
The Design and Evaluation of a Home Health Care System
(TeamVisit)
Wesam Shishah
a
, Hessah AlJowesir, Omaimah Subh and Ghaida Hassan
College of Computing and Informatics, Saudi Electronic University, Riyadh, Saudi Arabia
Keywords: Health Care System, e-Heath, User Centered Design, Usability and System Design.
Abstract: The usability of computer systems used in health care is a worldwide issue. Poor usability has been reported
as one of the most common problems in human-computer interaction, negatively affecting the workflow of
health care. Today, the demand for home health care is increasing. It must therefore be supported with a
system that is easy to learn and easy to use. The department of home health care at King Abdullah Medical
Complex in Jeddah (KAMCJ) uses a semi-manual system. This research introduced a system called
“TeamVisit,” which was designed to automate services and to enhance support for workflow management at
the KAMCJ. The User Centered Design (UCD) method was applied to design the TeamVisit system. The
system was designed in three stages: the first stage identified intended users and tasks, the second stage aimed
to confirm whether the system matched user requirements, and the final stage involved initial usability testing
of the TeamVisit system. The paper also summarizes the results of each stage. The paper concludes that users
were satisfied with the design of the TeamVisit system, finding it easy to use.
1 INTRODUCTION
Home health care comprises a wide range of health-
related services provided by health professionals at
the patient’s home or another place outside a medical
facility. Home health care is beneficial in cutting
hospitals’ operational costs, as providing medical
care at home reduces the length of a hospital stay, and
reduces the number of unnecessary hospital
admissions. Home health care also provides support
for the patient’s family and improves quality of
health.
King Abdullah Medical Complex in Jeddah
(KAMCJ) is a hospital in Saudi Arabia that applies
the Saudi Ministry of Health home care program. The
home health care team arranges appointments for
patients registered at KAMCJ and visits them
frequently in their home for regular checkups.
Currently, WhatsApp is used for appointments and
communication and paper forms are used during day
visits. Also, patients must use WhatsApp and come to
the hospital if they require refill order for
supplements or medication.
Poor communication between patients and
medical providers (doctors or nurses) could lead to
a
https://orcid.org/ 0000-0001-6947-9927
unnecessary excessive treatment causing unwanted
side effects (Organization, 2018). A usable computer
system enables users to pay attention to their required
task rather than to the technology itself. According to
Dray (1995), usable systems are easy to learn, easy to
remember, and easy to use. They are efficient,
minimize the chance of errors, and promote user
satisfaction.
The TeamVisit system was designed to enhance
workflow and communication at KAMCJ. This paper
describes the application of User Centered Design
(UCD) to the design stages of the TeamVisit system,
which enhanced its usability.
2 RELATED WORK
2.1 Home Health Care
Home health care began in Saudi Arabia in 1991. The
Home Health Care program (HHC) was developed by
King Faisal Specialized Hospital and Research
Center for patients with terminal cancer. Later, in
2008, the Saudi Ministry of Health established a
218
Shishah, W., AlJowesir, H., Subh, O. and Hassan, G.
The Design and Evaluation of a Home Health Care System (Teamvisit).
DOI: 10.5220/0010157502180224
In Proceedings of the 4th International Conference on Computer-Human Interaction Research and Applications (CHIRA 2020), pages 218-224
ISBN: 978-989-758-480-0
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

home health care program to provide health services
for all those in need, wherever they may be, to reduce
the pressure of hospital waiting times. The high
quality home health care service is provided to
international standards and according to Islamic
social values and traditions (Almoajel et al., 2016).
Different countries employ a variety of definitions
of home health care, but perhaps the most useful
definition is satisfying people’s health and medical
needs while in their home by providing appropriate
and high-quality home-based long-term or a short-
term health care (Genet et al., 2011).
Home health care grew at an annual average of
5.05% from 2007 to 2012 (Gitlin and Piersol, 2015).
As the population increased and technology evolved
there was a real need to develop new technologies in
home healthcare. In the early 1990s, telecare and
telemedicine were introduced for the first time.
