
Development of Health Software using Behaviour Driven
Development - BDD
Mohammad Z Anjum
1a
, Silvana Togneri Mac Mahon
1b
and Fergal McCaffery
2c
1
Regulated Software Research Centre, Dundalk Institute of Technology, Co. Louth, Ireland
2
School of Computing, Dublin City University, Dublin 9, Ireland
Keywords: Automated Acceptance Testing, Requirement Engineering, Behaviour Driven Development, BDD, Software
Requirements, Medical Software, Health Software.
Abstract: The health software industry is facing an immense challenge of managing quality and preventing software
failures. Poorly defined requirements are one of the significant cause of health software failures. Agile
practices are being increasingly used by the software industry to develop systems on time and within budget
with improved software quality and user acceptance. Behaviour-driven development (BDD) is an agile
software engineering practice that can help to improve health software quality vastly. BDD achieves this by
prioritising the illustration of software’s behaviour using ubiquitous language, followed by automated
acceptance testing to assess if the illustrated behaviour was achieved. This paper presents a review of BDD
literature, including the characteristics of BDD and examines how BDD can benefit health software quality.
The paper reviews health software standards and guidelines, to examine their compatibility with a BDD
approach. Finally, the paper details future plans for the development of a framework that provides health
software companies with a detailed step by step guideline on how to use BDD to develop safer health software.
1 INTRODUCTION
The software has become an imperative component
of medical devices to provide additional functionality
(PTC, 2012). Because of the increasing complexity
and reliance on software, the health software industry
faces an immense challenge of managing quality and
reducing defects (Ronquillo, J. G. et al. 2017). The
Food and Drug Administration (FDA) in the USA and
European Commission for medical devices in Europe
ensures patient safety by reviewing health software
products and recalling them if the products do not
meet the standards set by them (Zuckerman, D. M. et
al., 2011).
A study analysing computer-based failures in
medical devices reports that 2,303,441 recalls of
medical devices out of 12,024,836 were related to
software. Software issues accounted for 33.3% of
class I recalls, 65.6% of class II recalls, and 75.3% of
class III recalls (Alemzadeh, H. et al., 2013). Poorly
defined requirements are one of the most significant
a
https://orcid.org/ 0000-0003-2511-3047
b
https://orcid.org/ 0000-0003-0179-2436
c
https://orcid.org/ 0000-0002-0839-8362
causes of software failures (Ward, j. et al., 2003).
Inadequate time and effort are spent on the
requirements-related activities (FDA - medical
device recall report, 2013).
To minimise software failures, different software
engineering methodologies/practices have been
introduced. A software engineering methodology is a
framework used to structure, plan, and control the
process of developing software. Software engineering
methodology also comprises of different levels of
software quality assurance (SQA) activities. SQA
activities range from requirements engineering to
testing and inspections (Tian, J. 2005). Behaviour-
driven Development (BDD) is an agile software
engineering practice that encourages collaboration
between technical and non-technical stakeholders to
ensure that all relevant requirements are captured and
mutually agreed. (Smart, J. F. et al., 2015).
Although there have been misconceptions about
the suitability of the use of agile methods in safety
critical domain including health software, recent
Anjum, M., Mahon, S. and McCaffery, F.
Development of Health Software using Behaviour Driven Development - BDD.
DOI: 10.5220/0008984201490157
In Proceedings of the 8th International Conference on Model-Driven Engineering and Software Development (MODELSWARD 2020), pages 149-157
ISBN: 978-989-758-400-8; ISSN: 2184-4348
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
149

research has proved agile methods can be adapted to
the unique needs of health software and can be very
valuable for the development of high-quality health
software (AMMI, 2012). BDD focuses on
requirements engineering to generate tests cases by
illustrating software behaviour and then producing
automated acceptance tests (Egbreghts, A. 2017).
This paper considers how different BDD practices are
used to improve software quality and user acceptance.
The paper also considers how these practices can be
used in the health software domain, including for
medical device software development.
BDD is a software engineering practice invented
by Dan North in the early to mid-2000s to transform
Test-Driven Development -TDD into a more efficient
software development process . BDD draws on agile
and lean practices, in particular, TDD and Domain-
Driven Design DDD, (Solis, C. 2011).
