
The Effectiveness of Enhanced External Counterpulsation (EECP)
Therapy for Heart Disease Patients
Johannes Bastira Ginting
1
, M. K. M, Okta Jaya
2
1
Faculty of Public Health, University Prima Indonesia, Medan, Indonesian
2
Faculty of Computer Science and Technology, University Prima Indonesia, Medan, Indonesian
Keywords: EECP, angina pectoris 2019.
Abstract: According to the WHO, the estimated number of deaths by 2020 in the world, especially in developing
countries, will be caused by chronic diseases, and 71% due to ischemic heart disease. EECP (Enhanced
External Counterpulsation) is an FDA-approved non-invasive alternative therapy that is particularly beneficial
for patients with heart disease. This study is a qualitative study, conducted at the wellness center of Royal
Prima Hospital, June 2020, the number of samples as many as 15 respondents. Miles and Huberman's data
analysis with the encoding used in the data analysis process is open encoding, axial encoding, and selective
encoding. As a result of the study, the majority of respondents expressed chest pain (angina pectoris)
expressed a decrease of 13 people (86.7%) and stated chest pain was no longer as much as 2 people (13.3%).
In terms of quality of life, all respondents stated an increase in life, with an increase in physical activity that
can be felt by the respondent. Concluded research, that EECP therapy provides effectiveness that reduces
chest pain and improves the quality of life of respondents who have undergone therapy 35 times. In the future,
more and more health facilities are providing EECP therapy facilities, especially in Medan.
1 INTRODUCTION
According to WHO data, the estimated number of
deaths by 2020 worldwide, especially in developing
countries, 75% will be caused by chronic diseases and
71% due to ischemic heart disease, (WHO Technical
Report Series, 2013). The UK states coronary heart
disease (CHD) is the leading cause of death. One in
five men and one in six women die from CHD. Every
year 101,000 people die from CHD, (Colin Tidy, d.
2012). Sudden cardiac death (SCD) events reach
400,000 cases per year in developed countries such as
the United States.
Indonesia as a developing country, but the pattern
of disease is already the same as the pattern of
diseases of developed countries, CHD is still the most
common disease-causing sudden death, (Yuniadi Y,
2019).
From the data of the Indonesian Association of
Cardiovascular Specialists (PERKI) 2019, it is
reported that CHD (which is classified as circulatory
system disease) is the main cause and the first of all
deaths, which is 26.4%, this figure is four times
higher than the death rate caused by cancer (6%). In
other words, approximately one in four people who
died in Indonesia were from CHD (Firdaus. I. 2019).
Sudden death is often caused by dangerous
cardiac arrhythmias triggered by sudden blockages of
the coronary arteries that have been narrowed due to
plaque forming in the atherosclerosis process. The
process of atherosclerosis, which is the main cause of
CHD, begins from young adulthood, and the plaque
that forms increases in age or time (Suherman.J,
2019).
The main cause of plaque formation is an
endothelial injury that lines the inside of the blood
vessels. Factors that play a role in continuous
endothelial injury are LDL (Low-Density
Lipoprotein) levels, high cholesterol, hypertension,
smoking, diabetes mellitus, and others (Insull W Jr,
2009).
There are currently several non-pharmacological
alternative therapies for patients with or without heart
failure, namely: neurostimulation (electrical
stimulation of transcutaneous nerves and spinal
medulla stimulation), EECP (Enhanced External
Counterpulsation), laser revascularization
techniques, gene therapy, and recent interventional
procedures such as percutaneous in situ coronary
artery bypass. However, a non-invasive and FDA-
approved alternative therapy is EECP therapy. Where
the target of EECP therapy is to open the existing
196
Ginting, J. and Okta Jaya, M.
The Effectiveness of Enhanced External Counterpulsation (EECP) Therapy for Heart Disease Patients.
DOI: 10.5220/0010292601960201
In Proceedings of the International Conference on Health Informatics, Medical, Biological Engineering, and Pharmaceutical (HIMBEP 2020), pages 196-201
ISBN: 978-989-758-500-5
Copyright
c
2021 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
coronary artery collateral and form new blood vessels
to provide blood supply to the blood-deficient heart
muscle. EECP benefits more in people with
narrowing of one or two major vessels. Unfortunately
in Indonesia, not many choose this non-invasive
therapy that has proven beneficial. That may be
because there are still few facilities that provide
EECP therapy and information about eecp therapy
methods is still lacking.
