
Application of Virtual Travel for Alzheimer’s Disease
Hamdi Ben Abdessalem
1
, Alexie Byrns
1
, Marc Cuesta
2
, Valeria Manera
3
, Philippe Robert
3
,
Marie-Andrée Bruneau
2
, Sylvie Belleville
2
and Claude Frasson
1
1
Département d’Informatique et de Recherche Opérationnelle, Université de Montréal, Canada
2
Centre de Recherche de l’Institut Universitaire de Gériatrie de Montréal, Canada
3
CoBTeK Lab, Centre Mémoire, Association IA Université Côte d’Azur, France
{valeria.manera, probert}@univ-cotedazur.fr, frasson@iro.umontreal.ca
Keywords: Healthcare Applications, Sensor Networks Applications, Virtual Travel, Cognitive Environments,
Alzheimer’s Disease, Immersive Environments, Emotions, EEG Sensors.
Abstract: Negative emotions such as anxiety, frustration, or apathy can have an impact on the brain capability in terms
of memory and cognitive functions. This is particularly visible in Alzheimer’s disease where the participants
can have a deterioration of their brain connections which are often the cause of the disorders detected in
Alzheimer's participants. It seems important to reduce these symptoms to allow better access to memory and
cognitive abilities. Immersion in Virtual Reality is a means of providing the participant with a sense of
presence in an environment that isolates them from external factors that can induce negative emotions. The
virtual travel is a method that can mobilize the attention of the subject and revive their interest and curiosity.
We present here, an experiment in which a participant is immersed in a virtual train using a virtual headset
and EEG device to measure the brain signals. To measure the impact of this train on the memory and cognitive
functions, some cognitive tasks have been included before and after the travel. Experiments have been done
on participants with mild cognitive disorder. Preliminary results show an increase of memory functions and
in certain cases of cognitive functions, while negative emotions are reduced.
1 INTRODUCTION
Emotions and motivation play an important role in
cognitive tasks. It is well known that stress or anxiety
during a test can make students forget key
components of the answers or solutions to the
problems they must find. In fact, negative emotions
such as anxiety, frustration, or lack of interest such as
apathy (Robert et al., 2018; Zhu et al., 2019) have an
impact on the brain capability in terms of memory and
cognitive functions. This is particularly visible in
older adults with Alzheimer’s disease (AD) and
related disorders as individuals have reduced brain
reserve which may make them particularly vulnerable
to the effect of negative emotions.
AD is the most common form of dementia and
with the aging population, prevalence increases
dramatically. It is estimated that by 2050, 11 to 16
million persons will be diagnosed with AD in the U.S.
alone (Association, 2015). Despite intensive research,
effective pharmacological treatment has yet to be
discovered. Focus has therefore started to shift
towards non-pharmacological approaches to reduce
the impact of symptoms on autonomy and well-being.
Virtual reality (VR) has proven to be efficient in
treating certain disorders, such as phobia (crowd,
elevators, spiders) and can be used to reduce negative
emotions. The world in which a user is immersed
provides a feeling of safety and encourages
imagination. Also, the user is isolated from external
factors which can induce negative emotions. In this
scope, we have created a virtual train in which
participants are immersed and travel virtually looking
through the windows to the landscape. A major
difference between our approach and the existing
ones which use projection on a screen is that the
participant is equipped with a virtual headset and can
freely navigate in the train, turning their head and
looking around as if they were in a real train. Another
major innovation of our work is that we measured
emotions with an electroencephalography (EEG)
device, coupled with eye tracking techniques to detect
what the subject is looking at. Techniques such as
EEG and eye tracking, have been up to recent years
52
Ben Abdessalem, H., Byrns, A., Cuesta, M., Manera, V., Robert, P., Bruneau, M., Belleville, S. and Frasson, C.
Application of Virtual Travel for Alzheimer’s Disease.
DOI: 10.5220/0008976700520060
In Proceedings of the 9th International Conference on Sensor Networks (SENSORNETS 2020), pages 52-60
ISBN: 978-989-758-403-9; ISSN: 2184-4380
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

(Ben Khedher et al., 2018; Berka et al., 2007;
Maynard et al., 2013; Ben Abdessalem et al., 2019)
mainly used in strict laboratory conditions, but are
increasingly used in realistic emotional and learning
settings (Ben Khedher et al., 2019). Their capacity to
offer real-time qualitatively rich information about
the users' state has tremendous potential to assess
emotions coupled with VR immersion.
We conducted experiments with participants in
older adults with subjective cognitive decline in order
to verify the following hypotheses; H1: is it possible
to reduce negative emotions of the participant
through virtual travel? And H2: Does this system
improve memory and cognitive functions?
The rest of this paper is organized as follows. In
Section 2, we give an overview of the characteristics
of AD. In Section 3 we provide an overview of virtual
immersive environment and our solution with the
virtual train. In Section 4, we detail the experimental
procedure, the cognitive tests and the physiological
sensors that we use, and finally, in Section 5 we
present and discuss the obtained results.