1.1 Test-Driven Development - TDD
TDD is a software development practice that uses a
‘test first’ approach; it involves writing tests before
writing the code that is being tested. TDD relies on
the repetition of a very short development cycle.
Requirements are turned into specific test cases
(Smart, J. F. et al., 2015).
1.2 Domain-Driven Design (DDD)
DDD is an approach to the development of software
in which the focus is on the core domain in this case,
health software development. DDD is about making
the software a model of a real-world or process. In
DDD, developers work closely with a domain expert,
i.e., compliance manager or healthcare professional,
who explains how the real-world system works in his/
her domain. A ubiquitous language (UL) is used to
build a common language, to develop a conceptual
description of the system between the developer and
the domain expert (Evans, E. 2014).
This paper is structured as follows. Section 2
explains what BDD is. Section 3 discusses the
existing literature of behaviour-driven development.
Section 4 discusses health software standards and
guidelines. Section 5 discusses BDD for health
software and outlines plans for future work in this
area and Section 6 summary & conclusion.
2 BEHAVIOUR-DRIVEN
DEVELOPMENT
The objective of BDD is to create executable and
well-defined specifications of the software. The BDD
process can be divided into three stages.
Stage 1 - Three or more team members, a business
analyst or product owner, a developer and a tester;
known as the “Three Amigos.” will meet to discuss a
feature and write up examples. By getting these three
individuals to discuss features at the start ensures
clear requirements specification are generated.
This is because:
•The Product owner, e.g., Medical device
manufacturer, compliance manager or health expert
will have the domain knowledge to judge the
relevance of the different scenarios.
•The developer will ensure technical considerations.
•The tester, with a focus on validation, will be able to
suggest test cases and point out scenarios that the
other team members have overlooked.
This exercise enables the developer to have a deeper
understanding of the business requirements.
Stage 2 – The examples are converted into scenarios,
which are more structured to allow them to be
automated in the form of automated acceptance tests.
Stage 3 - The developers will use the TDD approach,
as discussed in section 1.1 to write the code required
to make this acceptance test pass (Smart, J. F. et al.,
2015).
These three Stages are discussed below in further
detail. Section 2.1 discusses Stages 1 and 2, and
Section 2.2 discusses Stage 3.
2.1 Requirements Capturing &
Specification
BDD offers a specification technique. It supports
continuous requirements engineering with the use of
stories. These stories help to specify executable
requirements in a natural language format using UL
(I. Lazǎr et al., 2010). Executable requirements act as
live documentation, making it easier to receive
feedback early and conduct acceptance tests. The UL
is used to write stories and scenarios and can guide
the developers in understanding what feature/
behaviour are needed to be implemented (Kenneth P.
2011).
2.1.1 Ubiquitous Language (UL)
Requirements are interpreted by the developers and
testers to produce software and test scripts. However,
different people interpret complex concepts
MODELSWARD 2020 - 8th International Conference on Model-Driven Engineering and Software Development
150

differently (Evans, E. 2014). Therefore, by using
ubiquitous language, BDD helps stakeholders to
understand functional specifications. UL allows
requirements to be consistent and readable to all,
which minimises the possibility of misunderstanding.
The UL used by BDD is referred to as Gherkin syntax
and is used by the BDD tool Cucumber. However,
JBehave, which is also a BDD tool, that has its own
syntax, was developed separately and has some
differences (Egbreghts, A. 2017).
2.1.2 Behaviour Illustration
According to Liz Keogh, a core member of the BDD
community and a contributor to some open-source
projects including J-Behave, ‘BDD is the art of using
examples in conversation to illustrate behaviour’. In
BDD, examples and conversation are used to discover
and describe the behaviour of the system. Using
conversation and examples to specify how you expect
a system to behave is a core part of BDD (
Keogh L.
2012). Examples are used by BDD to specify
scenarios. These examples can be used as a tool to
express and discuss business needs and expectations,
and they make it much easier to clear
misunderstandings (Solis, C. et al., 2011). These
BDD requirements tracing & specification techniques
can assist health software development companies, to
understand complex requirements, including
regulatory requirements more effectively. Once
requirements are defined, and the acceptance test is
written using ubiquitous language, the test is then
automated using BDD automation tools.
