
Computer Spirometry: Research of Respiratory System Functionality
and Its Enhancement in Young Swimmers
Anna Zakharova
a
, Alexey Gorelov
b
and Tatiana Miasnikova
c
Institute of Physical Education, Sport and Youth Policy, Ural Federal University named after the first President of Russia
B.N. Yeltsin, Mira Street, Ekaterinburg, Russia
Keywords: Respiratory System, Spirometry, Vital Capacity, Forced Vital Capacity, Swimmers, Respiratory Muscle
Training.
Abstract: The control of the swimmers' fitness should include an assessment the respiratory system. The aim of the
study to evaluate the age features of respiratory system in young swimmers and suggest the methods for
respiratory system improvement. Methods: young athletes underwent two tests with MicroLab spirometry;
relaxed and forced vital capacity measurement. Findings: (i) young swimmers 10-11 years old with at least 5
years of experience in swimming showed low spirometry indicators (85% of predicted value); (ii) the more
experienced and successful swimmers the better their respiratory system developed. High-performance sport
swimmers have high level (120 % of predicted value) of all spirometry indicators; (iii) breathing exercises
selected for solving the respiratory problems in swimmers improve the respiratory muscles functionality.
1 INTRODUCTION
Respiratory system is one of the essential factor
providing general endurance in sport (Sheel, 2010).
Competitive swimming is challenging to human
pulmonary system as (i) whole body muscles are
required for propulsion through water thus O
2
intake
should be high; (ii) swimmer’s face is submerged in
water; (iii) breathing is constrained by swimming
technique, that is stroke cycles, etc. Moreover, in
normal (dry land) breathing, only inhalation is active,
and exhalation occurs passively, due to the relaxation
of the muscles that provide inhalation. In water,
exhalation should be forced, with the participation of
the muscles that produce exhalation.
Breathing in swimmers was under consideration
in a number of articles (Vašíčková, 2017, Bovard,
2018, Rosser-Stanford, 2019). It was reported that
functional readiness of athletes-swimmers was
largely determined by functional mobilization of
physiological systems, namely of respiratory and
circulatory systems’ functionality.
Respiratory muscles dysfunction manifests itself
in a decrease in their functional properties - strength
a
https://orcid.org/0000-0002-8170-2316
b
https://orcid.org/0000-0002-9550-1793
c
https://orcid.org/0000-0002-0894-1337
(the ability to develop maximum effort) and/or
endurance (the ability to continuously maintain
submaximal efforts). is expressed in the development
of their fatigue or weakness (Segizbaeva, 2019). An
important result of numerous studies in recent years
is the physiological substantiation of the possibility of
training the respiratory muscles in order to increase
their strength and endurance, as well as increase the
overall physical performance of healthy subjects
(Segizbaeva, 2019) and athletes (Vašíčková, 2017).
The purpose of the study was twofold – to
evaluate the age features of respiratory system in
young swimmers and suggest the methods for
respiratory system improvement in young swimmers.
2 METHODS
The study was conducted in the laboratory
“Functional Testing and Complex Control in Sports”
of the Institute of Physical Education, Sports and
Youth Policy, Ural Federal University
(Yekaterinburg, Russia).
228
Zakharova, A., Gorelov, A. and Miasnikova, T.
Computer Spirometry: Research of Respiratory System Functionality and Its Enhancement in Young Swimmers.
DOI: 10.5220/0010147302280233
In Proceedings of the 8th International Conference on Sport Sciences Research and Technology Support (icSPORTS 2020), pages 228-233
ISBN: 978-989-758-481-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
The investigation conforms to the principles of the
Declaration of Helsinki of the World Medical
Association. Subjects involved in the study and their
parents had been provided with comprehensive
information on the procedures, methods, benefits and
possible risks before their written consent was
obtained. The study protocol was approved by the
Ural Federal University Ethics Committee (#05-
2020).
To evaluate respiratory system correctly it is
obligatory to determine the anthropometric
measurements as the lungs volume and their
functionality depend upon the patient physical
development (that is height and weight).
2.1 Anthropometry
The height was measured with height meter in
vertical position without shoes. Weighting was done
with Mi Body Composition Scale (Xiaomi, China).
