
Classification of Five Finger Movement, based on a Low-cost,
Real-time EMG System
Clive Seguna, Adrian Von Brockdorff, Jeremy Scerri and Kris Scicluna
Department of Electrical and Electronics Engineering, MCAST, Corradino Hill Paola, PLA9032, Malta
Keywords: EMG, Electromyography, Biopotential, Myoelectric.
Abstract: Researchers commonly use myoelectric signals to study the electrical activity produced by skeletal muscles
for the control of prosthetic arms, hands and limb replacement devices. Additionally, to the application in
prostheses, a myoelectric control system for multiple finger movements has the potential to develop
commercial products including advanced human-computer interfaces. The objective of this work is to
implement a set of low-cost active electrodes for the decoding of finger movement via time-domain analysis,
with an auto-gain adjustment technique. Different people will have different EMG amplitudes; therefore, it is
difficult to determine the gain required prior performing further signal processing. In this work, an auto-
adjustable gain amplifier circuit processes the maximum EMG signal amplitude and adjusts the gain stage
accordingly, without the need of any user interaction. This ensures that the gain is always automatically
adjusted to get the most effective performance from the data acquisition or analogue to digital converter (ADC)
module since the signal will be neither too low in amplitude to cause inefficient use of the ADC resolution,
nor too high to cause saturation of the signal. Through extensive experiments, the developed low-cost EMG
data acquisition system achieves reproducible and repeatable results for the detection and classification of the
five finger movements.
1 INTRODUCTION
This paper is an extension of the work originally
presented in NGCAS conference (Seguna, 2018).
Electromyography (EMG) signal acquisition is a
medicine technique used for recording and analysing
the electrical activity produced by skeletal muscles.
EMG systems detect the electrical potential generated
by muscles when they are neurologically activated
(Tsuji, 2000). The EMG signal can be used to obtain
several information related to muscle activity, such as
detecting medical abnormalities, muscle activation
levels, or to analyse the biomechanics of the human. It
is also used as a research tool for studying kinesiology,
which can then be used to control prosthetic devices
such as prosthetic arms, hands and lower limbs. This
is possible since muscles in the remaining part of the
limb function in a normal way, enabling the EMG
signals extracted from them to be used in limb
replacement devices. The benefit of this technique is
that the signal is acquired from the patient's remaining
limb muscles, which after appropriate processing can
be used to control motors. These motors can be used
to control several applications, including the control of
motorised wheelchairs and the control of prosthetic
devices which can be worn by amputees and activated
by their own EMG signals (Sudarsan, 2012),
(Osamu, 2003), (Jingpeng, 2013), (Côté, 2015)
provided. EMG studies in general are useful for
assessing the health of the neuromuscular system,
since certain diseases, such as multiple sclerosis,
suppress or even slow down normal nerve and muscle
firing. Surface EMG (sEMG) signal is the product of
all the action potentials which are picked from the
muscles below skin surface electrode. The amplitude
of sEMG signals is stochastic (random) in nature and
hence the reason why appropriate signal processing is
required for interpreting and using the signal.
Although the amplitude is random, it can be
reasonably represented by a gaussian distribution
function. The typical EMG amplitude varies from
microvolts to the low millivolts range (with the
maximum amplitude being around 10mV peak-to-
peak). The amplitude depends on the force applied
since the bigger the force, the more action potentials
will be stimulated which will trigger the contraction of
more muscle fibres (Naeem, 2012).
The more the action potentials are in reach of the
surface electrodes, the bigger the product result and
Seguna, C., Von Brockdorff, A., Scerri, J. and Scicluna, K.
Classification of Five Finger Movement, based on a Low-cost, Real-time EMG System.
DOI: 10.5220/0008978901490159
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 1: BIODEVICES, pages 149-159
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
149
therefore the higher the amplitude. The frequency of
EMG signals can range from a few hertz up to the
lower kilohertz range, but the frequencies below 20 Hz
and above 200 Hz are usually not considered to
contain any useful physiological information. For this
reason, EMG acquisition systems normally filter these
frequencies out. Since the 50 Hz power line frequency
is within this range and can contribute to interference
in the EMG data being analysed, it is sometimes
recommended to set the cut-off frequency of the low-
pass filter at 50 Hz to attenuate most of the power lines
interference, or else apply a notch filter at that
particular frequency (Khoshaba, 1990), (Ahmad,
2017). The EMG signal can also contain small DC
contents producing an EMG signal with a non-zero
baseline. The DC content is eliminated in the EMG
acquisition circuitry, usually by using an
instrumentation amplifier (IA) or a high-pass filter
(Hong Quach, 2017).
Table 1: Applications of EMG (Côté, 2015).