2.2 Automated Acceptance Testing
In BDD automation for acceptance test is achieved
through the tools like Cucumber, JBehave, SpecFlow,
frameworks, and test suites automation. BDD tools
allow scenarios to be run automatically and use UL
using “Given, When, Then” format. (Solis, C. et al.,
2011). Time to market has become key even in safety
critical domains and demand for implementing
continuous integration, and continuous delivery has
increased. Automated acceptance testing makes
continuous delivery possible. As new releases can be
deployed with low risk of introducing regression (G.
Lucassen. et al., 2017).
This section discussed requirements capturing &
specification techniques used in BDD as well as
automated acceptance testing. The next section
discusses state of the art, the existing literature of
behaviour-driven development and the use of
behaviour-driven development, particularly in the
safety-critical domain.
3 STATE OF THE ART – THE USE
OF BDD
This section discusses the existing literature of BDD
in safety-critical domains. It is to be noted that despite
it being an established practice in the software
industry, the academic literature of BDD is still
limited (Egbreghts, A. 2017) especially for safety-
critical domains.
C. Baillon and S. Bouchez-Mongardé conducted
a study and published their work in 2010 on
executable requirements in a safety-critical context.
They mention different characteristics of BDD as a
potential solution to a number of modern software
industry problems. The study also proposes that BDD
practices can be used to address challenges facing in
the safety-critical domain by legacy software. Legacy
software are often critical to the companies and over
the years have been maintained by a number of
programmers. Which means that many changes have
been made to the software but the supporting
documentation may not be up-to-date. The authors’
study proposes using BDD and executable
requirements to build a step-by-step understanding of
untested legacy software’s behaviour (C. Baillon et
al., 2010).
Similarly, in 2011, a systematic mapping study of
requirements specification and testing techniques
mention BDD as a new development paradigm to
address requirements traceability problems
(Egbreghts, A. 2017).
Diepenbeck and Kühne published a paper in 2015
on behaviour driven development for tests and
verification. They proposed BDD for design and
verification for safety critical hardware systems.
They introduced a new element for defining
properties called natural language and supported the
assembling of ‘property specification language’.
They presented an example of a BDD based flow that
combines testing and verification using natural
language tests and properties as a starting point for
the design of the hardware.
In 2017 Hatko, Mersmann, and Puppe published
their work where they have described an approach
inspired by BDD for specification and analysis of
Computer-Interpretable Clinical Guidelines (CIG).
These requirements, where stated by medical experts
in natural language and are used as design input for
the development of CIGs and their analysis using test
Development of Health Software using Behaviour Driven Development - BDD
151

cases. The paper demonstrated the applicability of
BDD for CIGs. They concluded the approach had
shown its applicability regarding usability and
expressiveness (Hatko, R., et al., 2014).
The above literature demonstrates the benefit of
using BDD, especially its requirement engineering
and automated acceptance testing approach. The
literature exhibits the potential benefit of using BDD
practices in safety critical domain. It also highlights
the need for further research in this area of safety
critical domains, including medical devices. The
literature also shows how particular BDD practices
can be used instead of the complete BDD
methodology to achieve the desired results.
This section discussed the existing literature of
behaviour-driven development in the safety-critical
domain. The next section looks at relevant health
software standards & guidelines to be considered in
order to use BDD to develop health software.
4 HEALTH SOFTWARE
REGULATION & BDD
There are a number of different standards and
guidelines from government and non-government
organisations to ensure standardisation and to
regulate the quality of safety-critical software. This
also applies to the safety of medical devices software.
Many standards are harmonised between USA and
EU via “recognised consensus standards” in the USA
(U.S. FDA) and European directives in the EU
(European Commission). To meet the regulatory
requirement, health software developers and medical
device manufacturers must understand what the
regulators are assessing. Two standards, one
guideline and technical information report have been
identified as relevant to this research.
