
Privacy-preserving Metrics for an mHealth App in the Context of
Neuropsychological Studies
Alexander Gabel
1 a
, Funda Ertas
2 b
, Michael Pleger
1 c
, Ina Schiering
1 d
and Sandra Verena M
¨
uller
2 e
1
Faculty of Computer Science, Ostfalia University of Applied Sciences, Salzdahlumerstraße 46/48, Wolfenb
¨
uttel, Germany
2
Faculty of Social Work, Ostfalia University of Applied Sciences, Salzdahlumerstraße 46/48, Wolfenb
¨
uttel, Germany
Keywords:
mHealth, Data Minimization, Privacy by Design, Privacy by Default, Data Aggregation, Metrics,
Neuropsychology, Empirical Study.
Abstract:
The potential of smart devices as smartphones, smart watches and wearables in healthcare and rehabilitation,
so-called mHealth applications, is considerable. It is especially interesting, that these devices accompany pa-
tients during their normal life. Hence they are able to track activities and support users in activities of daily life.
But beside the benefits for patients, mHealth applications also constitute a considerable privacy and security
risk. The central question investigated here is how data about the usage of mobile applications in empirical
studies with mHealth technologies can be collected in a privacy-friendly way based on the ideas of Privacy
by Design. The context for the proposed approach are neuropsychological studies where a mobile application
for Goal Management Training, a therapy for executive dysfunctions, is investigated. There a privacy-friendly
concept for collecting data about the usage of the app based on metrics which are derived from research ques-
tions is proposed. The main ideas underlying the proposed concept are a decentralized architecture, where
only aggregated data is gathered for the study, and a consequent data minimization approach.
1 INTRODUCTION
The use of mobile applications in healthcare and reha-
bilitation has in general a huge potential. Especially
smart devices as smartphones, smart watches, smart
glasses and wearables are widely used in health-
related research projects in areas as diagnosis, therapy
and rehabilitation (Garcia-Ceja et al., 2016; Gr
¨
unerbl
et al., 2015; Jamieson et al., 2019). Since these smart
devices accompany patients in daily life, data about
the behavior of patients can be tracked and patients
could be supported in their daily activities or they can
be coached to lead a more healthy life.
But on the other hand in health apps substantial
security and privacy issues were detected (Papageor-
giou et al., 2018; Huckvale et al., 2015) and in studies
about willingness of users to share data (Di Matteo
et al., 2018; Beierle et al., 2019) users stated privacy
a
https://orcid.org/0000-0002-2660-4350
b
https://orcid.org/0000-0002-7940-1178
c
https://orcid.org/0000-0001-5398-3694
d
https://orcid.org/0000-0002-7864-5437
e
https://orcid.org/0000-0003-4450-9936
concerns, especially since data transfer and usage is
not sufficiently transparent.
Concerning privacy and data protection in the Eu-
ropean Union compliance with the General Data Pro-
tection Regulation (GDPR) (European Union, 2016)
is required. The basis of this regulation is summa-
rized in the principles of data protection in Article 5
of GDPR as lawfulness, fairness, transparency, pur-
pose limitation, data minimisation, accuracy, storage
limitation, integrity, confidentiality and accountabil-
ity.
A central approach to integrate privacy early in the
development process of new systems resp. services
are Privacy by Design and Privacy by Default. To
model privacy risks, privacy protection goals (Hansen
et al., 2015) confidentiality, integrity and availabil-
ity, transparency, unlinkability and intervenability are
helpful. To integrate privacy requirements in sys-
tem architectures privacy design strategies (Colesky
et al., 2016) summarizing the important concepts min-
imize, hide, separate, abstract, inform, control, en-
force, demonstrate can be used.
These Privacy by Design methodologies were
used in the context of the research project SecuRIn
166
Gabel, A., Ertas, F., Pleger, M., Schiering, I. and Müller, S.
Privacy-preserving Metrics for an mHealth App in the Context of Neuropsychological Studies.
DOI: 10.5220/0008982801660177
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 166-177
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
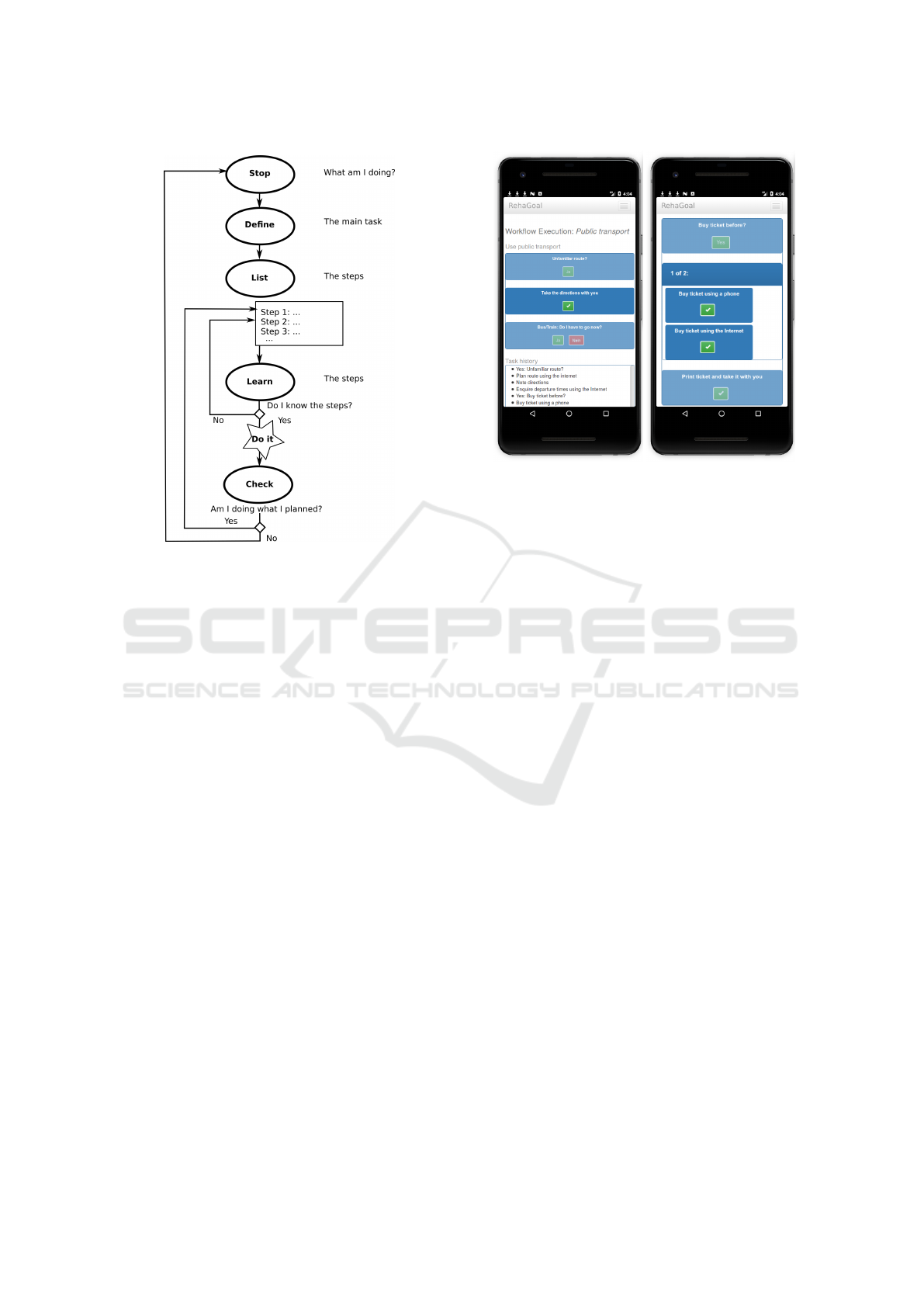
Figure 1: Goal Management Training.
where a mobile application for the so-called Goal
Management Training (GMT) (Figure 1) (Levine
et al., 2000; Bertens et al., 2013; Stamenova and
Levine, 2018), an important therapy for executive
dysfunctions, was developed (Gabel et al., 2018;
M
¨
uller et al., 2019).
Executive dysfunctions are deficits of brain-
damaged patients concerning “the selection and exe-
cution of cognitive plans, their updating and monitor-
ing, the inhibition of irrelevant responses and prob-
lems with goal-directed behaviour usually result in
disorganized behaviour, impulsivity and problems in
goal management and self-regulation” (Emmanouel,
2017, p. 17).