2 CHARACTERISTICS OF
ALZHEIMER’S DISEASE
2.1 Origin of Alzheimer's Disease
Alzheimer's disease (AD) is a neurodegenerative
disease which progressively gets worse over time. Its
most notable symptom is the deterioration of both
short- and long-term memory. The disease also
affects behavior, cognitive abilities as well as
physical abilities in affected individuals. Much
research has been conducted, investigating the causes
and underlying mechanisms of AD. These revealed
the significant role of neural damage in specific
regions of the brain. With the accumulation of this
damage, the disease ultimately interferes with the
individual's capacity to perform activities of daily
living, rendering them dependent of caregivers
(Association, 2015).
The progressive decay characteristic to AD is
suggested to be a result of the gradual loss of structure
and neural function. The affected regions in large part
involve the cortex, the limbic system and the
hippocampus (Association, 2015). These regions play
major roles in memory, emotions and higher-order
functions such as attention and thought. It is proposed
that symptoms of apathy could help identify
individuals at higher risk of the disease (Dubois et al.,
2007; van Dalen et al., 2018). As the disease
progresses, patients begin to display impaired
cognitive and functional abilities, resulting in
difficulties in decision-making, daily tasks,
communication and memory retrieval. Individuals
also experience a decrease in general interest and
often become apathetic. During the final stages of the
disease, patients become practically incapable of
communicating, have difficulty eating and display
extreme apathy (Association, 2015).
AD is also characterized by important atrophy in
distinct regions of the brain. Among the first
structures to suffer brain damage is the hippocampus,
which displays significant neuronal death. With the
hippocampus being a key structure in memory, its
damage is directly linked to memory loss in AD. The
cortex, which is responsible for higher-order
functions such as attention, awareness, thought and
memory, also experiences important atrophy (Pini et
al., 2016).
2.2 The Effect of AD on Non-cognitive
Symptoms and Quality of Life
With time, AD patients become increasingly reliant
of their caregivers and progressively unaware of their
condition. Studies focusing on quality of life of
patients investigated the difference between the
caregivers’ perception of the patient’s appreciation of
life and patient’s own appreciation. The study
revealed that caregivers perceive the patient’s quality
of life as significantly worse than the patient’s own
perception (Zucchella et al., 2015).
Another study investigated the frequency of
positive and negative emotions in both AD and non-
AD patients. The results showed that AD patients
experienced significantly more negative emotions
than non-AD patients (Lawton et al., 1996). With
apathy, confusion and loss of self being marked
symptoms of AD, it is possible that subjective reports
of quality of life from patients tend towards more
neutral levels of appreciation since individuals lose
reference to themselves and can poorly evaluate their
own state.
2.3 Virtual Reality as an Intervention
for Alzheimer’s Disease
There have been many reports revealing benefits in
using VR with AD patients. The dynamic,
multisensory and interactive aspect of VR allows for
a strong ecological validity (Cherniack, 2011). There
is some indication that VR intervention with
computerized cognitive training can improve
Application of Virtual Travel for Alzheimer’s Disease
53

cognitive domains in individuals with mild cognitive
impairment or AD (Coyle et al., 2015; Hill et al.,
2016). Moreover, participants prefer completing
cognitive training tasks in VR over its pencil-paper
counterpart (Manera et al., 2016). It is proposed that
more engaging training will be more effective.
As of now, most studies focus on how VR can
help participants at the cognitive or psychological
level (Appel, 2017; Biamonti et al., 2014; Laforte,
2018). However, a growing body of research is now
investigating the power of VR at a more physiological
level (Todd & Anderson, 2009; Vindenes et al.,
2018). For instance, immersion in a virtual
environment may alter synaptic activity in such a way
as to affect interstitial βA levels (Cirrito et al., 2005)
leading to tangible behavioral and cognitive benefits.
3 VIRTUAL IMMERSIVE
ENVIRONMENTS
3.1 Virtual Reality
Over the last few years, VR started to be used in many
fields due to its remarkable advantages, the major one
being full immersion. In fact, VR tricks the mind of
the users and increases their sense of presence in the
virtual environment. It makes them believe that they
are in a real world and promotes performance
(Biocca, 2006). Therefore, VR is increasingly being
seen as the most interesting way to present an
environment to users.
The main advantage of virtual reality compared to
other interactive environments is that the user is
isolated from external visual distractions. This
technology has been applied in the field of
psychology to treat various disorders, including brain
damage (Rose et al., 2005), anxiety disorders (Gorini
et al., 2008) and alleviation of fear (Alvarez et al.,
2007). For instance, Pedraza-Hueso et al. (Pedraza-
Hueso et al, 2015) introduced a VR system which
consists of different types of exercises with which the
user can train and rehabilitate several aspects
including cognitive capacities.
3.2 The Therapeutic Train: Our
Inspiration
A study published in 2014 (Biamonti et al., 2014)
investigated the impact of a virtual train travel on
people with AD. Installations recreating a fictitious
train station were placed in the retirement home to
simulate a real train station. Older adults participating
in the study were encouraged to take a train ticket at
the fake ticket office, and to wait for the train to arrive
in order to maximize the realism of the trip. The trips
lasted a maximum of 30 minutes and ended when the
train arrived at the next fictional station.
