
IT-structures and Algorithms for Quality Assurance in the Health
Insurance Medical Advisory Service Institutions in Germany
Vera Ries
1
, Klaus-Peter Thiele
2
, Martin Schuster
3
and Reinhard Schuster
4
1
Project Coordinator and Assistant to the Medical Director of the Medical Advisory Service
Institution of the Statutory Health Insurance in North Rhine (MDK Nordrhein), 40212 D
¨
usseldorf, Germany
2
Medical Director of the Medical Advisory Service Institution of the Statutory Health Insurance in North Rhine
(MDK Nordrhein), 40212 D
¨
usseldorf, Germany
3
Faculty of Epidemiology, Christian-Albrechts University Kiel, 24105 Kiel, Germany
4
Chair of Department of Health Economics, Epidemiology and Medical Informatics,
Medical Advisory Service Institution of the Statutory Health Insurance in Northern Germany (MDK Nord),
23554 L
¨
ubeck, Germany
Keywords:
Quality Assurance, Statutory Health Insurance, Medical Advisory Service Institution, Communication
Structures between Different IT-systems, Server Data Structures, Data Protection, Script Programming, Client
Office Answers using Perl Modules, Integer Linear Programming.
Abstract:
The 15 Regional Medical Advisory Service Institutions of the Statutory Health Insurance in Germany (MDK)
create medical expertises (sozialmedizinische Gutachten) on behalf of the Statutory Health Insurance Funds
in the fields of inpatient and outpatient treatment, incapacity of work and other fields. The process of internal
quality assurance within the local advisory service institutions as well as between them plays an increasing
role and got new impulses by actual national legislation. The assessment process was established in 2004 and
covers only one single indication: long-term care. It consists in a paper-based procedure focusing on a manual
distribution process performed by staff of the central quality assurance bureau. We will present organizational
concepts of the new standardized regional and nationwide peer review process that will cover the multitude
of all existing indications of health care. It is completely digitalized using mathematical IT-based procedures
not only for randomized sampling, but as well to achieve an equal distribution of the medical expertises to be
assessed by the peer Medical Advisory Service Institutions. These peer reviews are supposed to be distributed
among the institutions depending on occasion groups and further subtypes of medical expertises, posing a
constraint satisfaction problem that needs to be solved. Therefore we discuss models that address this kind
of problem type and present possible solutions for the concrete distribution problem mentioned above. We
further present our technical framework that will support the workflow needed for peer review distribution,
data collection and final result analysis. The 15 regional medical service institutions with different IT-system
have to be connected, while data protection concerns have to be taken into account. Finally, the statistical
distribution of the review results is analyzed.
1 INTRODUCTION
In Germany, 15 Regional Medical Advisory Ser-
vice Institutions are mandated by the German So-
cial Code to assist the Statutory Health Insurance
(Krankenversicherung) as well as the Statutory Long-
term Care Insurance (Pflegeversicherung). Overall,
nearly 10.000 employees are working within the Med-
ical Advisory Service Institutions, providing medical
knowledge by case management consultancy and by
medical expertise recommendation services in several
fields of long-term care and of healthcare.
1.1 Preexisting Quality Assurance Plan
For long-term care there was a preexisting qual-
ity assurance plan for medical expertises. About
3.500 specialized nurses are employed by the Medi-
cal Advisory Service Institutions in those both assess-
ment fields about long-term care. A national qual-
ity assurance plan was mandated by law since 2004
(Schmacke, 2016). It consists of the exchange of
paper printed medical expertises that are distributed
manually by staff of the central quality assurance bu-
reau. For two years now, the assessment forms are no
Ries, V., Thiele, K., Schuster, M. and Schuster, R.
IT-structures and Algorithms for Quality Assurance in the Health Insurance Medical Advisory Service Institutions in Germany.
DOI: 10.5220/0008912303530360
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 353-360
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
353

longer paper-based assessment sheets but can be filled
out using a web-based data platform as well.
1.2 Starting a New Quality Assurance
Plan in 2020
In 2020 a new quality assurance plan for medical ex-
pertises covering the multitude of all health care ser-
vice fields provided by the Statutory Health Insurance
Funds in 2020 will be started. For health care, the top-
ics covered by the Medical Advisory Service Institu-
tions’ consultancy and expertise services are diverse.
About 2.500 specialized physicians, 90 other health
care professionals and 400 medical coders are work-
ing in the health care division of the Medical Advi-
sory Service Institutions. The main tops are
• hospital quality and billing control on behalf of
the health care insurance funds (Thiele K.-P.,
2018),
• out-patient case management consultancy and
medical expert opinion service (N
¨
uchtern, 2008)
in multiple fields of medical treatment.
• To learn more about the German social system of
health care in detail, see (Altenstetter and Busse,
2005), (Cortina, 1993), (Machnik, 2009), (Saw-
icki and Bastian, 2008).
