
A Rule-based Content Management Framework for Effective
Development of Intelligent Mobile Apps in Healthcare
Mohammad Raahemi
1 a
, Benjamin Eze
1 b
, Cléo Mavriplis
2
and Liam Peyton
1
1
Faculty of Engineering, University of Ottawa, Ottawa, Canada
2
Bruyère Academic Family Health Team, Ottawa, Canada
Keywords: Healthcare Applications, Rule-based Content Management, Mobile Applications, Wellness.
Abstract: The number of published healthcare articles is increasing dramatically every year, making it difficult for
physicians and patients to stay current with the latest information related to healthcare. One possible approach
to improving the ability of physicians and patients to stay current with the latest trends in healthcare is through
the use of mobile applications. The challenge to this approach is the lack of a content management framework
that allows medical experts to continuously integrate new knowledge and content into the design of easy to
use software applications for patients and other healthcare personnel. This paper introduces the CANBeWell
mobile application, a rule-based content management application for collecting and aggregating important
medical data from medical experts, and disseminating this data to patients and other clinicians using a context-
aware mobile app in support of preventive healthcare.
1 INTRODUCTION
There is a major push to improve the quality of life
for patients with chronic and complex health
conditions through preventive healthcare (Deek,
2016). With the proliferation of misinformation on
the Internet today, it is becoming increasingly vital
that the content needed for preventive healthcare
comes from the validated sources and provided to
patients in a context that allows them to make
informed and accurate medical decisions (Wald et al.,
2007).
Intelligent mobile applications (apps) have been
developed in a number of areas to inform and help
patients and physicians manage chronic diseases such
as diabetes (Widmer, et al. 2015), inform and support
breast cancer patients (T Ginossar et al, 2017), and
provide app-based interventions for the prevention of
cardiovascular disease (Eng & Lee, 2013).
Also, wellness apps have been shown to increase
self-management in patients and improve outcomes
across various socioeconomic spectrums (Handel,
2011). However, evidence-based information is often
lacking in healthcare apps (Eng & Lee, 2013). Ideally,
medical experts need to be involved in organizing
a
https://orcid.org/0000-0002-3229-570X
b
http://orcid.org/0000-0001-8370-0042
reference medical information used in a mobile app,
so it is convenient for patients and providers to use.
But the effectiveness and efficiency of these wellness
apps are always a big concern for medical experts
(Yang & Silverman, 2014). As a result, medical
experts attempt to design and conduct various types
of surveys to resolve such concerns.
This paper proposes a rule-based content
management framework that integrates an easy-to-
use, context-aware mobile application with
preventative healthcare content. Our framework
incorporates an automated workflow for collecting
and aggregating important medical data from medical
experts, data which can then be disseminated to
patients and other clinicians using a context-aware
mobile app in support of preventive healthcare. This
is an early research work being conducted in
partnership with Dr. Cleo Mavriplis of the Bruyere
Research Institute, Faculty of Medicine, University of
Ottawa, with a focus on preventative healthcare
applications (apps).
The rest of this paper is organized as follows.
Section 2 provides some background on rule-based
content management application frameworks and the
usability of mobile applications. Section 3 discusses
522
Raahemi, M., Eze, B., Mavriplis, C. and Peyton, L.
A Rule-based Content Management Framework for Effective Development of Intelligent Mobile Apps in Healthcare.
DOI: 10.5220/0008987405220529
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 522-529
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All r ights reserved

some related work. Section 4 presents our framework
and CanBeWell application. Section 5 discusses our
findings. Section 6 shows the framework evaluation
based on a survey of the application users and Section
7 provides some conclusions and future work for this
research.
1.1 Motivation
A survey conducted by Paul Krebs and Dustin T
Duncan (Krebs & Duncan, 2015), shows that just
over half of the mobile phone users (934/1604,
58.23%) had downloaded a health-related mobile
app. North Americans are increasingly relying on
mobile technology and the internet for health-related
information and resources (Fox & Duggan, 2012).
The proliferation of smartphone ownership among
US adults, particularly among traditionally
underserved populations (e.g., low-income,
racial/ethnic minorities), has expanded the potential
reach of healthy eating, physical activity, and weight
loss programs. From 2011 to 2015, the percentage of
US adults owning a smartphone increased from 35%
to 68% (Anderson, 2015). In addition, low income
and racial/ethnic minority populations are more likely
to be smartphone-dependent, thus relying primarily
on their phones for health information (Smith, 2015).
In general, the development and adoption of
health and wellness smartphone apps have outpaced
empirical investigations (Boulos et al., 2011).
