
Challenges and Opportunities for Caregiving through Information
and Communication Technology
Jane Moloney
1
, Raja Manzar Abbas
2
, Sarah Beecham
2
, Bilal Ahmad
2
and Ita Richardson
2
1
Department of Computer Science and Information Systems, University of Limerick, Limerick, Ireland
2
Lero, the Irish Software Research Centre, University of Limerick, Ireland
Keywords: Caregivers, Technology, Qualitative Study, Older Adult Care, Monitoring, Prototype.
Abstract: The increased susceptibility of world’s population to diseases augmented with the decrease in the healthcare
workforce leads to over-reliance on caregivers. This increased burden on caregivers adversely impacts their
quality of life. However, information and communication technology (ICT) has the potential to facilitate
caregiving. Therefore, the objective of this study is to investigate the opportunities and challenges for
caregiving through ICT, the development of a prototype to support caregivers better monitor their care
recipients (known as clients) and the evaluation of that prototype. A qualitative study with 10 caregivers was
conducted to address the research questions from which data was coded and analysed. Using this data, a web-
based prototype was developed and evaluated by 5 caregivers and 5 technology experts. The instruments used
were interviews and focus groups. The results revealed eight categories for improving care identified by
caregivers.
1 INTRODUCTION
The world’s population is becoming more susceptible
to disease and disability, high birth rates with lower
mortality rates, the prospective workforce not
choosing healthcare as a profession and the shortage
of supported facilities. In Ireland, healthcare staffing
levels have dropped significantly within the public
sector since 2009 (Wells and White, 2014). This
situation leads to over-reliance on family or
professional caregivers, which adversely impacts
their quality of life (Canam et al., 1999, Osse et al.,
2006, Shiue et al., 2016), and it is noted that some of
the problems that caregivers encounter include
anxiety, depression and stress (Koyanagi et al., 2018,
Washington et al., 2018). Information and
Communication Technology (ICT) has the potential
to alleviate these problems and help caregivers
perform their duties efficiently and effectively
(Finkel et al., 2007, Chi et al., 2015, Czaja et al., 2016,
Demers et al., 2018). A recent systematic literature
review provides an in-depth analysis on the type of
ICT offerings in this context such as education,
consultation, behavioural therapy, social support,
data collection and monitoring and clinical care
delivery (Chi et al., 2015). This work also reveals that
only 20% of the technology developed falls under the
domain of monitoring, so further work is needed on
this topic. Our analysis indicates that only 2 tools
mentioned in research studies (Chou et al., 2012;
Shah et al., 2013) help in care management while also
solving other problems of caregivers such as social
isolation and quality of life. But, caregivers cited
problems with the design, reliability, weight, and size
of the equipment as serious challenges, decreasing
their satisfaction and increasing their frustration. A
literature review by some of this paper’s authors also
highlights problems with the technology which is
available to support the social life and healthcare of
patients such as older adults (Ahmad et al., 2017).
This situation advocates the need to continue research
in this area and explore the challenges and
opportunities for caregiving through ICT before
commencing the development of systems. The
objective of this study is to understand how ICT
monitoring in the home can alleviate the burden on
the caregivers, and provide a better quality of life
(QOL) for both stakeholders (caregivers and care
recipients). Care recipients are often older adults.
The nomenclature used by caregivers during
interviews when discussing care recipients is ‘client’,
and so, for consistency in this paper, we will refer to
care recipients as ‘clients’. An analysis of the
literature and a qualitative study of a small sample of
Moloney, J., Abbas, R., Beecham, S., Ahmad, B. and Richardson, I.
Challenges and Opportunities for Caregiving through Information and Communication Technology.
DOI: 10.5220/0008893603290336
In Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2020) - Volume 5: HEALTHINF, pages 329-336
ISBN: 978-989-758-398-8; ISSN: 2184-4305
Copyright
c
2022 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
329

stakeholders, led to the development and evaluation
of a web-based prototype for an optimized home
based monitoring system for caregivers.