So, there are many different health care topics cov-
ered by the Medical Advisory Service Institutions’
consultancy and medical expertises. For a long time,
however, there was no monolithic quality assurance
plan established for the health care segment of con-
sultancy and medical expertises. The Regional Med-
ical Service Institutions performed a kaleidoscope of
singular quality assurance measures lacking a nation-
wide perspective and any public reporting, instead. In
2017, a nationwide task force was established by the
medical directors’ conference of all regional Medical
Advisory Service Institutions to design, to initiate and
to implement a total quality assurance plan.
The preexisting regional quality assurance initia-
tives were used as a draft to establish a unified contin-
uous quality circle (Deming, 1982), (Shewhart, 1931)
suitable to the diversity of medical topics, perform-
ing annual quality measurements and validations. The
total quality assurance organizational framework es-
tablished addresses both, the internal quality assur-
ance of every Regional Medical Advisory Service In-
stitution as well as a nationwide quality assurance.
The quality assurance method is based on peer re-
views, a common method in statutory social insur-
ance frameworks in Germany (DRV, 2018), (Polak,
2018), (Strahl et al., 2016), (Strahl et al., 2018). By
facilitating mutual learning, thereby enhancing con-
tinuous quality improvement, both regionally and na-
tionwide. Crucial to this nationwide initiative was a
commitment by all Regional Medical Advisory Ser-
vice Institutions of a joint and uniform conception of
quality. A prime nationwide reporting of the qual-
ity assurance results of all Medical Advisory Service
Institutions starting in 2020 will contribute to a high
degree of transparency between each other and fosters
mutual learning. What is more, it inspires reliability
and trustworthiness towards their clients, the Statu-
tory Health Insurance Funds, and towards society.
All nationally and internationally available infor-
mation on quality assurance in general and especially
in health systems and health and pension insurance
have been adapted to the newly established system
with the conceptional time ending 2019 and the role
out starting in 2020.
2 MATERIAL AND METHODS,
PROCESS ORGANIZATION
The Medical Advisory Service Institutions yearly
produce about 2.5 million medical expertises about
inpatient hospital treatments and documentations for
on behalf of the statutory health insurance funds. A
random sample of 0.5% will be used for regional qual-
ity assurance using peer reviews. 10 % of those med-
ical expertises randomly chosen get a second exter-
nal peer review by another advisory service institu-
tion generating the nationwide perspective. Thereby
we get 12,500 peer reviews for regional quality assur-
ance and 1,250 nationwide peer reviews.
Additionally there are about 650 thousand medi-
cal expertises in other fields classifies in eight occa-
sion groups (inability of work, outpatient care, new
and unconventional treatment methods and drug treat-
ment, prevention and rehabilitation, remedies, den-
tistry, factual or putative medical treatment, claims
against third, other) with further subgroups. In anal-
ogy to industrial quality standards for production,
quality is defined as a measure that describes the de-
gree of correspondence between the service provided
by an deliverer and the service expected by the cus-
tomer (Masaaki, 1986), (Gerlach, 2001), (Kamiske
and Brauer, 2011), (Institute of Medicine; Commit-
tee to Design a Strategy for Quality Review and As-
surance in Medicare, 1990), (Institute of Medicine,
2001), (Internationale Organisation f
¨
ur Normung,
2015). The concept of nationwide and regional qual-
ity assessment is worked out and will be further
developed by the permanent commission of senior
physicians and quality managers. The questionnaire
HEALTHINF 2020 - 13th International Conference on Health Informatics
354
was developed by a task force based on an informa-
tion retrieval about preexisting regional quality assur-
ance concepts for the common set of quality crite-
ria followed by a modified Delphi method to shape
the different sets of indication-specific quality criteria
(Normand et al., 1998). Decisions are made by the
conference of medical directors conference (Leitende
¨
Arzte) and the conference of the managing directors
(Gesch
¨
aftsf
¨
uhrer).
In Germany the regions differ considerably in size
and population density. So, questions of equity are a
strong point in any discussion. Therefore the reviews
start with a minimal size setting feasible for any par-
ticipant.
The peer review process is organized quarterly. If
at least one medical expertise is transferred to every
other local advisory service institution, 14 expertises
have to be included per quarter or 56 per year. If we
demand, that at least the double size have to be in-
cluded for local quality assurance, we come to ask
for 112 expertises in each field. This leads to 11,660
medical expertises in total on the regional level and
5,300 medical expertises on the nationwide level in
peer review evaluations for all smaller occasion fields.
This number of medical expertises leads to a personal
and financial effort which should not be exceeded.
For reasons of practicability, we reduce the number
of medical expertises given to an external review pro-
cess for the smaller five medical service institutions
to a half (7 instead of 14 medical expertises for the 15
existing regional medical service institutions).
The internal number of peer reviews for hospital
expertises nearly equals the total number of all other
occasion groups, thereby is no need to enlarge the
number of hospital peer reviews.
The peer reviews for medical expertises are based
on pdf files and related meta data. Additional med-
ical treatment information is not used by reasons of
practicability (for instance large hospital treatment
records). The use of additional medical data in re-
gional quality assurance would create a bias towards
the nationwide quality assurance because the addi-
tional data like clinical case logs are unable to be
transfered for data protection and practicability rea-
sons. What is more, the medical expertises aims to be
perspicuous and understood without additional medi-
cal documentation data available.