These standards, guideline and technical
information report, listed below are primarily aimed
at health software developers, including medical
devices companies to assist them in understanding if
their product is designed with safety in mind
(Zuckerman, D. M., Brown, P., & Nissen, S. E. 2011).
a) IEC 62304 – Software Life Cycle Processes
The international standard IEC 62304 – medical
device software – software life cycle processes (IEC,
2015). This standard harmonised by the EU and the
FDA and can be used to ensure compliance for both
the EU and the USA market.
b) IEC 82304-1 Health Software Product
Processes
The international standard IEC 82304-1 deals with
general requirements for safety and security of ‘health
software products’. IEC 82304-1 inherits quite a lot
of its characteristics from IEC 62304 and refers to
health software products companies back to IEC
62304 (C. Michaud, 2016). The main reference is in
section 5 of IEC 82304-1 titled health software -
software lifecycle process.
c) FDA General Principles of Software
Validation; Final Guidance for Industry and FDA
Staff (GPSV)
GPSV is the guidance on general validation principles
that, the FDA considers to be applicable to the
validation of medical device. This guidance describes
FDA approach to evaluating a software validation
system.
d) AAMI - TIR45 - Guidance on the Use of Agile
Practices in the Development of Medical Device
Software
This Technical Information Report (TIR) provides
recommendations for complying with international
standards and FDA when using agile practices for the
development of medical device software.
The remaining of section 4 discusses these
standards and guidelines’ requirements compared
with the BDD’s practices.
4.1 Health Software Requirements
Poor software requirements are one of the main
reason for the failure of health software devices, as
discussed in section 1 of this paper. The both IEC
62304 & IEC 82304 – 1 put great emphasis in health
software requirements, particularly in section 5.2 of
IEC 62304 and section 4 of IEC 82304-1. As
discussed in section 3 of this paper, the BDD’s
requirements tracing and specification techniques
that result in stories are the key to BDD’s success.
These techniques can be aligned with the
requirements elicitation stages defined in section 5.2
of IEC 62304 and section 4 of IEC 82304-1. Below is
a list of individual requirements elicitation stages
from the two standards and how BDD aligns to the
requirements of these stages.
a) Requirements Gathering
Requirements gathering is discussed in detail in
section 5.2.2 of IEC 62304 (IEC, 2015) and section
4.2 IEC 82304-1 (IEC, 2017). Both of these standards
require different aspects of software requirements for
medical devices to be determined and documented
including functional and capability requirements,
software system inputs and outputs requirements,
interfaces between the software system and other
systems, security requirements and data definition
and database requirements to name a few. J. Ferguson
MODELSWARD 2020 - 8th International Conference on Model-Driven Engineering and Software Development
152
Smart, in his book ‘BDD in action’, explains that
product owner, along with the team will collectively
define requirements in amigos meetings as users’
stories for requirements gathering in BDD process
(Smart, J. F. et al., 2015). This can include
requirements required by these standards.
b) Risk Assessment
Risk Assessment is the section 5.2.3 and 5.2.4 of IEC
62304 and section 4.1 IEC 82304-1. The IEC 62304
asks the manufacturer to implement risk control
measures but leaves it up to the manufacturer to
decide how. IEC 62304 also requires the
manufacturer to re-evaluate the medical device risk
analysis after the software requirements are
established and updated (IEC, 2015). The TIR45
proposes elaborated stories to define risk
requirements and prioritising these stories in the
development of backlog (AMMI, 2012).
c) Verification of Requirements
Verification of Requirements is the section 5.2.6 of
IEC 62304 and section 4.3 IEC 82304-1. IEC 82304-
1 requires for four things at this stage; requirements
should not contradict each other, avoid ambiguity;
permit the establishment of test criteria, uniquely
identified (IEC, 2017). As discussed in section 2.1.1
of this paper by defining the requirements in UL,
BDD addresses all four of these requirements (IEC,
2017).
d) Updating Requirements
Updating requirements is the section 5.2.5 of IEC
62304 and section 4.4 IEC 82304-1. Backlog
refinement is a BDD activity, which addresses
updating requirements (AMMI, 2012). IEC 62304
asks the manufacturer to ensure that existing
requirements are re-evaluated and updated as
appropriate as a result of the software requirements
analysis activity (IEC, 2015). Similarly, the IEC
82304-1 asks the manufacturer to ensure that the
health software product use requirements are updated
as appropriate, e.g., as a result of health software
product use requirements verification or as a result of
validation (IEC, 2017).
In BDD, the process of backlog refinement allows
the team to remove user stories that are not
appropriate anymore, as well as defining new user
stories if new requirements have surfaced. The next
section discusses risk management while using BDD
to develop health software.