Telecare is the use of technology, such as remote
monitoring, to manage risks for the elderly so they
can receive help at home and continue to live
independently. Telemedicine is the use of
telecommunications technology, either synchronous
or asynchronous, to remotely consult a doctor or
access medical advice. This service may provide
valuable help in the homecare sector (Lamine et al.,
2019; Lyons et al., 2019).
Many studies have outlined the advantages of
home health care. One study, (de Mestral et al., 2019),
looked at patients who received post-surgery home
nursing, including 23,617 patients, of whom 9,002
(38%) received home medical assistance within 30
days of discharge. Results showed that there was less
chance of an emergency department visit or hospital
readmission among patients who received home
health care services (Abyad, 2017; de Mestral et al.,
2019).
2.2 Usability of Health Care Systems
Reports of unusable systems suggest the issue of
health care system usability has become a global issue
affecting health care workflow and potentially
introducing new errors, particularly those
technologically induced (Kushniruk et al., 2013).
According to (Riskin et al., 2015; Kellermann and
Jones, 2013), a number of problems have been
reported relating to human-computer interaction,
poor usage, systems failing to meet intended users’
needs, terminologies, and workflow. Several attempts
have been made, in the past, to foster the development
of health care systems and an encouraging and
compulsory user-centered system that is more usable
does exist. Different methods have been adopted for
testing for usability and for assessing systems and
their impact on patients’ safety. However,
(Kellermann and Jones, 2013; Riskin et al., 2015)
argue that reports of poor system usability continue.
User interface design must be easy to understand
and intuitive in order to prevent usability issues,
especially when designing an interface for older
adults. A study was conducted in Taiwan by (Chen
and Liu, 2017) investigating the intuitive interaction
and affordance relationship with elderly users. It
concluded that, in terms of usability, designs with the
simplest layout are best for elderly users.
Consequently, complex and composite arrangements
and information presentations that require
imaginative association should be avoided in the user
interface (Chen and Liu, 2017).
When implementing new systems in the field of
home health care, caregivers must be trained to
understand how the new system works to support the
physical, mental, and medical needs of their patients,
and adequate training must be provided for elderly
patients for them to accept and adopt the new
technological system (Chase et al., 2009). The
appropriate awareness, full commitment, and the
correct application of user-centered processes and
tools are all necessary to ensure success in the process
of designing a usable interface (Dray, 1995).
3 METHODOLOGY
The research method adopted in this project is User
Centered Design (UCD). This method emphasizes
user involvement at each stage of the design process
and Kashfi (2010) recommends its application in
health contexts. The major focus of UCD is the end
users and the needs for which the system will be used.
The main goal of this method is to make systems
usable and to achieve user satisfaction. The key
characteristic of UCD is its iterative nature, in which
prototypes are delivered to users regularly for
evaluation and enhancement during the design and
development process.
According to McCurdie et al. (2012), the UCD
process begins with the concept generation stage, in
which, once users are identified, a comprehensive
examination of their needs is performed in order to
understand the use and purpose of the system.
Different techniques can be used in this phase such as
ethnography, focus groups, and one-on-one
interviews.
On completion of the initial investigation of user
needs, our project proceeded to the next phase, which
is to translate the identified user needs into a set of
The Design and Evaluation of a Home Health Care System (Teamvisit)
219

functional requirements by designing initial
prototypes as simple sketches and wireframes.
The prototypes are then used to collect user
comments and feedback, and to get an in depth
understanding of the main goal of the system. As our
design process continued, designs were evaluated and
reframed iteratively with users through the use of
walkthroughs and usability testing. User comments
and feedback were used to verify that the
representation of the system matched user
requirements.
During walkthroughs, a facilitator supported users
through the process of using the proposed design
(Kaye and Crowley, 2000). This helped users to think
aloud and provide feedback on the issues and
obstacles they faced with the suggested workflow.