Section 2 describes the methodology used during
this research. Section 3 discusses the outcome from
caregiver interviews. Section 4 describes how the
findings of interviews were used to develop the
prototype. Section 5 presents the evaluation of the
prototype using focus groups. Section 6 concludes the
paper, presents the recommendations and outlines
future work.
2 METHODOLOGY
The objective of this study is to address the following
research questions:
1. Can ICT support the monitoring of clients in the
home for improved caregiving efficiency?
2. Could the provision of ICT monitoring reduce
burden of the caregiver and improve QOL of the
client?
To answer these research questions, we undertook
a qualitative study with clients and caregivers. Based
on this study, we developed a prototype device using
proprietary product, aimed at monitoring clients in
the home.
2.1 Data Collection: Interviews
We conducted semi-structured interviews over a 2-
day period, with a purposive sample of 10 caregivers
of clients (mainly older adults), based in Ireland (see
Lero Technical Report 2020-TR-01 for the interview
protocol). The primary objective was to identify the
difficulties associated with caregiving to clients and
how ICT might reduce some of the challenges for
caregivers. Using 14 questions, also available in
2020-TR-01, derived from related literature, we
uncovered a set of requirements. The average
duration of each interview was 30 minutes and was
audio recorded. We developed and evaluated a
prototype.
2.2 Data Collection: Focus Groups
To carry out the evaluation, we undertook a focus
group (see protocol in 2020-TR-01). This allowed us
to gain feedback on the prototype and to identify
features for future refinement. One 90-minute session
was held with a mix of participants – 5 caregivers and
5 technology experts. The key requirement for
technology experts was to involve researchers and/or
developers who are directly linked with homecare
technology development. All caregivers who
participated in the focus group had been involved in
the group of interviewees.
2.3 Data Analysis
Audio recordings of the interviews and focus groups
were transcribed, and were analysed using descriptive
coding (Saldana, 2015) to determine key topics. This
was achieved through labelling the important
concepts in the transcripts. These labels were
scrutinized against the research questions to gain
further context of the labels. Furthermore, memoing
and commenting was done liberally. Descriptive
coding was used as an input to perform pattern
coding, determining the high level concepts and the
relationships between them. Finally, axial coding was
undertaken which helped to gain a deeper
understanding of categories.
3 IMPROVING CARE
In this section, we outline our answer to Research
Question 1: Can ICT support the monitoring of clients
in the home for improved caregiving efficiency?
Interview analysis using descriptive and pattern
coding resulted in the identification of eight
categories.
1. Technology for Monitoring: A major concern
amongst all the caregivers was the lack of monitoring
of their clients. Eighty per cent of participants were
either family care or voluntary care persons who did
not earn a financial salary from the care they
provided. Therefore, they need to remain in full time
employment, meaning that they could not monitor
clients for large amounts of time. This same 80%
were concerned with external factors such as
temperature changes across seasons as, regardless of
whether a source of heating or cooling patients’
homes was available, some patients do not avail of
these methods. An extreme example is that one
patient did not use the heating for a few days,
ultimately causing hyperthermia. Temperature
monitoring would have averted this.
2. Technology to improve Safety: Caregivers were
worried about the safety of their clients and
highlighted the need for purpose built housing; clients
are at a vulnerable stage in their lives and likelihood
of injury is very high. One participant quoted that it is
becoming increasingly difficult for their client to
reach the first floor of their home where their main
sleeping quarters are located. Dangers include clients
HEALTHINF 2020 - 13th International Conference on Health Informatics
330
falling down the stairs and nobody knowing for a few
hours until a neighbour visited. Real-time monitoring
technology has the potential to provide a safer
environment.
3. Technology for Security: Participants stated that
clients face serious security issues such as strangers
calling to the doors of clients leading to burglary,
assault or confidence tricks, with all participants
reporting security-related events. One particular
example was when strangers attempted to convince
their client to pay a sum of money. Being
unsuccessful, they assaulted the person. Participants
suggested that there is a need for a technology which
can provide instant alerts to caregivers or emergency
services. They also shed light on clients’ lack of
familiarity with current technology such as
smartphones, indicating that technology should be
designed in an easy to use and intuitive fashion.