In this study, the researchers tested two different
types of virtual trains: the first prototype consisted of
two wooden doors that opened and led to a room with
two armchairs, a small table and a lamp. To simulate
the "train windows", there were two LCD screens that
showed videos taken by a real train. A total of 20
individuals tested this prototype. The second
prototype was more complex, created in collaboration
with the research group, an architect and therapists.
The appearance of the train was much more realistic,
and the car was isolated from the rest of the retirement
home, which was not the case for the first prototype.
A total of 37 individuals tried this prototype.
For the first prototype, no positive results were
obtained but the second prototype was more efficient.
With its more realistic look, 31 of the 37 participants
who tested the second prototype admitted to being in
a train, while this was the case for none of the
participants who had tried the first prototype. The
results show that the train reduced wandering (in 9 of
the 12 participants with wandering), reduced agitation
(in 8 of the 9 participants with agitation), and
positively influenced anxiety, apathy and sleep
(Biamonti et al., 2014).
3.3 The Virtual Train
The previous environment was not a virtual
environment but a simulation of a real train station.
As indicated in the section above, a virtual
environment could be a great solution to improve the
mood of AD people. The principle of immersion is
crucial for isolating the subject from the real world,
providing a relaxing environment and reducing
negative emotions (which on the other hand can still
be present in a simulated environment such as
Biamonti’s work). So, in order to achieve our first
goal which is reduce negative emotions of the
participant through virtual travel, we started by
designing and creating an immersive virtual travel
environment. To this end, we used Unity3D game
engine which contains a built-in physics engine able
to simulate real aspects of our virtual travel. This
environment represents a virtual train in which the
participants find a happy family sitting next to them
(Figure 1). The virtual train goes through 3 different
environments. The first one is about a forest with
trees and pacific animals.
SENSORNETS 2020 - 9th International Conference on Sensor Networks
54
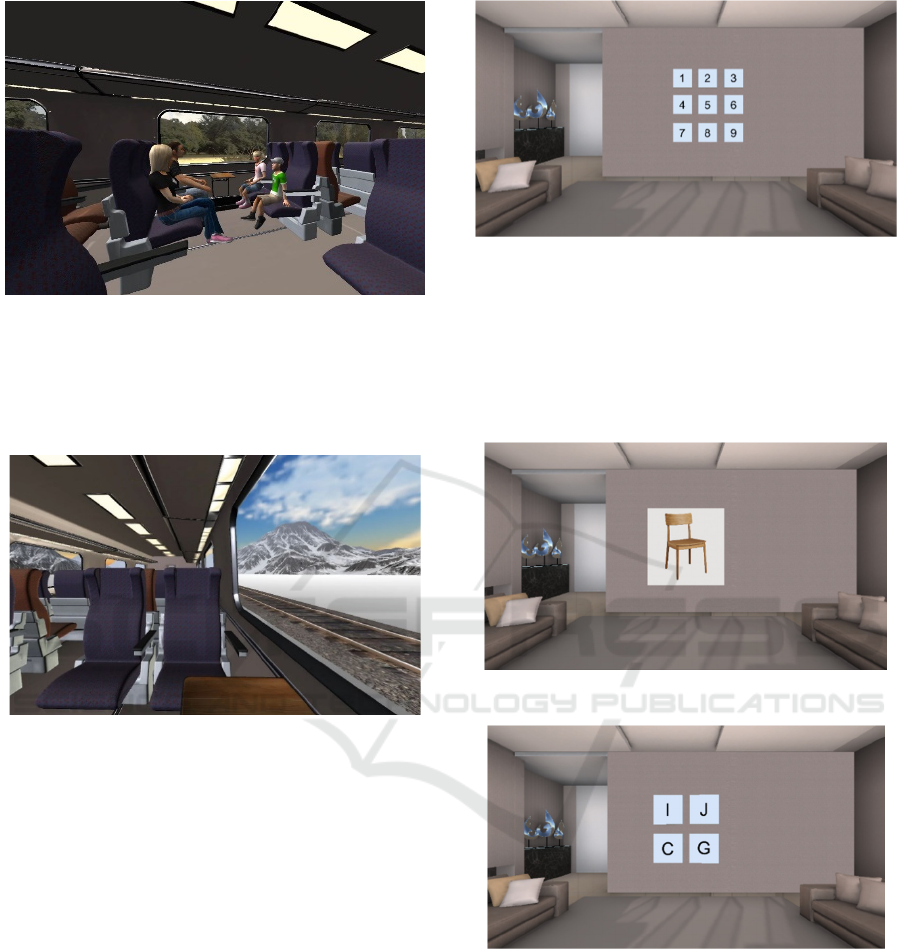
Figure 1: Screen capture of the virtual train.
In the second one, the train goes through a snow
environment with mountains and pacific animals
(Figure 2). The third and last environment is about a
sunny desert with a warm sun.