This study aims to identify the effectiveness of
EECP therapy against heart disease patients who are
undergoing therapy and who have undergone EECP
therapy. With the higher rate of morbidity and
mortality of coronary heart disease, it is expected that
later with this research, will add insight, public
information about EECP therapy, so that it can be
considered to the public in the treatment of CHD in
addition to the treatment of CABG surgery or less
invasive stent installation.
Several studies have been conducted to look at the
effectiveness of EECP therapy, which is used as
follows:
No Research Title Results
1 Effect of enhanced
external
counterpulsation therapy
on myeloperoxidase in
lowering cardiovascular
events of patients with
chronic heart failure
EECP therapy
lowers the MPO
levels of GJK
patients so that it
can decrease
cardiovascular
events within 6
months of
observation. The
higher the MPO
level correlated
with the higher the
incidence of
cardiovascular
events.
Researcher's name:
Starry H. Rampengan,
etc
Place and Time of
Research: General
Hospital of Prof Dr. R.
D. Kandou, Manado
Siloam Hospital,
Manado Adventist
Hospital, and Manado
Jade Cardiovascular
Clinic, January-
December 2012
(Rampengan, S. H,
2015).
Researcher's name:
Starry H. Rampengan,
etc
Time and Place of
Research: January 2014
and June 2015, Jade
Cardiovascular Clinic,
Manado, North
Sulawesi, Indonesia
(Rampengan, S. H,
2017).
2 Quality of life
improvement of
chronic heart failure
patients after the effect
enhanced external
counterpulsation
(EECP) therap
y
The WHO-5
questionnaire
resulted in false
before and after
EECP therapy, but in
the EECP group
showed statistically
significant
differences (p<0.05).
The WHO-5
questionnaire
attributes the results
to a significant
increase in feeling
cheerful and in good
spirits (p=0.03) and
waking up feeling
refreshed (p=0.030)
in the EECP group
compared to the fake
group. Conclusion:
EECP therapy is
effective for reducing
depression thus
improving quality of
life in CHF
p
atients
Researcher's name:
Starry H. Rampengan,
etc
Time and Place of
Research: January 2014
and June 2015, Jade
Cardiovascular Clinic,
Manado, North
Sulawesi, Indonesia
(Rampengan, S. H,
2017).
Nearly a century and a half ago, researchers at
Havard University began experiments with
counterpuIsasi. They have proven that this technique
can meaningfully reduce the workload and oxygen
consumption of the left ventricle. In 1953, Kantrowitz
et al. described diastolic changes as the cause of
increased coronary blood flow. Birtwell et al. in the
USA began the development of this technique, he first
implemented the concept by developing an artery
pulsator counter. Zheng et al. reported for the first
time the advantages of using external
counterpulsation in the 1980s, he used pneumatic
counterpulsation tools.
Lawson et al. at the State University of New York,
Stony Brook, analyzed several open studies of EECP
use between 1989-1998, using objective and
subjective viewpoints. These studies show that,
although open and not random, EECP users
statistically produce progress on exercise tolerance.
This is evidenced by thallium stress tests, which show
partial or total healing from coronary perfusion
defects. In 1999 for the first time, Arora et al. Report
the results of the multicenter Study of Enhanced
External Counterpulsation (MUST-EECP) double-
blind randomized placebo-controlled test. Since then,
EECP therapy has emerged as an effective, non-
invasive, and reliable alternative therapy for patients
with angina, even those with heart failure (Insull W
Jr, 2009). According to Prof. Peter Kabo, in
Indonesia, the first person to promote EECP is Prof.
The Effectiveness of Enhanced External Counterpulsation (EECP) Therapy for Heart Disease Patients
197
Dr. Syukri Karim. They did a simple study and the
results showed that EECP improved the
manifestations of CHD tested with ECG, treadmill
test, or talcum scintigraphy. In 1997, Indonesia was
the only country in Southeast Asia to have an EECP.
But currently, EECP has been used in Malaysia, Hong
Kong, Taiwan, Philippines, and Singapore as one way
of countermeasures cardiovascular (Suherman.J,
2019).