Medical
research
Rehabilitation Ergonomics
Sports
Science
Orthopedic Post-surgery
Analysis on
Demand
Biomechanics
Surgery
Neurological
Disorders
Risk
Prevention
Movement
Analysis
Functional
Neurology
Physical
Therapy
Ergonomics
Design
Athletes
Strength
Training
Gait &
Posture
analysis
Active
Training
Therapy
Product
Certification
Sports
Rehabilitation
Common EMG analysis techniques include amplitude
analysis, time duration analysis, frequency analysis
and time-frequency analysis. The amplitude of the
EMG signal expresses the level of the muscle activity
and it changes with the amount of electrical activity
detected by the electrodes. EMG acquisition systems
usually make use of techniques to smoothen the raw
EMG signal amplitude and form a better
representation with respect to time. The most common
techniques are the Root Mean Square (RMS) followed
by the Mean Absolute Value (MAV). The RMS
technique is considered to be the most meaningful
since it provides a measure of the power of the raw
EMG signal (Tijssen, 2000).The ability to correlate
EMG amplitude with muscle force allows one to
determine whether the respective muscle is inactive or
active. When a muscle is inactive, the EMG amplitude
is effectively at 0 V and when the muscle is active, the
amplitude gets greater than 0 V. When a muscle is
active, one can also determine the time duration of the
muscle being active. This is achieved by simply
measuring the time when the amplitude exceeds a pre-
set threshold. Frequency analysis applies Fast Fourier
Transform (FFT) technique to obtain meaningful
frequency information, for a fixed stationary time-
domain data segment. This factor makes frequency
analysis not the ideal method when fast data
processing is required, such as for the use of prosthetic
limbs. On the other hand, this type of analysis is ideal
for studying muscle fatigue since in various studies it
has been proven that the mean frequencies of the EMG
signal will decrease with time during tasks that induce
muscle fatigue. The frequency analysis can also be
used for detecting interfering frequencies in the raw
signal, such as power line frequencies. Time-
Frequency analysis comprises the study of EMG
signal in both the time domain and the frequency
domain simultaneously. As already discussed, both
the time domain and frequency domain analysis can
be used to extract specific muscle activity. For this
reason, many researchers have combined the two to
benefit from information the two types of domains can
offer. This type of analysis is sometimes used to
achieve multiple classifications from the same EMG
signal, such as the angle and the force applied at a
joint. This is because the muscle force show more
change in the time domain, while any change in the
joint angle is more visible in the frequency domain of
the EMG signal (Clancy, 2008). During the process of
EMG signal acquisition one must follow certain steps
to prevent unwanted factors that may influence the
process. Although the human body is a good
conductor of electricity, there are still many aspects
that effect the conductivity level. Tissue conductivity
level can vary with the type, thickness, physiological
changes and even with temperature. These conditions
will vary from one person to another and sometimes
may even vary within the same person when the test is
performed at different time. Additionally, the human
body has approximately 640 skeletal muscles which
are close to one another, it is difficult to monitor
signals originating from a single muscle when using
surface electrodes. Neighbouring skeletal muscles
may produce signals which will eventually be picked
from the electrodes together with the wanted signals.
This is known as cross-talk, and normally it does not
exceed 15% of the overall signal contents.
Electrocardiography (ECG) signals can also interfere
the EMG signal recording. This is especially common
when performing EMG monitoring near the upper
trunk or the shoulder muscle. Another factor that may
alter EMG reading is when the distance between the
skeletal muscle belly (origin of the signal) and the
surface electrode changes during the signal acquisition
process. This normally happen when the patient
BIODEVICES 2020 - 13th International Conference on Biomedical Electronics and Devices
150

moves which causes the electrode to change position.
To prevent this from happening, one must secure the
surface electrodes and any wires that may cause them
to move during signal monitoring. The EMG signal
whose amplitude is between 0-10mV, when passing
through various tissues, is contaminated by various
noises (Amrutha, 2017), (De Luca, 2010), (Guohua,
2009).Therefore, it is vital to understand the properties
of various unwanted electric signals. EMG signals are
very sensitive to external noise and artifacts, mainly
due to the signal ranging from a few microvolts.
Inherent noise present in all electronic equipment
cannot be eliminated but can be reduced drastically
through intelligent circuit design. Additionally, the
silver/silver chloride electrode are electrically stable
and as their size increases, the impedance decreases.
Most of these interferences may be filtered out using
active or digital filters, by preparing the skin and
placing the electrodes properly. If proper skin
preparation and proper electrode placing is not
fulfilled signal quality is deteriorated. The electrode
cable and interface will also cause movement
artefacts, where such artifacts can be reduced
significantly using recessed electrodes. Further to this,
between the surface of the skin and the electrode-
electrolyte interface, a conductive gel layer is applied.
Electrical noise causes EMG interference since most
of the electronic components generate electrical noise
(known as Johnson–Nyquist noise) whose frequency
can range from few hertz to thousands of hertz. Such
electrical noise can be reduced drastically by using
quality components and through the implementation
of a well-designed circuit. Ambient noise is the main
source of electromagnetic radiation whose amplitude
is sometimes one to three times greater than the
desired EMG signal.
The surface of the human body is constantly
flooded with electromagnetic radiation. To prevent
these interferences, one must use an IA with a high
CMRR. This will attenuate any common mode noise
at the inputs of the electrodes. Another technique to
reduce ambient noise is to use the shortest possible
leads. If long leads are used, they will serve as an
antenna which will pick any ambient noise in the
vicinity. The leads should also be shielded to reduce
the possibility of noise from being picked. If noise
problems persist, the EMG acquisition circuit can be
covered by a Faraday cage. This will shield the circuit
from any Electromagnetic interference (EMI). When
the Faraday cage is grounded, the electric field energy
is drained away without affecting the circuit
performance. EMG instrumentation can pick various
types of influences that one may not even be aware of,
which include emotions and thoughts. These factors
can cause skeletal muscles to slightly contract since
humans tend to tighten up with certain emotions or
thoughts. These influences are better known as
involuntary activities which are picked by an EMG
measuring equipment (Bekir, 2014). There are
various techniques used to process and classify EMG
signals. Researchers make use from both the
amplitude and the spectral properties of the raw EMG
signals to supplement information on the muscle
activity which is used to increase the classification
accuracy. Following are some of the commonly used
techniques for signal acquisition, processes used and
algorithms for eliminating unwanted artefacts,
process the raw EMG signals and for classifying
different muscle movements. EMG signals can be
picked up using surface electrodes in two different
configurations, these being the monopolar and the
bipolar. The monopolar configuration makes use of
two surface electrodes, where one is placed on the
belly of the muscle and the other electrode is placed
as a reference on an electrically neutral tissue (such
as joints or other bony areas). The difference of the
two electrodes is then compared and processed for
further filtering and smoothing (Hudgins, 1993). The
other technique is the bipolar. This configuration
makes use of two electrodes (known as the detecting
electrodes) which are both placed on the belly of the
muscle. The detecting electrodes are typically kept
one to two centimetres apart. Another electrode is
used as a reference and must be placed on an
electrically neutral tissue. The advantage of using this
configuration is that the common noise can easily be
eliminated, something which is not possible to
achieve with the monopolar configuration. When
eliminating the common noise or any interference,
one will achieve a better signal-to-noise ratio and
hence a clear raw EMG signal can be obtained. The
pre-amplification is one of the most important aspect
when it comes to processing very low signals such
that of EMG. This is because the components used in
this stage must be of high precision and produce the
minimum noise possible, or else the noise can be
interpreted as the wanted signal. The most common
pre-amplification component used in EMG devices is
the instrumentation amplifier. Instrumentation
amplifiers are used to amplify the difference between
two inputs, which are connected to the two detecting
electrodes. They are designed to reject any signals
that are common to both inputs and therefore, are
used where precision and gain accuracy must be
maintained within a noisy environment, and where
large common-mode signals are present. After
reviewing the literature, it was found that the most
commonly used instrumentation amplifiers for EMG
Classification of Five Finger Movement, based on a Low-cost, Real-time EMG System
151

devices are the INA126P, INA128, INA141, AD8221,
AD8421, AD623 and the AD642. Some papers
suggest that the IA gain must not be set too high or
else it may amplify the noise components together
with the wanted signal. Most of the EMG devices set
the instrumentation amplifier reference pin to half the
supply voltage (virtual grounding), while other
devices keep the output of the IA at a zero volts
baseline and then rectify the EMG signal prior
entering the ADC input. An experiment conducted by
the University of Utah includes the use of precision
rectifiers (super diodes) to rectify the raw EMG signal
prior inputting it to the IA. Other techniques were
used in other studies, which include the use of three
separate operation amplifiers that form the IA which
permits more flexibility in the selection of parameters.