Figure 2: Screen capture of the virtual train (second
environment).
4 EXPERIMENTS
In order to analyze the impact of the virtual train on
the memory and cognitive performances (particularly
attention), we created 6 attention and memory
exercises.
Attention exercises: In the first exercise, the
participant hears a series of numbers and is asked to
repeat them in the order of presentation using a
numerical pad; they are then presented with another
series of numbers but are now asked to report the
numbers in the backward order. Figure 3 shows how
the participant can interact with this exercise through
the numerical pad.
The second test is a selective attention exercise in
which the participant hears a list of letters at a rate of
one item per second and is asked to click the space
bar every time they hear the letter “A”.
Figure 3: Screen capture of exercise 1.
In the third exercise, we show images of different
objects for a short period of time. The image is then
replaced by a series of four letters and the participant
is asked to select the first letter of the object that was
just presented. Figure 4 and 5 show a screenshot of
the third exercise.
Figure 4: Screen capture of exercise 3.
Figure 5: Screen capture of exercise 3.
Memory exercises: For the first exercise,
participants are asked to memorize a series of objects
presented visually or orally with their name.
Participants are then presented to a series of object
images or words presented auditorily. Participants
are asked to determine whether the object was seen
visually, auditorily or never presented if the object
was not present. For instance, Figure 6 shows an
image of an airplane, and the participant should select
if they saw it, heard its name, or if the object was not
present in the previous sequence. In Figure 6, the
Application of Virtual Travel for Alzheimer’s Disease
55

participant already saw the picture of the plane, so
they select “Deja vu” (already seen in French).
Figure 6: Screen capture of exercise 4.
In the fifth exercise, several circles are presented
to the participant. A series of these circles is
highlighted one by one in order to create a sequence.
The participant is asked to memorize and reproduce
the same sequence. Figure 7 shows a screenshot of the
circles while one is highlighted.
Figure 7: Screen capture of exercise 5.
In the sixth and final exercise, participants are
asked to memorize sets of three pictures for a short
period of time. Then, we present four sets of three
pictures and the participant is asked to select the set
which corresponds to the one they saw. Figure 8 and
9 show an example of this exercise.
Figure 8: Exercise 6: Set to be memorized.
Figure 9: Exercise 6: Four sets from which the correct set
should be identified.
We tested our approach in 19 participants (11
Females) with subjective cognitive decline (SCD)
and a mean age = 69.68 (SD= 5.49). The participants
took part in two sessions. In the first one, they
attended a pre-experiment session (one hour) in
which we made sure that they met eligibility criteria
to make the experiment. Our eligibility criteria were
the following:
Older than aged 60 of age
Francophone
Normal or correct-to-normal vision
Normal hearing
Met the Consortium for the Early Identification
of Alzheimer’s Disease – Quebec (CIMA-Q)
criteria for SCD:
o Presence of a complaint defined as a
positive answer to the following
statements: “my memory is not as good as
it used to be” “and it worries me”
o MoCA 20-30
o No impairment on the logical memory
scale based on the education-adjusted
CIMA-Q cut-off scores.
During the pre-experimental session, participants
were provided with oral and written description of the
study and invited to sign a consent form. The session
then included the clinical tests that are necessary to
confirm diagnosis and characterize participants. If the