EECP tools work regulated by computers based
on the patient's electrocardiogram to increase arterial
diastolic blood pressure thereby improving diastolic
blood flow in the coronary, cerebral, and renal
arteries, as well as stimulating diuresis and natriuresis
(Insull W Jr, 2009). In 2002, the FDA approved
EECP therapy for patients with heart failure due to
myocardial ischemic. EECP (Enhanced external
counterpulsation) therapy is a non-invasive therapy
using three sets of pneumatic cuffs wrapped around
the calves, thighs, and hips. Air filling and emptying
in cuffs is regulated according to the heart cycle based
on a computer-controlled ECG.
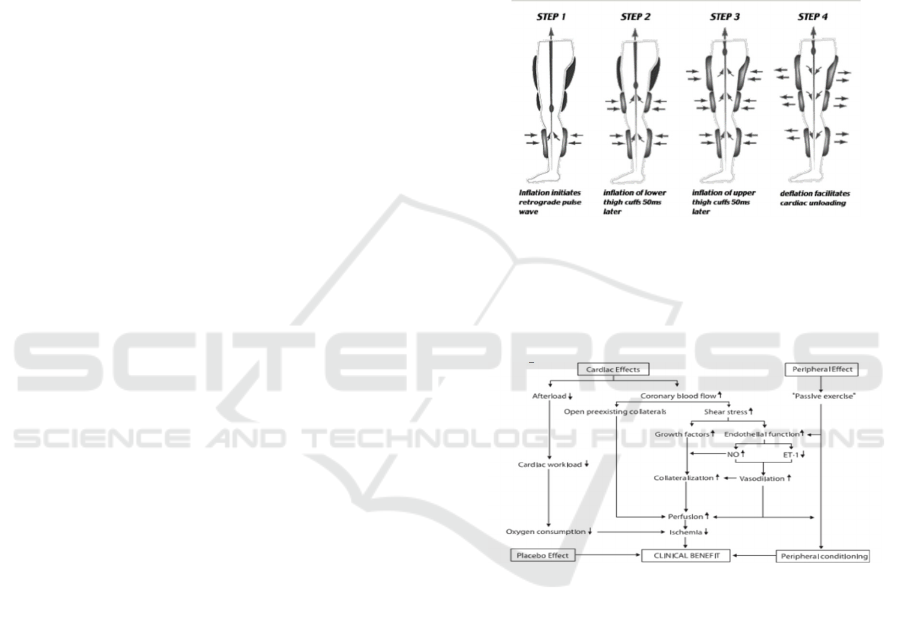
At the time of diastole onset, three sets of cuffs are
filled with air quickly with adjustable pressure,
sequentially starting from the calf, then the thigh, and
the last in the hip. Thus the blood from the lower
limbs is squeezed back and channeled to the base of
the aorta (counterpulsation). The increased diastolic
pressure increases the perfusion pressure of the
coronary artery, opens the existing collateral vessels
and shear stress that occurs in the coronary artery will
improve endothelial dysfunction.
Patients who will benefit from EECP therapy
include patients with angina attacks that cannot be
overcome by pharmacological therapy (refractory
angina) and limiting their activity to avoid angina
symptoms. Patients with coronary anatomy are not
suitable or at high risk for revascularization therapy.
EECP therapy is also not a great choice for patients
with microvascular angina (cardiac syndrome X) and
diabetic Mellitus patients with coronary heart disease.
The target of EECP therapy is to open the existing
coronary artery collateral and form new blood vessels
to provide blood supply to the blood-deficient heart
muscle. EECP benefits more in people with
narrowing of one or two major vessels. If narrowing
has occurred in the 3 main coronary vessels then
EECP therapy should be done after CABG.
Guidelines for EECP therapy are:
1. Therapy is carried out daily for one hour, a
week 6 times to 36 times.
2. All drugs are consumed as prescribed, except
diuretic drugs should not be taken before
therapy as it will interfere with therapy.
3. Patients do not eat or drink 2 hours before
therapy.
4. The patient empties the bladder before therapy
begins.
5. The patient wears cotton trousers that fit
perfectly.
6. The patient's blood pressure and pulse
frequency are checked before and after therapy.
7. ECG, heart rate frequency, and oxygen
saturation and plethysmograph monitored
during therapy
Figure 1. EECP (Rampengan, S. H, 2017) Therapy Stage
Diagram
Steps 1-3 of air are pumped in succession shortly after
pistol Step 4 air is sucked simultaneously shortly
before pistol.