Meta data contain the type (occasion) and date of
release of medical expertise, subregion of the local
advisory service institution and possibly additional
process parameters. Pdf files and meta data are re-
lated by a regional unique identity key.
With respect to m=9 occasion types (starting with
m=2) and further subtypes of medical expertises
the pear review process yields an n-dimensional (n
around 30 in different groups) quality vector with
components of k outcome types (actually used: ”cor-
rect”, ”improvement potential with no result rele-
vance”, ”incorrect” and ”not relevant”), cf. Figure
2. Only a minority of questions depend on the oc-
casion type. The questions for the peer reviews have
been tested with positive results in a reliability anal-
ysis which will be repeated periodically, cf. (B
¨
uhn
et al., 2017), (Wirtz and Caspar, 2002), (Eisinga et al.,
2012).
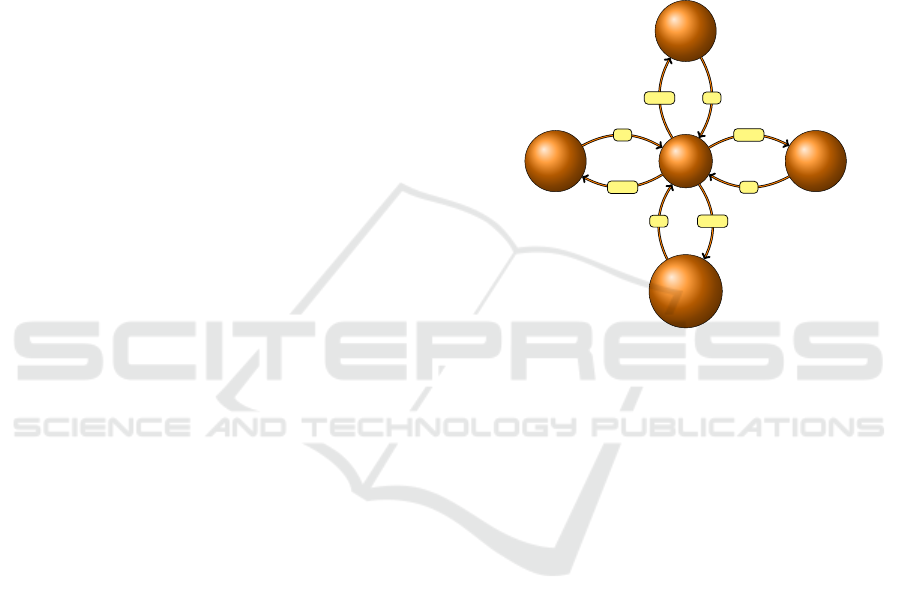
ServerMDK x MDK 1
MDK 2
consensus
down
up
down
up
down
up
down
up
Figure 1: Communication between Medical Advisory Ser-
vice Institutions (MDK) and the QA-server.
The central IT-system is a linux sever (Debian)
which is located in an external data center which
we will call QA-server (quality assurance). It uses
MySQL as database system, perl as the main script
language including the perl module writeexcel in or-
der to generate excel files to give overviews about
data and aggregate informations for medical review
service institutions. The communication uses a role
concept for administrative persons, medical experts,
peer reviewers and members of consensus confer-
ences. The server management uses the ssh protocol
with key pairs and a passphrase. The communication
between the server and the regional advisory service
institution use the https protocol. Every user needs
a personal password. All transfer actions are logged.
Data backups are made daily.
Every communication step is a pair of upload and
download exchange streams between advisory service
institutions with individual IT-structure and the QA-
server or between other participants as the consensus
conference and the server. It is a star topology with
the QA-server in the center, cf. Figure 1.
In order to start the quarterly local quality assur-
ance process, a matrix which contains all local medi-
cal expertise identities (pdf file names) with the men-
IT-structures and Algorithms for Quality Assurance in the Health Insurance Medical Advisory Service Institutions in Germany
355

tioned meta data concerning a period of a month or
quarter has to be uploaded. The respective download
answer gives the random sample for regional qual-
ity assurance. A second random sample for external
quality assurance is determined, but not transmitted to
the local advisory service institution. As a next step
the pdf files related to the sample have to be uploaded
to the QA-sever as single pdf files or as zipped files in
individual parts or totally. The server answer consists
in a first file structure analysis. The regional identity
is converted into an external unique file identity, the
transformation is stored in a MySQL table.
As a next step one or several peer review man-
agers distribute the medical expertise files e
i
with
meta data m(e
i
) to peer review experts r
j
as a func-
tion f : e
i
→ r
j
. This may be done using the detailed
occasion reasons or regional features due to local con-
figurations. It also can be done completely automatic.
The server provides a radio buttom formula and the
answer arranges the combination of review experts
and review documents.
In order to carry out the review, the review expert
first has to download the pdf file of the related medical
expertise. After that there is the possibility to use a
QA-server form online or to use a pdf form for offline
review. In both cases the server will give the result
of a formal answer check (all questions are answered
and for all incorrect points reasons are stated).