participants were eligible, they were invited to the
experiment which took place within the following 15
days.
In the experimental session, the participant was
first invited to fill the Positive and Negative Affect
Schedule (PANAS) scale (Watson et al., 1988) a self-
assessment of emotions, and the questionnaire of
cyber-sickness (Kennedy et al., 1993). We then
equipped participants with an EEG headset. When the
exercises were completed, we equipped them with the
Fove VR headset, and they started the immersive
virtual train experience. The virtual travel lasted
about 5 minutes. Following the virtual travel,
SENSORNETS 2020 - 9th International Conference on Sensor Networks
56
participants completed the cognitive and memory
tests again (using different examples). And they
filled-up the PANAS scale, cyber-sickness,
AttrakDiff 2 (Lallemand et al., 2015), and a self-
report form. The AttrakDiff 2 scale allows to evaluate
the user experience through 28 items on
attractiveness, pragmatic quality and hedonic
qualities (stimulation and identity) of the virtual
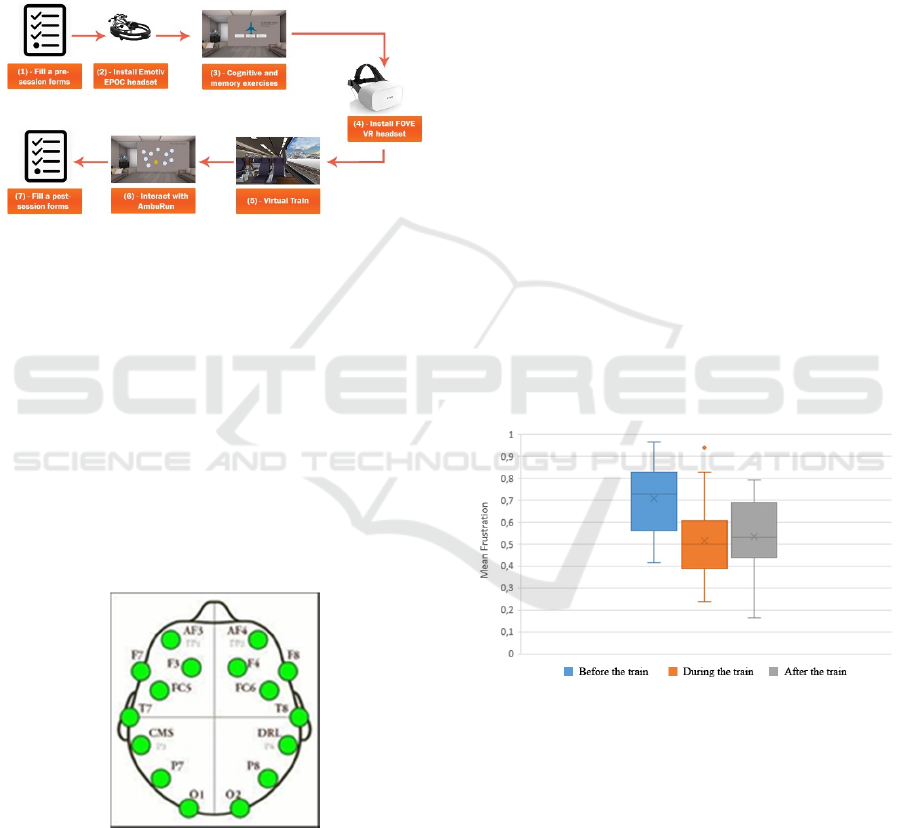
environment. Figure 10 shows the different steps of
the process of the experiment.
Figure 10: Process of the experiment.
4.1 EEG Measures
In this study, we used Emotiv Epoc+ EEG headset
technology to track the excitement of the player. The
headset contains 14 electrodes spatially organized
according to International 10-20 system, moist with a
saline solution. The electrodes are placed at antero-
frontal (AF3, AF4, F3, F4, F7, F8), fronto-central
(FC5, FC6), parietal (P7, P8), temporal (T7, T8) and
occipital (O1, O2) regions with two additional
reference sensors placed behind the ears. The detailed
position of the measured regions is shown in Figure
11.
Figure 11: Emotiv headset sensors placement.
Emotiv system generates raw EEG data (in µV)
with a 128Hz sampling rate as well as the five well-
known frequency bands, namely Theta (4 to 8 Hz)
Alpha (8 to 12Hz), low Beta (12 to 16 Hz), high Beta
(16 to 25 Hz) and Gamma (25 to 45 Hz). Furthermore,
the system uses internal algorithms to measure the
following mental states: mediation, frustration,
engagement, excitement and valence. They were used
to assess the effect of the virtual train on the emotions
of participants.
Even though we don’t have access to the system
proprietary algorithms to infer these mental states
from the raw data and the frequency bands, several
studies have established the reliability of the output
(Aspinall et al., 2015).
5 RESULT AND DISCUSSION
The first objective of this research was to discover
whether it is possible to reduce negative emotions of
the participant through a virtual travel. To this end,
we started by analyzing the emotions of the
participants before, during and after the virtual train
immersion. The results show that the mean frustration
of participants before the therapeutic train was 0.71,
(minimum 0.41 and maximum 0.96). The
participants’ mean frustration during the travel in the
train was 0.51 (minimum 0.24 and maximum 0.94).
After the therapeutic train, the mean frustration was
0.53 (minimum 0.17 and maximum 0.79). Figure 12
shows a boxplot of the mean frustration before,
during and after the travel in the virtual train.
Figure 12: Boxplot of general mean frustration.
Thus, the frustration decreased when the
participants were in the virtual train and the positive
effect on frustration was still observed after the
virtual train. Furthermore, in individuals whose
frustration increased after the train immersion, their
frustration level never reached its prior level.
Individual results are shown in Figure 13, in
which we note that the frustration decrease that was
found when considering the group mean is observed
in 17 of the 19 participants. Only participant 9 and
12 failed to show the effect.
