simply to use the mobile applica-
tion without registration (see Figure 4b). Obviously,
registered users have access to personalized account-
based services such as scheduling, instant messag-
ing and internal mailing (see Figure 4c). In addition,
registered users have the possibility to share individ-
ual contact information cards with community service
providers. Sharing contact information allow individ-
uals and community service providers to engage in a
secure and interactive collaboration to initiate, exe-
cute, track and follow up on services. The SCH mo-
bile app allows for individual interaction tracking and
monitoring.
The main goal of the SCH mobile application
is to match individual needs to available services
Smart Community Health: A Comprehensive Community Resource Recommendation Platform
619

(a) SCH Home Page (b) SCH Welcome Page (c) Demographics
Figure 4: Examples of the Smart Community Health mobile application graphic user interfaces.
listed by community service providers. This mo-
bile application uses a smart assessment tool that
allows to self-identify health strengths, challenges
and needs. This SCH mobile application integrate
MyStrengths MyHealth
TM
(MSMH), a whole-person
strengths-based consumer-facing tool designed for in-
dividuals, families, and communities to self-identify
strengths, challenges, and needs. This SCH mobile
application leverages the rigour of the Omaha System
(Martin and Scheet, 1992), a multi-disciplinary stan-
dardized health terminology and valid, reliable instru-
ment that addresses all of health across four domains
with 42 discrete concepts.
Surveys for each of the 42 concepts are embed-
ded using expert- and community-validated plain lan-
guage terms. In this SCH mobile application, the
Omaha System domains, Environmental, Psychoso-
cial, Physiological, and Health-related behaviors, are
called My Living, My Mind, Network, My Body, and
My Self-care (see Figures 5a). In the SCH mobile ap-
plication, signs/symptoms associated with the 42 con-
cepts were renamed Challenges (see Figure 5b), and
interventions are called Needs (see Figure 5c).
This community-friendly, consumer-facing instru-
ment generates data for community service providers,
health care organizations, education, and research.
Once an individual completes the assessment, the
SCH mobile application provide a selection of rec-
ommended community service providers that match
the expressed needs (see Figure 6).
3.4 SCH Community Dashboard
The SCH Community Dashboard is a web applica-
tion platform that serves community partners includ-
ing community service providers and health care or-
ganizations. It allows organizations to create an ac-
count and securely access and manage their profile
(see Figure 7a and 7b). Once logged in, an organiza-
tion representative can define a geospatial service area
where this organization offer services (see Figure 8a).
Each defined geospatial service area is characterized
with a set of services and ethnicities targeted by these
services (See Figures 8b and 9a ).
The SCH Community Dashboard has been de-
signed to address the needs from small, medium and
large scale organizations. Large scale organization
can hence define multiple branches, each servicing a
specific geospatial area and helping a set of commu-
nities or ethnicities. For example, an organization like
the Y (YMCA: Young Men’s Christian Association),
a worldwide organisation that aims to put communi-
ties into practice by developing a healthy ”body, mind,
and spirit”. Such a large organization counts 120 na-
tional associations worldwide and 2,700 separate lo-
cal YMCA entities in the USA only. The capability
of the SCH Community Dashboard to allow multiple
entities management and yet a centralized control tp
main entities make it a unique platform.