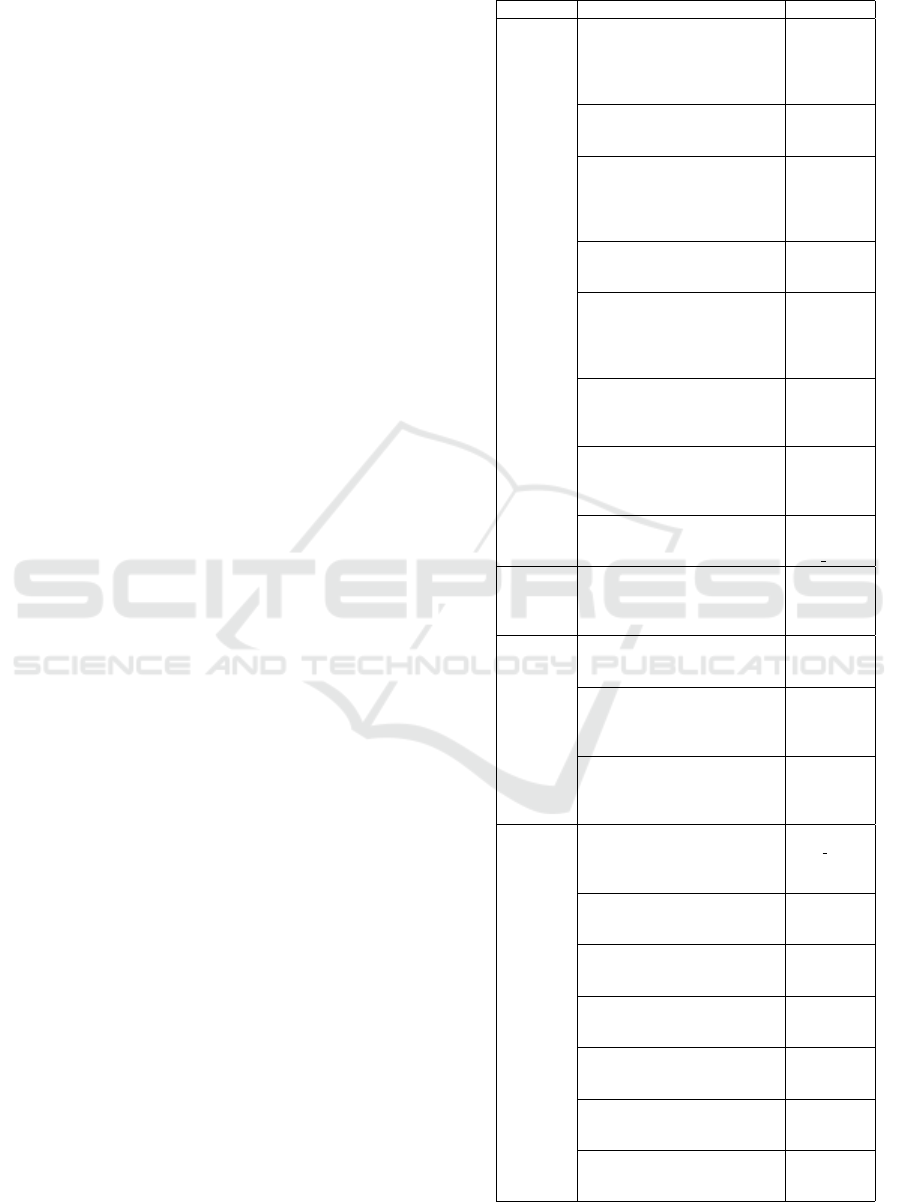
In the mobile application RehaGoal which is re-
alized as a web app, therapists can model individual
workflows in a visual editor (Eckhardt et al., 2019)
to help patients in activities of daily life as e.g. tak-
ing public transport, shopping or cleaning activities.
Workflows can then be executed on a smartphone (op-
tionally coupled with a smart watch), which will al-
ways display the current task, and can remind the user
regularly (Figure 2). Each task can contain a textual
description and an image. In addition there are ele-
ments as e.g. loops, yes/no questions, choices. To
further assist users, a text-to-speech (TTS) engine can
be enabled to read texts aloud. Workflows can be
arranged in a so-called schedule, such that multiple
workflows may be executed in a sequence.
The application is used in a neuropsychological
Figure 2: Screenshots of Individual Workflow.
intervention study and is compared with classical goal
management training. As pre/post tests are not able to
provide data during most time of the study, and self-
reports by patients can be biased, it is intended to ad-
ditionally collect data on the device in an automated
manner. Since the behavioral data involved may be
sensitive and may allow tracking, it is important that
this is done in a privacy-preserving way, following
Privacy by Design and data minimization principles.
With the introduction of the RehaGoal mHealth
app to the planned intervention study, new possibili-
ties regarding data collection were discussed, which
in the long-term could assist in therapeutic use-cases.
In addition to the pre/post tests as a common practice
in intervention studies, the use of mobile applications
allows to collect data from the day-to-day behavior of
the patients. On one side this allows additional in-
sights about the success of the therapy, as well as the
app usage, but on the other side this also might entail
significant privacy risks, as the device is potentially
able to track a large part of the users lifes. To address
these risks, the development process of mobile appli-
cations was integrated in a Privacy by Design process
(Gabel et al., 2018). One aspect of this Privacy by De-
sign process, the concept for privacy-preserving met-
rics to measure the impact of the mobile application,
is considered here.
In general the correlation between app usage and
test performance, as well as the usability of the app
was of interest. One of the goals was to minimize the
data collection needed for answering those questions,
without losing too much data quality. Therefore one
privacy-related question was, whether it is possible to
formulate research questions about the data, before
actually having collected the data in the context of
Privacy-preserving Metrics for an mHealth App in the Context of Neuropsychological Studies
167

a study. In many cases, foremost in big data analy-
sis, the questions are asked after (raw) data is already
available, or at the very least raw data is still avail-
able in order to reformulate questions or ask addi-
tional ones. However, in order to take data minimiza-
tion a step further and reduce the possibility of ad-
ditional inferencing based on the collected data, fol-
lowing purpose limitation, data was aggregated on the
device where it is collected, i.e. before data is trans-
ferred to the study provider. This meant, that much
care had to be taken in formulating the research ques-
tions and precisely checking, which data is needed in
order to get insight.
In this paper a Privacy by Design approach was
applied to develop metrics for an empirical study
based on the mobile application described above. To
this aim research questions were formulated before
the study. Based on the principle of data minimiza-
tion a metric language was derived from the research
questions. For the integration of metrics in the mobile
application, a metric architecture is proposed. The
approach presented here has a focus on data mini-
mization via aggregation and is based on the concept
of decentralization to foster privacy (Troncoso et al.,
2017).
The rest of the paper is organized as follows: In
section 2 an overview of existing approaches and is-
sues is given, section 3 summarizes the methodology.
In the following the concept for privacy-preserving
metrics is described. First research questions and de-
rived metrics are stated in section 4, afterwards the
metric language and the corresponding metric archi-
tecture is presented (section 5). Afterwards prelim-
inary results of the approach are summarized (sec-
tion 6).
2 RELATED WORK
Data collection using smartphones is already widely
used in mHealth. Use-cases can be classified by
whether they are using active data, requiring active
participation (e.g. surveys), or passively collected
data (i.e. sensor data) (Onnela and Rauch, 2016).
Furthermore there are applications which focus on
classical medicine, such as measuring the blood glu-
cose level (Cafazzo et al., 2012), as well as ones
which are located in the psychological area of re-
search. The latter applications often use data collected
by smartphones to measure behavior, e.g. regard-
ing to Digital Phenotyping (Onnela and Rauch, 2016;
Kleiman et al., 2018), or to gather insight on aspects
of the mental state of a person (Gr
¨
unerbl et al., 2015;
Garcia-Ceja et al., 2016). These approaches typically
collect a large amount of passive data and use active
data, as well as psychological tests as ground-truth
data. Using methods from the area of data mining
and machine learning, classifiers are trained, to infer-
ence mental state from certain behaviors. This has
been used to e.g. detect the manic/depressive state of
people with bipolar disorder (Gr
¨
unerbl et al., 2015),
as well as stress detection (Garcia-Ceja et al., 2016).
Often the data is first transformed by feature engineer-
ing & extraction using domain specific knowledge.