After the pre-amplification stage, most devices
perform filtering to remove unwanted signal prior
further processing. Different EMG devices divide this
section into different stages, with some using separate
circuit for the low-pass and high-pass filtering, others
make use of a band-pass filter circuit and other
devices perform this task either on a microcontroller
or desktop computer. Digital filtering is usually
performed using Infinite Impulse Response (IIR)
filtering structure or Finite Impulse Response (FIR)
filtering structure, with the latter being the most
popular since it is more stable and less likely to
introduce non-linear phase distortions.
Most of the existing devices which make use of
hardware filtering, achieve this by using active filters
based on operational amplifiers or by using dedicated
filter ICs. Some EMG data acquisition
implementations make use of a combination of a low
order hardware filtering stage, which is then followed
by a higher order software filter. This is usually done
so that the hardware filtering can perform the first
stage filtering, prior the signal is inputted to an
analogue to digital converter (ADC). Another
technique would be the use of an adaptive noise
cancellation. Such technique can be implemented
using the Least Mean Square algorithm and has been
proved to be reliable and efficient (Phinyomark,
2012).
This will contribute to better ADC processing
since it will eliminate any major baseline drift and
high amplitude noise. Further filtering of the EMG
signal is then achieved by a second stage digital filter.
Some existing devices also make use of notch filters
to attenuate any frequencies that may interfere with
the wanted signal, with the most common being the
50 - 60 Hz power line frequency. This type of filtering
is not suggested by some researches since the
frequencies in the 50-60 Hz range can contain useful
information on the muscle contraction. They suggest
that a high-end instrumentation amplifier with a high
CMRR should be used instead. This should attenuate
any common power line distortion picked up by the
human body.
Although many studies agreed that the low-pass
filter (LPF) cut-off frequency should be set to around
15 to 50 Hz, it was noted that when it comes to the
high-pass filter (HPF) cut-off frequency, different
papers used different values with the range varying
from 150 Hz up to 800 Hz. Some of the papers
recommend that a high cut-off frequency for the HPF
is preferred so that any rapid on-off bursts of EMG
activity will not be filtered out. EMG devices which
perform hardware smoothing need to first rectify the
signal. Some existing devices use half-wave
rectification, but the most popular is the full-wave
rectification. Devices that use full-wave rectification
have the advantage of maintaining all of the raw EMG
signal information, unlike half-wave rectification
where the negative cycles are completely blocked. The
common technique used for the signal rectification is
through the use of a precision rectifier (also known as
a super diode) which is a circuit that acts as an ideal
rectifier.
The stage following the EMG rectification, is
usually the signal smoothing stage which is normally
achieved through an integrator circuit or a low-pass
filter. A similar technique which is also commonly
used is the envelope detector circuit, which gives a
similar output effect as the integrator and the low-pass
filter circuits. There are other techniques which are
sometimes used instead of root-mean square (RMS),
these being the Absolute Mean Value (AMV), the
Difference Absolute Mean Value (DAMV) and the
Variant Value (VAR) (Garavito, 2016). A study
entitled “Evaluation of EMG processing techniques
using Information Theory” shows that the RMS
technique provides the most meaningful information
out of the EMG signal.
More complex EMG processing devices can make
use of different algorithms to achieve better results.
Some of the commonly used algorithms are the Neural
Network, the Support Vector Machine and the
Euclidean Distance. The last two algorithms are
typically used when monitoring and recording finger
movements. They are used to isolate individual finger
movements to be able to control individual outputs,
such as prosthetic limbs. On the other hand, Neural
Networks (Subasia, 2006), (Gutiérrez, 2011)
algorithms are artificial intelligence networks that can
acquire any non-linear mapping of trained data
through learning. This algorithm is normally used to
achieve successful classification for non-stationary
BIODEVICES 2020 - 13th International Conference on Biomedical Electronics and Devices
152

EMG signals. Euclidean distance is used to determine
the distance of the input data points from a set of
predefined target points. Based on the distance
acquired, the system will check if the new data input
lies within a pre-defined target border and is used to
classify the data related to a particular muscle activity
into the desired group of channels.
The concept of autoregressive modelling is to
assume that the real EMG can be approximated by
what is known as the AR process. With this
assumption settled, the order and parameters of the
appropriate autoregressive model are chosen in a way
to fit the acquired EMG signals as closely as possible.