The result of the peer review is transfered to the
author of the medical expertise for feedback. The
medical expert gives notice if she/he agrees or dis-
agrees with the peer review. This happens primarily
anonymously. However, the medical expert may ask
for a personal contact to the peer reviewer. Further
quality management actions are up to regional advi-
sory service institution decisions.
Alternatively, the regional advisory service insti-
tution may carry out the regional peer review proce-
dure in his own IT structure. In this case, the service
institution quality manager has to upload the results
in csv or xls-format again with a related answer check
procedure.
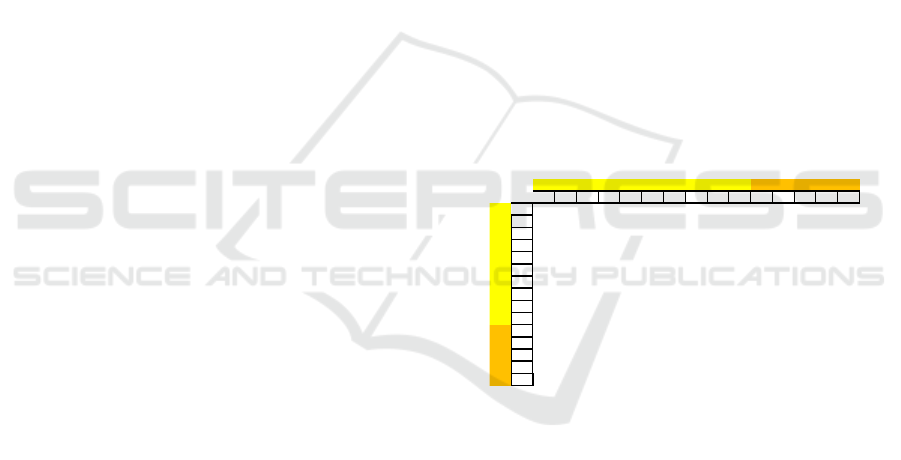
review
pdf
#01 #02 #03 #04 #05 #06 #07 #08 #09
1 3 3 1 1 3 3 2 2 3
2 1 1 1 1 2 1 1 1 1
3 1 1 1 1 3 1 3 1 1
4 1 1 1 1 3 3 3 1 1
5 1 1 1 1 1 1 1 1 2
6 1 1 3 2 3 3 3 1 1
7 1 1 1 2 3 1 3 2 1
8 1 1 1 1 2 3 2 3 1
9 1 2 3 1 3 2 2 2 1
10 1 1 1 1 3 3 3 1 1
11 1 1 1 1 3 1 1 1 1
12 1 1 2 2 2 1 3 1 1
review question
Figure 2: Upload regional review results with meaning
green: correct, yellow: improvement potential with no re-
sult relevance, red: incorrect.
Using the upload, a random sample is chosen for
the nationwide peer review. The related identities are
given as the server answer in order to select the related
pdf file for an upload. All identities are transformed
to QA-server identities. One regional extension of the
quality assurance is consisting in the demand, that ev-
ery physician who is included in the creation of med-
ical expertises shall be included in the peer review
process at least two times a year in each relevant oc-
casion group. If this is not reached by the random
process, additional expertises have to be included in
the regional peer review process. If this enlargement
is done in the last quarter, the number of added ex-
pertises remain as low as possible, but it results in an
unequal workload. The expertises of the enlargement
shall not be included in the random selection for exter-
nal peer reviews, because of the fact that it would in-
crease the possibility of physicians with a small num-
ber of expertises to be in the external peer review pro-
cess.
The distribution of the regional medical expertises
to external medical service institutions shall satisfy
the following conditions:
• Every advisory service institution shall do as
much peer reviews as it has given medical exper-
tises to the nationwide quality assurance using the
case numbers stated above
• Every other advisory service institution shall be
included in order to get large range of opinions
• Boards with more medical expertises shall get
more peer reviews (with possibly ”smaller” vio-
lations of this rule)
• The service institutions with the largest number of
medical expertises shall get as few peer reviews as
possible in order to avoid concentration of special
opinions in one spot
We will discuss the ILP based method to solve this
problem later on. Only for the hospital treatment the
distribution differs essentially from an equal distribu-
tion.
Before the medical expertises are forwarded to a
the external peer reviewers is realized, a further ran-
dom process is performed. The distribution of the
medical expertises to the peer reviewers is done by
an analogous procedure described for internal peer re-
viewers. Every peer reviewer may propose medical
expertises for a discussion in the consensus confer-
ence. For each occasion group there shall be two con-
sensus conferences each year. The external peer re-
viewer does not know the results of the internal peer
review. If the regional valuation differs from the na-
tionwide valuation, the internal reviewer is asked, if
he accepts the result of the external peer review. If the
HEALTHINF 2020 - 13th International Conference on Health Informatics
356

difference persists, the expertise has to be discussed
in the consensus conference. In order to organize this
comparison, every internal peer reviewer has to con-
sider differing results to his own peer review results
after peer reviews are completed. The comparison is
generated automatically by the QA-server.