Making these apps “smarter” through AI can enhance
their accuracy, effectiveness, and efficiency –
increasing users' trust while allowing input from
medical experts, which in turn increases the utility of
these applications.
Benferdia and Zakaria identified all the key user
groups of m-health apps. These groups are patients
(44%), the physicians – health specialists, doctors,
and nurses (37%), general users (13%), and finally
caregivers (7%). Providing the right health
information to the right person at the right time is one
of the most important features of every m-health
application (Benferdia & Zakaria, 2014).
2 BACKGROUND
2.1 Rule-based Content Management
Systems
Rule-based content management systems have been
studied for nearly two decades in application areas
such as geographical information systems (GIS),
metadata catalog systems, and healthcare (Beatty and
Lopez-Benitez, 2012). Based on these application
areas, content management systems can be classified
into two categories - content-type-specific and
general-purpose systems (He et al., 2007).
Content-type-specific systems include 1) video
adaptation scheme for adaptive video streaming
(Chang, Zhong and Kumar, 2001), 2) multimedia
content adaptation scheme such as InfoPyramid that
provides a multimodal, multiresolution
representation hierarchy for multimedia content
(Mohan et al., 2019).
The trade-offs imposed by rule-based systems in
terms of time to deliver content, memory
consumption, and fault tolerance have been analyzed
(Beatty and Lopez-Benitez, 2012). This work
presents a novel approach that uses a rule-based
system to regulate web page generation thereby
improving cache performance and query generation
with large unorganized data sets. Further, there are
approaches that use data mining and statistical
techniques to control content-based rules, such as
associating significant browsing events with specific
contexts (Wang, 2007).
Some general-purpose content adaptation systems
have also been developed, such as BARWAN
(Brewer et al., 1998), and Power Browser
(Buyukkokten et al., 2002). Each of these approaches
has some advantages. However, they do not provide
for flexible and extensible content adaptation. Their
adaptation approach is either fixed or hardcoded in
the system. When the adaptation goal is changed,
such as when a new client device or a new data type
is introduced into the system or a new adaptation
technique is developed, the system must be
redesigned to accommodate the change.
Finally, He et al. (2007) present an extensible
content adaptation system, Xadaptor. This uses a rule-
based approach to facilitate extensible, systematic
and accommodative content adaptation. It integrates
adaptation mechanisms for numerous content sorts
and organizes them into the rule base where rules are
invoked based on the individual client information.
(He et al., 2007)
2.2 Usability of Mobile Apps
Usability is considered important for users to accept
the system. A well-known concept in design and
healthcare systems development, the concept has its
roots in the development of information and
communication systems and human-computer
interaction (HCI) (Larsson, 2013)
Usability is defined as “the extent to which a
product can be used by the specified users to achieve
A Rule-based Content Management Framework for Effective Development of Intelligent Mobile Apps in Healthcare
523

specified goals with effectiveness, efficiency, and
satisfaction in a specified context of use” (Jokela,
Iivari, Matero & Karukka, 2003). Usability is an
important factor in mHealth wellness applications,
especially for people who may find it challenging to
interact with smartphones, PDAs, etc. Besides a user
perspective and an aim toward creating beneficial
solutions that are effective, efficient, and satisfactory,
the context is considered important and has a
significant impact on usability work.
Focusing on usability requires an understanding
of the context before, during and after
implementation (Larsson, 2013). This means that
usability work must be included in all steps of the
development process. Studies showed that hundreds
of thousands of products are returned each year, not
because of its functional behaviour but because of bad
user experience (Kalimullah, 2017)
User experience is a consequence of a user’s
internal state, the characteristics of the designed
system, and the context in which the interaction
occurs. User experience considers the wider
relationship between the product and the user in order
to investigate the individual’s personal experience of
using the product (Kalimullah, 2017). Researchers
and practitioners use different techniques and
methods to capture the customer’s psychological and
behavioural aspects toward a product and have those
incorporated into the design of future products.
2.3 Standards for Usability Testing
Standards and best practices have long been
considered beneficial, as they stop us from designing
based solely on personal opinion or experiences. To
that end, ISO 9241 was defined. This standard is a
multi-part standard from the International
Organization for Standardization covering
ergonomics of human-computer interaction. The ISO
9241-11 standard defines usability as "the extent to
which a product can be used by specified users to
achieve specified goals with effectiveness, efficiency
and satisfaction in a specified context of use"
(International Organization for Standardization,
1998). Poor usability is a major obstacle to health
information adoption (Yen et al., 2012) and a clear
cause of medical errors (Zhang et al., 2003). ISO
9241 identifies three metrics for usability testing:
1) Effectiveness: Measures the accuracy and
completeness towards achieving specified user
goals
2) Efficiency: Measures the resources expended
towards the accuracy and completeness of
achieving set user goals
3) Satisfaction: Measures the level of comfort and
positive attitudes towards the use of a product.
