
Does Prior Hamstring Strain Injury Affect Hamstring Muscle
Activation Patterns in Amateur Football Players? A Feasibility Study
Ahmed Ahmed
Queen Mary University of London, Mile End Road, Bethnal Green, London, E1 4NS, U.K.
Keywords: Hamstring, Activation, Injury, Football, EMG.
Abstract: Hamstring stains are very common injuries among athletes. Re-injury rate for hamstring strains is high and
factors effecting hamstring re-injury is a research topic of interest. The aim of this study was to determine if
there is a relationship between prior hamstring strain injury and medial:lateral (M:L) hamstring activation
ratio in amateur football players during normal gait. Six male amateur football players with a history of
unilateral hamstring strain injury volunteered for participation in this study. EMG data from the
semitendinosus and biceps femoris muscles was recorded across a full gait cycle. The results of this
preliminary, feasibility study show no significant difference between mean M:L hamstring activation ratios
in previously injured hamstrings (Mean (M)=2.54, Standard Deviation (SD)=1.56) and uninjured contralateral
hamstrings (M=3.06, SD=2.86) across the full gait cycle; t(10) = 0.73, p>0.05. Mean M:L activation ratios
during ‘Stance phase’ show no significant difference between case and control hamstrings; t(10)=0.88,
p>0.05. During ‘Swing phase’ there is no significant difference in mean M:L activation ratios between
previously injured and uninjured hamstrings; t(10)=0.61, p>0.05.
1 INTRODUCTION
Acute hamstring strains are the most common form
of injury in professional soccer players, making up
12% of all injuries (Ekstrand et al., 2009).
Biomechanical analysis of running suggests that the
injury occurs during terminal swing phase of the gait
cycle (Chumanov et al., 2007). The hamstrings must
change from contracting eccentrically to decelerate
knee extension, to contracting concentrically acting
as an active hip extensor (Thelen et al., 2005). This
rapid change from eccentric to concentric contraction
is when the muscle is most vulnerable to injury
(Verrall et al., 2001). The impact on the individual
and the resultant time-off is variable and often
prolonged due to issues surrounding rehabilitation
and recovery. Moreover, the recurrence rate of
injuries is very high, with re-injury occurring in up to
63% of hamstring strains (Brukner et al., 2013). Since
these types of injuries are so common and difficult to
prevent, hamstrings strains have proven to be a
prominent area of research.
Numerous studies have investigated the
relationship between the ratio of hamstring to
quadricep activation and how they relate to injury
occurrence. A systematic review by Opar et al.
investigated a potential relationship between prior
hamstring strain injuries and increased risk of future
anterior cruciate ligament tear (Opar et al., 2014).
One study included in this review looked at the
functional deficits caused by previous hamstring
strains. They found that ‘athletes with a history of
hamstring strain injury displayed lower
hamstrings:quadriceps strength ratio in the previously
injured limb when compared to the uninjured limb.
In 2015, Ardern et al. investigated hamstring
strength imbalances in professional soccer players in
Australia (Ardern et al., 2015). Hamstring strength
tests were performed on 42 players, 24% of which
were discovered to have hamstring strength
imbalances. One of the major findings was that the
strength imbalances were almost invariably found in
the stance leg of athletes. In this paper the researchers
were only assessing the prevalence of hamstring
strength imbalances, whereas further studies go on to
explore this topic in more depth, considering
aetiology and sequelae of strength imbalances.
Bourne et al. aimed to determine if eccentric knee
flexor strength imbalance is a risk factor for
hamstring strain injuries in rugby union (Bourne et
al., 2015). In this prospective cohort study 178 rugby
players had strength tests performed at the start of the
playing season with the primary outcome measure of
Ahmed, A.
Does Prior Hamstring Strain Injury Affect Hamstring Muscle Activation Patterns in Amateur Football Players? A Feasibility Study.