2.2 MICROLAB™ Spirometry
The portable spirometer MicroLab (Care Fusion,
USA) was used to measure respiratory volumes and
functions. The device is an essential spirometer in
today's healthcare professional. Vyaire's Gold
Standard Turbine measurement technology is
certified by the American Thoracic Society (ATS),
the internationally recognized body for spirometry
performance. MicroLab spirometer is provided with
Spirometry PC Software program to calculate the
expiratory and inspiratory indices, taking into account
age, gender, weight and height. There is a built-in
strip printer which prints out the individual report
after spirometry testing.
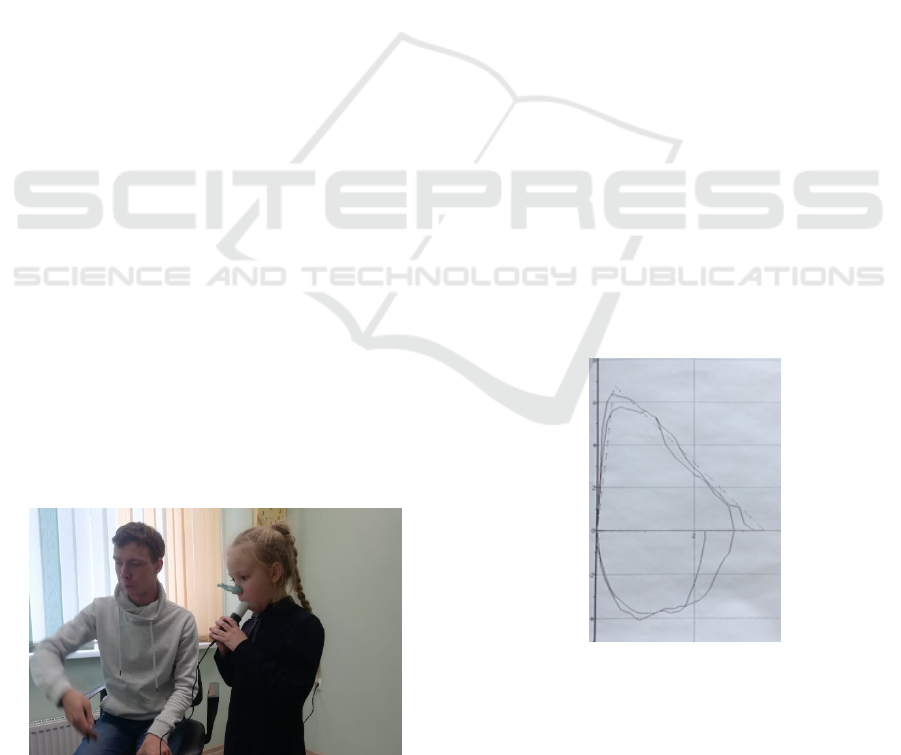
A nose-clip was used for accuracy of measured
spirometry data (Figure 1) and the disposable
mouthpieces Ø28 mm were used for the patients’
safety.
Figure 1: Spirometry test procedure.
Before running the spirometry tests it was
necessary to enter a patient’s details (identity, sex,
date of birth, height, weight).
Two tests were conducted: relaxed vital capacity
measurement prior to performing a forced vital
capacity manoeuvre.
2.2.1 Relaxed Vital Capacity Measurement
For relaxed vital capacity (VC) testing the patient was
instructed to breathe in until their lungs are
completely full, to seal the lips around the mouthpiece
and to blow out at a comfortable rate until he (she)
cannot push out any more air.
Three attempts were allowed.
2.2.2 Forced Vital Capacity Measurement
A Forced vital capacity test was conducted three
minutes later after completion of a Relaxed VC test.
The patient was instructed to breathe in as in the
previous test ̶ until the lungs were completely full,
seal their lips around the mouthpiece and blow out as
hard and as fast as possible until he (she) cannot push
any more air out, then breathe in immediately after
the expiratory manoeuvre and repeat this cycle
(inspiration-expiration) three times without stop.