4. Technology to Support Emergencies:
Participants advocated the need for a ‘single action
alert’ or a ‘voice-activated alert’ to alleviate the
difficulty vulnerable people face while reporting
emergency situations using technology such as
smartphones. They also said that clients are not well
versed with the latest technology and some are living
without mobile phones and Internet, so alternative
mechanisms to report emergencies would be
appreciated and could be more easily adopted by their
clients.
5. Resources: A lack of resources was identified, for
example, where multiple clients are co-habiting, as in
the case of spouses. One participant quoted that their
deaf client had to take care of a blind person. It is
obvious from this how much support these clients can
provide to each other, and that any technological
solution which improves this situation would be
welcomed.
6. Primary Care: A positive outcome was ease of
access to general practitioners through appointments,
but transportation was still troublesome, e.g. “While
the request is relatively simple to submit and it only
takes 24 hours to get approval, it is still the difference
of 30 minutes to 24 hours in the case of something
that may be more of a serious case than first thought”
- Participant C4. This delay in primary care
concerned the participant who understood that
insurance implications needed to be adhered to as
well.
7. Assistive Technology: Participants agreed that
assistive technology would be beneficial for
providing homecare. Forty per cent of the participants
revealed that significant injury had happened to their
clients during the provision of care. An advance could
be to have lifting technology (operated via a computer
user interface) to reduce injuries.
8. Processing of Requests: The government is
providing lifting technology to eligible clients but the
processing time is extremely slow. One participant
said: “It should not have taken that long to receive a
chair I could have purchased online and received in
a fraction of the time for my mother to have basic
comfort in her own home” - Participant C9. It was
clear from participants’ reviews that the request
submission process should be changed.
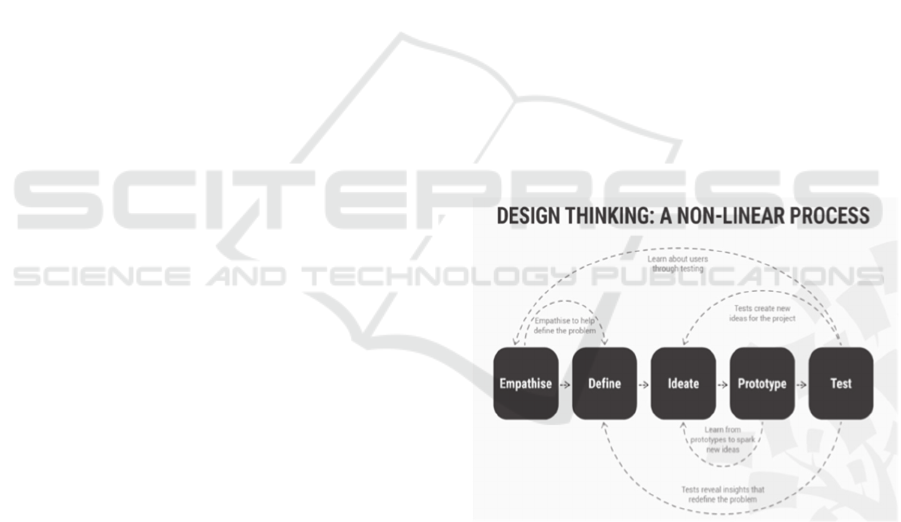
4 PROTOTYPE DEVELOPMENT
Based on our interview analysis, a prototype was
developed using design thinking (Siang, T. 2019), see
Figure 1. Prototyping an application is crucial in
helping participants understand the key aspects of a
proposed system are and allows them to interact with
features as if it were a real-life system. Design
thinking was used as it helps to strip away non-
essential aspects of the problem situation. Within
design thinking, there are 5 stages – empathize,
define, ideate, prototype and test. In this project, we
undertook the first 4 stages.
Figure 1: Design Thinking Process (Siang, T. 2019).
4.1 Empathize
The interview data was reviewed to understand the
caregiver’s feelings, needs, and problems and pain
points. A spectrum of feelings and the associated
behaviours of all of the participants were extracted
through the review of interview data as indicated in
Table 1 in Lero Technical Report No: 2020-TR-01.