3 RELATED WORK
Similar to our framework, most content management
systems (CMS) used in preventive healthcare
integrate with a clinical decision support system.
There are two broad categories: 1) event-driven CMS
systems - triggering notification based on some
clinical contexts and 2) portal or mobile-based CMS
– use a portal or an app to allow patients to choose the
context for the information they need. Our framework
belongs to the second category.
Gunaratnam et al. (2012) propose a conceptual
framework for a perinatal clinical decision support
system that uses a knowledge-base of rules, a
workflow engine, and a notification engine to help
physicians to send notifications to families on
preventative measures for managing at-risk
pregnancies. The knowledge-base is a content
management system that comes from validated
medial information combined with the patient
electronic medical record required to provide the
context for the notifications sent to the participants.
Cleland et al. (2017) present the usability
evaluation of a mobile app for managing diabetic foot
disease that uses a CMS with thermal imageries,
customized educational content, and game-based
scenarios that help diabetic patients to self-manage
their conditions.
Barbara et al. (2017) describe an evidence-based
database for educating geriatrics-focused public
health professionals. This portal-based CMS provides
reliable health information that informs their
management of care for elder patients. The portal
provides searchable evidence-based content but lacks
annotated graphics or a rules engine for context
customization.
Kuo & Fuh (2011) proposes a clinical decision
support system that uses rules to interpret health
examination results. This work supports a custom rule
syntax for implementing computer-interpretable logic
for interpreting health examinations. These rules rely
heavily on ontologies such as diagnosis code,
procedure codes, rankings, etc., and a reasoning
engine that employs a rule combining algorithm for
decision making. The challenge with this system is
that it lacks a graphical user interface for managing
the rules. That means changes to the rules would
require software changes which is a gap for most
medical experts.
HEALTHINF 2020 - 13th International Conference on Health Informatics
524
4 RULE-BASED CONTENT
MANAGEMENT APPLICATION
4.1 Framework Overview
Our rule-based content management application
leverages declarative rules developed by medical
experts with information on the common health
challenges that affect various organs of the body for
different ages and gender.
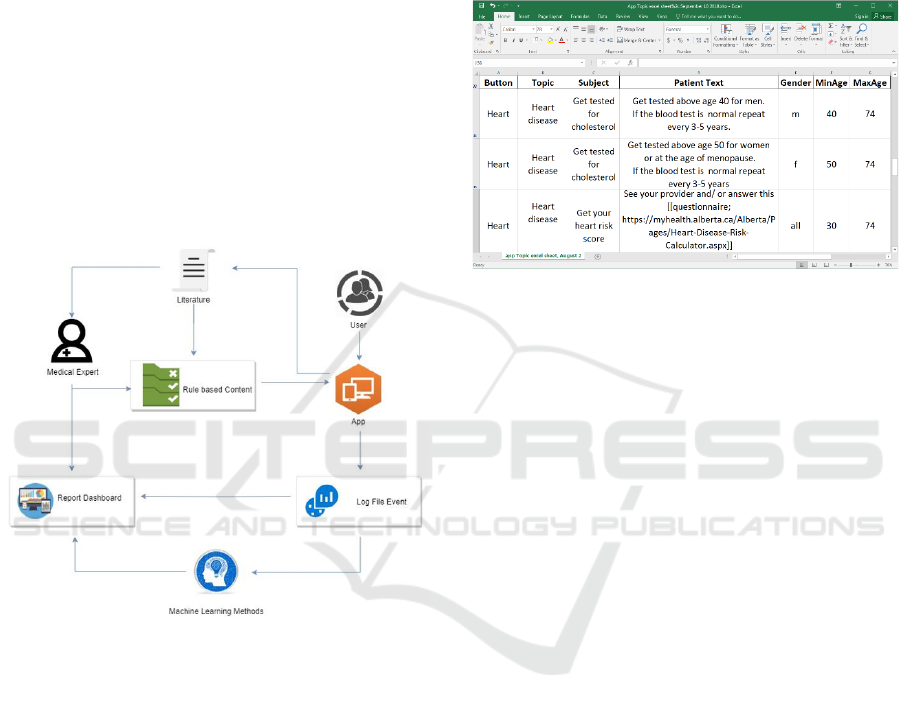
As shown in Figure 2, rules are created and
managed by medical experts based on research and
findings from the literature. These rules are then
converted to a machine-readable JSON file and
pushed to a mobile app that is made available to users
using very interactive, mobile-friendly user
interfaces.