Figure 2. Mechanism of eecp therapy clinic benefits
2 RESEARCH METHODS
This research was conducted with a qualitative
approach. This means that the data collected is not in
the form of numbers, but rather it comes from
interview scripts, field notes, personal documents,
memo notes, and other official documents, so the
purpose of this qualitative research is to portray the
empirical reality behind the phenomenon in-depth,
detail and complete. This research was conducted at
the Royal Prima Wellness Center Hospital 5th Floor,
in 2019. The population is all coronary heart patients
undergoing therapy at Wellness Center Rs Royal
Prima Medan. From the initial survey, data found that
HIMBEP 2020 - International Conference on Health Informatics, Medical, Biological Engineering, and Pharmaceutical
198
the average coronary heart patient undergoing EECP
therapy is 5-7 people per month. Therefore,
researchers determined the number of samples as
many as 15 patients, this is because every one patient
takes about 7 to 8 weeks to complete EECP therapy
following EECP therapy guidelines. So that later this
research can be completed according to the schedule
that has been determined.
The data source in this study was the subject from
which the data was processed, primary data being
direct data from patients using semi-structured
interview techniques and documentation. Secondary
data is data from the patient archives at the Wellness
Center of the Royal Prima Hospital and previous
research literature to strengthen the results of the
research and complete the information that has been
collected through in-person interviews with
informants.
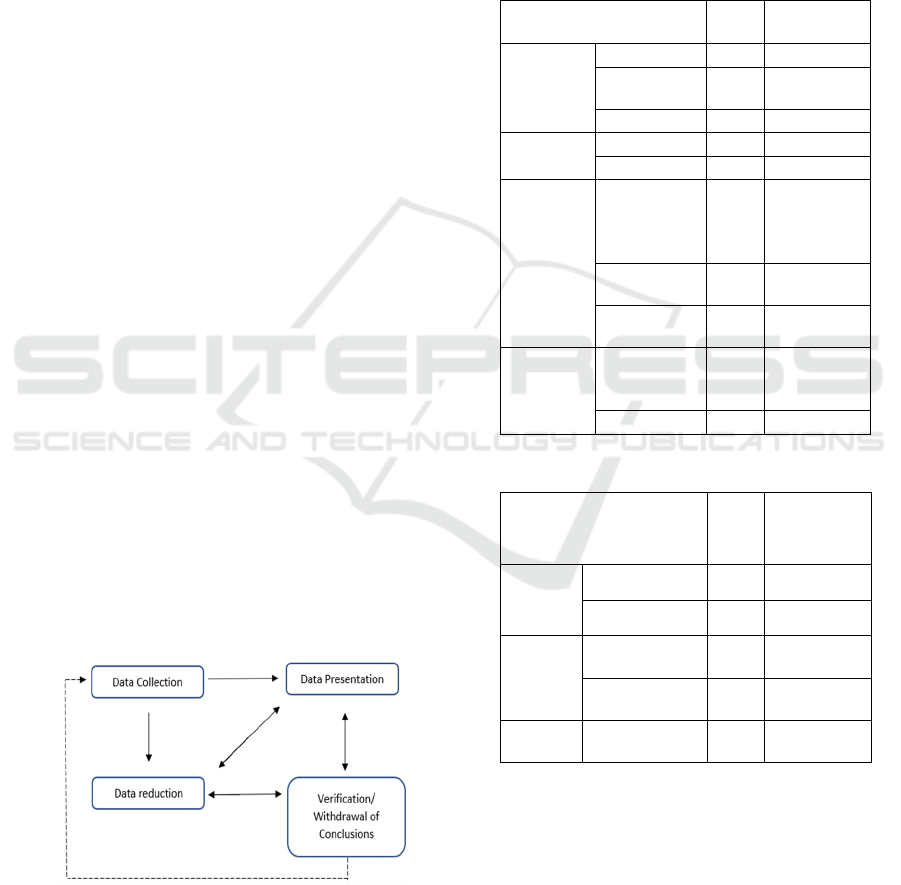
The data analysis techniques used in this study use
Miles and Huberman interactive model data analysis
techniques that include data reduction, data display,
and conclusion drawing/ verification (Saldana. et al,
2014).
Here's an explanation:
a. Data Reduction
At this stage, researchers are sorting through
the results of interviews and documentation
that are still complex and unstructured so that,
researchers obtain data relevant to the study's
problems.
b.
Display Data Display data is the presentation of
data into the corresponding matrix. In
qualitative research, display data or data
presenters can be done in the form of briefs,
charts, and relationships between categories,
flowcharts, and the like. Withdrawal of
Conclusions or Verification In concluding,
researchers begin to look for the meaning of the
data that has been collected (Sugiyono. 2008).