These include anxiety, guilt and regret and they were
observed amongst all participants at some stage
during the interviews. Particularly harrowing was the
Challenges and Opportunities for Caregiving through Information and Communication Technology
331
guilt and anger, which were two common feelings
portrayed. One participant spoke of the decision to
put their client into a professional care home due to
the lack of availability of help, time and facilities
when the client was cared for at home. Such
information was used in prototype design.
4.2 Define
After understanding caregivers’ feelings and
behaviours, they were translated into point of views
(POV), which constitutes of three measures i.e. User,
Need and Insight. Table 2 (in Lero Technical Report
No: 2020-TR-01) presents the complete point of view
analysis table. These user needs and insights were
then used to generate ‘How Might We’ (HMW)
questions. The POV table and the HMW questions
were later used as an input to brainstorm and define
the problem statement:
“Design and develop a product that aids family
carers who care for clients in the clients’ own home.
This should enable a more stable life balance maybe
only requiring touch points with client, to a full care
suite. This should encompass features that allow
monitoring, safety in the home, security features and
alert features”.
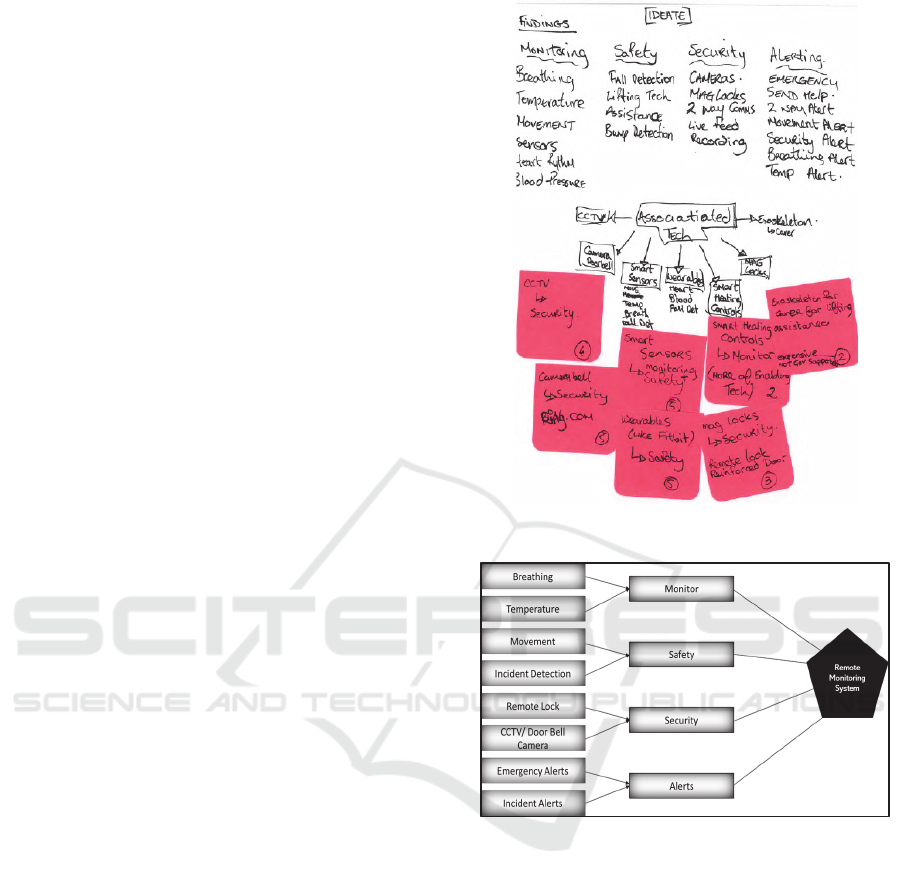
4.3 Ideate
Ideation was the third phase and it constituted of
brainstorming by the researcher to generate numerous
ideas by broadly exploring the solution space to
determine the best outcome. Typically, this phase
requires a team, but due to time constraints, the first
author completed this activity and later validated the
results using a focus group. Mind mapping was used
as an aid during this phase, ultimately inputting to the
development of the prototype. The raw outcome of
the ideation phase in shown in Figure 2 and the model
is depicted in Figure 3. This model applies technology
to homecare situation to see the positive effects on the
client. Based on the findings, the main aspects of the
model and the resulting system should include
monitoring of the clients’ breathing and temperature,
ensuring the safety of the client and incident
detection, the security of the client and enabling alerts
to the caregiver with specific consideration to
emergency alerts.