Using the SCH Community Dashboard, organi-
zations can reach out to individuals who experience
HEALTHINF 2020 - 13th International Conference on Health Informatics
620
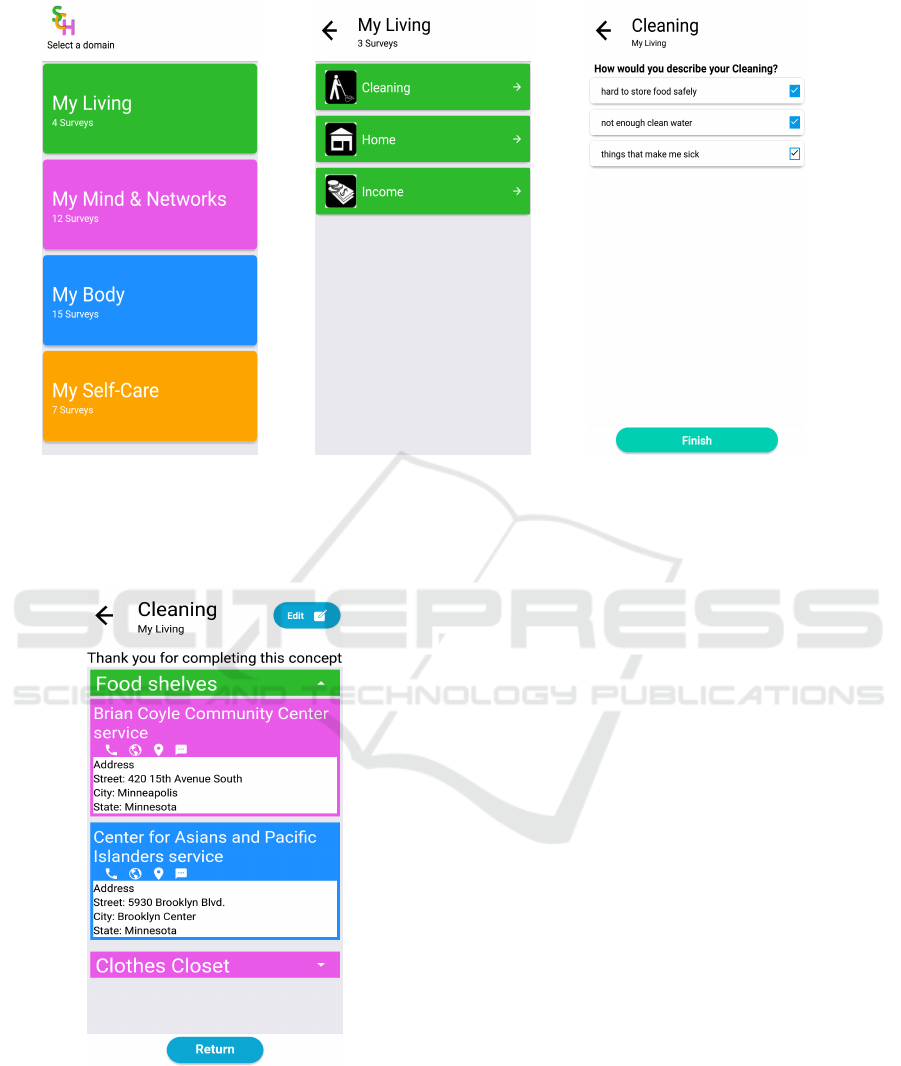
(a) List of Domains (b) List of Challenges for My Living (c) List of Needs for Cleaning
Figure 5: The Smart Community Health mobile application component. Sub-Figures 5a, 5b, 5c describe the smart assessment
process. The illustrated challenges in Sub-Figure 5b are associated with the domain ”My Living”. The proposed screening
questions in Sub-Figure 5c are associated to the challenge ”Cleaning”.
Figure 6: The recommended community service providers
grouped by service category for the ”Cleaning” need. Note
the user engagement interactive anchors to useful services
including phone call, web browsing, routing and instant
messaging.
needs that can be addressed by their services. Organi-
zations utilize the internal messaging, email and cal-
endar services and benefit from the notification man-
aging services for a closed-loop tracking of referrals.
Finally, the SCH Community Dashboard provide or-
ganizations with a real-time analytics dashboard en-
abling full control, management and monitoring of
provided services and serviced communities (see Fig-
ure 9b).
4 CONCLUSION
In this paper, we presented Smart Community Health,
a full-service, end-to-end community service provider
recommendation platform designed to help address
pressing social, environmental, and health needs
within our communities. The platform is composed
of a mobile application for individuals looking for ser-
vices and the Community Dashboard platform for ser-
vice providers.