In turn, for every particular autoregressive model, the
power spectrum of the corresponding AR process can
be analytically determined. Thus, the AR method
provides an alternative way for EMG spectral
properties estimation. The work entitled “Real-Time
Computer Control using Pattern Recognition of the
Electromyogram” claimed a 95% accuracy in
classification was achieved when using the
Autoregressive modelling technique.
2 ANALYSIS OF EMG SIGNALS
Analyses of various EMG signals was done using a
pair of electrodes placed over the palmaris longus
muscle, which is mostly active when the ring finger
is contracted. The raw EMG signal was processed
through root mean square calculation. Figure 1
illustrates the result of the processed signal where it
is observed that the amplitude increases relatively
proportional with every 10 N of extra force applied.
This signal feature can be utilized in prosthetic hands
to apply variable force depending on the EMG
amplitude.
Figure 1: RMS of the EMG bursts with different forces,
starting from a force of 1 kg and increasing the force by 1 kg
with every burst.
The amplitude and frequency components of the ring
finger being closed at different angles were analysed.
Figure 2 illustrates the EMG signals obtained at
different angles, starting from 0 degrees (finger fully
opened) up to an angle of 180 degrees (fully closed),
with intervals of 45 degrees. The rectified EMG signal
amplitude increases quasi-proportional with the angle
of the finger. This feature can be utilised for prosthetic
hands for adjusting individual finger angle. A test was
conducted to analyse the EMG signal pattern with
respect to muscle fatigue. The setup used is shown in
Figure 3.
Figure 2: Rectified EMG amplitude signal at various finger
angles, starting from angle 0 degrees (finger fully opened)
up to an angle of 180 degrees (fully closed).
Figure 3: Setup for analysing EMG signal pattern with
respect to muscle fatigue.
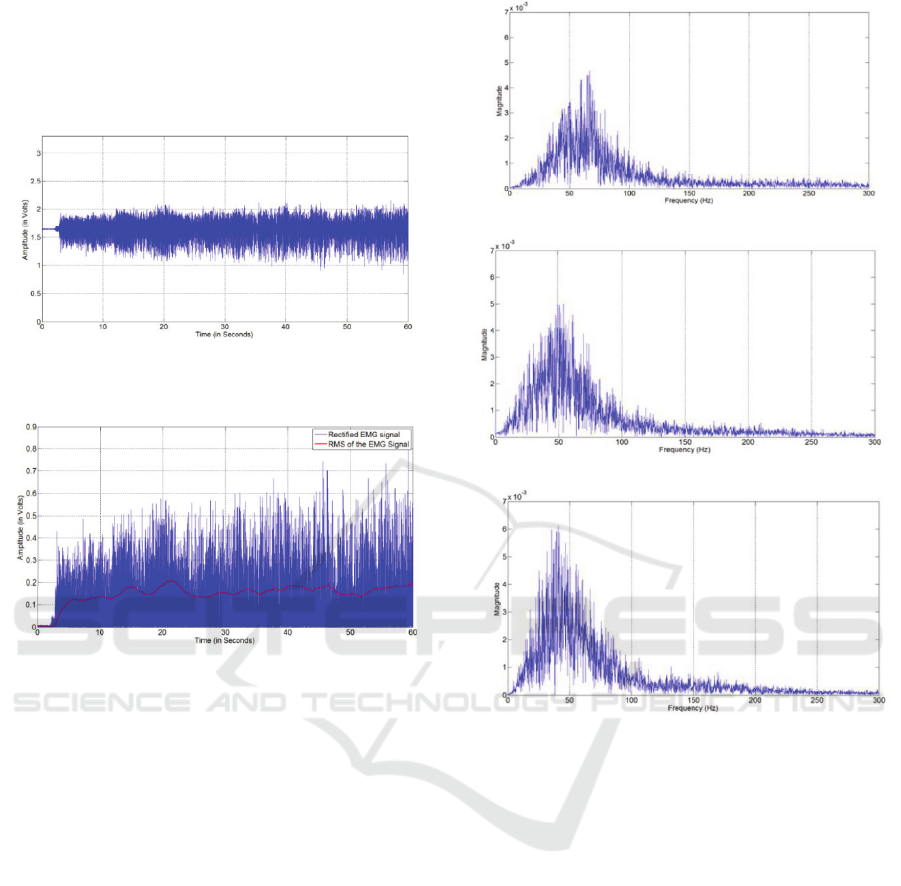
The EMG signal for this test is shown in Figure 4. The
RMS equivalent is illustrated in Figure 5 showing the
profile of an EMG signal obtained for the ring finger
when a constant force of 5 kg for a period of 60
seconds was exerted. As shown in Figure 5 the
amplitude of the EMG signal increases slightly with
muscle fatigue when applying a constant force of 5 kg.
Therefore, since the difference in amplitude is
minimal the signal was then analysed in the frequency
domain where it was noticed that the frequency of the
EMG signal shifts to the lower side with muscle
fatigue as shown in Figure 6.
The amplitude frequency spectrum was performed
on a raw EMG signal at various angle position of the
finger. Figure 7 illustrates the magnitude frequency
spectrum plots obtained for four different ring finger
angles. From the results obtained, the magnitude of the
Classification of Five Finger Movement, based on a Low-cost, Real-time EMG System
153
100 Hz frequency bin increased with angle position.
Frequency domain analysis could be challenging to
apply with accuracy due to problems such as
frequency resolution, magnitude accuracy at steady
state, and more generally, due to data processing.
Figure 4: EMG signal pattern with ring finger exerting a
constant force of 50 N.
Figure 5: RMS of the EMG signal with the ring finger
exerting a constant force of 50 N.
The time domain feature analysis is concerned with
the extraction of various EMG signal features in time
domain. Time domain features such as mean absolute
value, root mean square and wavelength were the most
popular in EMG pattern recognition because of high
processing speed in classification. The mean absolute
value of an EMG signal is defined as the average of
the total absolute value, while root mean square is the
amplitude modulated Gaussian random process
related to muscle force and contraction Time domain
features can easily and efficiently be used for the
recognition of an EMG pattern recognition. On the
other hand, frequency domain features can be used to
estimate the EMG power spectrum in frequency form.