Figure 3. Miles and Huberman Interactive Data
Analysis Model
The results of the study were conducted to 15
respondents, the majority of patients of the male
gender (>65%), the age of the majority of respondents
over 50 years (80%), in terms of education, the
majority of respondents are highly educated (60%), in
terms of employment, the majority of respondents are
self-employed, namely (46.7%), for more details can
be seen in Table 1.
Table 1. Overview of Research Respondents, by Age,
Gender, Education and Employment Status
Variable
Characteristics
Sum
Percentage
(%)
Age
< 40 years 1 6.7
40 s/d 50
years
2 13.3
> 50 years 12 80.0
Gender
Male 10 66.7
Female 5 33.3
Job
PNS,
BUMN,
TNI,
Government
2 13.3
Private
Employees
6 40.0
Self-
employe
d
7 46.7
Education
Higher
Education
(S1, S2, S3)
9 60.0
High school 6 40.0
Table 2: Overview of Research Variables
Research Variables Sum
Percentage
(%)
Therapy
EECP
< 35 Times 5 33.3
≥35 Times 10 66.7
Chest
Pain
Reduced
Chest Pain
13 86.7
Chest Pain
Is Gone
2 13.3
Quality
of Life
There Are
Im
p
rovements
15 100
From table 2, it can be seen by current and current
respondents who have undergone therapy for <35
times as many as 5 (33.3%), who have undergone
therapy ≥35 times as many as 10 (66.7%).
Respondents who expressed chest pain decreased by
13 people (86.7%), and who stated chest pain was no
longer there (never relapsed) as many as 2 people
(13.3%). In terms of quality of life, all respondents
The Effectiveness of Enhanced External Counterpulsation (EECP) Therapy for Heart Disease Patients
199

stated that the quality of life there was an increase of
15 people (100%).
From the results of the study, respondents stated
that the symptoms of chest pain (angina pectoris)
were reduced, and some claimed to have never felt or
experienced chest pain. The researcher's assumption,
that respondents who are and have undergone EECP
therapy have felt the benefits of such therapy.
Whereas we know, the target of EECP therapy is to
open up existing coronary artery collateral and form
new blood vessels to provide blood supply to the
blood-deficient heart muscle. EECP benefits more in
people with narrowing of one or two major vessels.
So it can be concluded EECP therapy has
effectiveness in the treatment of patients who have
coronary heart disorders.
This is in line with research conducted by Darren
PC. Et al, 2008, found that EECP is effective in
reducing plasma levels of alpha tumor necrosis factor
(TNF-α), monocyte protein chemoattractant-1 (MCP-
1), and these changes are in parallel with reducing
chest pain symptoms. Of the quality of life variables,
all respondents stated that this therapy was shown to
improve their quality of life, judging by the patient's
passion and joy to undergo therapy. Because
according to the patient, after undergoing therapy,
their sleep at night is very good, so in the morning the
patient feels very healthy. Also, seen from some
respondents' statements, after EECP therapy, patients
felt the physical improvement was increasing. Where
before undergoing therapy, some respondents can
only walk a few meters, after undergoing therapy,
patients can already increase the intensity of exercise
(walking) more than before undergoing therapy.
There was one respondent, who had previously
been unable to walk again (already in a wheelchair),
after undergoing therapy 35 times, that respondent
had improved, where the respondent was already able
to walk even though he was still bricked up and
helped to walk. This research is in line with the results
of research conducted by Rampengan, S. H, 2015,
wherein his research stated EECP therapy is safe and
effective as well as beneficial on improving quality of
life in patients with chronic heart failure as shown by
the increased walking distance in the six-minute
walking test.
The downside of EECP therapy, there are some
complaints received by researchers from respondents,
namely concerning the problem of the time it takes to
complete the therapy is felt long enough, namely 35
times therapy for 35 days (1 day, therapy 1 hour).
Where if the patient does not live on schedule, then
the therapy should be repeated from the initial count,
to achieve maximum results. And the facilities that
provide EECP therapeutic facilities are still limited.
However, because the respondent immediately felt a
good effect starting from the first therapy, the
respondent felt the weakness of the time was
considered not a big problem. Some statements from
patients who have undergone therapy for 35 times,
continue therapy, with schedule settings 1 therapy
every 1 week, to still be able to maintain their health
condition. According to the respondent's assumption,
with this follow-up therapy, this is done to prevent the
possibility of chest pain as early as possible.