For the usability tests, a representative user
worked independently in a controlled environment
through a set of scenarios representing typical usage
of the system, while at the same time thinking aloud,
as suggested by (Fu et al., 2002). The facilitator who
observed the study, recorded notes on the
participants’ behavior as well as their comments and
issues that arose, helping to detect any hidden
requirements and interface design errors. Section 4
will describe how the UCD will be conducted in our
work and which techniques will be used.
4 THE DESIGN AND
EVALUATION OF THE
TeamVisit SYSTEM
The TeamVisit system development team was
multidisciplinary, and included an interaction design
expert, who also served as domain expert, and three
University students with different backgrounds in
software engineering, programming, and user
interface design. However, other experts and users
were involved in different phases of the evaluation.
The design of the TeamVisit system was conducted
in three stages, as discussed below.
4.1 Stage 1: Identification of Intended
Users and Task
The development team conducted a focus group with
four users, two members of the home health care team
and two members of the hospital’s IT department.
Focus groups were selected as the most suitable
method of data collection as they allow a diversity of
views to be shared, developed, and discussed (Heary
and Hennessy, 2002). The focus group lasted for
approximately two hours. The aim of this stage was
to identify the intended users and the main tasks for
each type of user. The leader of the development
team, who had experience of developing systems and
in conducting focus groups, facilitated the group
session. The remaining research team members noted
comments and suggestions during the session. An
example of questions prepared to foster this focus
group included: explain the current satiation of work,
what are the responsibilities of each member of the
home health care team, what tools are currently used,
and are there any problems or issues?
Following the focus group, the development
team designed a low-fidelity prototype (Figure 1).
Then, the leader of the development team conducted
a one-on-one interview with the leader of the home
health care team. This interview was conducted in
order to come to an agreement about the main tasks
of the system using the low-fidelity prototype and to
elicit initial feedback for the system design. The
leader of the development team took notes that were
then taken into consideration in designing the next
prototype. The development team analyzed the
collected data and categorized the evidence.
Figure 1: Low-fidelity prototype in stage 1.
4.2 Stage 2: Confirming the Functional
Requirements and Workflow of the
Functions
The development team developed a mobile prototype
for this stage, as shown in (Figure 2). The team
examined the mobile prototype with two members of
the home health care team. Each participant examined
the features by navigating the mobile prototype and
providing feedback, comments, and notes. The
development team observed each participant and took
notes. The examination of the prototype lasted for
approximately two hours, its main goal being to test
the workflow of the system’s functions.
CHIRA 2020 - 4th International Conference on Computer-Human Interaction Research and Applications
220

Figure 2: The mobile prototype in stage 2.
4.3 Stage 3: Usability Testing of the
TeamVisit System
A responsive web application was developed (Figure
3) involving two sides: the patient and the caregiver.
This was selected in response to the requirement
identified in Stage 1 that the design of the system
should be compatible with different sizes of screen. A
responsive web application fits in any screen size,
runs on any device, and works with any operating
system. The web programming languages used were
HTML, CSS, and JavaScript for client-side scripting,
and PHP and MySQL for server-side scripting.
Testing is an important phase in software
development, and, for thoroughness, unit testing,
integration testing, and usability testing were applied.
During development, unit testing was conducted on a
daily basis for each feature to ensure that each
functionality performed as expected. After
completing development, the development team
carried out integration testing in order to verify that
all functions in the system produced the expected
results. Then, usability testing was carried out with
five participants from different backgrounds. Before
the study, the development team prepared eight test
cases to be examined (Table 3). Then, the leader
commenced the process by thanking the participants
for their participation and then explained the purposes
and aims of the research study. Participants were
asked to interact with the TeamVisit system to
perform the selected test cases. During the testing, the
leader conducted a think-aloud procedure by asking
users to verbalize their thoughts whilst performing the
tasks. The development team members observed each
participant and took notes.
Figure 3: Example of responsive web application. The left
image is the TeamVisit system on a mobile screen, the
image on the right is the TeamVisit system on a desktop
screen.