In addition, the frequency domain spectrum is
commonly used in muscle fatigue and muscle force
estimation. Therefore in this work the classification of
finger movement was performed through the time
domain analysis rather than frequency spectrum.
(a)
(b)
(c)
Figure 6: Frequency spectrum shifting to the lower side of
the spectrum with muscle fatigue for various time durations
(a) 5-15 (b) 15-25 (c) 35-45 seconds.
3 CLASSIFICATION OF FINGER
MOVEMENT
H124SG muscle sensor surface electrodes were
placed at a particular area on the hand as shown in
Figure 8. The forearm has nineteen major muscles
responsible for the flexion, extension and other
movements of the fingers, wrist and elbow.
Reviewing the anatomy of the muscles, it was
concluded that the muscles used for the contraction of
the fingers are mostly exposed at the lower part of the
forearm Muscles responsible for finger movement
include the flexor digitorum superficialis (responsible
for
flexing all fingers -primarily at proximal
interphalangeal joints), flexor digitorum profundus
BIODEVICES 2020 - 13th International Conference on Biomedical Electronics and Devices
154
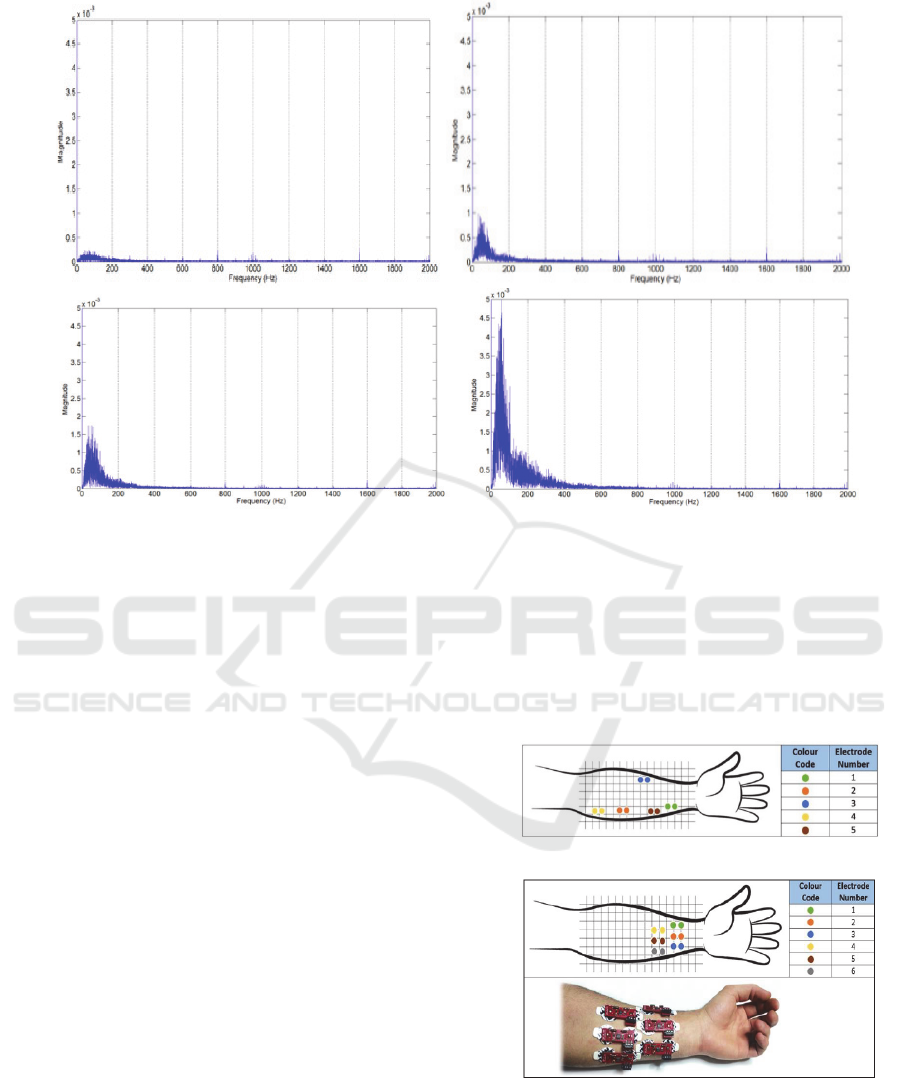
Figure 7: Frequency magnitude spectrum of an EMG signal for (a) 0°, (b) 90°, (c) 135°, and (d) 180° ring finger angle position.
(responsible for flexing the distal and proximal
interphalangeal joints) and flexor pollicis longus
(responsible for flexing the thumb).
This work covered two different experiments. In
the first experiment the electrodes were placed along
various muscles as shown in Figure 8a, while in the
second experiment six electrodes were placed on the
lower part of the forearm. The first experiment did not
show repeatable results from person to person. This
was mainly caused by the fact that not every person
has the same muscle anatomy and not every person
has the same amplitude peaks for the same muscle.
The physical factor of the person also played a big role
in the lack of consistency. When the system was used
on overweight people, it was noticed that it is difficult
to get finger movement classification. This is due to
the constantly changing physical distance between the
surface electrodes and the muscles being monitored.
To avoid the use of complex algorithms and other
additional signal processing for isolating finger
movements from other unwanted muscle activities,
such an area was selected. Calibration process
followed electrode placement. This process consisted
of contracting each finger multiple times one at a time.
With each contraction, the amplitudes acquired
from all electrodes being recorded. This process was
repeated for a pre-defined amount of repetitions so to
establish the required thresholds. EMG bursts were
monitored and processed so to evaluate the upper and
lower thresholds for each finger contraction, with the
highest monitored amplitude being set as the upper
threshold and the lowest amplitude being set as the
lower threshold. The maximum and minimum
amplitudes detected at each electrode after the raw
square algorithm.
(a) First Experiment
(b) Second Experiment
Figure 8: Electrode placement for (a)1
st
and (b) 2
nd
Experiment.