While there is research towards privacy-sensitive deep
learning techniques, e.g. based on differential pri-
vacy (McMahan et al., 2018) or federated learning
approaches using a cryptographic protocol for secure
aggregation (Bonawitz et al., 2017), deep learning is
still not used as often, due to e.g. overfitting at smaller
sample sizes (Mohr et al., 2017). However, publica-
tions often do not state, whether features are designed
before the actual data collection or afterwards, as well
as when, where (which device) and how often the fea-
tures are calculated on the raw data. All these factors
potentially have privacy implications. The amount of
information which may be inferenced from raw data
is much harder to approximate than for specially de-
signed features. Privacy by Design and Data Mini-
mization are therefore not always implemented as in-
tended by the GDPR (European Union, 2016). For ex-
ample (Gr
¨
unerbl et al., 2015) designed a smartphone
logging application, which collects information about
phone calls, sound & voice features to e.g. detect
emotional state, physical motion (accelerometer), as
well as travel patterns (GPS). The patient may decide
for every day whether she/he is comfortable with stor-
ing the data. No voice recognition was performed,
phone numbers where anonymized and GPS tracks
were transformed to an artificial coordinate system,
where (0, 0) always indicates ”home”. Some require-
ments (e.g. regarding the GPS tracks), were later de-
manded by an ethics board instead of integrating Pri-
vacy by Design in the design process of the applica-
tion. It is not clear, whether the raw data is stored
on the phone or when it is aggregated. In the worst
case, the smartphone may collect raw streams of sen-
sor data and later on researchers “anonymize” this
raw dataset, which includes computing the features.
In contrast a much better way would be to calculate
the features locally on the smartphone, while storing
as little temporary raw data as possible. Many fea-
tures may also be calculated directly from the raw
data stream, i.e. only storing intermediate values for
aggregation.
Another area, where sensor data is collected on
mobile devices, are so-called fitness apps. For these
applications often existing frameworks are used as
HEALTHINF 2020 - 13th International Conference on Health Informatics
168

e.g. Google Fit SDK
1
, Apple HealthKit
2
, Samsung
Health SDKs
3
, or Garmin Health API
4
. These typ-
ically include APIs for recording data from sensors,
including data types for a common representation of
units, as well as interfaces for querying data sets. The
basic architecture mainly relies on storing raw data
on provider-specific cloud services. Aggregates may
be computed afterwards based on this raw data. Most
services furthermore require the data to be stored on
their cloud service (Google, Samsung: data is syn-
chronized with server, Garmin: Data needs to be up-
loaded to Garmin Connect), with Apple HealthKit be-
ing the only exception (data is kept locally on the
user’s device). Furthermore in all cases accurate
timestamps (often millisecond precision) are always
included for every event. Samsung also includes a
unique device identifier (UUID) in every event. Re-
garding data minimization, it would be preferable to
only collect and store aggregate values, to specify the
needed accuracy (i.e. bucketing), and only include
additional data if required for the specific use case.
For example timestamps are most likely not required
to milli- or nanosecond (Google) precision. Further-
more e.g. step counts aggregated into minute buckets
or smaller time steps might also be unnecessary for
most use-cases.
There have also been several analyses regarding
the privacy and security of mHealth apps from app
stores (Mart
´
ınez-P
´
erez et al., 2015; Knorr and As-
pinall, 2015; Morera et al., 2016; Treacy and McCaf-
fery, 2016; Papageorgiou et al., 2018). Huckvale et
al. (Huckvale et al., 2015) assessed several aspects of
accredited health and wellness apps, including data
entered into the app, whether data is transmitted to
online services and whether it is encrypted, but also
other properties, such as the privacy policy or operat-
ing system permissions. Two-thirds of the apps col-
lected strong identifiers (which enable linkability) and
71 % had a mandatory registration process, while half
captured weak identifiers and 57% recorded poten-
tially sensitive information. It is at least questionable,
whether a Privacy by Design process was applied in
the development, as strong identifiers (email address,
full name, etc.), as well as a registration could pos-
sibly be avoided in a minimal use-case of most apps,
i.e. without sharing data with other parties following
the principle of data minimization. Concerning secu-
rity vulnerabilities, Huckvale et al. furthermore dis-
covered insecure data storage, data leakage or weak
server-side controls, as well as insufficient connec-
1
https://developers.google.com/fit/
2
https://developer.apple.com/documentation/healthkit
3
https://developer.samsung.com/health
4
https://developer.garmin.com/health-api/overview
tion encryption. He et al. found similar issues (He
et al., 2014) and noted, that in the case of using third
party servers, such as Amazon Web Services, it is
mostly unclear, whether data is stored in an encrypted
fashion, such that third parties do not have access
to potentially sensitive data. End-to-end encryption
is not mentioned, which however could strongly im-
prove the users’ control over their own data, includ-
ing the decision, whether to actually share data and
with whom. Goyal et al. specifically assess wear-
able health trackers (Goyal et al., 2016). Recently Pa-
pageorgiou et al. also found various major issues in
mHealth applications, including transmission of iden-
tifiers, personal or health data to third parties, some-
times even unencrypted. Mense et al. discovered
similar issues, particularly with third-party advertis-
ing or analytics solutions (Mense et al., 2016). This
sometimes includes GPS coordinates, age (group) &
gender, as well as health-related data, such as heart
rate. Additionally strong identifiers including email
address and device IDs are transmitted to the applica-
tion developer’s website.
3 METHODOLOGY
In the interdisciplinary team consisting of neuropsy-
chologists and computer scientists research questions
were identified and discussed based on experiences
from pilot studies and questions about the use of fea-
tures of the mHealth application. This was an iterative
process, in which abstract topics were broken down
step by step into separate questions, for which data on
the devices could be collected. For a better overview
research questions are grouped according to research
motivation (Table 1).
Ideas to measure the part of the patients behaviour
which is important for the study were validated based
on the question whether the amount of data is nec-
essary in proportion to the intended aim. The corre-
sponding terminology of the approach is summarized
in Table 2.
The amount of data and needed granularity was
expressed in the form of metrics (Table 3). A scheme
was developed for formulating metrics. In this context
especially the concept of an adequate granularity was
important. The mobile application allows to schedule
workflows consisting of tasks. Hence it is possible to
measure metrics based on tasks, single executions of
workflows, aggregate over all executions of a work-
flow or over schedules which comprise several work-
flows. It is possible to aggregate data at more than
one of these levels. Therefore this workflow based
granularity was named assignment.
Privacy-preserving Metrics for an mHealth App in the Context of Neuropsychological Studies
169
To describe the exact moment when the measure-
ment should take place during the execution of the
software, e.g. at the start of the execution of a work-
flow, a so-called record point needs to be stated, that
represents this point of time in the software.
Furthermore it needs to be specified, if several
measurements should be aggregated or if single mea-
surements are captured and stored. Concerning the
aggregation, also the aggregation function needs to be
stated. In the following this methodology is applied to
the research questions of studies in the context of the
mHealth application considered here. Each research
question could be described by one or more metrics
formulated based on this scheme (section 4). Metrics
and the metric scheme were used as the basis of a met-
ric language and a flexible architecture based on the
metric language is described (section 5).
4 RESEARCH QUESTIONS &
METRICS
As a first step research questions of the interdisci-
plinary team were developed (Table 1). Motivations
for research questions are to detect correlations be-
tween the results of the neuropsychological tests, an-
swers in questionnaires, interviews and the use of the
mobile application (therapeutic results), usability of
the mobile application and usage of features in work-
flow design (usability), implications of the specific
design of workflows (workflow design). Since some
research questions are related to more than one moti-
vation, they are categorized as follows:
• Therapeutic results
• Usability & Therapeutic results
• Usability & Workflow design
• Usability
Because in the context of the study the usage of
workflows by participants and therefore the results
of metrics highly depend on the modeling of partic-
ular workflows, also workflows, potentially in differ-
ent versions are stored, including pictures, such that in
the evaluation of the study problems such as potential
modeling and design issues can be understood. Every
modification of a workflow therefore gets assigned its
own workflow version identifier, which can be used to
group metrics for a specific version.
Some questions have multiple metrics assigned,
as there may be different time granularities, aggre-
gate functions, events (when to record the metric), or
obligatory private metrics recording temporary data
necessary for answering them. Table 1 gives an
Table 1: Research questions and associated metrics.