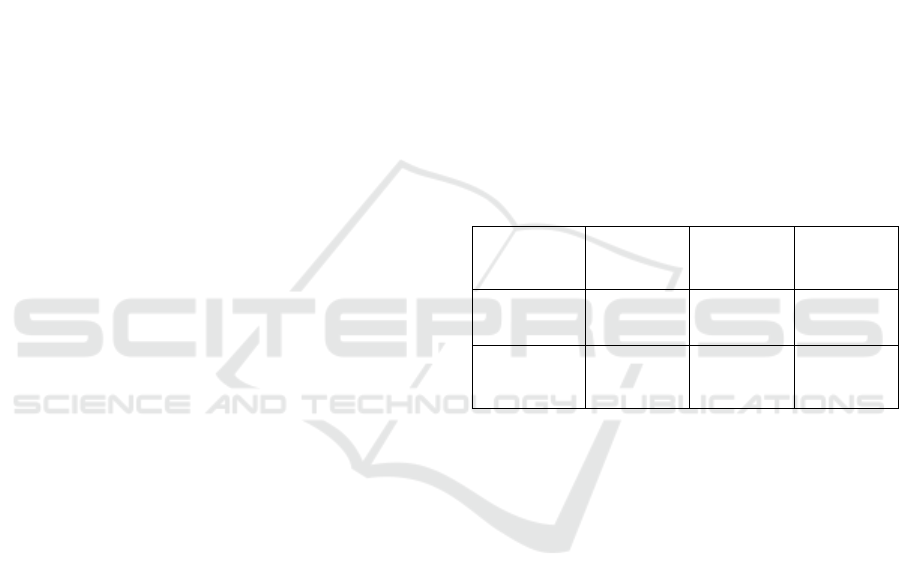
As the patient details had been entered before the
first test the spirometry screen displayed the predicted
Flow/Volume curve as a dashed line. During the test
the patient is looking after his Flow/Volume curve
and predicted one (dashed line) and try to enhance the
breathing performance to achieve the breathing
pattern (Figure 2).
Figure 2: The Flow/Volume loop.
2.2.3 Spirometry Test Results
After the completion of both tests Spirometry PC
Software fulfills manoeuvre quality check to allow a
decision to be made to accept or reject these blows.
There are four quality checks performed on each
Computer Spirometry: Research of Respiratory System Functionality and Its Enhancement in Young Swimmers
229
spirometry manoeuvre to determine its acceptability.
If the patient performs an acceptable manoeuvre
‘Good blow’ is displayed at the top of the screen.
Automatically or manually the ‘best’ blows for the
report are selected (MicroLab Operating Manual,
2004).
The MicroLab Spirometer report includes (i)
respiratory performance and (ii) a graphic depiction
of the breathing loop and (iii) the contours of the
proper breathing loop based on the patient's height,
weight and age.
Following indicators were under consideration:
vital capacity (VC, l), forced vital capacity (FVC, l)
and forced expiratory volume in the first second
(FEV1) as well as the percentage of the predicted
values along with the Flow/Volume loop.
The testing procedures were explained to each
participant and informed consent was obtained in
accordance with the Declaration of Helsinki of the
World Medical Association.
2.3 Statistics
Statistical analysis was performed with the use of
statistic software package “SPSS Statistics 17.0”
(IBM). The descriptive analysis of the obtained data
was applied. Normality of distribution was assessed
by the Shapiro-Wilk test. Mean value (M) and
standard deviation (SD) of the measured parameters
were calculated. The level of significance was set at
P < 0.05.
2.4 Subjects
In October 2019 in the sport scientific laboratory of
the Ural Federal University stage control including
spirometry was carried out for the group of swimmers
(6 boys and 5 girls) 10-11 years old (height 148.9 ±
9.12 cm, weight 38.8 ± 7.87 kg). These athletes have
been engaged in sports swimming for at least 5 years
and had I youth and III sport category in swimming
In Russia there is a system of sport categories
according to competition results: to achieve I youth
category and III sport category in swimming one must
cover the distance of 200 m for boys 3:08.0 and 2:42.5
and for girls 3:29.0 and 2:58.0 in crawl swimming
respectively.
To reveal the level of respiratory system
development in other athletes spirometry tests were
carried out with a group of 12 young professional
hockey players of 9 years old (height 135.75 ± 4.69
cm, weight 34.3 ± 2.22 kg) and 10 amateur hockey
players 10–11 years old (height 143.33 ± 4.46 cm,
weight 35.7 ± 5.92kg), engaged in the outdoors
training all year round.
For comparison “young athletes vs a group of
classmates” 28 pupils of one form (18 boys and 10
girls) aged 9-10 years (height 138.9 ± 7cm, weight 32
± 6.32kg) were studied with spirometry (Zakharova,
2020).