The mobile application integrates a health assess-
ment tool that builds on top of an existing validated
screening tool, My Strengths My Health. It gener-
ates international disease classification (ICD) codes
that can be stored within all healthcare systems. Plac-
ing the assessment in the mobile app reduces the bar-
rier to accessing services, because the app is freely
available to anyone regardless of healthcare status or
the organization they belong to. When participants
Smart Community Health: A Comprehensive Community Resource Recommendation Platform
621
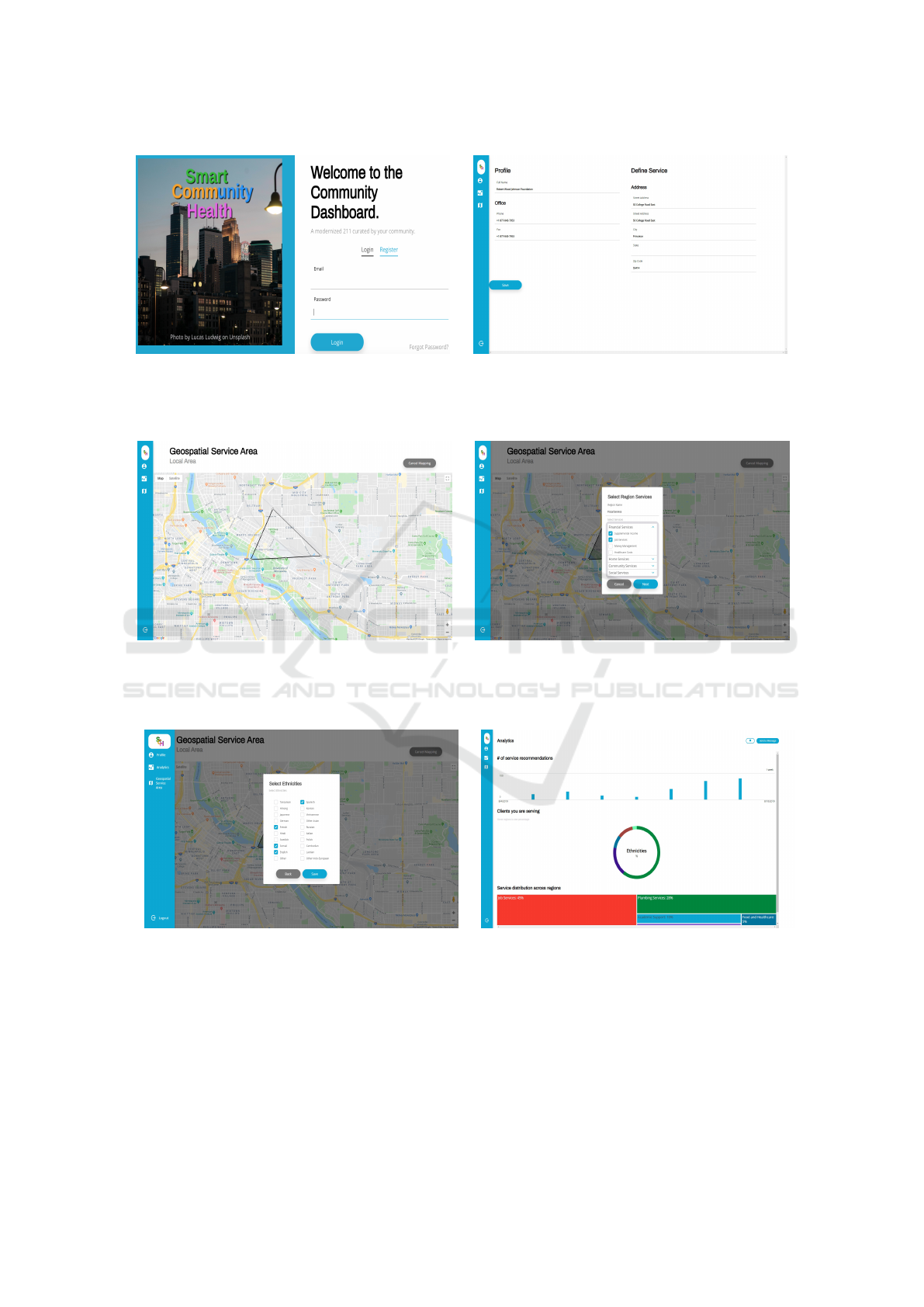
(a) Hme page (b) Service provider profile page
Figure 7: The Smart Community Health web app Community Dashboard component. Community service providers securely
register and access this platform.
(a) Specification of the geospatial service area. (b) Specification of the offered services.
Figure 8: The Smart Community Health web app Community Dashboard component. Community Dashboard offers an
interactive map allowing for polygon drawing.
(a) Specification of served ethnicities. (b) Available real-time analytics.
Figure 9: The Smart Community Health web app Community Dashboard component. Community service providers use this
platform as a dashboard to track, control and manage their listed services.
use the assessment and indicate they have a need they
are immediately presented with information connect-
ing them to organizations that provide those services.