4.2 Risk Management for Health
Software with BDD
Regulations require medical device companies to
follow a robust set of human safety risk management
activities in their product development. Such
activities include risk planning, risk analysis, risk
control identification, and risk control verification.
The documentation and approval activities should be
in place in accordance with the organisation’s quality
management system. In the case of health software
companies the ISO 13485, medical devices - quality
management systems is the regulatory standard that
can be used as the organisation’s quality management
system.
A backlog can be considered as a ‘to-do list’ that
details specific outcome based on proposed features,
changes to the existing features and the infrastructure,
as well as software bugs that need addressing. The
backlog allows the team to ensure that they are only
using one authoritative source of ‘to-do list’.
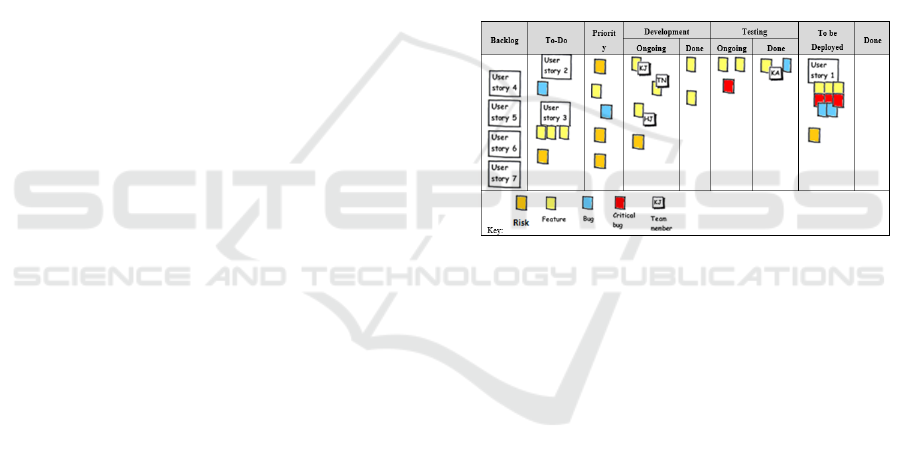
Table 1: Example backlog board with priority column and
risks.
The backlog board in table 1 shows an illustration of
proposed health software backlog. Two new columns
‘priority’ and ‘to be deployed’ has been added to
satisfy the requirements of the standards discussed
above. The illustration also uses a different colour to
identify different tasks. For example, risks are
identified in orange colour on the backlog board, and
risk management policy can be used to ensure that the
team always prioritise risk on the backlog board.
A similar approach was discussed by G. K Hanssen
and T. Stalhane in SafeScrum – Agile Development
of Safety-Critical Software.(Hanssen. G. K. et al.,
2018).
The nature of health software is safety critical and
does not always allow the software to release as
frequently as non-safety critical software (AMMI,
2012). The backlog board’s ‘to be deployed’ column
allows teams to use the column as a place holder until
it is considered safe to release the iteration. Similarly,
what is classed, as ‘done’ for stories of health
software has to be more defined and detailed. For this
reason, the DoD for health software requirements
must be defined as part of the requirement elicitation
process. The following section of this paper discusses
this further.
Development of Health Software using Behaviour Driven Development - BDD
153

4.3 Definition of Done (DoD) for
Health Software Requirements
A doneness policy & procedure can be created to help
define what will be classed as ‘done’ for a health
software story and the individuals that will need to
sign off on doneness. These doneness policies &
procedures are known as DoD, a set of criteria which
must be met before a software item is considered to
be complete. The DoD is agreed upon by the
development team and the product owner. The DoD
can be used at various points in a development
project; for example, a DoD can be created to ensure
a software system is complete, or to ensure a software
requirement is complete. Part of the doneness policy
& procedure will be to verify and validate the story to
assess the doneness. This is done using a number of
different verification and validation techniques.
This section discussed the health software
regulations with respect to how BDD can be used and
adapted to develop safer health software. The
following section proposes a framework for health
software development using BDD characteristics
discussed in this paper.
5 BDD FOR HEALTH SOFTWARE
This section of the paper will focus on outlining an
approach to the development of a behaviour-driven
health software framework (hBehave), as the solution
for the problems detailed in this paper. This section
will also discuss, how this framework will be
validated. As discussed in section 1 agile practices
including BDD despite being very successful in non-
health industry are rarely used in medical software
development , because of health software companies
uncertainty around losing their certification by
changing their practices (AMMI, 2012) (Clarke, P. et
al., 2014).