3 RESULTS
Analysing the spirometry indicators of the respiratory
system in a group of swimmers aged 10-11 (Table 1),
we found that only 2 swimmers or 18% of the studied
subjects showed a normal VC with a proper
individual indicator above 100%, 2 swimmers (18%)
were within the norm of 95-100%, 27% (3 swimmers)
had the result below normal (80–95% of VC) and
36% or 4 swimmers had extremely low VC.
Table 1: Pulmonary system function indicators of
swimmers’ group 10-11 years old (М±m (min-max)).
Indicator
Vital
capacity
Forced
Vital
Capacity
FEV1
Absolute
measure, l
2.50±0.58
(1.51-2.9)
2.41±0.58
(1.37-3.3)
2.03±0.40
(1.36-2.7)
Percentage
of proper
value, %
86.2±15.3
(60-111)
85.2±16.7
(55-108)
85.6±12.9
(65-109)
One swimmer coped with the FVC test as he had
only excellent indicators (above 100%) of the FVC
test (VC, FVC and FEV1) and 27% (3 swimmers)
were within normal FVC.
7 swimmers showed an FVC indicator below
normal: 4 swimmers demonstrated 80-95% of
predicted FVC and 3 swimmers had poor FVC, that
is, below 80% of predicted FVC).
Taking into account that, first, predicted by
Spirometry PC Software values of respiratory system
intend for healthy children but not for athletes
specially and, second, larger lungs are necessary for
competitive swimming, we conclude that young
swimmers with more than 5 years of sport swimming
experience showed poor results in spirometry tests.
So we came to the idea to check the spirometry in
other young athletes and non-athletes of the same age.
Ice hockey players (n=12) training in modern
indoor ice palaces demonstrated satisfactory
spirometry data (table 2).
icSPORTS 2020 - 8th International Conference on Sport Sciences Research and Technology Support
230
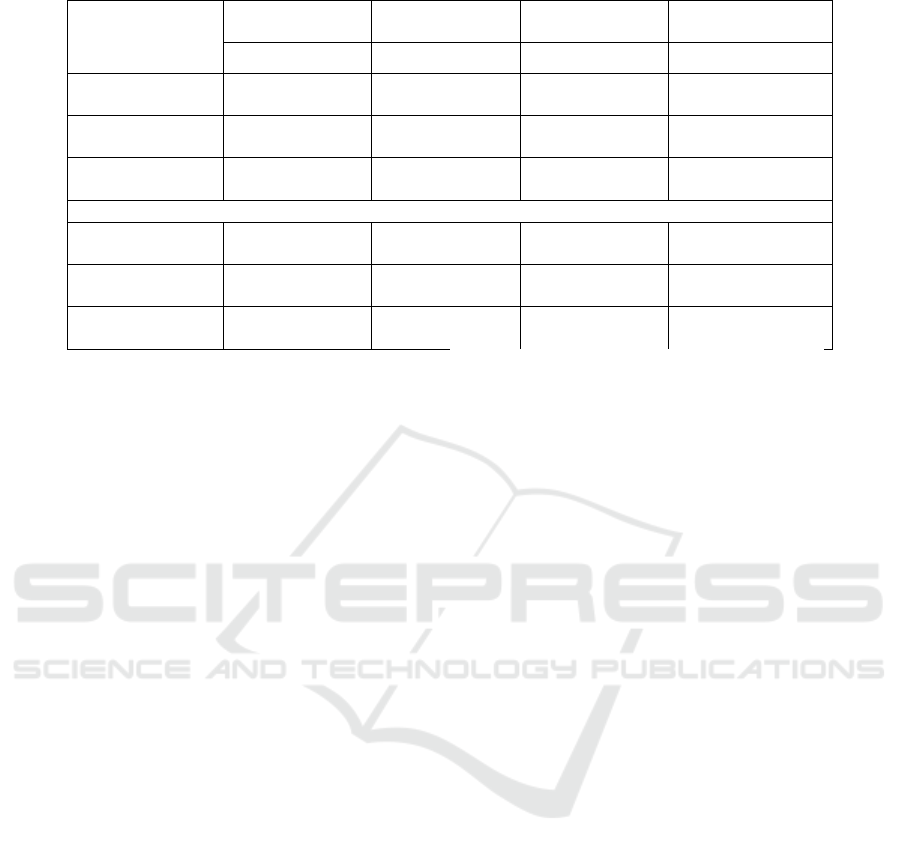
Table 2: Spirometry indicators of different groups of children 9-11 years old (М±m (min-max)).