Application of Virtual Travel for Alzheimer’s Disease
57
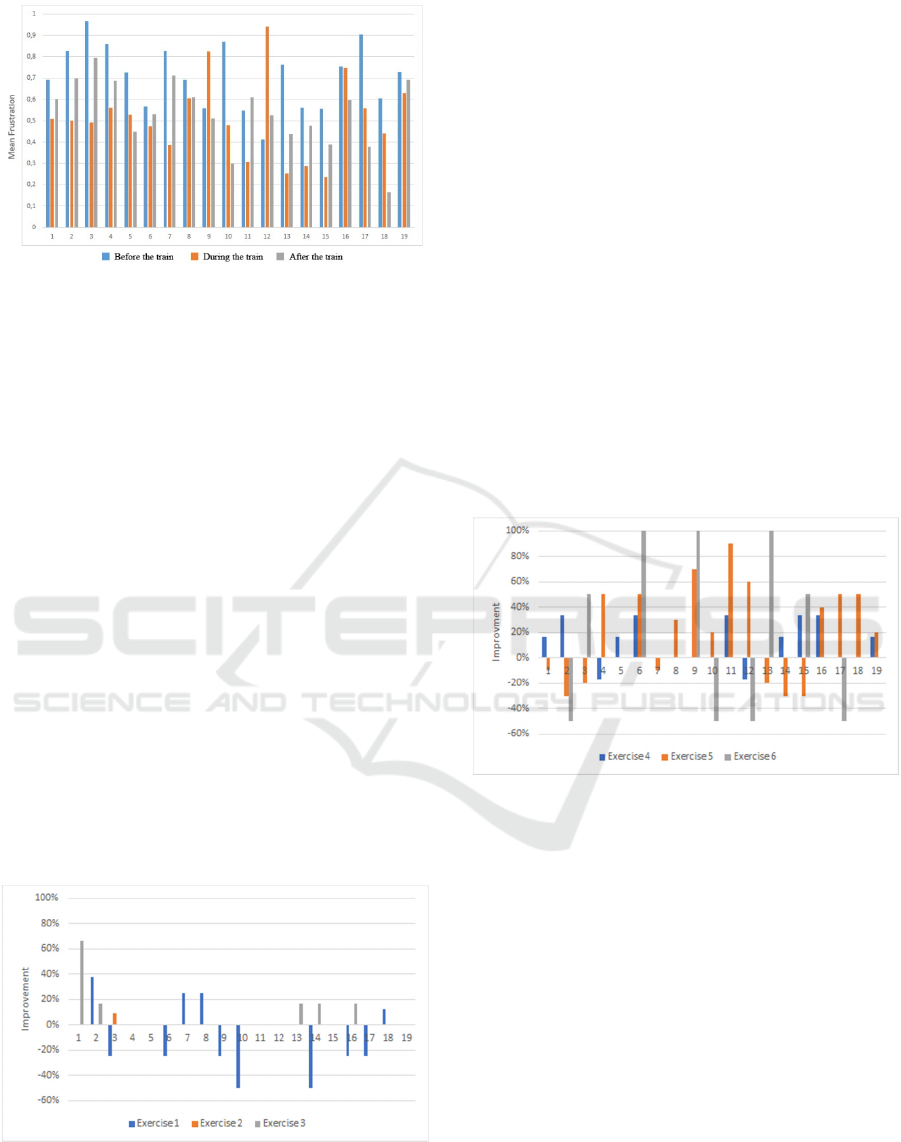
Figure 13: Histogram of mean frustration in individual
participants.
An effect on frustration is also observed when
examining participants’ self-report. Before the train,
31,6% of them reported that they were stressed. After
the train, only 15,8% of them reported that they were
stressed.
The effect obtained in our first analysis lead to our
second research question which is: does this system
improve cognitive (attention) and memory functions?
To this end, we analyzed performance improvement
on the three attention exercises. On exercise 1, the
general mean improvement was negative by 6.58%.
On the second exercise, there was a mean
improvement of 0.48%. The performance
improvement on the third exercise was 7.02%.
More detailed results are shown in Figure 14.
When comparing performance for exercise 1 prior to
and after the virtual train, four participants showed
improvement, seven decreased performance and eight
participants kept the same performance. Only one
participant showed improvement on exercise 2, while
the others kept the same performance. Finally, on the
third exercise, 4 participants showed improvements
and the others kept the same level of performance.
Figure 14: Histogram of performance improvement in
exercise 1, 2 and 3.
We also analyzed the performance improvement
for the three memory exercises. For exercise four, a
10.53% mean improvement is observed. For the fifth
exercise, the mean improvement is 20% which is the
highest percentage of improvement. Finally, the mean
improvement is 10,53% for exercise six.
Individual results are shown in Figure 15, in
which we can see that for the fourth exercise, nine
participants had improvement, two participants had a
decrease of performance, and the rest kept the same
level of performance. For exercise 5, eleven
participants showed improved performance while one
kept the same level of performance and the eight had
a decrease of performance. Finally, five participants
improved on the last exercise, while four of them had
a decrease of performance and the rest kept the same
level of performance. We note that it is in this
exercise that a participant showed the highest
improvement performance with participant 1
showing a 100% improvement. Finally, participant 6
was unable to perform the exercise before the train
and succeeded after the train.
Figure 15: Histogram of performance improvement in
exercise 4, 5 and 6.
Finally, we compared improvement in cognitive
exercises versus memory exercises. To this end, we
grouped the exercises into two groups, and we
calculated by averaging the mean performance
improvement for exercises 1, 2 and 3
(cognitive/attention) and 4, 5 and 6 (memory). Figure
16 shows a clear difference between the improvement
of performance on the cognitive exercises versus the
memory exercises.
SENSORNETS 2020 - 9th International Conference on Sensor Networks
58

Figure 16: Histogram of performance improvement
cognitive vs memory exercises.