Every participant of the consensus conference will
be provided with detailed information about all ex-
pertises proposed to the consensus conference of the
respective occasion group. Every advisory service
institution sends out a member into this conference.
The conference members only get labels of the peer
reviews done by members of there home advisory
service institution in order to remain information as
anonymous as possible at the one hand and to get
additional information about reasons of review deci-
sions as deep as possible at the other hand. If the con-
sensus conference does not reach an agreement with
respect to a special expertise, the simple majority will
decide about the final result. The responsible manager
of the consensus conference has to upload the final de-
cisions to the QA-server, this can be done during the
conference.
The amount of uploaded data in relation to the
stated case numbers and the fraction of realized peer
reviews may be requested by the quality managers
with the related roles (regional or nationwide level).
Additionally frequency results of all parts of the re-
view process can be downloaded at every time. The
results are given as files in xls or xlsx format with
choosable evaluation contents. Every advisory ser-
vice institution can download all details about the ex-
pertises of his home service institution including the
external peer review results, but there are no labels
which external service institution gave the nationwide
evaluation. The overall amount of analysis is done via
background processing.
Aggregated results of the regional and the nation-
wide peer review process will be published. In or-
der to get information about the security of the results
confidence levels are calculated. Tables and figures of
the results in the decided amount are produced by the
QA-server.
3 RESULTS, MATHEMATICAL
MODELS
A first pretest in the field of incapacity of work and
a second pretest outpatient care with the subgroups
DRG (diagnoses related groups) and PEPP (pay
groups in psychiatry and psychosomatic medicine)
has been used to reduce the variance and to increase
the kappa values between the reviewers with respect
to the questions and with respect to the medical opin-
ions. After improvement and clarifying of the ques-
tionnaire we got an intraclass correlation coefficients
(average measures) of 0.923, 0.903 and 0.868 in the
mentioned fields and thereby a good reliability was
reached, cf. (Cortina, 1993), (Eisinga et al., 2012),
(Wirtz and Caspar, 2002). Let w(i, k) be the result
with value 1 (resp. 2 and 3) for correct (resp. im-
provement potential with no result relevance and in-
correct) medical opinions of the expert from the eval-
uation of the reviewer for medical opinion i and ques-
tion k. Then
d(x, y) =
∑
i
|w(i, x) − w(i, y)|
is the Manhattan distance of the opinion vector with
respect to the questions x and y. For each question
we look for the other questions with the smallest two
distances. We use the questions as the vertices of a
graph and the edges we get by the shortest distances.
Using the modularity method we get graph communi-
ties. For the calculations we have used Mathematica
by Wolfram Research. An example for the pretest is
shown in Figure 3. The results after a year of qual-
ity assurance will give further hints for improvement
of questions and further training opportunities for the
medical experts.
1
8
5
2
4
3
9
7
12
6
15
13
14
10
11
Figure 3: Graph Communities of questions Selection.
Let n(i, j) be the number of medical expertises
which are transfered from medical service institution
i the medical expert to the medical service institution
j of the reviewer and w(i) the number of expertises
from service institutions i given in the external review
process. The order of medical service institutions are
chosen such that w(i) ≥ w( j) for i > j. No expertise
remains in the same medical service institutions, so
the the matrix n(i, j) has an empty diagonal. If one
would use the proportional approach
n(i, j) = int(w(i)
w( j)
∑
k6= j
w(k)
)
IT-structures and Algorithms for Quality Assurance in the Health Insurance Medical Advisory Service Institutions in Germany
357
one would not get a balance between ingoing and out-
going expertises (rounding problems are only a minor
effect). One could implement a random process with
certain rules, but it would result in under- and over-
representation of certain medical service institutions
in most quarters.
We will look for solutions of equations and in-
equalities with integer solutions with a certain optimal
solution. As a balance demand and the demand the no
expertise stay in the same medical service institutions
we state
∑
j
n(i, j) = w(i)
∑
i
n(i, j) = w( j)
∑
i
n(i, i) = 0.
If we require the symmetry of the matrix n(i, j) it will
reduce the number of variables which may reduce the
machine time, but it may lead to insolvability of the
problem. Let m(i, j) the matrix we get from n(i, j
by deleting the main diagonal (delete in columns).
We could demand monotony in the columns and rows
without the main diagonal:
m(i, j) ≥ m(k, j) for i > j
m(i, j) ≥ m(i, k) for i > j
Already with w(l) < l (l number of medical service
institutions) the problem is unsolvable. So we will
take a weaker demand:
m(i, j) + d ≥ m(k, j) for i > j
m(i, j) + d ≥ m(i, k) for i > j
with d as small as possible for solvability.
The reviews should concentrate as little as possi-
ble to large service institutions and be as uniformly as
possible between the medical service institutions. To-
gether with the weak monotony demand we will use
n(1, 2) + n(2, 1) −→ Min!
as an optimization condition.
In the case w(i) = 14 for 1 ≤ i ≤ 10 (large medi-
cal service institutions) and w(i) = 7 for 11 ≤ i ≤ 15
(small medical service institutions) as an example for
two equal groups which will be applied for all occa-
sion groups except of hospital care a balance between
and within the groups can be reached by additional
constraints as
15
∑
i=11
n(i, j) = 2 for j = 11, ..., 15
15
∑
j=11
n(i, j) = 2 for i = 11, ...,15.