Indicators
Ice hockey
Outdoor amateur
ice hockey
Swimming Pupils of one class
9 years old 10-11 years old 10-11 years old 9-10 years old
VC, l
2.35±0.3
(1.88-2.51)
2.53±0.15
(2.36-2.75)
2.50±0.58
(1.51-2.92)
2.11±0.36
(1.45-3.12)
FVC, l
2.32±0.26
(1.98-2.55)
2.57±0.24
(2.28-2.95)
2.41±0.58
(1.37-3.33)
2.10±0.36
(1.38-3.16)
FEV1, l
2.13±0.19
(1.93-2.40)
2.24±0.28
(1.82-2.59)
2.03±0.40
(1.36-2.77)
1.87±0.26
(1.35-2.56)
Percentage of predicted value
VC, %
97.3±16.8
(72-106)
98±4.65
(93-105)
86.2±15.3
(60-111)
89.7±11.2
(64-112)
FVC, %
98.5±17.1
(78-110)
101.8±6.27
(94-112)
85.2±16.7
(55-108)
89.9±10.4
(74-110)
FEV1, %
108±17.06
(91-128)
105.5±6.69
(99-117)
85.6±12.9
(65-109)
97.3±7.9
(85-114)
VC- vital capacity, FVC- forced vital capacity and FEV1 - forced expiratory volume in the first second
Amateur hockey players (n=10), training outdoors
all year round had even better results in relative
values than young professional hockey players.
Group of 11 athletes-swimmers and ordinary
pupils from one class both have the spirometry data
statistically not distinguished.
So all average spirometry indicators (VC, FVC
and FEV1) in swimmers (Table 2) were lower than
necessary for healthy children. We found that
swimmers 10-11 years old with at least 5 years of
experience have an insufficiently developed
respiratory system, that is, they cannot breathe
correctly and use the respiratory muscles effectively.
These spirometry results were unexpected both
for us and for the coach. What is the reason of such a
backlog in the respiratory muscles functionality?
In conversation with the swimming coach it was
revealed that the motor tasks for breathing were used
in training of studied swimmers: under water
swimming without breath, swimming with one intake
of breath for three- four strokes, etc. These exercises
adapt the swimmers for swimming in lack of
breathing but do not improve the breathing pattern.
So we can’t consider these exercises as respiratory
muscle training. Moreover, speed swimming with
high frequency of strokes suppress the normal
breathing.
It was reported that swimming training did not
enlarge the lungs in children (Bovard, 2018). To
reveal the level of the respiratory system development
in swimmers of different sport categories we carried
out the spirometry research with young swimmers
(n=10) aged 11-12 years old (height 149.2±8.78 cm,
weight 37.9±7.59kg), more experienced swimmers
(n=5) 15-18 years old (height 184.4±4.4 cm, weight
77± 4.2 kg) and high performance sport swimmers
(n=4) 20-23 years old (height 187.5±3.5cm, weight
84.5±2.1kg) and used the earlier obtained data of
studied swimmers aged 10-11 (Table 3).
The spirometry results of swimmers (Table 3)
prove that the more experienced and successful
swimmers the better their respiratory system
developed. High-performance sport swimmers have
high level (120 % predicted value) of all spirometry
indicators.
It is not clear: the large lungs of swimmers is the
result of intensive training or swimmers with low
respiratory functions give up competitive sport. But
our next task was to help the young swimmers with
low respiratory functions to improve them.
From the above mentioned spirometry results and
swimmers’ Flow/Volume loops with insufficient
strength of expiration muscles and short breathing
cycle (Figure 3) we stated following respiratory
problems in swimmers:
Low vital capacity;
Low FEV1 id est power of expiratory muscles;
Insufficient (short) expiration;
Weak inhale.
FEV1 is associated with the power of expiratory
muscles as the power is defined as the ability to
produce large force in a limited period of time with
high rates of force development. So the value of
Forced Expired Volume in the first second may be
high only in case of good strength and what is more
important of good ability to produce high expiration
in short time.