Placebo from the results of this study, according
to respondents who have undergone therapy, said that
although EECP therapy is very helpful to overcome
chest pain but to get the most results, respondents
must also follow the treatment given by the doctor,
consume additional vitamins, and also no less
important, namely the support of the family in the
treatment of their disease.
3 CONCLUSIONS AND
SUGGESTIONS
3.1 Conclusions
In the conclusion of this study, the majority of
patients stated that after undergoing EECP therapy,
chest pain or angina was less than 13 people (86.7%),
even respondents also stated chest pain was no longer
there. In terms of quality of life, all respondents stated
an improvement in the quality of life of 15 people
(100%), characterized by an increase in physical
activity that can be done by respondents after
undergoing therapy. EECP therapy is a non-invasive
for patients with coronary heart disease, whether it
has undergone revascularisation or not. For patients
who experience coronary heart disease because of
complications from DM type2, because with the
presence of EECP therapy then a small probability of
revascularisation action.
This therapy is hilly to improve the quality of life
of the sufferer, visible from the spirit and joy of
patients to undergo such therapy. Since the result of
EECP therapy can make the heart perfusion better and
open the collateral blood vessels that have been and
are thought to form new collateral vessels.
3.2 Suggestions
Because of the limited researchers in the deep dive
into the effectiveness of EECP therapy until
laboratory tests, researchers hoped for the future,
HIMBEP 2020 - International Conference on Health Informatics, Medical, Biological Engineering, and Pharmaceutical
200

researchers could continue with the research by
collaborating with more clinical teams. Expected for
the future, more health facilities that provide EECP
therapy facilities, especially in the city of Medan.
REFERENCES
WHO Technical Report Series. Diet, nutrition, and the
prevention of chronic disease. 916 Geneva. 2003 [cited
2019 June 15]. Available from: https://
whqlibdoc.who.int/trs/WHO_TRS_916.pdf.
Colin Tidy, d. (2012) Epidemiology of coronary heart
disease. Cited 04 05, 2020, from
https://patient.info/pdf/2102.pdf.
Yuniadi Y. Kematian mendadak (tidak) hanya dialami
pria! [cited 2019 June 20],
http://ezcobar.com/dokteronline/dokter15/
Firdaus. I. 2019, Press Release, World Heart Day PERKI
2019, Cited at 26 September 2020.
http://www.inaheart.org/news_and_events/
Suherman.J. Tinjauan Terapi Enhanced External
Counterpulsation (EECP), JKM.Vol.10. No. 1 Juli
2019 :83-90
Munro JM, Cotran RS. The pathogenesis of
atherosclerosis: atherogenesis and inflammation. Lab
Invest. 1988; 58(3):249-61.
Insull W Jr. The pathology of atherosclerosis: plaque
development and plaque responses to medical
treatment. Am J Med. 2009; 122(1 Suppl): S3-S14.
Rampengan, S. H., Prihartono, J., Siagian, M., &
Immanuel, S. (2015). The effect of enhanced external
counterpulsation therapy and improvement of
functional capacity in chronic heart failure patients: a
randomized clinical trial. Acta Medica Indonesiana,
47(4).
Rampengan, S. H., Dundu, A., Prihartono, J., Immanuel, S.,
& Siagian, M. (2017). Quality of life improvement of
chronic heart failure patients after the effect enhanced
external counterpulsation (EECP) therapy. Journal of
Global Pharma Technology, 9(5), 11-21.
Saldana., Miles & Huberman. 2014. Qualitative data
analysis. America: SAGE Publications
Sugiyono. 2008. Memahami Penelitian Kualitatif.
Bandung: cv. Alfabeta
Poerwandari, E.K. (2007). Pendekatan Kualitatif dalam
penelitian Psikologi. Jakarta: LPSP3 Universitas
Indonesia. Darren PC, Conti CR, Nichols WW, Choi
CY, Khuddus MA, Braith RW. Effect of Enhanced
External Counterpulsation (EECP) on inflammatory
cytokines and adhesion molecules in patients with
angina pectoris and angiographic coronary artery
disease. Am J Cardiol. 2008; 101(3):300–2.
The Effectiveness of Enhanced External Counterpulsation (EECP) Therapy for Heart Disease Patients
201