Figure 2: The Generalized Model of Rule-Based Content
Management.
As users interact with the application, logs are
collected and used to feed both an analytics
dashboard and machine learning algorithms that also
feed analysis results to the report dashboard. Usage
data and analytics results are fed back to experts to
help provide more content to patients and service
providers.
4.2 Managing Rule-base Content
Rule-based contents are then used to dynamically
display the correct content based on the language of
the user, gender and age of the patient, and whether
they want information appropriate for a patient or a
provider. Since most medical experts are familiar
with using spreadsheets, we decided to use an Excel
spreadsheet to organize and classify information for
these experts. Figure 3 shows a snipped of the Excel
spreadsheet that was used with our rule-based
application. Each of the columns corresponds to the
classification of content. Each row is a rule that says
what content to display, depending on the value of
gender and the age range.
Figure 3: Content Rules Spreadsheet for Medical Experts.
The content in the first row of the spreadsheet is
for a male patient between 40 and 74 years old. The
content in the second row is for a female patient
between 50 and 74. The content in the third row is for
patients of all gender, between 30 and 74 years.
The simple guidelines for the medical expert to
follow are summarized in a single simple
documentation web page that they can refer to. We
have defined two simple annotations that the medical
expert can use. One is to include links with an
appropriate text anchor for supplementary materials.
The other is to embed images in the content
displayed.
The content from the Excel spreadsheet from the
experts is then translated into different languages as
needed to support the targeted users. These files are
then converted to machine-readable JSON files. The
choice of a JSON file is because of its flexibility with
various web and mobile application development
platforms. Regression tests are run on the app to
ensure that it is functioning properly. And finally, the
medical expert manually tests the app to be sure the
content specified is displaying correctly.
To support French and English users, there are
four content files for the application. One file,
topics_en.json, for content on proactive wellness
topics and one file, tests_en.json, for content on the
screening test. There are French versions of those
files as well (topics_fr.json, tests_fr.json).
A Rule-based Content Management Framework for Effective Development of Intelligent Mobile Apps in Healthcare
525
4.3 CANBeWell Application
The CANBeWell application was developed by
engineering students in the Biomedical Engineering
Smartphone Training program at the University of
Ottawa in collaboration with Dr. Cleo Mavraplis who
is the medical expert. It is intended for use by both
patients and primary care providers.
CANBeWell organizes information on proactive
wellness topics and recommended screening tests by
age and gender in an easy to use interface that
includes an annotated anatomical image where the
user can click on different parts of the body. Users
log in as either a provider or a patient and by clicking
on different parts of the annotated anatomical body
image, text and important links with supporting
evidence and supplementary information are
displayed based on the context of the use – provider
or patient.
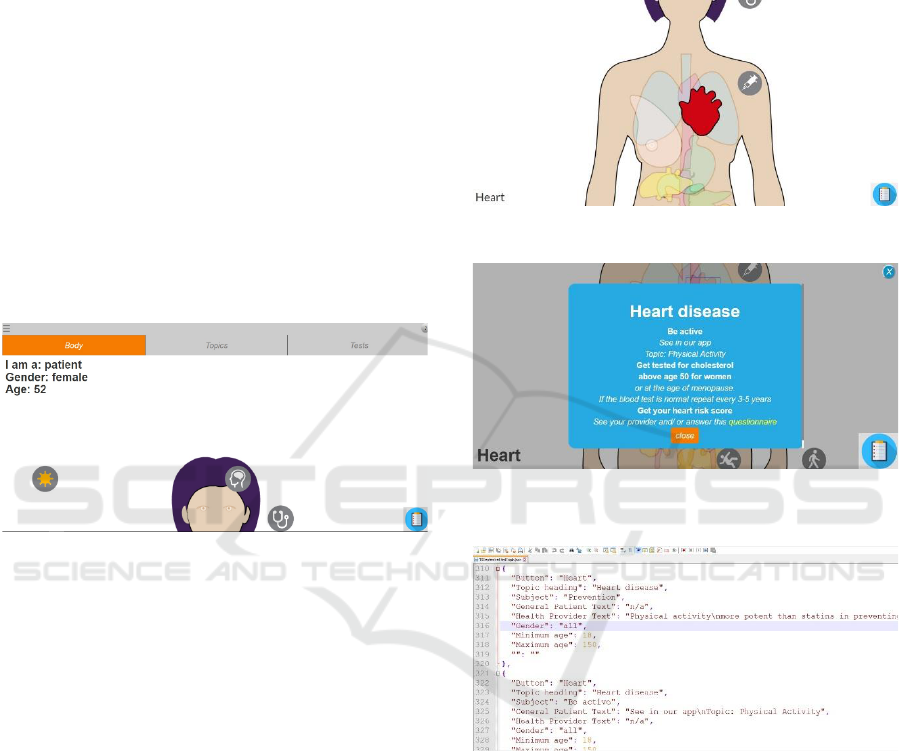
Figure 4: CANBeWell Application Banner.