Thereby we have got an integer linear program (ILP).
This can by solved (if there is a solution at all) e.g. a
Python program and using CPLEX bindings. We also
could first solve a linear program without the restric-
tion to integers and then do a post processing step to
obtain integer solutions by local changes. This can
be done with Mathematica by Wolfram Research or
also using Python and CPLEX, cf. (Shinano et al.,
2003). For finding a suitable distribution matrix for
distributing the reviews over the medical advisory we
use an integer linear programming approach. Inte-
ger linear programs (ILP) allow to formulate an op-
timization problem with an linear objective function
and constraints given as a series of linear inequalities.
Then, an integer valued assignment of the variables
is wanted that fulfills all constrains. Although solv-
ing ILP problems is computationally hard (NP-hard
to be more specific), there are powerful ILP solvers
available that perform well on our concrete problem
formulations, see (Newman, 2006).
A solution with the smallest value d = 1 is shown
in Figure 4. In each quarter one should apply a ran-
dom permutation within the two groups and/or use an
other solution of the ILP system. One solution of the
ILP is shown in Figure 5.
BY NR BW HE WL NI NO RP BB SN ST TH MV SL HB sum
BY 1 2 1 1 1 2 1 1 2 1 1 14
NR 1 2 2 1 1 1 1 1 2 1 1 14
BW 1 2 2 1 1 1 1 1 1 1 1 1 14
HE 1 2 1 2 1 1 2 1 1 1 1 14
WL 1 1 1 2 2 1 1 1 1 1 1 1 14
NI 1 1 1 1 2 2 1 1 1 1 1 1 14
NO 2 1 1 1 1 2 1 1 1 1 1 1 14
RP 2 2 1 1 1 1 1 2 1 1 1 14
BB 1 1 1 1 1 1 1 2 2 1 1 1 14
SN 2 1 1 1 1 1 1 2 2 1 1 14
ST 1 1 1 1 1 1 1 7
TH 1 1 1 1 1 1 1 7
MV 1 1 1 1 1 1 1 7
SL 1 1 1 1 1 1 1 7
HB 1 1 1 1 1 1 1 7
sum 14 14 14 14 14 14 14 14 14 14 7 7 7 7 7
quarterly permutation
quarterly permutation
Figure 4: Distribution matrix of medical expertises to exter-
nal peer reviews for occasion group ”incapacity of work” of
medical service institutions.
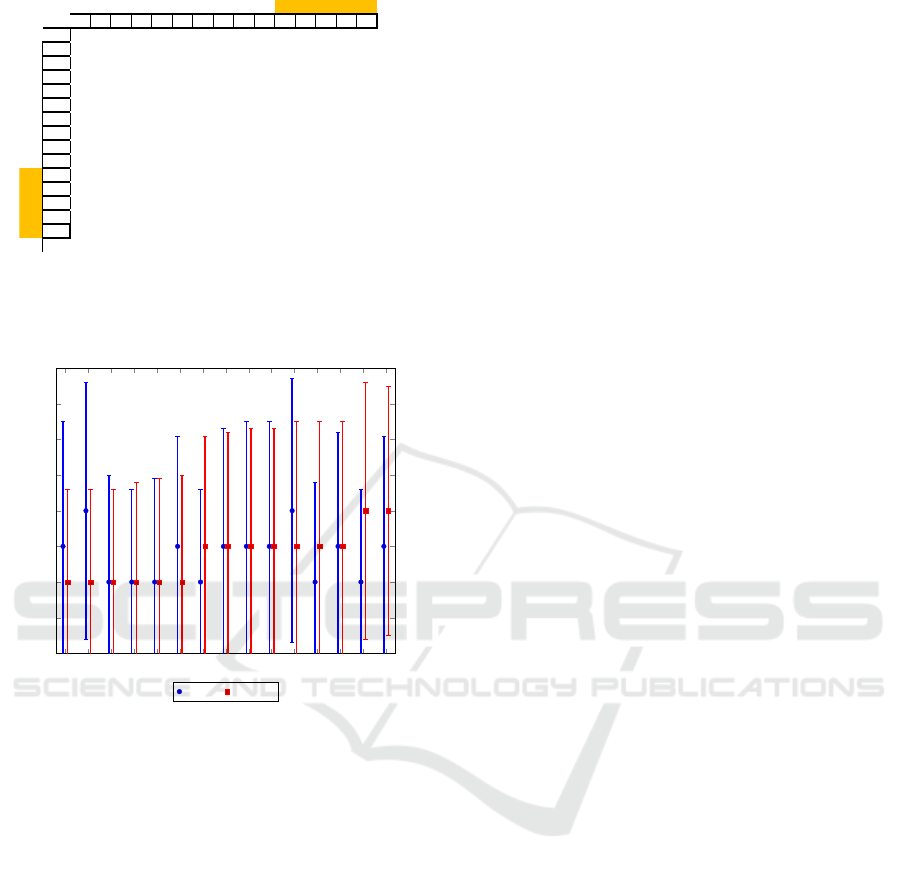
The result of the review (i.e. probability of im-
provement potential) may be considered as binomial
distribution and one can calculate confidence inter-
vals for yearly reports. Such confidence intervals are
much more suitable values which contain much noise.