Figure 2: Ideating Phase Outcome.
Figure 3: Model for Remote Monitoring System.
4.4 Prototype
The model was used as the basis for prototype
development. The underlying assumptions during the
development of prototype were that some ambient
living solutions were available. The clients’ home
has been fitted with detection sensors and cameras
and a doorbell with a camera and 2-way intercom on
the exterior. Motion and temperature sensors, smart
thermostats and intelligent heating controls have been
fitted inside. Clients have been given a smart watch
to monitor vitals and to increase accuracy on fall
detection.
While we recognise that this set of systems is
complicated in themselves, they are each readily
available commercially, and the requirement from the
HEALTHINF 2020 - 13th International Conference on Health Informatics
332

caregiver focuses on the ability to monitor clients’
activities. A sitemap of the prototype was developed
(available in the technical report), with each branch
having its own individual dashboard. An example of
one high level dashboard is shown in Figure 4.
Figure 4: Remote Monitoring System - Client Dashboard.
5 PROTOTYPE EVALUATION
To answer Research Question 2: Could the provision
of ICT monitoring reduce burden of the caregiver and
improve QOL of the client?, the prototype was
evaluated through a focus group with caregivers and
technology experts. By following the guidelines by
Jankowicz (1995), the researcher remained cognitive
and provided appropriate interjections to keep the
discussion focused, probing deeper into the topic to
encourage participants to express their views in
detail, thus enriching the data. Eight key items were
identified, and are discussed here under the headings
of features and usability.
5.1 Features
Overall, the participants liked the features of fall
detection, body temperature and access to
surveillance remotely from a mobile device. For
example, a participant highlighted the importance of
this prototype system in general: “I had an incident
where my client had fallen down the stairs and had
not been found until the following morning. With this
the response is almost immediate meaning my client
will never have to experience that again” - Caregiver
C1.
5.1.1 Dashboard
Participants were pleased with the simple navigation
through the slide-out menu allowing them to switch
between dashboards quickly and easily. “This menu
displays basic information of the client for
identification and reassurance. Having the option to
view the profile from my client for further information
such as medical history, personal details makes it
easier for me to relay medical history and
information on our GP Visits” – Caregiver C5.
All of the participants agreed on the need for a
feature ensuring that, if they do have an incident, their
client is found and treated within a short period of
time. They also appreciated the clean and easy to use
interface and navigation, but shared a concern of
additional Wi-Fi data charges, as the application
constantly refreshes itself: “Is this not supposed to
help carers regain a balance? Their wallet will be
heavily affected if they have more than eight to ten
clients on the system at each time, data is expensive
outside a set price plan” - Caregiver C3
5.1.2 Alerts
Participants liked the idea of alerts, and shared the
possibility of having additional alerts including
delivery tracking, power outage alert and an increased
audio sensitivity: “There is potential to have more
various on the alerts, while I understand this is just
phase one of the application, it has infinite
possibilities to adapt features to service many other
medical situations” – Technology Expert T1.
Participants were satisfied that the alerts are
automatically assessed by the system to determine the
urgency of each detection for quick analysis by the
user: “This is so beneficial for us to decide whether
the level of care and how urgently we need the client
to be treated after the incident. This could become
and invaluable feature for a lot of work we do, it
allows us to rely on our judgement more”- Caregiver
C3. Moreover, they were pleased with the ability to
get rid of ‘clutter’ and show only the necessary
information: “It’s great that I can pick and choose
what I want to display on dashboard of each of my
clients, there are some things I don’t need to see and
may become cluttered and confusing” - Caregiver C1.
The option to call first responders, emergency
services and family members really impressed all of
the participants: “It is great to see that we are starting
to see the utilization of the rural first responder as
first point of contact before emergency services are
needed. There are certain situations that a first
responder can deal with without having to call
emergency services. It causes extreme anxiety and
stress to care recipients having ambulances arrive to
the home when they are possibly not needed in some
cases” - Caregiver C4.