Figure 4 shows the banner of the application.
Information is presented to the users visually through
the Body tab or by alphabetically sorted topics if they
click on the Topic tab. The top left corner displays the
current configuration. The content displayed in
Figure 2 is relevant to a female who is aged 52. If the
user clicks in that top left corner configuration panel,
they can change the configuration so that content is
displayed for a different user context and patient. For
example, to a physician, or a patient of different ages
(18-149) and different gender (female, male or all).
In figures 4 and 5, one can see parts of the body
map (In this case for a female). Individual body parts
can be clicked on. In Figure 3, the heart has been
clicked on and is highlighted but one can see and click
on other body parts (lungs, liver, kidneys). There are
also additional icons. A needle for vaccinations is
shown in Figure 5 A sun icon for sun exposure, a
stethoscope icon for physical exams, and a brain icon
for memory problems in Figure 4.
In figure 6, the content available is displayed.
Clicking on the Heart Icon brings up the Heart
Disease topic, and there are three subjects for that
topic: Be Active, Get Tested for Cholesterol, Get your
Heart Risk Score. The specific content that is
displayed depends on the age and gender specified in
Figure 2, and whether the information is intended for
a patient or a physician.
Figure 5: Annotated Body Image with associated icons.
Figure 6: Context-based popup displays information by
subject for a given topic.
Figure 7: JSON document specifying content-based rules
for the application.
Links to evidence or supplementary information
are highlighted. When clicked on, they bring up a
browser to display the evidence or supplementary
information. CANBeWell has built-in multi-lingual
support and is currently available in both English and
French. The content is classified based on Button
clicked, Topic heading, Subject, Patient test, Provider
test, Gender and Age range (Minimum, Maximum).
The topics or tests from the appropriate JSON file
(based on language) are filtered based on patient vs
provider, gender and age. When using the Body tab,
the list is further filtered to only include those
corresponding to the button clicked.
HEALTHINF 2020 - 13th International Conference on Health Informatics
526
The .json files (figure 7) used in the CANBeWell
app are generated from the Excel Spreadsheet. First,
macros are used to scan the file and check for any
formatting errors, missing values, and incorrect
values (gender or age out of range, incorrect button
label, etc.).
5 DISCUSSION
CANBeWell app has gone through several iterations
of testing, including two third-party assessments by
healthcare app usability experts. It is now undergoing
a research trial with 30 patients and 10 providers,
which will provide quantitative and qualitative
feedback on usability being carefully monitored as
they use the application.
Enumerated below are some of the strong features
of the application.
▪ Bilingual support (currently supports English and
French).
▪ Optimized for smartphones but runs on any device
(laptop, tablet, smart TV, cell phones) with a
browser.
▪ Body image interface.
▪ Separately and optimally worded text for both
patients and providers.
▪ Easy Filtering and Navigation (body parts, age,
gender, health topics, common tests, patient vs
provider text)
▪ Use of embedded images and supporting links in
the content.
▪ Additionally, the current integration of the app has
support for content management by the medical
expert.
The first iteration of the application was hardcoded as
a native android app. The content was communicated
to developers in documents, but they were
responsible for manually coding the content into the
application.
This approach gave great flexibility in being
creative in how to display the content, but it was not
practical since changes to the content requires code
changes and redeployment of the application.
Especially, since evaluations by usability experts
indicated that consistency and predictability in how
content was displayed in the application were better
overall in terms of usability for the end-user.