5 RESULTS AND DISCUSSION
The involvement of users in the early stages of the
design process supported developers in collecting
useful data for the TeamVisit system. This supports
the results of previous studies that highlight the
important role of the user in the design process (van
de Kar and Den Hengst, 2009).
The focus group conducted in Stage 1 identified
the direct users of TeamVisit and the main tasks. The
direct users for the system include:
Head of the home health care department at
KAMCJ, who authorizes team members to use the
system. (Moderator)
KAMCJ home health care team members whom
the moderator grants permission to log in.
(Caregiver)
Patients registered with the KAMCJ home health
care department and a relative who has knowledge
of the patient’s required data. (Patients)
The use case diagram shown in (Figure 4) shows
different ways in which users (patient, caregiver, and
moderator) can interact with the TeamVisit system
and what tasks they can perform.
Feedback from the interview was highlighted for
consideration in future design. For example, rather
than specifying the type of user (caregiver, patient) at
the login page, log in to the system should be by
national ID, for both the caregiver and the patient, so
the system can automatically recognize the type of
user and move on to the appropriate page. In addition,
the design of the system should be compatible with
different sizes of screen.
The Design and Evaluation of a Home Health Care System (Teamvisit)
221
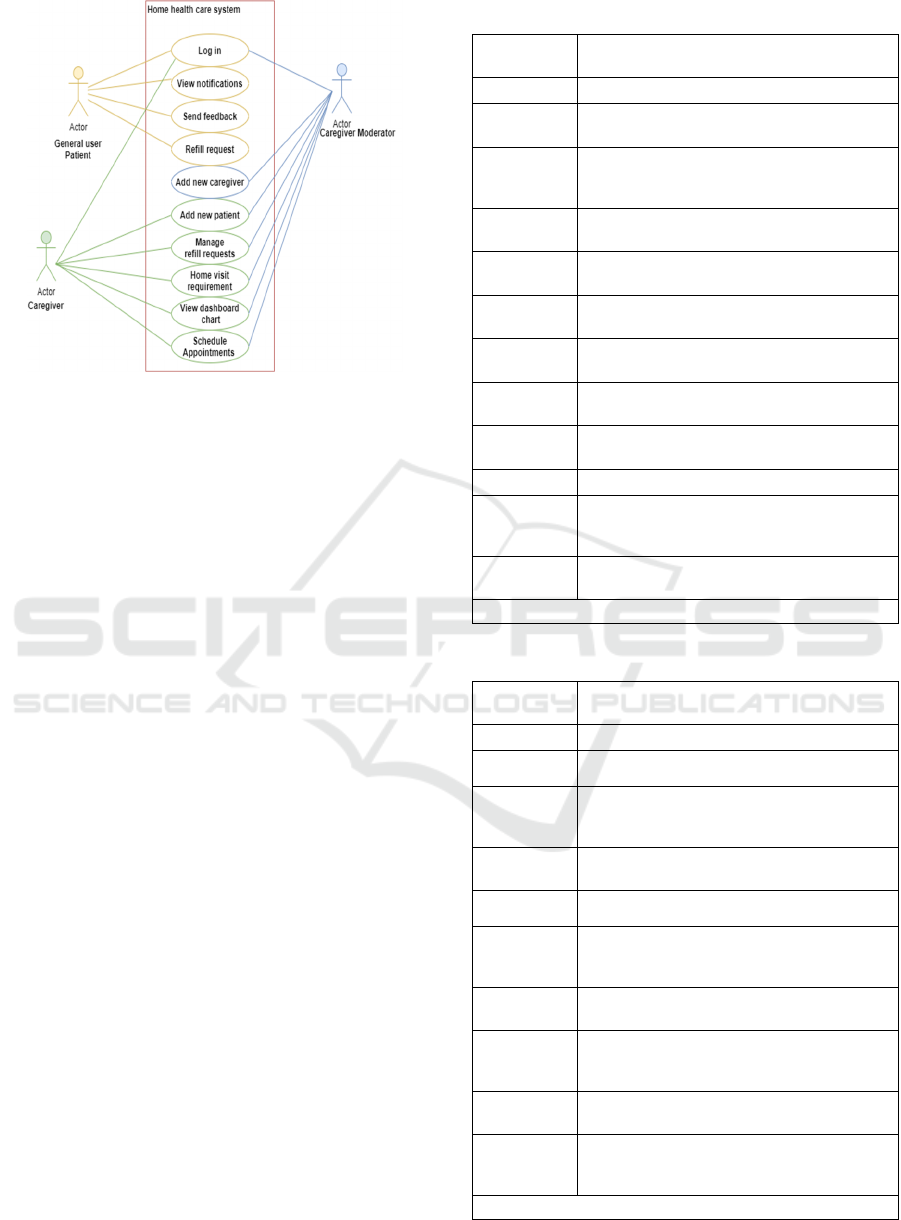
Figure 4: The use case diagram.