Challenges and Opportunities for Caregiving through Information and Communication Technology
333

5.1.3 Security
Caregivers were particularly overwhelmed and
grateful because their clients’ stories received distinct
attention during the prototype development and
features were included to ensure their security. They
certainly believe that the security feature will make
difference in their clients’ life: “This security tab
would have certainly made noticeable difference …
Besides providing a solid opportunity to catch the
culprit but it would have offered my client a sense of
feeling safe in their home. Unfortunately, my client
fears being home now alone, so I think this feature
will make a major difference to my client’s quality of
life.”- Caregiver C1.
Technologists, however, pointed out that the
current sensors might provide unnecessary alerts to
the care providers. But, using less sensitive sensors
can alleviate this: “These sensors are so sensitive they
would pick up a leaf in the wind, this may cause
unnecessary alerts to the carer that would revert to
them being on edge more than they are now. The
doorbell-activated camera would be best to detect
people coming to the front door. I think standard
surveillance for the exterior home would be fit for
purpose here” - Technologist T2.
5.1.4 Safety
The safety tab offers real time information based on
incident detection and movement in the home. The
beneficial feature that was highlighted here was that
incidents are automatically analysed by the system
based on urgency. Non-urgent detections are sent to
the alerts tab but do not notify the user. In the
prototype, falls are considered major and then
notification is sent to the caregiver immediately:
“This is a great feature, you can tell if the client is
constantly bumping into something because they may
have forgotten the item is there and it will need to be
moved from the area to mitigate any other incidents
from happening. I know my client’s family bought
them a new chair and the client kept bumping into it
because it was not part of their home originally. It
eventually ended in removing the item because from
consistently bumping the same area repeatedly and
caused a fracture for the client” – Caregiver C2
5.1.5 Monitoring
The monitoring tab highlights the client’s vital data in
real time. This was well accepted by participants,
highlighting that certain clients might be at high-risk
status for pulmonary problems, needing constant and
consistent monitoring. “This is of particular benefit
to my client as the client has an irregular heartbeat
that constantly has to be monitored but this is
extremely difficult for me to do when I have to
maintain my full-time job at the same time. If the
client has an episode, I don’t want it to be my fault
because I was unable to monitor the client closely” -
Caregiver C5.
Technologists were a little bit concerned about the
type of technology that is going to be used to gather
this vital information: “I know this system is still in
its infancy, but I would have concern regarding the
technology you have decided to collect that data with.
There is a fear that the client may not wear the watch
or take it off while an event is occurring. This would
raise a major concern for me, but I am sure there are
better technologies for gathering this information” -
Technologist T4.
5.2 Usability
5.2.1 Aesthetic and Minimalistic Design
Participants complimented the overall design of the
application as it follows the current trend of sleek, flat
minimal design that can easily be familiar for the
user. The participants commented that this makes
analysing information much clearer and easier to
understand, preventing possible errors: “The design
is very attractive, and it has the added bonus that you
don’t need to be a data analyst to understand the
output information and can help carer’s make a
decision to the urgency of the incident at hand and
deal with it remotely” – Technologist T3
This design helps to keep everything organized. It
also notifies the caregiver about the most important
information. It has the potential to alleviate
distractions and ease the decision-making process.
5.2.2 Flexibility and Efficiency of Use
The caregiver can fully customize the user interface
to suit their needs while prioritising information
based on their clients’ needs. The application gives
the caregiver insights rather than having to search for
the information they need. The application is flexible
where icons, tabs and menu panels can be rearranged.
“It’s great how simple it is to use without prior
training. I can move and rearrange items with ease.
This is incredible as I have used other software that
it complicated and I eventually stopped interacting
with it. I actually want to interact with this
application” - Caregiver C2.
One technologist mentioned that a system like this
would help improve the caregiver’s efficiency. The
prototype stays consistent using the side bar menu,
HEALTHINF 2020 - 13th International Conference on Health Informatics
334

which is accessible on every page, and it follows
standard user interface layouts. The opening
dashboard gives full system visibility with quick
information from all possible features.