Computer Spirometry: Research of Respiratory System Functionality and Its Enhancement in Young Swimmers
231
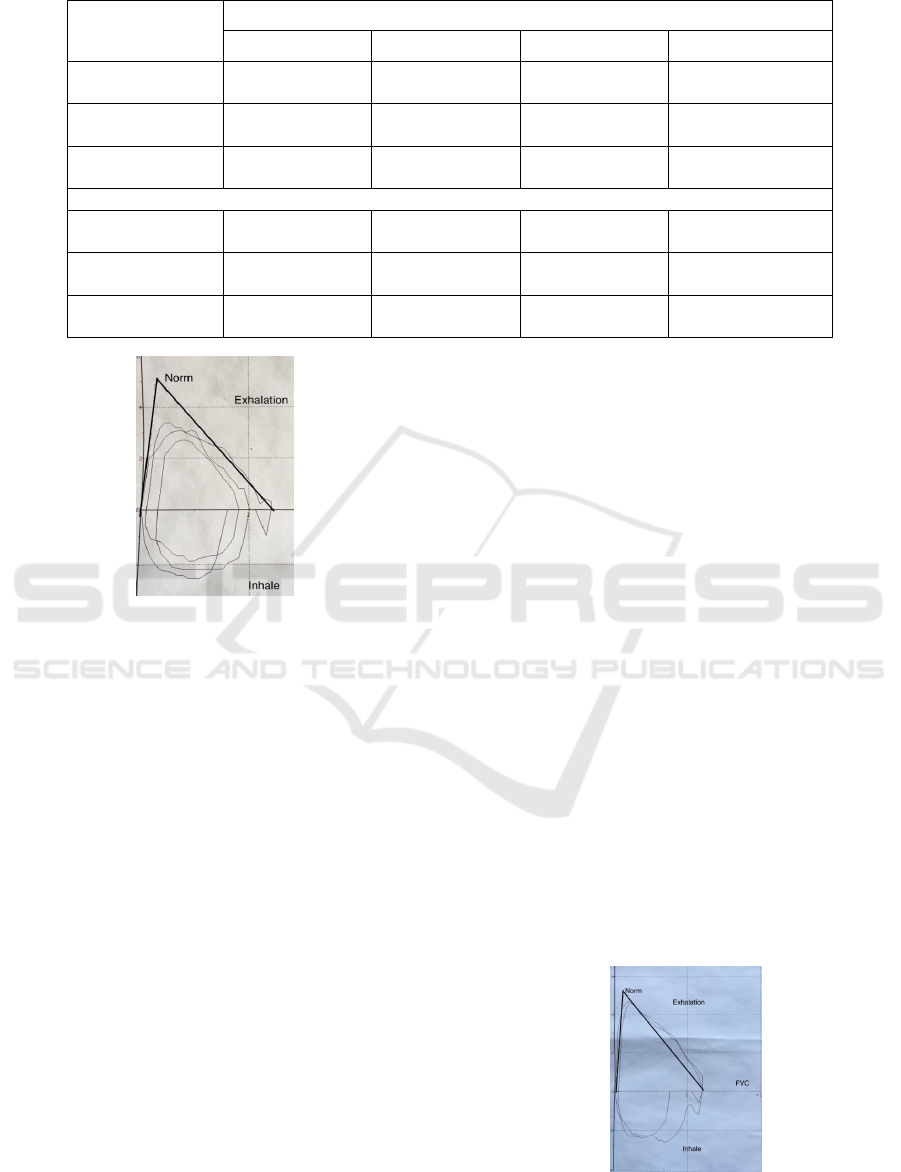
Table 3: Spirometry indicators of swimmers of different sport qualification (М±m (min-max)).
Spirometry
indicators
Age
10-11 years old 11-12 years old 15-18 years old 20-23 years old
VC, l
2.50±0.50
(1.51-3.28)
2.74±0.47
(2.09-3.28)
5.99 ± 1.7
(4.18-7.59)
7.42±0.1
(7.35-7.49)
FVC, l
2.41±0.58
(1.37-3.337)
2.72±0.51
2.07-3.33
5.63±1.5
(3.96-6.82)
7.12±0.06
(7.07-7.16)
FEV1, l
2.03±0.40
(1.36-2.77)
2.51±0.46
(1.84-3.32)
4.85±1.1
(3.75-5.96)
5.62±0.19
(5.48-5.75)
Percentage of predicted value
VC, %
86.2±15.3
(60-111)
96.1±13.16
(70-115)
117.3±9.7
(109-135)
120±4.24
(117-123)
FVC, %
85.2±16.7
(55-108)
97.7±12.18
(80-120)
117.3±9.7
(109-128)
120±4.24
(117-123)
FEV1, %
85.6±12.9
(65-109)
107.2±9.70
(93-120)
114±5.6
109-120
120.5±7.78
(115-126)
Figure 3: The Flow/Volume loop of the swimmer#1.