The framework will provide health software
companies with detailed step by step guideline on
how to use BDD to develop health software. The
framework will also detail how to adapt BDD to
satisfy different health software regulations. The aim
of the hBehave framework will be to act as a
handbook for health software companies to help
migrate their development process to BDD. It will be
broken down into different processes derived from
IEC 62304 and agile software development life cycle
as detailed in AMMI TIR45 (AMMI, 2012). The
remaining section of this paper discusses different
aspects of the hBehave framework including the
framework processes, processes table structure and
framework validation.
5.1. Behaviour-Driven Health Software
Framework – hBehave
The framework processes detailed below derive from
IEC 62304, figure 1, software development processes
and activities.
5.1.1 Framework Processes
a) Development Planning
Development Planning is the first activity according
to software development processes and activities
defined in figure 1 of IEC 62304 – Medical device
software – software life cycle processes (IEC, 2015).
Development planning is also the first activity of each
layer of software development in BDD / agile
development as detailed in AMMI TIR45 in figure 4
(AMMI, 2012). The development planning is
performed at each layer of the BDD development,
including project, release, increment, and story layer
(AMMI, 2012). The main activities and output of this
process of the framework will be the development of
a backlog board, unique for each project and project
policies and procedures including the definition of
done.
b) Requirement Elicitation
Requirement elicitation is the 2nd activity according
to software development processes and activities
defined in figure 1 of IEC 62304 – Medical device
software – software life cycle processes titled as
requirement analysis (IEC, 2015). Requirement
elicitation is also the 2nd activity of project and story
layer of software development in BDD / agile
development as detailed in AMMI TIR45 in figure 4
(AMMI, 2012). The main activities and output of this
process of the framework are requirement discovery,
requirement definition and formation of
requirements.
c) Software Architecture & Design
Software Design covers 3rd and the 4th activities in
software development processes and activities
defined in figure 1 of IEC 62304 – Medical device
software – software life cycle processes titled as
software architectural design and software detailed
design (IEC, 2015). Software design is also the 3rd
activity of project layer of software development in
BDD / agile development as detailed in AMMI TIR45
in figure 4; labelled as infrastructure spikes. Spikes
are stories that will result in the team learning,
prototyping, and ultimately developing execution
strategy. Software emergent, the 3rd activity of the
MODELSWARD 2020 - 8th International Conference on Model-Driven Engineering and Software Development
154

story layer and as software detailed design, the 4th
activity of the story layer (AMMI, 2012).
d) Unit Implementation & Verification
Unit implementation & verification is the 5th activity
in software development processes and activities
defined in figure 1 of IEC 62304 – Medical device
software – software life cycle processes (IEC, 2015).
This activity is also the 5th activity of story layer of
agile development life cycle as detailed in AMMI
TIR45 in figure 4 (AMMI, 2012). This process of the
framework will follow the test-driven development –
TDD’s approach and main activities and output of
this process are unit implementation (TDD), unit
testing (TDD) and refactoring (TDD).
e) Software Integration & Integration Testing
Software integration & integration testing is the 6th
activity in software development processes and
activities defined in figure 1 of IEC 62304 – Medical
device software – software life cycle processes (IEC,
2015). In BDD / agile development life cycle, the
Software integration & integration testing is
performed in release layer, increment layer as well as
story layer as detailed in AMMI TIR45 (AMMI,
2012).
f) System & Regression Testing
System testing is the 7th activity in software
development processes and activities defined in
figure 1 of IEC 62304 – Medical device software –
software life cycle processes (IEC, 2015). System &
regression testing is performed in release layer,
increment layer and the system testing is performed
story layer in BDD / agile development life cycle, as
detailed in AMMI TIR45 in figure 4 (AMMI, 2012).
g) Software Release
Software release is the 8th activity in software
development processes and activities defined in
figure 1 of IEC 62304 – Medical device software –
software life cycle processes (IEC, 2015). Software
release is performed in release layer of BDD / agile
development life cycle, as detailed in AMMI TIR45
in figure 4 (AMMI, 2012). The main activities and
output of this process of the framework are
automation of acceptance testing and generation of
living documentation.