5.2.3 Probability and Feasibility
Technologist T1’s statement - “Communication
between devices and public service systems is key for
this to succeed, reliance on Wi-Fi connections is a
concern as rural internet infrastructure is not as
developed as urban areas, the introduction of 5G in
the future could contribute to the rural infrastructure
but that is yet to be tested” - generated rich
conversations around infrastructure in Ireland and
whether it will be developed to accept our proposed
solution. The researcher clarified that this research
assumes that the infrastructure is ready. Another
important aspect that was noted was that General
Data Protection Regulations (GDPR) would have a
significant effect on this system and how it is
implemented if it ever became a viable solution.
Security concerns regarding CCTV and live data
would need to be examined thoroughly and cyber
security would need strong protection from system
hackers. As stated by technologist T4: “You would
need to introduce a strong standard around signing
and maintaining consent forms, there would be
significant churn in the public eye around this issue
and vulnerable persons, it may not be held in the best
light”. The participants felt that it was a very feasible
system assuming that all approvals were obtained,
and that privacy was maintained throughout the
development of the system. The prototype sets out to
apply advanced technologies to support home care
providers in their caring roles. Ninety per cent of the
participants felt that it met the goals it set out to do
and feel that if it were ever to be a commercialised
product that was affordable the caregivers would not
hesitate to install it in their clients’ homes.
In short, participants were pleased with the
features and the usability of the proposed application
and gave some useful recommendations for future
work. They mentioned that the fully functional
application would have the potential to give them
back their life balance, allowing them to be free to
work full time and maintain involvement in
recreational activities. Most importantly, it would
support the dignity of their clients.
6 CONCLUSION
This research focused on applying ICT to the home
care sector with a view to optimising the work of
family caregivers. The application of such
technologies was theoretically intended to allow such
caregivers to re-establish or to maintain their life-
balance. It could also support private caregivers to
split their time between several clients. The findings
suggest an overall positive response by the
participants about the prototype developed and its
potential to be commercialized. Some
recommendations were recognised as possibilities for
further development of the application:
System and technologies must grow at the same
pace as other technologies grow and develop.
24/7 customer support will be needed in case of
errors and system crashes.
The system could predict incidents through
gathering information for the implementation of
artificial intelligence (AI) to predict incidents.
Better monitoring technology or other forms of
monitoring technology should be utilised.
Improved user interface aesthetics helps to build
a positive relationship, workflow and interaction
of the caregiver.
Remote locking of front and back doors could be
included in the application.
Other safety measures could be implemented,
such as slip detection, recognition of
overheating, and vital sign measurement.
Our future work, particularly through our
membership of the Ageing Research Centre and our
industry links within Lero – the Irish Software
Research Centre, will investigate further how such
technologies can support caregivers in their vital job
of caring for older persons, while also providing
effective care to the client.
ACKNOWLEDGMENTS
This work was supported, in part, by Science
Foundation Ireland grant no. 13/RC/2094. It was
carried out in partial fulfilment of the MSc in
Technology Management at the University of
Limerick (Atlantic University Alliance Ireland) and
the research ethics number is Ref.2019_07_04_S&E.
Challenges and Opportunities for Caregiving through Information and Communication Technology
335

REFERENCES
Ahmad, B., Richardson, I. and Beecham, S., 2017,
November. A Systematic Literature Review of Social
Network Systems for Older Adults. In International
Conference on Product-Focused Software Process
Improvement (pp. 482-496). Springer, Cham.
Ahmad, B., Richardson, I., McLoughlin, S. and Beecham,
S., 2018, July. Assessing the level of adoption of a
social network system for older adults. In Proceedings
of the 32nd International BCS Human Computer
Interaction Conference (p. 225). BCS Learning &
Development Ltd.
Britto, M.T., Jimison, H.B., Munafo, J.K., Wissman, J.,
Rogers, M.L. and Hersh, W., 2009. Usability testing
finds problems for novice users of pediatric portals.
Journal of the American Medical Informatics
Association, 16(5), pp.660-66.