These results show a clear increase in memory
performance following the virtual train and in some
cases an improvement in attention abilities. Negative
emotions like frustration, are reduced. A post-
experience evaluation questionnaire confirmed that
the virtual train is relaxing and reduces stress (73,7%
participant confirmed that the virtual train is very
relaxing). The questionnaire confirmed the
participants’ interest for this method, and their
appreciation of virtual reality and its immersion
effect. In fact, 89,5% of them confirmed the good
aspect of immersion and 79% confirmed also that VR
has a positive impact on their experience.
6 CONCLUSION
In this paper, we presented a novel approach which
could be used to improve AD patients’ memory
performance using a virtual train. Experiments were
conducted during which the participants performed
cognitive and memory exercises, then travelled in the
virtual train in order to relax them, and then
performed the memory and cognitive exercises again.
Results showed that the virtual train helps relax the
participants and decreases negative emotions, most
notably frustration. In addition, results showed that
the participants’ performance in the attention
exercises did not improve or improved very mildly.
On the other hand, the participants’ performance on
the memory exercises was improved.
The first hypothesis (reducing the negative
emotions) was clearly reached. The second
hypothesis was partly accomplished. We can improve
the memory performance of the participants by using
the immersive virtual train which is a consequence of
reducing the negative emotions.
These results indicate that the virtual train can
reduce negative emotions and that this might have a
positive impact on the memory performance of older
adults.
ACKNOWLEDGEMENTS
We acknowledge NSERC-CRD, and Beam Me Up
for funding this work.
Sylvie Belleville holds a Canada Research Chair
on Cognitive Neuroscience of Aging and Brain
Plasticity.
REFERENCES
Alvarez, R. P., Johnson, L., & Grillon, C. (2007).
Contextual-specificity of short-delay extinction in
humans: Renewal of fear-potentiated startle in a virtual
environment. Learning & Memory, 14(4), 247–253.
Appel, L. (2017). How Virtual Reality could Change
Alzheimer Care. Technologie. Retrieved from
https://fr.slideshare.net/TechnoMontreal/how-virtual-
reality-could-change-alzheimer-care
Aspinall, P., Mavros, P., Coyne, R., & Roe, J. (2015). The
urban brain: Analysing outdoor physical activity with
mobile EEG. British Journal of Sports Medicine, 49(4),
272–276.
Association, A. (2015). 2015 Alzheimer’s disease facts and
figures. Alzheimer’s & Dementia, 11(3), 332–384.
Ben Abdessalem, H., Chaouachi, M., & Frasson, C. (2019).
Toward Real-Time System Adaptation Using
Excitement Detection from Eye Tracking. 15th
International Conference on Intelligent Tutoring
Systems, 214–223.
Ben Khedher, A., Jraidi, I., & Frasson, C. (2018). What Can
Eye Movement Patterns Reveal About Learners’
Performance? 14th International Conference on
Intelligent Tutoring Systems, 415–417.
Ben Khedher, A., Jraidi, I., & Frasson, C. (2019, January
18). Tracking Students’ Mental Engagement Using
EEG Signals during an Interaction with a Virtual
Learning Environment. Journal of Intelligent Learning
Systems and Applications, pp. 720–726.
Berka, C., Levendowski, D. J., Lumicao, M. N., Yau, A.,
Davis, G., Zivkovic, V. T., … Craven, P. L. (2007).
EEG correlates of task engagement and mental
workload in vigilance, learning, and memory tasks.
Aviation, Space, and Environmental Medicine, 78(5
Suppl), B231-244.
Biamonti, A., Gramegna, S., & Imamogullari-Leblanc, B.
(2014). A Design Experience for the Enhancement of
the Quality of Life for People with Alzheimer’s
Disease. What’s On: Cumulus Spring Conference.
Biocca, F. (2006). The Cyborg’s Dilemma: Progressive
Embodiment in Virtual Environments [1]. Journal of
Computer-Mediated Communication, 3(2), 0–0.
Cherniack, E. P. (2011). Not just fun and games:
Applications of virtual reality in the identification and
Application of Virtual Travel for Alzheimer’s Disease
59

rehabilitation of cognitive disorders of the elderly.
Disability and Rehabilitation: Assistive Technology,
6(4), 283–289.
Cirrito, J. R., Yamada, K. A., Finn, M. B., Sloviter, R. S.,
Bales, K. R., May, P. C., … Holtzman, D. M. (2005).
Synaptic Activity Regulates Interstitial Fluid Amyloid-
β Levels In Vivo. Neuron, 48(6), 913–922.
Coyle, H., Traynor, V., & Solowij, N. (2015).
Computerized and Virtual Reality Cognitive Training
for Individuals at High Risk of Cognitive Decline:
Systematic Review of the Literature. The American
Journal of Geriatric Psychiatry, 23(4), 335–359.
Dubois, B., Feldman, H. H., Jacova, C., DeKosky, S. T.,
Barberger-Gateau, P., Cummings, J., … Scheltens, P.