Short expiration may have place in two cases: low
strength or endurance of expiratory muscles.
For each respiratory problem the exercises were
selected:
1) to increase VC, it is necessary to ensure
correct posture, chest mobility with stretching and
bending, and elasticity of the muscles responsible for
the function of breathing, especially the diaphragm;
2) for the development of the expiratory
muscles power - blowing out the candles, blowing off
the ball rolled from A4 paper sheet and explosive
exhalations through a swimming tube dipped in
water.
or the development of the duration of
exhalation;
3) for longer expiration ̶ blowing off a paper ball
folded from a napkin; play "tennis" blowing a paper
ball in pairs, blowing out 5–10 candles placed in a
row at a distance of 5–10 cm from each other, etc;
4) for developing the strength of inspiration –
swimming with a tube with a clamp restricting the
flow of air.
We considered these exercises would help young
swimmers to learn how to breathe correctly.
The experiment for respiratory system
improvement via exercises was organized. Initial
spirometry testing were held in October 2019 with the
group of swimmers 10-11 years old. The coaching
part of the experiment included:
• Conversation with the trainer based on the test
results;
• Conducting theoretical and practical classes on
respiratory system exercises with the swimmers;
• Informing parents about the importance of
breathing exercises for encouraging the swimmers to
fulfil the exercises at home;
• Performing breathing exercises during the
period from December 1, 2019 to February 16, 2020,
at home (daily) and in training (5 times a week).
Due to the outbreak of acute respiratory none in
January-February 2020 only 4 swimmers were able to
take part in post-experiment spirometry. Comparing
the results of spirometry indicators before and after
experiment in four swimmers, we found
improvements in the functioning of the respiratory
system for each indicator (Table 4). In swimmer # 1
after the experiment we found an increase in the FVC,
FEV1 and his Flow/Volume loop was normalized
(Figure 4) in comparison with his primary spirometry
(Figure 3).
Figure 4: Post- experiment Flow/Volume loops of swimmer
#1.
icSPORTS 2020 - 8th International Conference on Sport Sciences Research and Technology Support
232
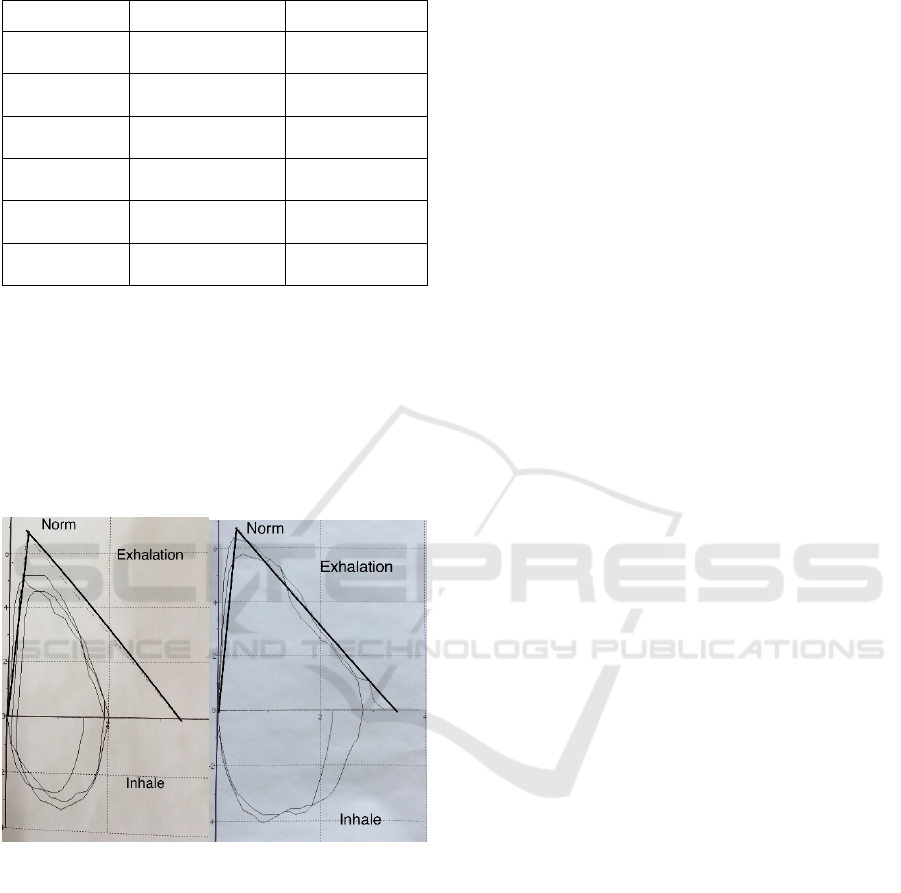
Table 4: Spirometry indicators of young swimmers before
and after experiment (М±m (min-max)).