The review results may depend on further parameters
which can be used to optimize the quality assurance
process. An example of the comparison of the re-
sults of the considered medical service institutions is
shown in Figure 6, real results can be given after for
quarters of quality assurance, which will be started in
2020.
HEALTHINF 2020 - 13th International Conference on Health Informatics
358
BY NR BW HE WL NI NO RP BB SN ST TH MV SL HB sum
BY 7 6 5 6 5 5 5 5 5 1 1 51
NR 6 6 6 4 5 5 1 1 2 1 1 1 39
BW 6 6 6 5 4 2 2 1 2 1 1 1 37
HE 5 5 6 4 2 1 1 2 1 1 1 29
WL 6 4 5 3 3 1 1 1 1 1 1 1 28
NI 6 4 3 2 2 2 1 1 1 1 1 1 25
NO 5 5 3 1 1 1 2 1 1 1 1 1 23
RP 5 2 2 1 1 1 2 2 1 1 18
BB 5 1 1 1 1 1 1 2 1 1 1 1 17
SN 5 2 2 1 1 1 1 1 1 1 1 17
ST 1 1 1 1 1 1 1 7
TH 1 1 1 1 1 1 1 7
MV 1 1 1 1 1 1 1 7
SL 1 1 1 1 1 1 1 7
HB 1 1 1 1 1 1 1 7
sum 51 39 37 29 28 25 23 18 17 17 7 7 7 7 7
quarterly permutation
Figure 5: Distribution matrix of medical expertises to ex-
ternal peer reviews for for occasion group ”hospital care”
among medical service institutions.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
0
1
2
3
4
5
6
7
8
medical board
number of mistakes
Mistake in question 16 (hospital care)
internal external
Figure 6: Results and confidence intervals for external and
nationwide failure medical expertises.
4 CONCLUSIONS
The quality assurance process in the sense of the con-
sidered PDCA cycle will be especially successful if
acceptance, practicability and transparency support
each other. In each Medical Advisory Service Insti-
tution has to reach each medical expert in order to
reach a continuous development of a common un-
derstanding ans progression of quality. The exter-
nal peer reviews shall reach a common understanding
of quality in each region with a transparent presen-
tation of the results to the public. In Germany there
is a considerable heterogeneity in size and number of
employees among the medical service institutions in-
volved. Questions of equity are a constant concern.
The discussed methods provide the necessary frame-
work that enables all medical advisory service insti-
tutions to take part and to shape trustful cooperation
among each other.
The distribution of the regional expertises to na-
tionwide reviews are subject to distributional fairness.
All regions have to be appropriately included on the
one hand and larger resources of larger services on the
other hand must be taken into account. There shall
be no avoidable regional concentrations of peer re-
views as well as no no overemphasis on certain cou-
pling patterns. It is realized as a solution of an integer
linear program which shall not only change slightly
from quarter to quarter. An important point is the
reliability and validity of the valuation results. It is
essential to communicate confidence intervals for the
results instead of single values so that the public is
in a position to distinguish between random and se-
cured differences. In the practical implementation the
interaction of different IT systems used by the medi-
cal experts in terms of good manageability and great
security is a big challenge.
The implementation uses a Linux based MySQL
server which is reached by the regional medical ad-
visory institutions as well as for coordinating work-
ing groups by the https protocol. In the working pro-
cess are used predominantly perl scripts. Overviews
are generated on the server as excel tables. There are
flexible regional design options through configuration
tables. The described concept should enable a fast
nationwide development of a common understanding
and improvement of quality. Quality conferences in
each occasion group twice a year will discuss dif-
ferent views and will lead to a final decision process
which has to be communicated in each region by the
quality managers.
REFERENCES
Altenstetter, C. and Busse, R. (2005). Health Care Reform
in Germany: Patchwork Change Within Established
Governance Structures. Journal of Health Politics,
Policy and Law, 30(1-2):121–42.
B
¨
uhn, S., Mathes, T., Prengel, P., Wegewitz, U., Ostermann,
T., Robens, S., and Pieper, D. (2017). The risk of bias
in systematic reviews (ROBIS) tool showed fair relia-
bility and good construct validity to assess the risk of
bias in systematic reviews. Journal of Clinical Epi-
demiology, pages 121–128.
Cortina, J. (1993). What Is Coefficient Alpha? An Exami-
nation of Theory and Applications. Journal of Applied
Psychology, 78 (1):98–104.
Deming, W. E. (1982). Out of the crisis. Cambridge: Mas-
sachusetts Institute of Technology.
DRV (2018). Qualit
¨
atssicherung der sozialmedizinis-
chen Begutachtung. Manual zum Peer Review-
Verfahren. Berlin: Deutsche Rentenversicherung
Bund.