(2007). Research criteria for the diagnosis of
Alzheimer’s disease: Revising the NINCDS–ADRDA
criteria. The Lancet Neurology, 6(8), 734–746.
Gorini, A., & Riva, G. (2008). Virtual reality in anxiety
disorders: The past and the future. Expert Review of
Neurotherapeutics, 8(2), 215–233.
Hill, N. T. M., Mowszowski, L., Naismith, S. L., Chadwick,
V. L., Valenzuela, M., & Lampit, A. (2016).
Computerized Cognitive Training in Older Adults With
Mild Cognitive Impairment or Dementia: A Systematic
Review and Meta-Analysis. American Journal of
Psychiatry, 174(4), 329–340.
Kennedy, R. S., Lane, N. E., Berbaum, K. S., & Lilienthal,
M. G. (1993). Simulator Sickness Questionnaire: An
Enhanced Method for Quantifying Simulator Sickness.
The International Journal of Aviation Psychology, 3(3),
203–220.
Laforte, M. (2018). Zoothérapie: Tout savoir sur la thérapie
assistée par les animaux. Retrieved October 23, 2019,
from Canal Vie website:
http://www.canalvie.com/famille/animaux/zootherapie
-1.1767466
Lallemand, C., Koenig, V., Gronier, G., & Martin, R.
(2015). Création et validation d’une version française
du questionnaire AttrakDiff pour l’évaluation de
l’expérience utilisateur des systèmes interactifs. Revue
Européenne de Psychologie Appliquée/European
Review of Applied Psychology, 65(5), 239–252.
Lawton, M. P., Van Haitsma, K., & Klapper, J. (1996).
Observed Affect in Nursing Home Residents with
Alzheimer’s Disease. The Journals of Gerontology
Series B: Psychological Sciences and Social Sciences,
51B(1), P3–P14.
Manera, V., Chapoulie, E., Bourgeois, J., Guerchouche, R.,
David, R., Ondrej, J., … Robert, P. (2016). A
Feasibility Study with Image-Based Rendered Virtual
Reality in Patients with Mild Cognitive Impairment and
Dementia. PLOS ONE, 11(3), e0151487.
Maynard, O. M., Munafò, M. R., & Leonards, U. (2013).
Visual attention to health warnings on plain tobacco
packaging in adolescent smokers and non-smokers.
Addiction (Abingdon, England), 108(2), 413–419.
Pedraza-Hueso, M., Martín-Calzón, S., Díaz-Pernas, F. J.,
& Martínez-Zarzuela, M. (2015). Rehabilitation Using
Kinect-based Games and Virtual Reality. Procedia
Computer Science, 75, 161–168.
Pini, L., Pievani, M., Bocchetta, M., Altomare, D., Bosco,
P., Cavedo, E., … Frisoni, G. B. (2016). Brain atrophy
in Alzheimer’s Disease and aging. Ageing Research
Reviews, 30, 25–48.
Robert, P., Lanctôt, K. L., Agüera-Ortiz, L., Aalten, P.,
Bremond, F., Defrancesco, M., … Manera, V. (2018).
Is it time to revise the diagnostic criteria for apathy in
brain disorders? The 2018 international consensus
group. European Psychiatry, 54, 71–76.
Rose, F. D., Brooks, Barbara. M., & Rizzo, A. A. (2005).
Virtual Reality in Brain Damage Rehabilitation:
Review. CyberPsychology & Behavior, 8(3), 241–262.
Todd, R. M., & Anderson, A. K. (2009). The neurogenetics
of remembering emotions past. Proceedings of the
National Academy of Sciences, 106(45), 18881–18882.
van Dalen, J. W., van Wanrooij, L. L., Moll van Charante,
E. P., Brayne, C., van Gool, W. A., & Richard, E.
(2018). Association of Apathy With Risk of Incident
Dementia: A Systematic Review and Meta-analysis.
JAMA Psychiatry, 75(10), 1012.
Vindenes, J., de Gortari, A. O., & Wasson, B. (2018).
Mnemosyne: Adapting the Method of Loci to
Immersive Virtual Reality. In L. T. De Paolis & P.
Bourdot (Eds.), Augmented Reality, Virtual Reality,
and Computer Graphics (Vol. 10850, pp. 205–213).
Watson, D., Clark, L. A., & Tellegen, A. (1988).
Development and validation of brief measures of
positive and negative affect: The PANAS scales.
Journal of Personality and Social Psychology, 54(6),
1063–1070.
Zhu, C. W., Grossman, H. T., & Sano, M. (2019). Why Do
They Just Sit? Apathy as a Core Symptom of Alzheimer
Disease. The American Journal of Geriatric Psychiatry,
27(4), 395–405.
Zucchella, C., Bartolo, M., Bernini, S., Picascia, M., &
Sinforiani, E. (2015). Quality of Life in Alzheimer
Disease: A Comparison of Patients’ and Caregivers’
Points of View. Alzheimer Disease & Associated
Disorders, 29(1), 50–54.
SENSORNETS 2020 - 9th International Conference on Sensor Networks
60