Category Research question Metrics
Therapeutic
Results
Does the number of work-
flow executions correlate with
changes in the goal attainment
scale / neuropsychological tests
/ subjective well-being?
m1
Does the repeated application of
a workflow correlate with less
assisted executions over time?
m2, m2a
Does the number of completed
workflow executions correlate
with changes in the goal attain-
ment scale / neuropsychological
tests / subjective well-being?
m3
Does the repeated completion of
a workflow correlate with less
assisted executions over time?
m4, m4a
Does the number of canceled
workflow executions correlate
with changes in the goal attain-
ment scale / neuropsychological
tests / subjective well-being?
m5
Does the repeated cancellation
of workflows correlate with less
assisted workflow executions
over time?
m6, m6a
Does the repeated completion of
a workflow correlate with the
time taken for the execution of
it?
m7
How does the amount of re-
minders per task change over
consecutive executions?
m9, m9a,
m9b,
m9c private
Usability
& Ther-
apeutic
Results
Does the usage of TTS correlate
with the number of completed/-
canceled workflows?
m17 – m21
Usability &
Workflow
Design
What could be possible reasons
for the active cancellation of a
workflow?
m8
How far are workflows executed
when they are canceled? Are
workflows canceled at specific
tasks?
m22
Does the type of presentation
correlate with changes in the
time taken for completing a
task?
m23 – m28
Usability
Are reminders closed once the
task has been completed or as
soon as the dialog appears on
the device?
m10, m11,
m11 private
How often was the scheduling
feature used (and therefore pos-
sibly better integrated)?
m12
Is the scheduling feature can-
celed less over time? (and there-
fore possibly better integrated)?
m13
How are schedules used? How
many (different) workflows are
scheduled?
m14
How are schedules used? How
many workflows were executed
before canceling a schedule?
m15
How is the distribution of the
number of workflows in com-
pleted schedules?
m16
How many (different) work-
flows are executed in a com-
pleted schedule?
m15, m16
HEALTHINF 2020 - 13th International Conference on Health Informatics
170
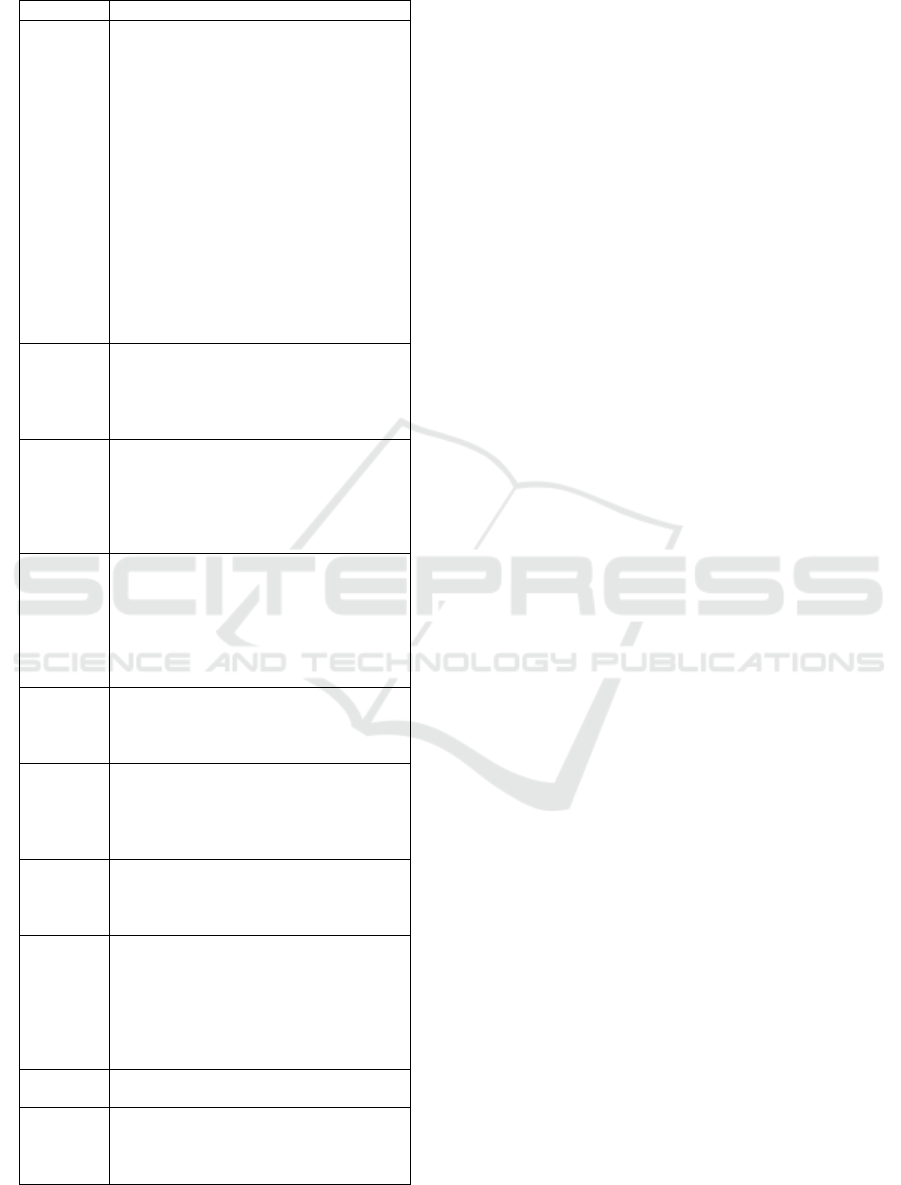
Table 2: Terminology.
Term Explanation
Assignment Inside a metric definition: The names
of the keys under which values of a
metric should be grouped. For example
[’workflow’, ’execution’] would
mean that the metric records separate
snapshots for every combination of work-
flow(Id) and execution(Id). Furthermore
these concrete values are stored in the
corresponding snapshot.
In the context of a record point: A map-
ping of (at least) all assignment keys in
metric definitions for this record point
to the value for the current event. For
example {workflowId: ’123-456’,
executionId: 42} would be a valid
assignment for the assignment definition
above.
Execution A workflow is being executed, when it
is being performed by a human assisted
by the application. From the start of a
workflow to the completion or cancellation
counts as being part of the execution.
Metric Measures or computes a certain value in
the context of a given assignment. Metrics
may aggregate several measurements into a
single value, store each measurement sep-
arately and can also trim the accuracy of a
value before it is stored.
Metric
Type
Currently four different types are defined:
number metrics (integer and floating
point metrics) measuring primitive values,
duration metrics measuring the time dif-
ference between two record points, and
meta metrics, which compute a value
based on another metric
Recording A metric is recorded when it is triggered by
a record point and measures or computes
a value which is then stored in the metric
database.
Record
Point
Named event in the program source code
which may trigger the recording of several
metrics. Apart from a required assignment,
an optional (dynamic) value may be pro-
vided.
Schedule A schedule consists of multiple workflows
which should be executed in a given order.
It can be created dynamically by the user
when needed.
Snapshot A snapshot consists of one or more mea-
surements aggregated into a single value,
sometimes including additional informa-
tion necessary for updating the aggregate
or (trimmed) timestamps. Furthermore
each snapshot stores its assignment and a
sequential index.
Task Simple step in a workflow, which is not be-
ing broken down into steps any more.
Workflow Representation of a task consisting of
many steps performed by human, modeled
using a block-based visual programming
language
overview about research questions and the derived
metrics used in our intervention study.
A selection of these metrics (marked as bold) used
to illustrate the concept is detailed in Table 3. The
metric definition scheme developed here consists of
the following parts:
• #: Metric ID
• Subject: Description of the metric
• Type: Determines what type of value should be
recorded.
• Assignment: describes for which identifiers data
may be collected and potentially aggregated. The
columns correspond to schedule (s), workflow
(w), workflow version (v), execution index (e) and
task index (t). These are arranged in a kind of
hierarchy, i.e. a schedule can contain multiple
workflows, a workflow may have multiple ver-
sions, a version may be executed more than once
and during execution different tasks occur. Met-
rics can have an assignment which covers multi-
ple areas, e.g. it could be of interest to collect
information about sequential executions of a par-
ticular workflow (w,e), but it may also be useful
to instead find out about sequential executions per
user. A global assignment in the table actually
corresponds to an assignment per device/user, i.e.
no assignment in the other categories.
• Record Point: named events in the program
source code which should trigger the recording of
the metric
• Aggregate: Aggregation function (op.) and aggre-
gation interval (time) (if applicable)
• #Sn: number of metric results that are collected,
denoted as snapshot count
• Options: More specific options, e.g. accuracy
Based on the emphasized metrics this metric
scheme is explained in more detail. The goal of metric
m1 is to count the number of workflow executions for
each workflow separately. In the example workflows
are denoted by a title explaining the aim of the work-
flow instead of the workflow ID. As a potential result
the workflow “Make coffee” may have been executed
only once, while “Write a letter” may have been exe-
cuted 12 times. Since the result of the metric is a natu-
ral number, the type of the metric would be int. The
metric should be increased by one when the record
point workflowStart is reached in the mobile app.