Ten EMG bursts were recorded during this
calibration procedure. From the plots shown in Figure
9, it is observed that the thresholds for each finger
(c)
(d)
Classification of Five Finger Movement, based on a Low-cost, Real-time EMG System
155
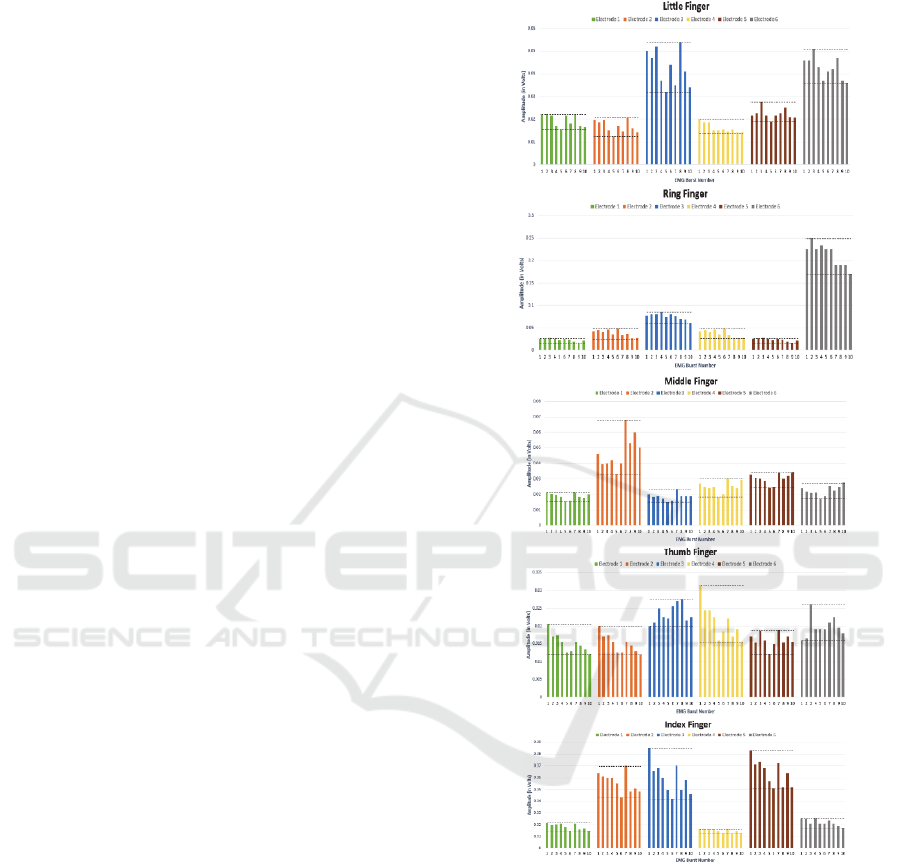
contributed to a unique pattern thus enabling EMG
signals were processed using the root mean- the
possibility of classifying various finger movements.
4 ACTIVE ELECTRODES FOR
ECG
Most EMG devices use of passive electrodes. In this
work active electrodes were used because they tend
to perform better for applications where very low
signals need to be acquired. Active electrodes
contribute to a have high input impedance with
minimal stray-capacitances at the inputs and low
output impedance contributing to a low cable
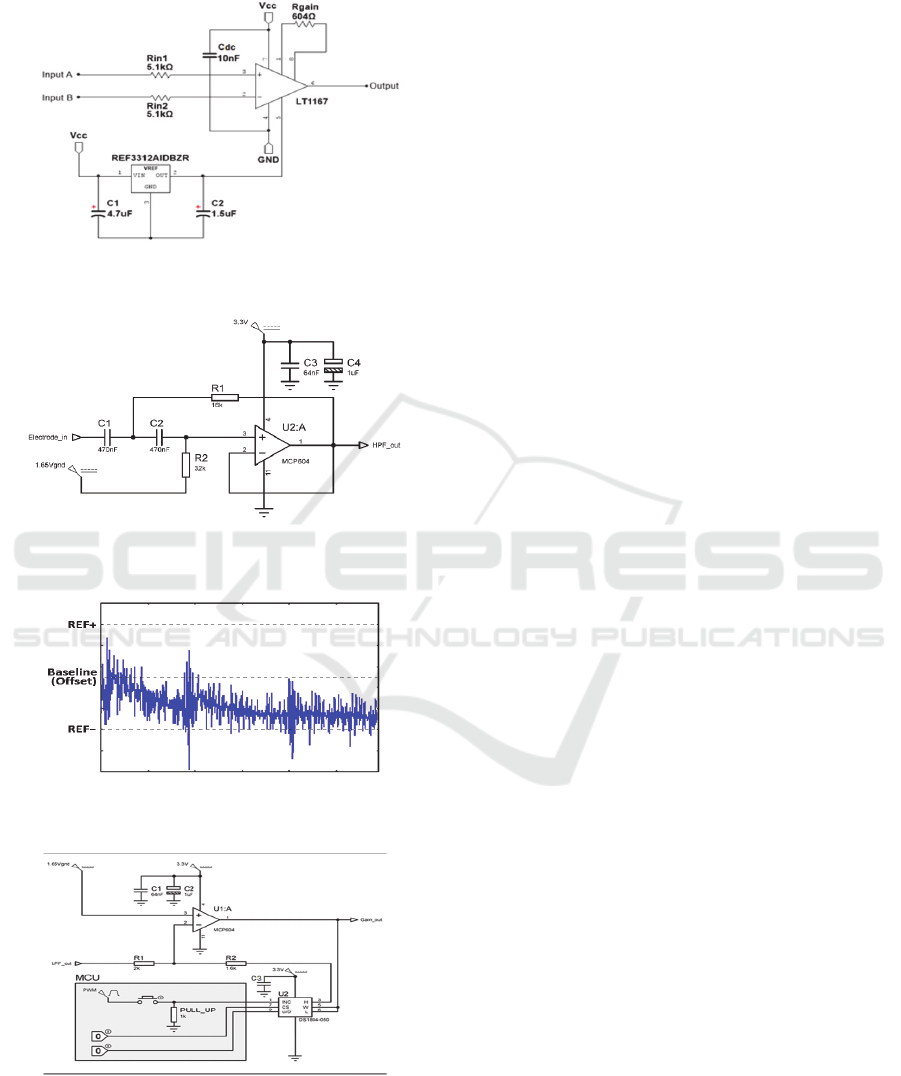
movement artifact. As shown in Figure 10 the main
front-end component for the developed active
electrode module is the LT1167 instrumentation
amplifier (IA). The LT1167 operates with a single or
dual rail supply voltage of ±2.3 V, common-mode
rejection ratio (CMRR) of 126 dB, and input
impedance of 1000 GΩ, thus contributing to less
attenuation in the input signal. Such parameters
satisfy the Surface Electromyography for the Non-
Invasive Assessment of Muscles (SENIAM) standard.