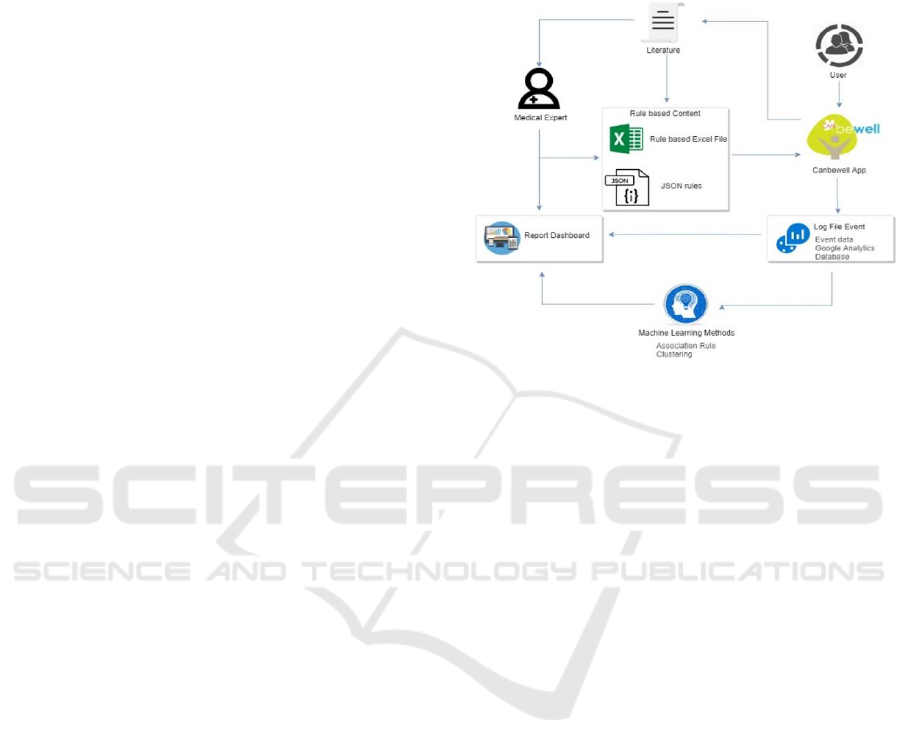
The latest iteration of the app is based on the
operational model depicted in figure 8. In this
iteration, the rule-based content framework was
completed. This new version achieves the desired
consistency and flexibility as required by the medical
experts. Most importantly, occasional errors in the
spreadsheet maintained by the medical expert are
easily identified and fixed. Changes were easily made
by simply editing the spreadsheet and regenerating
the .json files.
Figure 8: The operational model.
6 EVALUATION
CanBeWell was evaluated in an Urban Academic
Family Practice in Ottawa through a usability survey.
The survey is adapted from the System Usability
Scale (SUS) and administered as an online
questionnaire to 22 respondents (16 patients and 6
providers). The respondents were allowed a period of
1 month to use the app before they are allowed to
complete the usability survey.
These respondents range from 28 to 64 years old,
with average and median ages of 45 and 40
respectively. The mean age for patients and providers
was 46.6 (25-70) and 32.5 (27-46) respectively. All
the respondents used smartphones – 46% iPhones and
54% android phones. A survey was administered to
these users on the usability of the application.
Answers were scaled from Strongly Disagree to
Strongly Agree (5 Steps).
As shown in Figure 9, the responses show that the
biggest strengths of the app centres around ease of
use. The respondents are confident that they can use
the app, they found it simple to use and follow, and
would even recommend it to their families and
friends. The biggest negative is that most respondents
would not use the app often. They also didn’t feel
enthused with recommending the app to their
healthcare provider.
A Rule-based Content Management Framework for Effective Development of Intelligent Mobile Apps in Healthcare
527
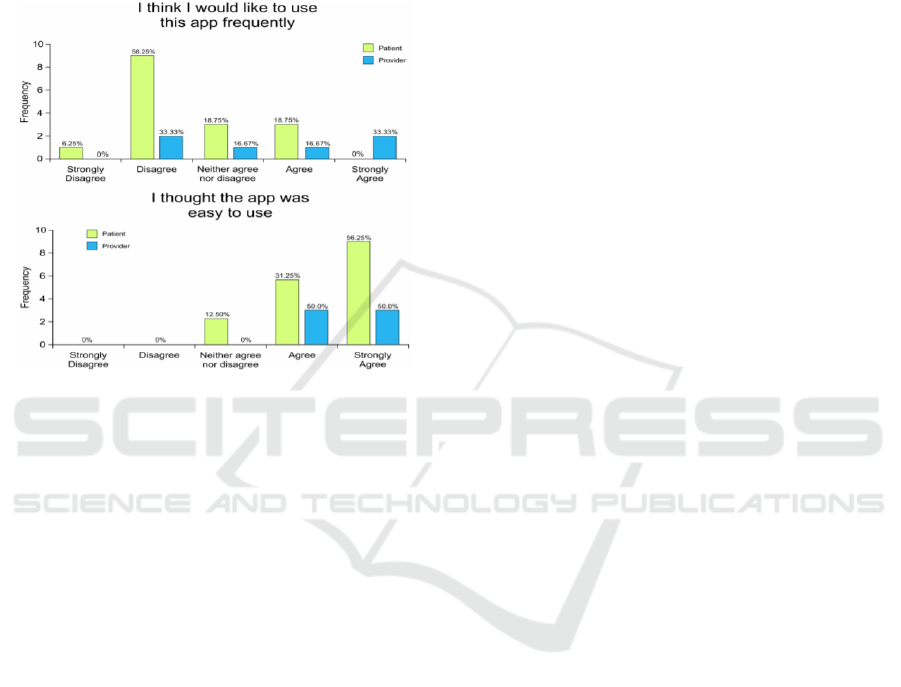
While we couldn’t be very conclusive on these
results because of the small number of respondents, it
points to some areas of improvement with the depth
of content that should be made available to the users.