This section detailed the processes for the
behaviour driven health software framework, as part
of the proposed future work. To continue the
development of the framework, our future work will
focus on further development of different aspects of
the hBehave framework. The future work will also
focus on validation of Behaviour-driven health
software framework. The research will consider the
following points in terms of the validation the
efficiency of proposed framework, the reliability of
proposed framework and ease of adaptability of
proposed framework.
Data will be requested from health software
companies to understand their existing software
development processes, in particular around
requirement engineering processes and acceptance
testing processes. After analysing this data, the
proposed hBehave framework will be revised to
reflect health software companies’ needs derived
from the data collected. The framework will then be
presented to health software companies for
implementation, and the results will be observed. This
method of validation will be used to assess the quality
of hBehave in terms of efficiency, reliability and
adaptability.
6 SUMMARY & CONCLUSION
In this paper, the software engineering practice BDD
was discussed. As well as how BDD practices can
help to address requirements related to health
software failure as identified in section 1. This paper
explained software quality problems in health
software. The benefits of behaviour-driven
development’s practices were outlined with the
empirical examples from the literature. BDD’s
practices can be used to address challenges such as
poorly defined requirements.
Section 4 of the paper identified two standards
IEC 62304 and IEC 82304-1, a guideline by FDA, the
GPSV and technical information report by AMMI,
the TIR45 as relevant to this research. Followed by,
the identified standards and guidelines were
discussed in detail along with BDD to established
BDD’s compatibility as a health software engineering
practice. The IEC 82304-1 is seen as a breakthrough,
as it works along IEC 62304 to provides the flexibility
needed by health software developers to use agile
approaches to develop software (C. Michaud, 2016).
Section 5 of this paper details future work,
including behaviour-driven health software
framework – hBehave, as the potential solution for
the problems detailed in this paper, as well as how this
proposed solution will be validated. The proposed
framework aims to provide health software
companies with detailed step by step guideline on
how to use BDD to develop safer health software.
In conclusion, our research findings show that
BDD has the potential as a health software
development technique. Furthermore, BDD’s
practices, in particular requirements tracing &
specification and automated acceptance testing, has
Development of Health Software using Behaviour Driven Development - BDD
155

the potential to address the research problem detailed
in section 1 of this paper. High-level mapping has
been done between Behaviour-driven health software
frameworks processes and IEC 62304 & IEC 82304,
which shows promising compatibility. However,
significant work has to be done to develop Behaviour-
driven health software framework and where required
adapt BDD to fulfil the regulatory requirements to
build confidence among health software companies.
ACKNOWLEDGEMENTS
This work was supported with the financial support
of the Science Foundation Ire-land grant 13/RC/2094
and co-funded under the European Regional
Development Fund through the Southern & Eastern
Regional Operational Programme to Lero - the Irish
Software Research Centre (www.lero.ie).
REFERENCES
PTC (2012). Software Development for Medical Devices,
Software Development for Medical Devices, PTC.
Ronquillo, J. G., & Zuckerman, D. M. (2017). Software-
Related Recalls of Health Information Technology and
Other Medical Devices: Implications for FDA
Regulation of Digital Health. The Milbank Quarterly,
95(3), 535–553. doi: 10.1111/1468-0009.12278
Zuckerman, D. M., Brown, P., & Nissen, S. E. (2011).
Medical device recalls and the FDA approval process.
Archives of Internal Medicine, 171(11), 1006–1011.
doi: 10.1001/archinternmed.2011.30
Egbreghts, A. (2017). A Literature Review of Behavior
Driven Development using Grounded Theory.
Medical Devices, European Commission (2019). Retrieved
from https://ec.europa.eu/growth/sectors/medical-
devices_en
Keogh L. It's about the examples you can't find, not the ones
you can. Liz Keogh, lunivore. https://lizkeogh.com/
2012/02/20/its-about-the-examples-you-cant-find-not-
the-ones-you-can/. Published February 20, 2012.
Accessed December 17, 2019.
Alemzadeh, Homa, et al. Analysis of Safety-Critical
Computer Failures in Medical Devices. IEEE Security
& Privacy, vol. 11, no. 4, 2013, pp. 14–26.,
doi:10.1109/msp.2013.49.