Byczkowski, T.L., Munafo, J.K. and Britto, M.T., 2014.
Family perceptions of the usability and value of chronic
disease web-based patient portals. Health informatics
journal, 20(2), pp.151-162.
Canam, C. and Acorn, S., 1999. Quality of life for family
caregivers of people with chronic health problems.
Rehabilitation Nursing, 24(5), pp.192 200.
Chi, N.C. and Demiris, G., 2015. A systematic review of
telehealth tools and interventions to support family
caregivers. Journal of telemedicine and telecare, 21(1),
pp.37-44.
Chou, H.K., Yan, S.H., Lin, I.C., Tsai, M.T., Chen C.C. and
Woung, L.C., 2012. A pilot study of the telecare
medical support system as an intervention in dementia
care: the views and experiences of primary caregivers.
Journal of Nursing Research, 20(3), pp.169-180.
Czaja, S.J., 2016. Long-term care services and support
systems for older adults: The role of technology.
American Psychologist, 71(4), p.294.
Demers, L., Fast, J., Mortenson, W.B., Routhier, F., Auger,
C., Ahmed, S., Boger, J., Rudzicz, F., Plante M. and
Eales, J., 2018. Developing innovative interdisciplinary
technological solutions for caregivers of older adults
within Canada's technology and aging network. Annals
of Physical and Rehabilitation Medicine, 61, p.e409.
Finkel, S., Czaja, S.J., Martinovich, Z., Harris, C., Pezzuto,
D. and Schulz, R., 2007. E-care: a telecommunications
technology intervention for family caregivers of
dementia patients. The American journal of geriatric
psychiatry, 15(5), pp.443-448.
Maher, M., Kaziunas, E., Ackerman, M., Derry, H.,
Forringer, R., Miller, K., O'Reilly, D., An, L.C.,
Tewari, M., Hanauer, D.A. and Choi, S.W., 2016. User-
centered design groups to engage patients and
caregivers with a personalized health information
technology tool. Biology of Blood and Marrow
Transplantation, 22(2), pp.349-358.
Osse, B.H., Vernooij-Dassen, M.J., Schadé, E. and Grol,
R.P., 2006. Problems experienced by the informal
caregivers of cancer patients and their needs for
support. Cancer nursing, 29(5), pp.378-388.
Saldana, J., 2015. The coding manual for qualitative
researchers. Sage.
Shah, M.N., Morris, D., Jones, C.M., Gillespie, S.M.,
Nelson, D.L., McConnochie, K.M. and Dozier, A.,
2013. A qualitative evaluation of a telemedicine
enhanced emergency care program for older adults.
Journal of the American Geriatrics Society, 61(4),
pp.571-576.
Shiue, I. and Sand, M., 2016. Quality of life in caregivers
with and without chronic disease: Welsh Health
Survey, 2013. Journal of Public Health, 39(1), pp.34-
44.
Siang, T. (2019). What is Design Thinking? [online] The
Interaction Design Foundation. Available at:
https://www.interactiondesign.org/literature/topics/des
ign-thinking [Accessed 1 Oct. 2019].
Koyanagi, A., DeVylder, J.E., Stubbs, B., Carvalho, A.F.,
Veronese, N., Haro, J.M. and Santini, Z.I., 2018.
Depression, sleep problems, and perceived stress
among informal caregivers in 58 low-, middle, and
high-income countries: a cross-sectional analysis of
community-based surveys. Journal of psychiatric
research, 96, pp.115-123.
Washington, K.T., Parker Oliver, D., Smith, J.B., McCrae,
C.S., Balchandani, S.M. and Demiris, G., 2018. Sleep
problems, anxiety, and global self-rated health among
hospice family caregivers. American Journal of
Hospice and Palliative Medicine®, 35(2), pp.244-249.
Wells, J. and White, M. (2014) ‘The impact of the economic
crisis and austerity on the nursing and midwifery
professions in the Republic of Ireland – “boom”, “bust”
and retrenchment’. doi: 10.1177/1744987114557107.
HEALTHINF 2020 - 13th International Conference on Health Informatics
336