¨
Uberarbeitete Fassung August 2018.
IT-structures and Algorithms for Quality Assurance in the Health Insurance Medical Advisory Service Institutions in Germany
359

Eisinga, R., Grotenhuis, M., and Pelzer, B. (2012). The
reliability of a two-item scale: Pearson, Cronbach or
Spearman-Brown? International Journal of Public
Health, 58 (4):637–642.
Gerlach, F. M. (2001). Qualit
¨
atsf
¨
orderung in Praxis und
Klinik: eine Chance f
¨
ur die Medizin. Stuttgart:
Thieme.
Institute of Medicine (2001). Crossing the Quality Chasm:
A New Health System for the 21st Century. Washing-
ton, DC, National Academy Press.
Institute of Medicine; Committee to Design a Strategy for
Quality Review and Assurance in Medicare (1990).
Medicare: A Strategy for Quality Assurance. Volume
II: Sources and Methods., volume 2. Washington
(DC): National Academies Press (US).
Internationale Organisation f
¨
ur Normung (2015). DIN
EN ISO 9001:2015-11. Qualit
¨
atsmanagementsysteme
- Anforderungen. Beuth Verlag.
Kamiske, G. F. and Brauer, J.-P. (2011).
Qualit
¨
atsmanagement von A bis Z: Wichtige Be-
griffe des Qualit
¨
atsmanagements und ihre Bedeutung.
Carl Hanser Verlag.
Machnik, W. (2009). 20 Jahre MDK Nordrhein. Ju-
bil
¨
aumsschrift. MDK Nordrhein.
Masaaki, I. (1986). Kaizen: The Key To Japan’s Competi-
tive Success. McGraw-Hill Education.
Newman, M. (2006). Finding community structure in net-
works using the eigenvectors of matrices. Physical
Review E, 74.
Normand, S.-L., Mcneil, B., Peterson, L., and Palmer, R.
(1998). Eliciting expert opinion using the Delphi tech-
nique: identifying performance indicators for cardio-
vascular disease. International Journal for Quality in
Health Care, 10:247 – 260.
N
¨
uchtern, E. (2008). Das professionelle Gutachten. Beson-
derheiten in der gesetzlichen Krankenversicherung.
MedSach, 105 (3):96–98.
Polak, U. W. (2018). Evaluation von Durchgangsarzt-
berichten mithilfe eines Peer-Review-Verfahrens.
Trauma Berufskrankh, 20 (Suppl. 4):237–240.
Sawicki, P. and Bastian, H. (2008). German Health Care: A
Bit of Bismarck Plus More Science. BMJ, 337:a1997.
Schmacke, N. (2016). Zur Positionierung des MDK in
der gesetzlichen Kranken- und Pflegeversicherung,
Gutachten im Auftrag des AOK-Bundesverbandes. In
IPP-Schriften, Eds. Bolte, G, G
¨
orres, S. and Ger-
hardus, A., page Bd. 14. Institut f
¨
ur Public Health und
Pflegeforschung (IPP) der Universit
¨
at Bremen.
Shewhart, W. A. (1931). Statistical Method from the view-
point of quality control. (Reprint im Jahr 1986 einer
Ver
¨
offentlichung des Department of Agricultuire Mil-
waukee 1931). New York: Dover Publication.
Shinano, Y., Fujie, T., and Kounoike, Y. (2003). Effective-
ness of Parallelizing the ILOG-CPLEX Mixed Inte-
ger Optimizer in the PUBB2 Framework. In Euro-Par
2003 Parallel Processing, pages 451–460. Springer
Berlin Heidelberg.
Strahl, A., Gerlich, C., Alpers, G., Ehrmann, K., Gehrke,
J., M
¨
uller-Garnn, A., and Vogel, H. (2018). Devel-
opment and evaluation of a standardized peer-training
in the context of peer review for quality assurance in
work capacity evaluation. BMC Medical Education,
18:135–145.
Strahl, A., Gerlich, C., Wolf, H.-D., Gehrke, J., M
¨
uller-
Garnn, A., and Vogel, H. (2016). Qualit
¨
atssicherung
in der Sozialmedizinischen Begutachtung durch Peer
Review - ein Pilotprojekt der Deutschen Rentenver-
sicherung. Gesundheitswesen, 78:156–160.
Thiele K.-P., Kreuzer C., M. R. (2018). Krankenhaus-
landschaft in Deutschland: Zukunftsperspektiven, En-
twicklungstendenzen, Handlungsstrategien, chapter
Exkurs 3: MDK-Pr
¨
ufung - Fluch oder Segen?, pages
89–94. Stuttgart: Kohlhammer.
Wirtz, M. and Caspar, F. (2002).
Beurteiler
¨
ubereinstimmung und Beurteilerrelia-
bilit
¨
at: Methoden zur Bestimmung und Verbesserung
der Zuverl
¨
assigkeit von Einsch
¨
atzungen mittels
Kategoriensystemen und Ratingskalen. G
¨
ottingen:
Hogrefe.
HEALTHINF 2020 - 13th International Conference on Health Informatics
360