To count instead only workflow executions
that are completed (m3), instead the record point
workflowEnd is used. To count values, the aggre-
gate operation sum adds the constant 1 to the metric
value, every time the event described by the record
Privacy-preserving Metrics for an mHealth App in the Context of Neuropsychological Studies
171

point occurs (Option constValue: 1). Since it is
not intended to measure a progression over time in
this metric, the value is aggregated over the whole
study (measurement period) which is denoted by time
all time.
Another example is metric m8, which measures
the duration of workflow execution executed before
it was actively canceled by the participant. In this
case the type is duration dur, and the time inter-
val from workflowStart to workflowAbort is mea-
sured. Since cancellation of workflows is very impor-
tant in the context of the corresponding reserach ques-
tion, a separate value for each workflow execution is
collected, i.e. no aggregation is applied. In this case
the assignment in the metric scheme is workflow and
execution. Since there is no limit for the number of
values, the snapshot count is infinite.
A more complex construct of a so called meta
metric is a metric whose values are calculated based
on the values of a second metric as e.g. m11 based
on m11 private. The corresponding research ques-
tion has a focus on usability and investigates when
so called reminders are closed.
Every element in a workflow can be augmented by
such a reminder element. Elements can be e.g. tasks,
repetitions, decision questions. It can be defined after
which time interval the participant is reminded of an
element. This is especially helpful if elements require
a longer time or participants are often distracted. It is
interesting to see when reminders are closed, directly
when the reminder appears on the screen or when the
task is finished, and to see how often the reminders
appear.
The idea is that if a user confirms the reminder
more often per element, this indicates that the user
is more tightly interacting with the device, while less
often (e.g. only once per task) may indicate that the
user rather interacts with the device only after com-
pleting a task (m10 collects additional information for
the question). However, since the number of con-
firmed reminders per task needs to be known before
computing the average, These are counted per task
(m11 private), but are stored only temporarily for the
calculation.
The average can then be recalculated over the tem-
porary values every time a value changes (m11). Both
metrics are recorded at the same record points: when
a (task-)block is entered, which initializes the count
to 0, and every time a reminder is accepted, which
increases the count by one (Option constValueMap).
Since (m11
private) is counted for every task of an
execution per workflow separately, its assignment is
(w, e, t). Meta metrics are recorded after other metric
types have been computed, therefore after counting,
we always compute the latest average over all tempo-
rary values (m11 is referenced by metaReference).
After the workflow is completed or aborted, all tem-
porary snapshot values collected by m11 private for
this workflow can be deleted (deleteSnapshots).
Another example is metric m13, where the number
of actively canceled schedules per week is counted.
This results in a separate value for each week, which
can be used later on to gain insight about the change
over time (aggregate time). Since the value is not tied
to a specific schedule, workflow etc., it is collected
per user resp. device (global) in the case of shared
devices. Every time a scheduleAbort event occurs,
our count (the sum) for this week is increased by one
(constValue). The number of snapshots, i.e. in this
case the number of retained weeks where at least one
schedule was aborted, is not limited in the study con-
text.
It is also possible to record values as a parameter
of the record point, as it is done e.g. in m17 for record-
ing the average setting of the text-to-speech speed.
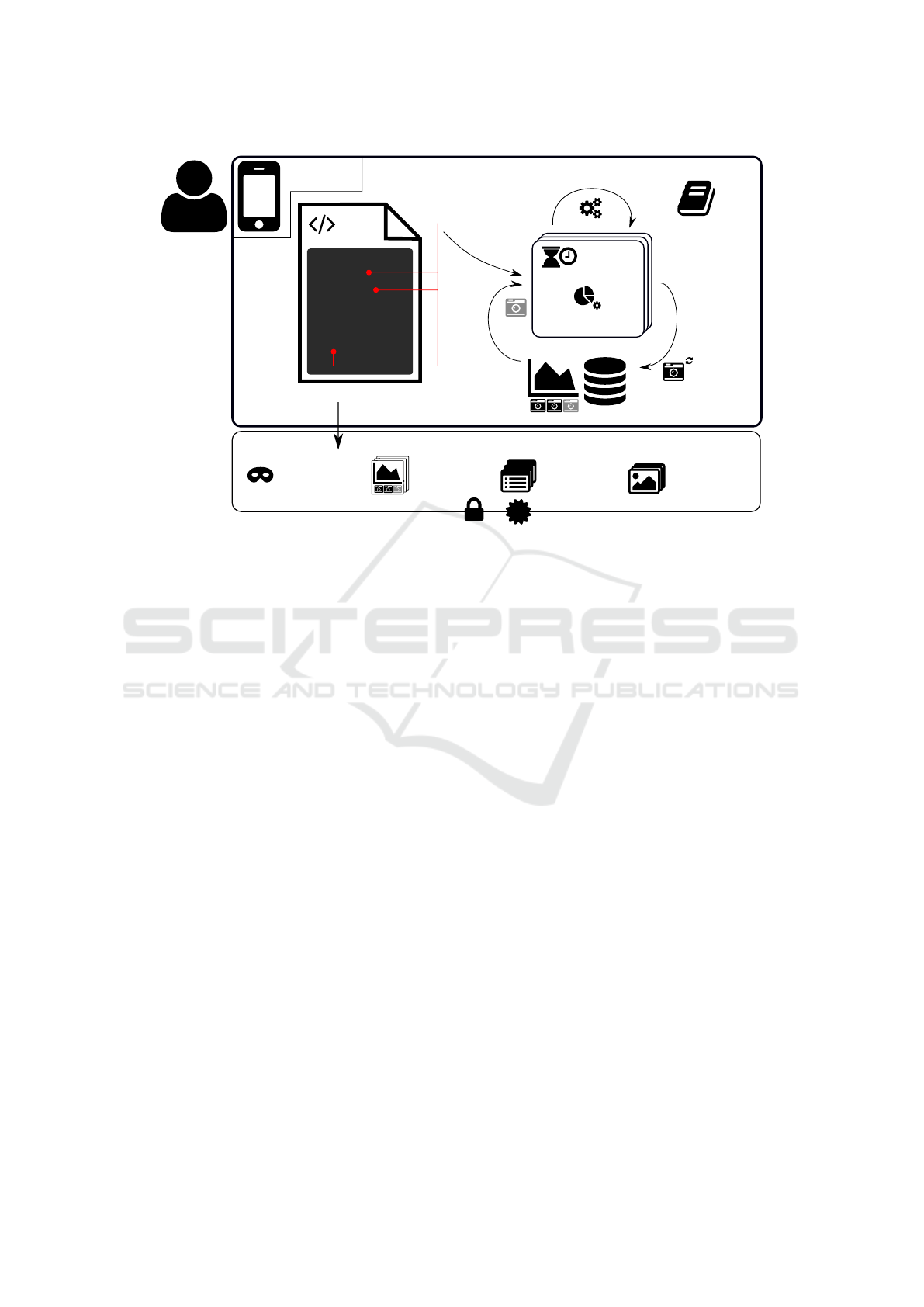
5 METRIC ARCHITECTURE &
METRIC LANGUAGE
In the following a domain specific language (DSL)
for describing metrics and the corresponding metric
architecture for the integration of metrics in an appli-
cation are described (Figure 3).
5.1 Metric Language
In order to allow a flexible addition and reconfigu-
ration of metrics, a DSL for describing metrics was
defined based on requirements identified during the
development of metrics in section 4. This DSL is
descriptive rather than containing code for evaluat-
ing the metrics. The idea behind this was to sim-
plify the specification and readability of metrics, re-
duce code duplication, and to integrate the consider-
ation of privacy-related questions into the DSL, e.g.
“What data is needed? Which time resp. value ac-
curacy? Are timestamps needed for each measure-
ment?”. Each time new research questions are added
or research questions are modified and hence metrics
need to be added or adjusted this should be done in a
privacy-friendly way.