With more content, users are more likely to use the
app more frequently and with increased use, it would
start coming up at discussions with their healthcare
providers.
Figure 9: User survey responses analysis.
7 CONCLUSIONS AND FUTURE
WORK
It is important to provide researchers and healthcare
experts a platform for managing content in a
systematic manner using tools they are familiar with.
Equally vital is the ability to update the healthcare app
without requiring developer intervention.
The CANBeWell app has the potential to greatly
improve the ability of patients and physicians to stay
current with the latest medical advice on wellness.
The app is easy to use in both English and French and
provides personalized content based on the age and
gender of the user and whether they prefer content
designed for patients or for physicians. More
importantly, the approach to content management is
practical and sustainable allowing the medical
expert(s) to manage the content on their own.
In the future, we plan to include a number of
improvements. We would like to provide the medical
expert with an easy to use HTML interface that allows
the medical expert to use the exact same rule-based
content management that is used now, but with an
interface that can provide immediate rule and content
verification, and optimized support during data entry.
It would also store the content directly into JSON
format so that the effects of the changes can be seen.
We would also like to instrument the application
with clickstream logging and IP address logging. This
will allow us to collect and analyze statistics to see
which content is being accessed, how often, by whom
based on geography, age, and gender.
It would also be useful to have a utility that
constantly monitored all the links to supporting
evidence embedded in the content. A report could be
sent to the medical expert(s) any time a link broke
(supporting evidence no longer available) or the
content referred to by the link changed (update to the
supporting evidence).
Finally, it would be advantageous to link this
development with a news service that monitored and
classified new developments in wellness research and
organized them as a service to the medical expert(s)
maintaining the application.
ACKNOWLEDGEMENTS
This research was funded by an NSERC Discovery
grant and an NSERC CREATE grant.
REFERENCES
Anderson M. (2015). Technology device ownership: 2015.
Retrieved from
http://www.pewinternet.org/2015/10/29/technology-
device-ownership-2015/. Accessed 28 April 2019.
Barbara, A. M., Dobbins, M., Haynes, R. B., Iorio, A.,
Lavis, J. N., Raina, P., & Levinson, A. J. (2017).
McMaster Optimal Aging Portal: an evidence-based
database for geriatrics-focused health professionals.
BMC research notes, 10(1), 271.
Beatty, D. and Lopez-Benitez, N. (2012). Rule-based
Management of Large Unorganized Data Sets.
Information Technology: New Generations (ITNG),
International Conference on Technology- New
Generations, pp.835-838.
Benferdia, Y., & Zakaria, N. (2014). A Systematic
Literature Review of Content-Based Mobile Health.
Journal Of Information Systems Research And
Innovation.
Boulos, M. N. K., Wheeler, S., Tavares, C., & Jones, R.
(2011). How smartphones are changing the face of
mobile and participatory healthcare: an overview, with
example from eCAALYX. Biomedical engineering
online, 10(1), 24.
Brewer, E., Katz, R., Amir, E., Balakrishnan, H., Chawathe,
Y., Fox, A., Gribble, S., Hodes, T., Nguyen, G.,
Padmanabhan, V., Stemm, M., Seshan, S. and
Henderson, T. (1998). A Network Architecture for
HEALTHINF 2020 - 13th International Conference on Health Informatics
528

Heterogeneous Mobile Computing. IEEE Personal
Communications, 5(5), pp.8-24.
Buyukkokten, O., Kaljuvee, O., Garcia-Molina, H.,
Paepcke, A. and Winograd, T. (2002). Efficient web
browsing on handheld devices using page and form
summarization. ACM Transactions on Information
Systems, 20(1), pp.82-115.
Chang, S., Zhong, C. and Kumar, R. (2001). Real-Time
Content-Based Adaptive Streaming of Sports Videos.
Conf.Workshop Content-Based Access of Image and
Video Libraries, (1), pp.139-146.
Cleland, I., Rafferty, J., Synnott, J., Cundell, J., Boyd, A.,
Nugent, C., ... & Burns, S. (2017, November). A
Holistic Technology-Based Solution for Prevention and
Management of Diabetic Foot Complications. In
International Conference on Ubiquitous Computing and
Ambient Intelligence (pp. 453-465).