FDA - Medical Device Recall Report (2013). Retrieved
from http://www.fda.gov/downloads/AboutFDA/
CentersOffices/OfficeofMedicalProductsandTobacco/
CDRH/CDRHTransparency/UCM388442.pdf
Ward, j, Shefelbine, S., & Clarkson, P. J. (2003).
Requirements capture for medical device design. In
requirements capture for medical device design.
Martin, J., Murphy E.A., Crowe, J.A. and Norris B. (2006).
Capturing User Requirements in Medical Device
Development: The Role of Ergonomics, Physiological
Measurement 27(8) pp. R49-R62.
Smart, J. F., & North, D. (2015). Bdd in action: behavior-
driven development for the whole software lifecycle.
Shelter Island, NY: Manning.
G. Lucassen, F. Dalpiaz, J. M. E. M. van der Werf, S.
Brinkkemper and D. Zowghi. (2017) "Behavior-Driven
Requirements Traceability via Automated Acceptance
Tests," IEEE 25th International Requirements
Engineering Conference Workshops (REW), Lisbon,
2017, pp. 431-434.
Wallace, D. R., & Kuhn, D. R. (1999). Lessons from 342
Medical Device Failures. In Lessons from 342 Medical
Device Failures.
Ward, J. R., & Clarkson, P. J. (2004). An analysis of
medical device-related errors: prevalence and possible
solutions. Journal of Medical Engineering &
Technology, 28(1), 2–21. doi: 10.1080/
0309190031000123747
Tian, J. (2005). Software Reliability Engineering. Software
Quality Engineering, 371–387. doi: 10.1002/
0471722324.ch22
(AMMI, 2012), “Technical Information Report AAMI
TIR45 : Guidance on the use of AGILE practices in the
development of medical device software.
Evans, E. (2014). Domain-driven design reference:
definitions and pattern summaries. Indianapolis: Dog
ear publishing.
Solis, C., & Wang, X. (2011). A Study of the
Characteristics of Behaviour Driven Development.
2011 37th EUROMICRO Conference on Software
Engineering and Advanced Applications. doi:
10.1109/seaa.2011.76
Hatko, R., Mersmann, S., & Puppe, P. (2014). Behaviour-
driven development for Computer-Interpretable
Clinical Guidelines. In Behaviour-driven development
for Computer-Interpretable Clinical Guidelines (Vol.
1289).
I. Lazǎr, S. Motogna, and B. Pârv. (2010) “Behaviour-
driven development of founda-tional UML
components,” Electron. Notes Theor. Comput. Sci., vol.
264, no. 1, pp. 91–105, 2010.
Kenneth P. (2011), Lean-Agile Acceptance Test-Driven
Development: Better Soft-ware Through Collaboration.
C. Baillon and S. Bouchez-Mongardé. (2010). Executable
requirements in a safety-critical context with Ada,” Ada
User J., vol. 31, no. 2, pp. 131–135.
U.S. FDA. Recognized Consensus Standards. Retrieved
from https://www.accessdata.fda.gov/scripts/cdrh/
cfdocs/cfStandards/search.cfm
European Commission. Harmonised Standards - European
Commission. Retrieved from https://ec.europa.eu/
growth/single-market/european-standards/harmonised-
standards_en
IEC, (2015). “Medical device software — Software life-
cycle processes,” Bs En 62304-2006 +a12015, vol. 3,
no. November 2008, 2015.
IEC, (2017). BS EN 82304-1:2017 - Health Software -Part
1: General requirements for product safety BS,” 2017.
MODELSWARD 2020 - 8th International Conference on Model-Driven Engineering and Software Development
156

FDA, (2002) - General Principles of Software Validation;
Final Guidance for Industry and FDA Staff
C. Michaud, (2016) “IEC 82304-1 - Consequences on agile
software development pro-cesses - Software in Medical
Devices, by MD101 Consulting.” [Online]. Retrieved
from: https://blog.cm-dm.com/post/2016/04/08/IEC-
82304-1-Consequences-on-agile-software-
development-processes.
Hanssen. G Kjetil, Stålhane. T, Myklebust, T , (2018)
SafeScrum® – Agile Development of Safety-Critical
Software
Development of Health Software using Behaviour Driven Development - BDD
157