In Stage 2 of the TeamVisit design process, the
mobile prototype proved useful, as suggested in
previous studies (Kaye and Crowley, 2000), for
getting comments and feedback from users. In
general, the home health care team agreed with most
functions of the system and the functional workflow.
Further highlighted notes need to be considered in the
design. For example, in the current design (Figure 2),
appointment bookings can only be performed by the
patient. This needs to be changed so that the caregiver
can perform the task while the patient responds by
accepting or rescheduling. The reason for this is to
allow the home health care team to organize visits so
they can visit patients who live close to each other on
the same day. The main features for caregivers are
described in Table 1 and the main features for patients
are described in Table 2. Also, the priority status for
each feature was identified as (High, Medium and
low) which help the development team in the
implementation phase.
In Stage 3 of the design process, the results of the
usability testing were summarized (Table 3). Five
users participated in this study, following (Nielsen,
2000), suggestion that testing with five users results
in identifying the majority of usability problems. All
the 5 users performed both the caregiver and the
patient tasks. The expected time to complete the tasks
is 45-50 minutes and users completed the tasks in
acceptable duration time between 40 minutes to 1
hour. In general, users seemed satisfied with the
TeamVisit system and found it interesting to use.
However, there was some apprehension that needs to
be resolved in order to enhance the usability of the
system (Table 3).
Table 1: The main features for caregivers.
Feature
Feature description and the priority of
implementation
Log in Log in using National ID and password. (H)
Profile
view personal information and update contact
details and password. (H)
Add new
patient
Register patients using the required data such as
National ID, Medical Record Number (MRN),
name, age, gender, location (H)
Adds the order of medications, diet, and medical
supplements for each home health care patient
Manage refill
request
Manages patients’ requests by viewing,
accepting, editing, or rejecting. (H)
Books
appointment
Books appointments to visit patients in their
home. (H)
Visiting
requirements
Fills out the visiting requirements for
appointments (M)
Messages
Receives text or image messages from home
health care patients. (L)
Messages
status
Applies a status to messages received from
patients: read or unread. (L)
Charts Views dashboard charts. (M)
Search
Searches using a patient name and searches
appointments by date and status (accepted,
rejected, pending, completed). (H)
Add new
caregiver
(Moderator only) can Add/Delete caregiver
members. (H)
(H) = High priority / (M) = Medium priority / (L) = Low priority
Table 2: The main features for patients.
Feature
Feature description and the priority of
implementation
Log in Log in using National ID and password. (H)
Profile
view personal information and update contact
details and password. (H)
Notifications
users can be notified of scheduled appointments
and receive a response to their refill order
requests. (M)
Refilling
requests
Requesting to refill medications, diet
supplements, or medical needs. (H)
History
view the past five refill orders or appointments.