The Community Dashboard powers the mobile
app assessment, by allowing community organiza-
tions to register services they provide into our appli-
cation. It start by providing a suite of curated ser-
vices from our partnered organizations, then it allows
the community to add their “pop-up services”. It also
provides community service providers with analytics
for informed and meaningful actions. The Dashboard
platform provides full-service analytics for organiza-
HEALTHINF 2020 - 13th International Conference on Health Informatics
622

tions, allowing them to understand what is happen-
ing in their community. In particular, it focuses on
providing a common framework that allows health
providers and city planners to understand the spatial
and temporal relationships between social determi-
nants of health and health outcomes.
To conclude, the main contribution of Smart
Community Health is it community focused design,
its community curation, its community engaged ap-
proach and its advanced analytics that allow for a
greater understanding of community needs.
5 FUTURE WORK
The development of the Smart Community Health
platform has not finish yet. Several features and func-
tionalities in the product backlog are still waiting for
grooming to be addressed by the coming sprints. The
coming steps will include a live pilot with a real com-
munity service provider and a representative focus
group of actual users.
One of the areas we are interested in investi-
gating is the assessment component. Although the
SmartCommunity Health platform integrates a well-
established health assessment tool that builds on top
of an existing validated screening tool, My Strengths
My Health. We believe emerging Artificial Intelli-
gence technologies and more particularly conversa-
tional agents could benefit our platform. The term
‘Conversation Agent’ has come to mean a wide vari-
ety of systems with varying capabilities and purposes,
with the underlying assumption that the agent partic-
ipates in a human-machine dialog. Licklider’s ‘Man-
machine symbiosis’ (Licklider, 1960) was one of the
earliest discourses from a Human Computer Interac-
tion (HCI) perspective that visualized humans inter-
acting with machines in a natural manner. Research
in conversation agents started with messaging-based
chatbots, whose purpose was to maintain a conversa-
tion with a human user.
In the last decade, conversational agents started
focusing more on utility, with the goal of accom-
plishing specific tasks. Nowadays, conversational
agents range across several modalities, including
speech (such as Siri, Alexa, Cortana), text-messaging
(such as Domino’s, CNN, Pandorabots, Burberry, etc.
found on Messenger, Slack, and/or Skype platform),
and as multimodal embodied agents. Table 1 provides
a summary of most popular text-messaging based
CAs, called chatbots.
Using chatbots to engage individuals in a natu-
ral language based conversation will move our Smart
Community Health platform from static assessments
Table 1: Timeline of Chatbot (Bieliauskas and Schreiber,
2017).
Year Timeline of Chatbots
1950 Chatbots Revolution Concept of truly in-
telligent Machine
1966 Eliza – MIT – Simulate Human Conversa-
tion
1972 Parry- Added Conversational Strategy
1988 JABBERWACKEY- Simulate natural hu-
man Chat with Entertaining and Humorous
Manner
1992 Dr. SBAITSO- Speech Synthesis Program
1995 Alice- Artificial Linguistic Internet Com-
puter Entity – Heuristic Patten
2001 SMARTERCHILD- Fun Personalized net-
work; Precursor to Apple’s SIRI
2006 IBM’s WATSON- Natural Language Pro-
cessing; Machine Language
2010 SIRI- Apple’s IOS, Natural Language UI
2012 Google Now- uses natural language for
google search on mobile
2015 Alexa- Amazon Echo Device; using lan-
guage processing Algorithms
2015 CORTANA- Bing Search; Natural Voice;
Different Language
2016 Facebook user bots
2016 TAY- Microsoft to mimic the speech and
habit of teenage girl
towards more dynamic evolutive and learning assess-
ment approach.
REFERENCES
Baby, K. T. (2019). Generating internal motivation through
mobile application technology. In Metacognition in
Learning. IntechOpen.
Bieliauskas, S. and Schreiber, A. (2017). A conversational
user interface for software visualization. In 2017 IEEE
Working Conference on Software Visualization (VIS-
SOFT), pages 139–143. IEEE.
BroadBandSearch (2018). Mobile Vs. Desktop Usage.