Additionally this specification of data captur-
ing allows to derive automatically information about
which data is collected, how this is done and when
the data is collected as input for a privacy dashboard
(Murmann and Fischer-H
¨
ubner, 2017) to foster trans-
parency for users. The DSL is defined based on
HEALTHINF 2020 - 13th International Conference on Health Informatics
172
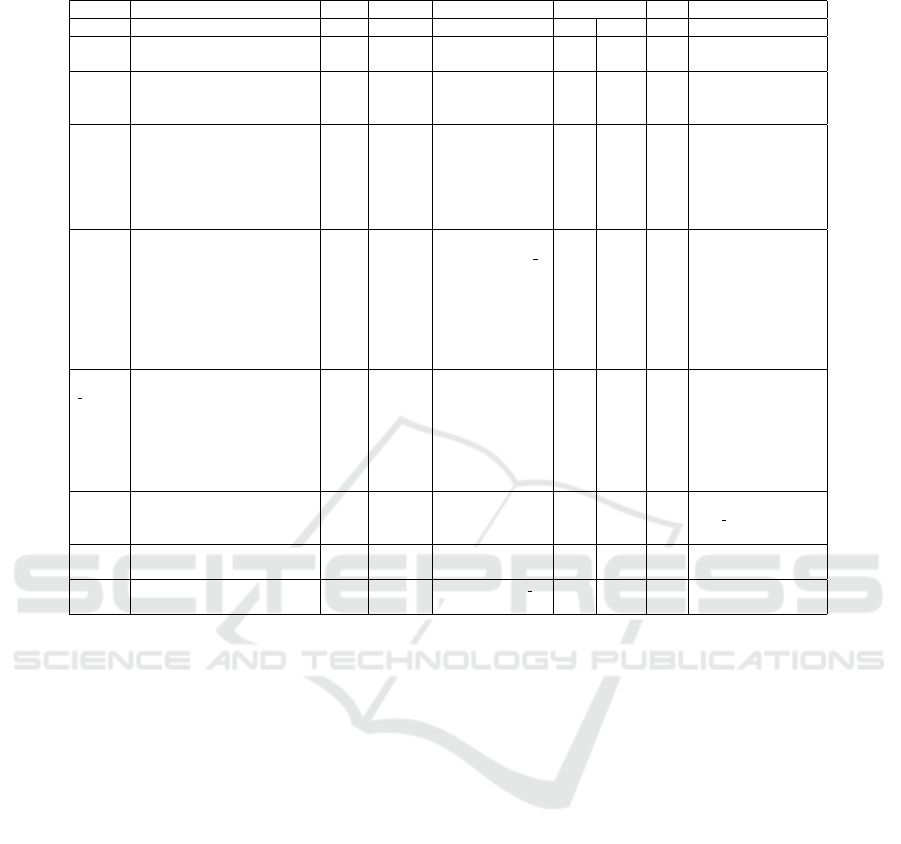
Table 3: Excerpt of declared metrics and their properties.
# Subject Type Assign. Record point Aggregate #Sn Options
op. time
m1 Number of workflow execu-
tions per workflow
int w workflowStart sum all 1 constValue: 1
m3 Number of completed work-
flow executions per work-
flow
int w workflowEnd sum all 1 constValue: 1
m8 Time taken per (actively)
canceled workflow execu-
tion
dur w,e workflowStart
→workflowAbort
– – ∞ durationAccuracy: 1s,
clearIncomplete:
[workflowEnd,
workflowStart],
handleIncomplete:
ignore
m10 Average time between con-
firmation of last reminder
and marking a task as fin-
ished per execution of a
workflow
dur w,e reminderAccept
→blockAccept
withAccepted
Reminder
avg all 1 durationAccuracy: 1s,
clearIncomplete:
[workflowEnd,
workflowAbort],
handleIncomplete:
ignore,
agg.durationAccuracy:
1s
m11
private
Number of confirmed re-
minders per task per execu-
tion of a workflow
int w,e,t reminderAccept,
blockEnter
sum all ∞ private: true,
constValueMap:
{reminderAccept: 1,
blockEnter: 0},
deleteSnapshots:
[workflowEnd,
workflowAbort]
m11 Average number of con-
firmed reminders per task
per execution of a workflow
meta w,e reminderAccept,
blockEnter
avg all 1 metaReference:
m11 private
m13 Number of (actively) can-
celed schedules per week
int global scheduleAbort sum week ∞ constValue: 1
m17 Average speed setting of
TTS in workflow executions
float global workflowStart
ttsSpeed(x)
avg all 1
JavaScript Object Notation (JSON), as it is a com-
mon, human-readable format already widely used in
web and mobile applications. The language is spec-
ified as a TypeScript definition file and therefore al-
lows syntax checking and auto completion in inte-
grated development environments (IDEs). Further-
more many possible mistakes in the description of a
metric can be detected at compile-time through rather
restrictive types.
To separate the actual raw measurements and
events from the metrics depending on them and to
keep the actual metric binding code less intrusive (i.e.
when measurements happen in application code), the
concept of record points was introduced. These are
places in the application code, where a potentially
metric-relevant event happens, possibly including a
context-related value. In the description of a metric,
such record points may be referenced via their name,
which causes the metric to be bound to that particular
record point. Every time the event occurs, all metrics
with a binding to the record point will be executed
and will record a value. This decouples the defini-
tion of metrics from the events in code, i.e. instead
of specifying which metrics are relevant at a certain
event, only the event is specified and metrics declare
what events they listen to. New metrics, which reuse
existing record points, can be added simply by adding
a definition, without changing further code.
Metrics differ in the types of values they record
and their recording behavior. The simplest types
are integer (int) and floating point (float) met-
rics, which record values of the particular type.
In order to prevent type confusion, i.e. record-
ing floating point values in an integer metric, run-
time checks are performed. If no value is provided
at the record point, the metric has to either spec-
ify a constant value for all record points (Option
constValue) or for each record point separately (Op-
tion constValueMap). For example if only the count
of certain events is needed, a constant value may be
sufficient. Metrics can also record a duration. A
duration is specified by two record points – a start
(recordStart) and a stop (recordStop) – and the
duration is measured between both events. The last
type are meta metrics, which can compute new val-
ues derived from a base metric referenced through its
name in metaReference. Metrics can be marked as
private which causes them to be excluded from ex-
Privacy-preserving Metrics for an mHealth App in the Context of Neuropsychological Studies
173
MetricRegistry
Keeps track of
registered Metrics
& RecordPoints
Icons: Font Awesome (CC BY 4.0)
(https://fontawesome.com/license)
Study export
Participant
Pseudonym
Workflows
Workflow
Images
Metric
Snapshots
Encrypted (RSA)
for StudyProvider
Signed with
Participant's
Private Key
OpenPGP.js
U
p
d
a
t
e
a
g
g
r
e
g
a
t
e
Duration
Metric
1
2
3
Number
Metric
Meta
Metric
Duration
Metric
1
2
3
Number
Metric
Meta
Metric
Duration
Metric
1
2
3
Number
Metric
Meta
Metric
RecordPoint
JS
38
39
40
41
42
43
44
45
46
47
48
49
50
51
function A() {
if (...) {
// ...
}
process();
for (...) {
// ...
}
}
/** Doc */
function B() {
const c = 3.14;
// ...
}
S
t
o
r
e
u
p
d
a
t
e
d
Metrics Database
F
e
t
c
h
u
n
fi
n
i
s
h
e
d
s
n
a
p
s
h
o
t
t
r
i
g
g
e
r
s
m
e
t
r
i
c
(
s
)
s
n
a
p
s
h
o
t
Participant
Mobile Device
Figure 3: Metric Architecture.
ports and therefore makes them inaccessible for the
study provider. This can be useful in combination
with meta metrics, which are based on private met-
rics and compute an aggregate value. The separation
into private and public metrics leads to further data
minimization even for aggregate functions such as the
median, which require storing all (counts of) values.
All metric types have in common, that they have
an assignment, which states the scope in which met-
ric values are collected or aggregated. This enables
not only to record global metrics, but also metrics
which are relating to a certain context. An example
would be m3 which counts the number of completed
workflow executions per workflow. In this example
the assignment is to the workflow, since the value
is needed for each distinct workflow. Assignments
can also be empty (for global metrics) or consist of
multiple elements. For example to measure the time
per completed execution per workflow (assignment:
["workflow", "execution"]). Specifying only
"execution" would result in in an aggregated value
for executions of workflows in general, while speci-
fying only "workflow" would not group the recorded
values per execution. This is especially relevant when
computing aggregates, which are computed for each
group separately.
A central aim of the DSL for metrics is to aggre-
gate values on the device instead of collecting raw
data. For aggregation operations the metric descrip-
tion has to include the otherwise optional agg ele-
ment and specify the aggregate operation, as well
as the time frame over which the aggregation should
be performed. Currently supported aggregate oper-
ations are min, max, sum, average, median and
variance, while supported time frames are week,
day, 1/4day, hour. Furthermore there is the spe-
cial time frame all, which states that the aggregation
should be over the complete time while metrics are
recorded. Aggregation operations are performed in an
incremental fashion, if possible, i.e. temporary values
are kept to a minimum. For example we use Welford’s
online algorithm (Welford, 1962; Chan et al., 1983)
for computing the variance in a numerically stable
way.