(M)
Responds to
requests
users can respond to appointment requests for
home visits arranged by the home health care
team. (H)
Shares
location
For each appointment, users can share their
current location. (M)
Messages
Users can send text messages as feedback or
comments to caregiver and upload images to
describe their health condition. (L)
Contact us
view contact details about home health care team
members. (L)
Satisfaction
rating
The patient can give a satisfaction rating for the
service provided (Excellent, Very good, Good,
Acceptable, Poor). (L)
(H) = High priority / (M) = Medium priority / (L) = Low priority
CHIRA 2020 - 4th International Conference on Computer-Human Interaction Research and Applications
222
Table 3: Summary results of the usability testing.
N
User
background
Task given
Time
Notes by development team members
Positive
feedback
Negative
feedback
Suggestion
1
Business
administrator
Test Case 1:
User login.
Test Case 2:
Adding a new
caregiver user.
Test Case 3:
Adding a new patient.
Test Case 4:
Caregiver manages
refill orders for
medication or diet
supplement.
Test Case 5:
Caregiver schedules
appointment for
patients.
Test Case 6:
Caregiver adds
appointment’s
requirement on the
visit day.
Test Case 7:
Patient orders refill.
Test Case 8:
Patient sends message.
45
minutes
Adding a patient
is really easy and
no difficulties
were faced.
Appointment status is
confusing.
None
2 Dentist
50
minutes
The interface and
main functions
are easy to use
even though there
are many
scenarios.
None
The refill
feature is
limited (e.g. no
information
about dose).
3 Nurse 1hour
Managing
appointments is
smooth using the
search by date
and status.
None
Patient history
is limited.
4 IT student
40
minutes
The whole
system looks
good.
Some interface icons
(such as the mail icon
in the login page) does
not give the right user
impression.
None
5 Teacher 1 hour
Requesting a
medication refill
is clear.
Sending messages
without receiving a
reply is not really
useful.
None
6 CONCLUSION AND FUTURE
WORK
This paper describes the design stages of a proposed
system for the home health care department in
KAMCJ called “TeamVisit,” which aims to provide
automated services and enhance communication
between patients and the home health care team.
Users were involved at point in the design process and
initial usability testing was conducted.
Using the UCD method, users were involved in
each stage of the design in order to get appropriate
data. In Stage 1 of the design process, a focus group
and interview were used to collect data about the
intended users and their main tasks. Next, in Stage 2
of the process, a mobile prototype was used to
confirm the requirements of the TeamVisit system.
Finally, initial usability testing was conducted, which
found that users were satisfied with the TeamVisit
system and found it interesting to use.
For further research or future work, more usability
testing should be performed using other techniques in
order to gather more useful information. Also, a field
study may be conducted to gather data in a natural
setting; this can be performed by observing users
while they interact with the TeamVisit system.
Furthermore, tests could be conducted with a larger
sample of users in order to carry out quantitative
analysis of usability problems.
Further features were recommended for
development in order to enhance the performance of
the system, some of which are highlighted below:
• patient appointment booking, to give them more
flexibility;
• live direct messages with a doctor so patients
can describe their medical condition and get
immediate medical advice; a video call feature
would further improve medical consultation;
• an upgrade of the responsive web application to
a native mobile application would provide many
advantages;
• car tracking of the team member due to visit the
patient at home;
• report generation such as number of patients
served in each location, downloaded in pdf
format.
The Design and Evaluation of a Home Health Care System (Teamvisit)
223

ACKNOWLEDGEMENTS
Many thanks to all participants of this project and
special thanks to Dr. Khalid Alabbasi at King
Abdullah Medical Complex in Jeddah (KAMCJ).
REFERENCES
Abyad, A. (2017). The Future Home Health Care in the
Middle East Region. Part I: International Perspective.
Middle East Journal of Nursing, 101(4098), 1-11.
Almoajel, A., Al-Salem, A., Al-Ghunaim, L., & Al-Amri,
S. (2016). The Quality Of Home Healthcare Service In
Riyadh/Saudi Arabia. Asian Journal of Natural &
Applied Sciences Vol, 5, 2.