Deek, H., Hamilton, S., Brown, N., Inglis, S. C.,
Digiacomo, M., Newton, P. J., ... & FAMILY Project
Investigators. (2016). Family‐centred approaches to
healthcare interventions in chronic diseases in adults: a
quantitative systematic review. Journal of advanced
nursing, 72(5), 968-979.
Eng, D., & Lee, J. (2013). The Promise and Peril of Mobile
Health Applications for Diabetes and Endocrinology.
Pediatric Diabetes, 14(4), 231-238. doi:
10.1111/pedi.12034
Fox S. and Duggan M. (2012). Mobile health 2012.
Retrieved from http://www.pewinternet.org/
2012/11/08/mobile-health-2012/. Accessed 28 April
2019.
Gunaratnam, M., Frize, M., & Bariciak, E. (2012).
Conceptual Framework for A Perinatal Decision
Support System using a Knowledge-Based Approach.
CMBES Proceedings, 35.
He, J., Gao, T., Hao, W., Yen, I. and Bastani, F. (2007). A
Flexible Content Adaptation System Using a Rule-
Based Approach. IEEE Transactions on Knowledge
and Data Engineering, 19(1), pp.127-140.
Kalimullah K, Sushmitha D (2017) Influence of design
elements in mobile applications on user experience of
elderly people. Procedia Comput Sci 113:352–359.
Khan Pathan, A. and Buyya, R. (2012). A Taxonomy
and Survey of Content Delivery Networks.
Krebs P., Duncan, D.T. Health App Use Among US Mobile
Phone Owners: A National Survey JMIR Mhealth
Uhealth 2015;3(4):e101
Kuo, K., & Fuh, C. (2009). A Rule-Based Clinical Decision
Model to Support Interpretation of Multiple Data in
Health Examinations. Journal Of Medical Systems,
35(6), 1359-1373.
Larsson, M. (2013). Traceability in Healthcare Innovation
Maintaining the Relations Between Needs and
Solutions.
Handel, M.J., "mHealth - using apps for health and
wellness." EXPLORE: The Journal of Science and
Healing 7.4 (2011)
Mohan, R., Li, C. and Smith, J. (2019). Content adaptation
framework: bringing the Internet to information
appliances. Global Telecommunications Conference,
1999. GLOBECOM '99, 4, pp.2015-2021.
Jokela, T., Iivari, N., Matero, J., & Karukka, M. (2003). The
standard of user-centered design and the standard
definition of usability. Proceedings Of The Latin
American Conference On Human-Computer
Interaction - CLIHC '03. doi: 10.1145/944519.944525
J. Zhang, T. R. Johnson, V. L. Patel, D. L. Paige, and T.
Kubose, "Using usability heuristics to evaluate patient
safety of medical devices," /. Biomed. Inform., vol. 36,
no. 1-2, pp. 23-30, Feb. 2003.
Yen, P.Y. and Bakken S., "Review of health information
technology usability study methodologies.," J. Am.
Med. Inform. Assoc., vol. 19, no. 3, pp. 413-22, Jan.
2012.
Smith A. (2015). U.S. smartphone use in 2015. Retrieved
from http://www.pewinternet.org/2015/04/01/us-
smartphone-use-in-2015/. Accessed 26 April 2019.
Ginossar, T., Shah, S. F. A., West, A. J., Bentley, J. M.,
Caburnay, C. A., Kreuter, M. W., & Kinney, A. Y.
(2017). Content, usability, and utilization of plain
language in breast cancer mobile phone apps: a
systematic analysis. JMIR mHealth and uHealth, 5(3).
Wald, H. S., Dube, C. E., & Anthony, D. C. (2007).
Untangling the Web—The impact of Internet use on
health care and the physician–patient relationship.
Patient education and counseling, 68(3), 218-224.
Wang, F. (2007). A Contextualization Method of Browsing
Events in Web-based Learning Content Management
System for Personalized Learning. Seventh IEEE
International Conference on Advanced Learning
Technologies (ICALT).
Widmer, R., Collins, N., Collins, C., West, C., Lerman, L.,
& Lerman, A. (2015). Digital Health Interventions for
the Prevention of Cardiovascular Disease: A
Systematic Review and Meta-analysis. Mayo Clinic
Proceedings, 90(4), 469-480. doi: 10.1016/j.mayocp.
2014.12.026
Yang, Y. and Silverman, R. (2014). Mobile health
applications: the patchwork of legal and liability issues
suggests strategies to improve oversight. Health
Affairs, 33(2), 222-2277.
A Rule-based Content Management Framework for Effective Development of Intelligent Mobile Apps in Healthcare
529