Recorded values are stored in so-called snapshots.
Every snapshot additionally has an index, the concrete
assignment (e.g. workflow identifier and execution in-
dex) and may optionally store additional information
for tracking aggregate values (such as welford state,
number of measurements) and the start of the mea-
surement (rounded timestamp). To limit the amount
of recorded data, metrics have to specify the maxi-
mum amount of snapshots, which might also be infi-
nite. This for example allows to keep data for a fixed
number of weeks when combined with the time frame
week for aggregation, or a fixed number of the last
recorded values. The oldest snapshot is deleted, when
a new one is to be recorded when the maximum num-
ber of snapshots is reached.
HEALTHINF 2020 - 13th International Conference on Health Informatics
174

Metrics may also specify accuracy of values or
duration. This can also be used to built histograms,
since values in a certain range fall into the same accu-
racy bucket. Accuracy is described by a number and
an optional unit in the case of duration accuracy. For
example [5, "s"] states that all durations should be
only stored to an accuracy of five seconds. An accu-
racy can be applied to raw values and aggregate val-
ues.
Often it is not necessary to store the timestamp
of an event, as it may be sufficient to store the or-
der of snapshots. Sometimes even that might not be
required. Also when a timestamp is necessary, in al-
most all cases it does not need to have the full accu-
racy provided by the system. For the use case investi-
gated here as timestamp in certain metrics the hour of
events is recorded. Metrics may declare that a times-
tamp should be recorded, by specifying its accuracy
in the timestamp field. Timestamps are also auto-
matically recorded for aggregate metrics with a time
frame option which is not ‘all‘.
Since private metrics may accumulate many snap-
shots, which may not be necessary after an aggrega-
tion operation is finished there is an additional option
(deleteSnapshotsEvents) to delete snapshots of a
metric on certain record points or events.
In addition it needs to be defined what should be
done with accumulated snapshots of private metrics
in exceptional situations. There are two cases con-
sidered in the DSL: When the next duration mea-
surement of the same metric and assignment starts,
but the previous has not finished yet, it has to be
decided how the incomplete measurement should be
handled (Option handleIncomplete). It could be de-
cided to ignore the measurement, or to truncate
the duration to end at the current time, i.e. when
the next measurement starts. If a certain measure-
ment cannot be completed and there is no chance
that another measurement with the same assignment
would occur e.g. since the defined end of the study
is reached, the snapshots which are accumulated
for these measurements have to be deleted (Option
clearIncompleteEvents) An example of a metric
definition is shown in Listing 5.1.
Listing 1: Example metric definition.
{
” name ” : ” Number o f w ork flo w e x e c u t i o n s p er w o rkf low p er
week ” ,
” typ e ” : ” i n t ” ,
” r e c o r d P o i n t s ” : [ ” wo r k f l o w S t a r t ” ] ,
” con s t V a lu e ” : 1 ,
” ass i g n m en t ” : [ ” wo rkf l ow ” ] ,
” s n a p s h o t s ” : ” i n f ” ,
” agg ” : {
” o p e r a t i o n ” : ” sum ” ,
” t i m e ” : ” week ”}
}
5.2 Metric Architecture
For the integration of the metric DSL the following
metric architecture was developed. The code respon-
sible for creating a record point by coupling produc-
tive code to the metric architecture, should be as min-
imal as possible. Furthermore logic regarding metrics
should be kept at a minimum by describing most of
the logic in the metric definition. In the metric archi-
tecture presented here the coupling can be realized by
two different methods record, recordValue. which
accept as parameters the record point name, the con-
crete assignment (e.g. workflow and execution iden-
tifier), as well as a value (float or int) in the case of
recordValue.
Metrics are registered by providing a metric defi-
nition to a MetricRegistry, which keeps track of all
record points and associated metrics. Record points
are embedded in the code by calling the record or
recordValue methods of the MetricService. This
allows the flexible addition or modification of metrics,
as definitions can be changed in a descriptive man-
ner independent of their record points. Furthermore
record points can mainly be added with the addition
of a single line in the production code (Listing 5.2)
since most logic, such as aggregation, is described in
the metric definition.
Metrics are only recorded until the end of the
study (predefined date). An export of the study data
(Figure 3) is then encrypted with the public key of the
study provider and signed with the participant’s pri-
vate key using OpenPGP.js
5
.
Listing 2: Code changes necessary for adding a new metric
and record point.
// r egi st er m etr ic ( a ppl ic at ion s tar tup )
c o n s t m e t r i c D e f i n i t i o n = . . . ; // m et ric de fi ni tio n in DS L
m e t r i c S e r v i c e . r e g i s t e r ( m e t r i c D e f i n i t i o n ) ;
// .. . So mew he re in pr od uct io n co de .. .
// a ss ign me nt : co nt ain s wo rkf low Id , e x ec ut ion Id etc .
m e t r i c S e r v i c e . r e c o r d ( ’e xa mp le Rec or dP oi nt ’ , a s s i g n m e n t ) ;
// or : ( v a l ue is a nu mbe r )
m e t r i c S e r v i c e . r e c o r dV a l u e ( ’ rp Val ue ’ , a s s i g n m e n t , v a l u e ) ;
6 PRELIMINARY RESULTS
At the moment, the presented metric concept is eval-
uated in the context of several studies. First prelim-
inary results are presented here. A group of n = 4
participants executed workflows while metrics were
recorded for a period of five weeks. The results of the
full study will be published in a separate publication.
Three different types of workflows were modeled by
5
https://openpgpjs.org/
Privacy-preserving Metrics for an mHealth App in the Context of Neuropsychological Studies
175
Table 4: Preliminary results: participant number, workflow,
number of started, completed workflows and average exe-
cution duration.
# p. workflow # start. # comp. Ø dur.
1 Shopping 11 10 32.11 s
2 Clean-up 8 4 6290 s
3 Public
transport
9 9 38.11 s
4 Clean-up 4 3 5659 s
neuropsychologists in the team: shopping, apartment
cleaning and using public transport.
In the following results of the preliminary eval-
uation are summarized. The number of started work-
flow executions per patient was relatively low ranging
between four and eleven executions. The number of
finished workflows (not canceled) had a lower range
between three and ten. The total number of finished
workflow executions over all patients was 26. Half
of the participants had a workflow execution duration
which fits the workflow type, while other executions
indicate that some have been completed in less time
than we would expect for that task. This may indicate
that workflows have been skipped through while not
performing the tasks during that time. For example
the participants may have looked through the work-
flow before actually performing the tasks. Half of
the participants had mostly workflows with relatively
short execution times compared to the workflow type.
Mainly two types of errors occurred: one work-
flow was running for multiple days which is not plau-
sible for the workflow type, 6 times workflows were
canceled not inside the mobile application, where this
would also be possible, but by external causes. Possi-
ble causes are that the app is terminated by the user or
the operating system or the device lost power. Ta-
ble 4 shows the workflows for each participant to-
gether with the number of started and completed ex-
ecutions, and the average execution duration. Errors
are excluded from the statistics in Table 4.
7 CONCLUSION
Collecting data during empirical studies with mobile
devices gives important insights beside pre/post tests.
The approach presented here shows that it is possi-
ble to derive metrics from research questions ensuring
data minimization via aggregation and decentraliza-
tion in the context of a Privacy by Design approach.
The presented concept is promising. The metric lan-
guage and the metric architecture ensure that the ap-
proach is flexible and research questions can easily
be described and adjusted. It is intended to use the
metric language also as a basis for automatically gen-
erated privacy dashboards to inform users about data
processing in a transparent way.
ACKNOWLEDGEMENTS
This work was supported by the Ministry for Sci-
ence and Culture of Lower Saxony as part of SecuRIn
(VWZN3224).
REFERENCES
Beierle, F., Tran, V. T., Allemand, M., Neff, P., Schlee,
W., Probst, T., Zimmermann, J., and Pryss, R. (2019).
What data are smartphone users willing to share with
researchers? Journal of Ambient Intelligence and Hu-
manized Computing, pages 1–13.
Bertens, D., Fasotti, L., Boelen, D. H., and Kessels, R. P.
(2013). A randomized controlled trial on errorless
learning in goal management training: Study rationale
and protocol. BMC Neurology, 13(1):64.