To minimize the gain error and achieve best CMRR
the REF pin of the LT1167 was connected to a 1.25
V supplied by the REF3312AIDBZT voltage
reference IC. This IC required low supply current
(typically 3.6 μA), has low temperature drift and has
an internal accuracy of ±0.15%. The maximum output
impedance does not exceed 0.1Ω, assuming the
output of the REF3312 is not switching at high
frequencies. This integrated circuit is also suggested
for use in medical applications. A 4.7 μF and 1.5 μF
supply bandpass capacitors are connected to the input
and output of the REF3312 respectively for better
stability of the input and output signal. A 604 Ω
resistor is used to set a fixed gain of 83. Note that this
gain will only amplify the raw EMG signal to around
500 mV peak-to-peak as per requirement. The two
5.1 kΩ resistors connected in series to each input of
the instrumentation amplifier input. These resistors
are made from carbon composition which can
withstand large short-term pulses and high voltages
when compared to other resistor types. Although
these resistors will contribute to higher noise at the
inputs of the IA, they are necessary to protect the IC
from any ESD.
The filtering stage consists of a 2
nd
order
Butterworth high-pass filter with a cut-off frequency
of 15 Hz, a 5
th
order low-pass filter with a cut of
frequency of 500 Hz. A digital amplifier followed
the filtering stage.
Figure 9: RMS and threshold plots for various finger
movements.
The high-pass filter is required so that the baseline
drift will not affect the ADC performance. The
operational amplifier for the active high-pass filter
selected is the MCP604, which is a single supply, rail-
to-rail, unity gain stable CMOS quad op-amp IC.
Such component has a Butterworth response and can
operate at 3.3V, while consuming maximum current
of 1.2mA. The input of the filter comes directly from
the electrode, which pre-amplifies the raw EMG gain
accordingly. DS1804-050 is a 50kΩ potentiometer
BIODEVICES 2020 - 13th International Conference on Biomedical Electronics and Devices
156
that has 100 tap-points. The DS1804-050 can operate
from 3V or 5V.
Figure 10: Schematic diagram for the front-end component
interfaced with active electrodes.
Figure 11: Low-pass filtering stage based on the MAX7414
5
th
order LPF.
Figure 12: Baseline drift causing the EMG signal to be
saturated by the ADC references.
Figure 13: Digital Potentiometer.
This digital potentiometer also has a built in
EEPROM to store the wiper position even when the
supply is disconnected. This is useful so that the
system will not have to be re-calibrated every time the
supply is turned off. The DS1804 is specified to
provide an absolute linearity of ±0.60 LSB, which is
irrelevant for this application. It has a -3dB cut-off
frequency of 200 kHz. Since the EMG frequencies are
low, 200 kHz are enough for this application.
Developed software monitors the signal amplitudes
from each electrode and adjust the gain accordingly
through the digital potentiometer. Such technique will
not require the user interaction. The digital amplifier
circuitry consists of the DS1804-050 and the
MCP604 operational amplifier (same op-amp IC used
for the high-pass filter). The op-amp is configured as
an inverting amplifier, which can vary the gain from
1 (unity) up to 25. The MCP604 can be supplied with
a single rail supply between 2.7 V to 5.5 V. The
inverting configuration was used, so to implement a
linear gain amplification, by incrementing the
feedback resistance at equal intervals. The non-
inverting input of the op-amp is connected to a 1.65V
reference supply to offset the output by half the
supply voltage.
5 CONCLUSION
In this work, we proposed the successful
implementation of an active, noise cancelling,
affordable and wearable 6-channel sEMG data
acquisition system for the detection and classification
of finger movement. Such classification feature can
be combined with other systems for myoelectric
control applications. Additionally, unlike other
systems the gain is auto-adjusted using a digital
amplifier. Finger movement can be detected and
classified easily via EMG time domain rather than
frequency domain analysis. The most basic and
effective algorithm for enveloping the raw EMG
signals was found to be root-mean-square (RMS)
with a wide averaging window of 3000 instead of
1000. RMS only requires basic mathematical
calculations, which sums up in a system that requires
less processing power. As a result, a wider selection
of microcontrollers could be used for processing
EMG signals. The classification of finger movement
was done through the placement of six electrodes at
the lower part of the forearm. For this experiment,
there was no need for the electrodes to be placed
precisely in a specific area. The forearm was selected
because it has thin layer of fat, thus reducing the
problem of baseline drift drastically. After studying
the anatomy of the muscles, it was also concluded that
the muscles used for the contraction of the fingers are
Classification of Five Finger Movement, based on a Low-cost, Real-time EMG System
157

mostly exposed at the lower part of the forearm. The
developed active electrodes with integrated IA placed
as close as possible to the input electrodes contributes
a better signal to noise ratio. The use of an auto-
adjustable gain stage contributed to a practical user-
friendly system. This circuit monitors the maximum
EMG signal amplitude and adjusts the gain stage
accordingly, without any user interaction. This
ensures that the gain is always adjusted to get the most
effective performance from the ADC module since
the signal will be neither too low in amplitude to
cause inefficient use of the ADC resolution, not too
high to cause saturation of the signal. A comparison
of our active electrode sEMG processing system with
other systems available in the literature and
commercial products in terms of frequency, weight,
supply voltage, wearable and other classification
features is shown in Table 2. Through extensive
experimentation system was tested by ten different
people of various weights, size and genders with
classification results observed to be repeatable and
reproducible.