Chase, J.-A. D., Russell, D., Rice, M., Abbott, C., Bowles,
K. H., & Mehr, D. R. (2009). Caregivers’ Experiences
Regarding Training and Support in the Post-Acute
Home Health-Care Setting. Journal of Patient
Experience, 2374373519869156.
Chen, L.-H., & Liu, Y.-C. (2017). Affordance and intuitive
interface design for elder users with dementia. Procedia
CIRP, 60, 470-475.
de Mestral, C., Kayssi, A., Al-Omran, M., Salata, K.,
Hussain, M. A., & Roche-Nagle, G. (2019). Home care
nursing after elective vascular surgery: an opportunity
to reduce emergency department visits and hospital
readmission. BMJ quality & safety, 28(11), 901-907.
Dray, S. (1995). The importance of designing usable
systems. interactions, 2(1), 17-20.
Fu, L., Salvendy, G., & Turley, L. (2002). Effectiveness of
user testing and heuristic evaluation as a function of
performance classification. Behaviour & information
technology, 21(2), 137-143.
Genet, N., Boerma, W. G., Kringos, D. S., Bouman, A.,
Francke, A. L., Fagerström, C., . . . Devillé, W. (2011).
Home care in Europe: a systematic literature review.
BMC health services research, 11(1), 207.
Gitlin, L. N., & Piersol, C. V. (2015). Home: An evolving
context for health care. In Occupational therapy with
aging adults: Promoting quality of life through
collaborative practice (pp. 423-427): Elsevier Inc.
Heary, C. M., & Hennessy, E. (2002). The use of focus
group interviews in pediatric health care research.
Journal of pediatric psychology, 27(1), 47-57.
Kashfi, H. (2010). Applying a user centered design
methodology in a clinical context. Paper presented at
the MedInfo.
Kaye, R., & Crowley, J. (2000). Guidance for Industry and
FDA Premarket and Design Control Reviewers:
Medical Device Use-Safety: Incorporating Human
Factors Engineering into Risk Management. Food and
Drug Administration, Center for Devices and
Radiological Health, Division of Device User
Programs and Systems Analysis, Office of Health and
Industry Programs, Washington, DC, 33.
Kellermann, A. L., & Jones, S. S. (2013). What it will take
to achieve the as-yet-unfulfilled promises of health
information technology. Health affairs, 32(1), 63-68.
Kushniruk, A., Nohr, C., Jensen, S., & Borycki, E. (2013).
From usability testing to clinical simulations: Bringing
context into the design and evaluation of usable and
safe health information technologies. Yearbook of
medical informatics, 22(01), 78-85.
Lamine, E., Bastide, R., Bouet, M., Gaborit, P., Gourc, D.,
Marmier, F., Toumani, F. (2019). Plas' O'Soins: An
Interactive ICT Platform to Support Care Planning and
Coordination within Home-Based Care. IRBM, 40(1),
25-37.
Lyons, J. P., Watson, K., & Massacci, A. (2019). The
Evolution of Elderly Telehealth and Health Informatics.
In Health Technology and Informatics-Technology in
Primary and Advanced Healthcare: IntechOpen.
McCurdie, T., Taneva, S., Casselman, M., Yeung, M.,
McDaniel, C., Ho, W., & Cafazzo, J. (2012). mHealth
consumer apps: the case for user-centered design.
Biomedical instrumentation & technology, 46(s2), 49-
56.
Nielsen, J. (2000). Why you only need to test with 5 users.
In: Useit. com Alertbox.
Organization, W. H. (2018). Continuity and Coordination
of Care: World Health Organization. Regional Office
for Europe.
Riskin, L., Koppel, R., & Riskin, D. (2015). Re-examining
health IT policy: what will it take to derive value from
our investment? Journal of the American Medical
Informatics Association, 22(2), 459-464.
van de Kar, E., & Den Hengst, M. (2009). Involving users
early on in the design process: closing the gap between
mobile information services and their users. Electronic
Markets, 19(1), 31-42.
CHIRA 2020 - 4th International Conference on Computer-Human Interaction Research and Applications
224