Bonawitz, K., Ivanov, V., Kreuter, B., Marcedone, A.,
McMahan, H. B., Patel, S., Ramage, D., Segal, A.,
and Seth, K. (2017). Practical secure aggregation
for privacy preserving machine learning. Cryptology
ePrint Archive, Report 2017/281. https://eprint.iacr.
org/2017/281.
Cafazzo, J. A., Casselman, M., Hamming, N., Katzman,
D. K., and Palmert, M. R. (2012). Design of an
mHealth App for the Self-management of Adolescent
Type 1 Diabetes: A Pilot Study. Journal of Medical
Internet Research, 14(3):e70.
Chan, T. F., Golub, G. H., and Leveque, R. J. (1983). Al-
gorithms for computing the sample variance: Analy-
sis and recommendations. The American Statistician,
37(3):242–247.
Colesky, M., Hoepman, J. H., and Hillen, C. (2016). A
critical analysis of privacy design strategies. In 2016
IEEE Security and Privacy Workshops (SPW), pages
33–40.
Di Matteo, D., Fine, A., Fotinos, K., Rose, J., and Katzman,
M. (2018). Patient willingness to consent to mobile
phone data collection for mental health apps: struc-
tured questionnaire. JMIR mental health, 5(3):e56.
Eckhardt, K., Schiering, I., Gabel, A., Ertas, F., and M
¨
uller,
S. V. (2019). Visual Programming for Assistive Tech-
nologies in Rehabilitation and Social Inclusion of
People with Intellectual Disabilities. In MuC ’19.
Emmanouel, A. (2017). Look at the frontal side of life: An-
terior brain pathology and everyday executive func-
tion: Assessment approaches and treatment. PhD the-
sis, Radboud University.
European Union (2016). Regulation (EU) 2016/679 of the
european parliament and of the council of 27 april
HEALTHINF 2020 - 13th International Conference on Health Informatics
176

2016 on the protection of natural persons with re-
gard to the processing of personal data and on the
free movement of such data, and repealing directive
95/46/EC (general data protection regulation). Offi-
cial Journal of the European Union, L119:1–88.
Gabel, A., Schiering, I., M
¨
uller, S. V., and Ertas, F.
(2018). mHealth Applications for Goal Management
Training - Privacy Engineering in Neuropsychologi-
cal Studies. In Hansen, M., Kosta, E., Nai-Fovino,
I., and Fischer-H
¨
ubner, S., editors, Privacy and Iden-
tity Management. The Smart Revolution: 12th IFIP
WG 9.2, 9.5, 9.6/11.7, 11.6/SIG 9.2.2 International
Summer School, Ispra, Italy, September 4-8, 2017,
Revised Selected Papers, IFIP Advances in Informa-
tion and Communication Technology, pages 330–345.
Springer International Publishing, Cham.
Garcia-Ceja, E., Osmani, V., and Mayora, O. (2016). Au-
tomatic Stress Detection in Working Environments
From Smartphones’ Accelerometer Data: A First
Step. IEEE Journal of Biomedical and Health Infor-
matics, 20(4):1053–1060.
Goyal, R., Dragoni, N., and Spognardi, A. (2016). Mind
the Tracker You Wear: A Security Analysis of Wear-
able Health Trackers. In Proceedings of the 31st An-
nual ACM Symposium on Applied Computing, SAC
’16, pages 131–136, New York, NY, USA. ACM.
Gr
¨
unerbl, A., Muaremi, A., Osmani, V., Bahle, G.,
¨
Ohler,
S., Tr
¨
oster, G., Mayora, O., Haring, C., and Lukow-
icz, P. (2015). Smartphone-Based Recognition of
States and State Changes in Bipolar Disorder Patients.
IEEE Journal of Biomedical and Health Informatics,
19(1):140–148.
Hansen, M., Jensen, M., and Rost, M. (2015). Protection
goals for privacy engineering. In 2015 IEEE Security
and Privacy Workshops, pages 159–166.
He, D., Naveed, M., Gunter, C. A., and Nahrstedt, K.
(2014). Security Concerns in Android mHealth Apps.
AMIA Annual Symposium Proceedings, 2014:645–
654.
Huckvale, K., Prieto, J. T., Tilney, M., Benghozi, P.-J., and
Car, J. (2015). Unaddressed privacy risks in accred-
ited health and wellness apps: A cross-sectional sys-
tematic assessment. BMC Medicine, 13:214.
Jamieson, M., Jack, R., O’Neill, B., Cullen, B., Lennon, M.,
Brewster, S., and Evans, J. (2019). Technology to en-
courage meaningful activities following brain injury.
Disability and Rehabilitation: Assistive Technology,
0(0):1–14.
Kleiman, E. M., Turner, B. J., Fedor, S., Beale, E. E., Pi-
card, R. W., Huffman, J. C., and Nock, M. K. (2018).
Digital phenotyping of suicidal thoughts. https://
onlinelibrary.wiley.com/doi/abs/10.1002/da.22730.
Knorr, K. and Aspinall, D. (2015). Security testing for
Android mHealth apps. In 2015 IEEE Eighth Inter-
national Conference on Software Testing, Verification
and Validation Workshops (ICSTW), pages 1–8.
Levine, B., Robertson, I. H., Clare, L., Carter, G., Hong,
J., Wilson, B. A., Duncan, J., and Stuss, D. T.
(2000). Rehabilitation of executive functioning: An
experimental–clinical validation of goal management
training. Journal of the International Neuropsycho-
logical Society, 6(3):299–312.
Mart
´
ınez-P
´
erez, B., de la Torre-D
´
ıez, I., and L
´
opez-
Coronado, M. (2015). Privacy and Security in Mo-
bile Health Apps: A Review and Recommendations.
Journal of Medical Systems, 39(1):181.
McMahan, B., Ramage, D., Talwar, K., and Zhang, L.
(2018). Learning differentially private recurrent lan-
guage models. In International Conference on Learn-
ing Representations (ICLR).
Mense, A., Steger, S., Sulek, M., Jukic-Sunaric, D., and
M
´
esz
´
aros, A. (2016). Analyzing privacy risks of
mHealth applications. Stud Health Technol Inform,
221:41–45.
M
¨
uller, S. V., Ertas, F., Aust, J., Gabel, A., and Schier-
ing, I. (2019). Kann eine mobile anwendung helfen
abzuwaschen? Zeitschrift f
¨
ur Neuropsychologie,
30(2):123–131.
Mohr, D. L., Zhang, M., and Schueller, S. M. (2017). Per-
sonal Sensing: Understanding Mental Health Using
Ubiquitous Sensors and Machine Learning. Annual
review of clinical psychology, 13:23–47.
Morera, E. P., D
´
ıez, I. d. l. T., Garcia-Zapirain, B., L
´
opez-
Coronado, M., and Arambarri, J. (2016). Security
Recommendations for mHealth Apps: Elaboration of
a Developer’s Guide. Journal of Medical Systems,
40(6):152.
Murmann, P. and Fischer-H
¨
ubner, S. (2017). Tools for
achieving usable ex post transparency: a survey. IEEE
Access, 5:22965–22991.
Onnela, J.-P. and Rauch, S. L. (2016). Harnessing
Smartphone-Based Digital Phenotyping to Enhance
Behavioral and Mental Health. Neuropsychopharma-
cology, 41(7):1691–1696.
Papageorgiou, A., Strigkos, M., Politou, E., Alepis, E.,
Solanas, A., and Patsakis, C. (2018). Security and
Privacy Analysis of Mobile Health Applications: The
Alarming State of Practice. IEEE Access, 6:9390–
9403.
Stamenova, V. and Levine, B. (2018). Effectiveness of goal
management training
R
in improving executive func-
tions: A meta-analysis. Neuropsychological Rehabil-
itation, 0(0):1–31.
Treacy, C. and McCaffery, F. (2016). Data Security
Overview for Medical Mobile Apps. International
Journal on Advances in Security Volume 9, Number
3 & 4, 2016.
Troncoso, C., Isaakidis, M., Danezis, G., and Halpin,
H. (2017). Systematizing decentralization and pri-
vacy: Lessons from 15 years of research and deploy-
ments. Proceedings on Privacy Enhancing Technolo-
gies, 2017(4):404–426.
Welford, B. P. (1962). Note on a Method for Calculating
Corrected Sums of Squares and Products. Technomet-
rics, 4(3):419–420.
Privacy-preserving Metrics for an mHealth App in the Context of Neuropsychological Studies
177