Cartier, Y., Fichtenberg, C., and Gottlieb, L. (2019). Com-
munity resource referral platforms: A guide for health
care organizations. Technical report, Social Interven-
tions Research & Evaluation Network (SIREN).
Cupala, S. J., Ye, L., and Garg, N. (2019). Selective update
of core mobile device user interface through applica-
tion marketplace. US Patent App. 10/235,155.
Glinz, M. (2007). On non-functional requirements. In 15th
IEEE International Requirements Engineering Con-
ference (RE 2007), pages 21–26. IEEE.
Gundersen, C. and Ziliak, J. P. (2015). Food insecurity and
health outcomes. Health affairs, 34(11):1830–1839.
Smart Community Health: A Comprehensive Community Resource Recommendation Platform
623

Han Rebekah Wong, S. (2012). Which platform do our
users prefer: website or mobile app? Reference Ser-
vices Review, 40(1):103–115.
Kaya, A., Ozturk, R., and Gumussoy, C. A. (2019). Usabil-
ity measurement of mobile applications with system
usability scale (sus). In Industrial Engineering in the
Big Data Era, pages 389–400. Springer.
Kim, S.-H. and Kim, W.-J. (2019). Evaluation of soft-
ware quality-in-use attributes based on analysis net-
work process. Cluster Computing, 22(1):2101–2114.
Koh, H. K., Piotrowski, J. J., Kumanyika, S., and Field-
ing, J. E. (2011). Healthy people: a 2020 vision for
the social determinants approach. Health Education
& Behavior, 38(6 suppl):551–557.
Kovalcik, J. and Altman, E. (2019). Amazon web services
(aws) & digital initiatives.
Kushel, M. B., Gupta, R., Gee, L., and Haas, J. S. (2006).
Housing instability and food insecurity as barriers to
health care among low-income americans. Journal of
general internal medicine, 21(1):71–77.
Licklider, J. C. (1960). Ire transactions on human factors
in electronics. online]. URL https://goo. gl/vndAUs
(2017-11-13).
Lurie, N. and Dubowitz, T. (2007). Health Disparities and
Access to Health. JAMA, 297(10):1118–1121.
Mahalakshmi, M. and Sundararajan, M. (2013). Traditional
sdlc vs scrum methodology–a comparative study. In-
ternational Journal of Emerging Technology and Ad-
vanced Engineering, 3(6):192–196.
Martin, K. S. and Scheet, N. (1992). The omaha system. Ap-
plications for Community health nursing, page 1992.
McGowan, A. K., Kramer, K., and Teitelbaum, J. B. (2019).
Healthy people: The role of law and policy in the
nation’s public health agenda. The Journal of Law,
Medicine & Ethics, 47(2 suppl):63–67.
Molfenter, T. (2013). Reducing appointment no-shows: go-
ing from theory to practice. Substance use & misuse,
48(9):743–749.
One Degree (2019). One Degree.
Pang, K. L. and Teh, H. S. (2019). Mobile-based access
control system. US Patent App. 16/059,537.
Pieces Iris (2019). Pieces Iris.
Pinpin, M. B. G., Greathouse, W. E., Wall, J. J., Kendall,
K. L., and Li, D. (2019). User personalization of third-
party webpage images. US Patent App. 10/248,812.
Sen, S., Spatscheck, O., Huang, J., Mao, Z. M., and Qian,
F. (2019). Facilitation of mobile device resource opti-
mization. US Patent App. 10/172,041.
Shah, J. J. and Rogers, M. T. (1988). Functional re-
quirements and conceptual design of the feature-
based modelling system. Computer-Aided Engineer-
ing Journal, 5(1):9–15.
Smith, T., Mattingly, T. J., and Slabaugh, L. (2019). Im-
proving health determinants outside of the clinic does
not mean outside of clinical science. In Healthcare.
Elsevier.
Smith, W. R., Betancourt, J. R., Wynia, M. K., Bussey-
Jones, J., Stone, V. E., Phillips, C. O., Fernandez,
A., Jacobs, E., and Bowles, J. (2007). Recommen-
dations for teaching about racial and ethnic disparities
in health and health care. Annals of Internal Medicine,
147(9):654–665.
TAVHealth (2019). TAVHealth/TAVConnect.
Unite Us (2019). Unite Us.
HEALTHINF 2020 - 13th International Conference on Health Informatics
624