Indicators Pre- Post-
VC, l
2.15± 0.58
(1.51-2.92)
2.59 ±0.39
(2.32-3.16)
FVC, l
2.05±0.24
(1.81-2.38)
2.46 ±0.48
(2.1-3.14)
FEV1, l
1.91±0.18
(1.64-2.05)
2.21 ±0.6
(1.7-2.93)
VC, %
80.7±15.6
(60-97)
97.2 ±4.79
(92-103)
FVC, %
81.5±18.8
(59-98)
94.2 ±5.3
(88-100)
FEV1, %
89.7±17.7
(71-109)
99.5 ±11.7
(89-114)
In swimmer #2 at the first testing the following
problems were identified: weak inhalation, weak
exhalation and its duration (Figure 5a). After the
experiment there was an improvement in the depth of
inhalation, the peak of exhalation and the duration of
exhalation as well as in FVC (Figure 5b). Thus we
can conclude that breathing exercises helped the
swimmer#2 to improve his respiratory muscles
functionality: enhance their strength and workability.
a b
Figure 5: Pre- and post- experiment Flow/Volume loops of
swimmer #2.
Although the results of the experiment reveal no
statistically significant differences (Table 4) but
qualitative information from the Flow/Volume Loops
(Figures 4 and 5) proves that experiment was
successful.
Thus breathing exercises selected according to
respiratory system problems revealed with the help of
MicroLab spirometry are effective for young
swimmers.
4 CONCLUSIONS
1. Competitive swimming does not develop
respiratory system in young swimmers.
2. The level of respiratory functionality of
swimmers must be under supervision with the help of
computer spirometry.
3. Swimmers’ breathing requires special training
including exercises for lungs enlargement,
development of power and endurance of expiratory
muscles as well as strength of inspiratory muscles.
ACKNOWLEDGEMENTS
The work was supported by Act 211 Government of
the Russian Federation, contract № 02.A03.21.0006.
REFERENCES
Bovard, J. M., Welch, J. F., Houghton, K. M., McKenzie,
D. C., Potts, J. E., & Sheel, A. W., 2018. Does
competitive swimming affect lung growth?. In
Physiological reports, 6(15), e13816. https://doi.org/
10.14814/phy2.13816
MicroLab Operating Manual 069-12 Revision 1.4 August
2004. Micro Medical Limited, 2004. Micro Medical
Ltd., PO Box 6, Rochester, Kent ME1 2AZ ENGLAND
www.micromedical.co.uk
Rosser-Stanford, B., Backx, K., Lord, R., & Williams, E.
M., 2019. Static and Dynamic Lung Volumes in
Swimmers and Their Ventilatory Response to Maximal
Exercise. In Lung, 197(1), 15–19.
Segizbaeva M. O., & Aleksandrova N. P., 2019.
Assessment of the Functional state of Respiratory
Muscles: Methodical Aspects and Data Interpretation.
In Human Physiology, 45(2), 213–224.
Sheel, A. W., MacNutt, M. J., & Querido, J. S., 2010. The
pulmonary system during exercise in hypoxia and the
cold. In Experimental physiology, 95(3), 422–430.
https://doi.org/10.1113/expphysiol.2009.047571
Vašíčková, J., Neumannová, K., & Svozil, Z., 2017. The
Effect of Respiratory Muscle Training on Fin-
Swimmers' Performance. In Journal of sports science
& medicine, 16(4), 521–526.
Zakharova, A. V., Gorelov, A. N., Makarov D., Nikitina J.
G., 2020. Role of physical culture and sports in the
development of the respiratory system at children aged
9-10 years old (on the example of one class). In J
Uchenye zapiski universiteta imeni P.F. Lesgafta,
5(183), 169-174.
Computer Spirometry: Research of Respiratory System Functionality and Its Enhancement in Young Swimmers
233