6 FUTURE WORK
A small footprint prototype board is currently under
development and planned to be finalized by 2020.
This new prototype will enable the extraction of more
finger muscle movement features including finger
angle and muscle fatigue. Additionally, such a
wearable module will enable the processing of EMG
signals wirelessly over the cloud so to help of patients
suffering from conditions such as Carpal Tunnel,
Diabetic Peripheral Neuropathy, Ulnar Neuropathy,
Chronic fatigue syndrome, and Fibromyalgia, among
others.
Table 2: Comparison with other similar systems.
This
work
Myo
Armband
Biometrics
Datalog
Hercules
(Mert, 2018)
Classification
of Finger
Movement
Yes No No No
Contraction
Detection
Yes No No Yes
Wearable Yes Yes No Yes
Bandwidth (Hz) 20-589 - 20-460 20-500
Supply Voltage 2.5V - 3V 3.7V
REFERENCES
Seguna, C., et al., “Development of a New Low-Cost EMG
Monitoring System for the Classification of Finger
Movement”, 2018 New Generation of CAS (NGCAS),
pp. 126-129, 2018.
Tsuji, T., et al., “Pattern classification of time-series EMG
signals using neural networks”, International Journal of
Adaptive Control And Signal Processing, pp. 829-848,
2000.
Sudarsan. S., et al., “Design and Development of EMG
Controlled Prosthetics Limb”, International Conference
On Modelling Optimization And Computing, p. 3547-
3551, 2012.
Osamu, F., “A Human-Assisting Manipulator Teleoperated
by EMG Signals and Arm Motions,” IEEE transactions
on Robotics and Automation, vol. vol 19, no. 2, APRIL
2003.
Jingpeng. W, et al., “Surface EMG Signal Amplification
and Filtering”, International Journal of Computer
Applications, November 2013.
Côté, J., Electromyography (EMG): Intro to The Muscle
Activity Assesment Technique, Sept 2015.
Naeem, U. J., et al., (2012). “EMG-muscle force estimation
model based on back-propagation neural network”,
IEEE International Conference on Virtual
Environments Human-Computer Interfaces and
Measurement Systems (VECIMS) Proceedings, pp.
222-227, 2012.
Khoshaba. T., et al. “EMG Pattern Classification Based On
Back Propagation Neural Network For Prosthesis
Control”, Proceedings of the Twelfth Annual
International Conference of the IEEE Engineering in
Medicine and Biology Society, pp. 1474 – 1475, 1990.
Ahmad, J., Et al., “Multiclass Myoelectric Identification of
Five Fingers Motion using Artificial Neural Network
and Support Vector Machine”, Advances in Science,
Technology and Engineering Systems Journal Vol. 2,
Issue 3, pp. 1026-1033, 2017.
Hong Quach, J, “Surface Electromyography: Use, Design
& Technological Overview”, Concordia University,
2007.
Tijssen, M. A., et al. “Frequency analysis of EMG activity
in patients with idiopathic torticollis”. Brain: A Journal
of Neurology, pp. 677-686, 2000.
https://doi.org/10.1093/brain/123.4.677.
Clancy, E. A., et al. “Time- and frequency-domain
monitoring of the myoelectric signal during a long-
duration, cyclic, force-varying, fatiguing hand-grip
task”, Journal of Electromyography and Kinesiology,
pp. 789–797, 2008.
Amrutha, A., “A Review on Noises in EMG Signal and its
Removal,” International Journal of Scientific and
Research Publications, Vols. Volume 7,, no. issue 5,
May 2017.
De Luca, C. J., et al. “Filtering the surface EMG signal:
Movement artifact and baseline noise contamination”,
Journal of Biomechanics, pp. 1573– 1579, 2010.
BIODEVICES 2020 - 13th International Conference on Biomedical Electronics and Devices
158

Guohua, L., et al., “Removing ECG noise from surface
EMG signals using adaptive filtering”, Neuroscience
Letters, pp. 14-19,2009.
Bekir, K., et al., “Machine Learning Algorithms for
characterization of EMG Signals”, International
Journal of Information and Electronics Engineering,
Vol. 4, No. 3, May 2014.
Hudgins, B., et al., “A new strategy for multifunction
myoelectric control,” IEEE Trans. Biomed. Eng., vol.
40, no. 1, pp. 82–94, Jan. 1993.
Phinyomark, P., et al., “Fractal analysis features for weak
and single-channel upper-limb EMG signals,” Expert
Syst. Appl., pp. 11156–11163, 2012.
Garavito, F., et al, “EMG signal analysis based on fractal
dimension for muscle activation detection under
exercise protocol,” in Proc. 21
st
Symp. Signal Process.,
Images Artif. Vis., pp. 1–5, 2016.
Subasia. A, et al., “Classification of EMG signals using
wavelet neural network”, Journal of Neuroscience
Methods, pp. 360–367, 2006.
Gutiérrez, J. M., et al. “Wavelet Neural Network as EMG
classifier”, Pan American Health Care Exchanges, pp.
67 – 71, 2011.
Thalmic Labs. (2015). Myo Gesture Control Armband
[Online]. Available: https://www.thalmic.com/en/myo/.
Biometrics Ltd, Newport, U.K., “Datalog MWX8”.
Available: http://www.biometricsltd.com/datalog.htm
Mert, E., et al., “An Embedded, Eight Channel, Noise
Cancelling, Wireless, Wearable sEMG Data
Acquisition System with Adaptive Muscle Contraction
Detection”, IEEE transactions on biomedical circuits
and systems, 2018.
Classification of Five Finger Movement, based on a Low-cost, Real-time EMG System
159