DOI: 10.5220/0010117702170222
In Proceedings of the 8th International Conference on Sport Sciences Research and Technology Support (icSPORTS 2020), pages 217-222
ISBN: 978-989-758-481-7
Copyright
c
2020 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved
217

prospective hamstring strain injuries. The results of
their study showed that a between-limb imbalance in
eccentric knee flexor strength of ≥20% increased the
risk of a hamstring strain 3.4-fold (95% CI, 1.5 -7.6;
p = 0.003). This provides evidence to support the
rational that strength imbalances should be corrected,
particularly in those with previous hamstring strains
to prevent future injury.
A study by Sole et al. investigated EMG activity
of thigh muscles in people with a recent hamstring
injury during a weight bearing exercise (Sole et al.,
2011). They found that EMG onsets of the hamstrings
were significantly earlier in those with a previous
hamstring injury when compared with a control
group. These results indicate that hamstring strains
can effect muscle activation patterns post injury.
The insight gained from a review of the literature
provided the bases for developing a research question
and in choosing methodology. It has already been
shown that prior hamstring strain injury can result in
strength imbalances. This is true when comparing
ipsilateral, injured and contralateral, uninjured sides,
as well as when comparing quadriceps to hamstring
strength ratios on ipsilateral injured side (Opar et al.,
2014; Ardern et al., 2015). Moreover, studies have
shown that an imbalance of strength in antagonistic
muscles of the thigh increased the risk of hamstring
strain injury (Bourne et al., 2015). However, to our
knowledge changes in activation ratios of the
synergistic hamstring muscle group, post-injury has
not been investigated.
Our study will focus on amateur football players
with previous hamstring strain injuries. The aim of
our study is to assess the medial:lateral hamstring
activation ratio in amateur football players during on-
ground walking.
The primary objective is to identify if there is an
association between previous hamstring strain injury
and altered hamstring activation patterns when
comparing medial and lateral hamstrings. We
hypothesise that a prior hamstring strain injury results
in altered medial:lateral activation ratio when
compared to the contralateral uninjured side. It is
hoped that a better understanding of how a hamstring
strain injury affects muscle activation and the
different hamstring groups may lead to lower injuries
and recurrence rates.
2 METHODS
2.1 Sample Size
This study was designed as a feasibility study, with
the aim of determining whether further testing may
be applicable, if a relationship between prior
hamstring strain injury and medial:lateral (M:L)
hamstring activation ratio is observed. As such a
relatively small sample size was used; including only
6 study participants.
2.2 Inclusion & Exclusion Criteria
Criteria were chosen with the aim of limiting
confounding factors and generating a homogenous
sample group. Six, male, amateur level football
players, aged 22 with a history of a unilateral
hamstring strain injury sustained within the previous
24 months were included. Participants were excluded
if they had: a current symptomatic hamstring strain
injury, a history of bilateral hamstring strains or a
history of cardiovascular disease.
2.3 Participant Characteristics
Six amateur football players (from St Bartholomew
and The Royal London 1st XI football team)
volunteered for this study. Players trained once per
week, playing in competitive matches in an amateur
level league twice per week. All participants were 22
year old males with a mean height of 178.7cm ±
3.2cm and an average body mass of 72.35kg ±9.8kg.
All recruited individuals had a history of a unilateral
hamstring strain injury within the previous 24
months. Hamstring strains were self-reported and
defined as an acute onset posterior hamstring pain
that occurred during sprinting and resulted in time off
sport. All participants provided written consent prior
to participating in the study. Ethical approval was
given by the Queen Mary Committee of Research
Ethics. were chosen with the aim of limiting
confounding factors and generating a homogenous
sample group. Six, male, amateur level football
players, aged 22 with a history of a unilateral
hamstring strain injury sustained within the previous
24 months were included. Participants were excluded
if they had: a current symptomatic hamstring strain
injury, a history of bilateral hamstring strains or a
history of cardiovascular disease.
icSPORTS 2020 - 8th International Conference on Sport Sciences Research and Technology Support
218
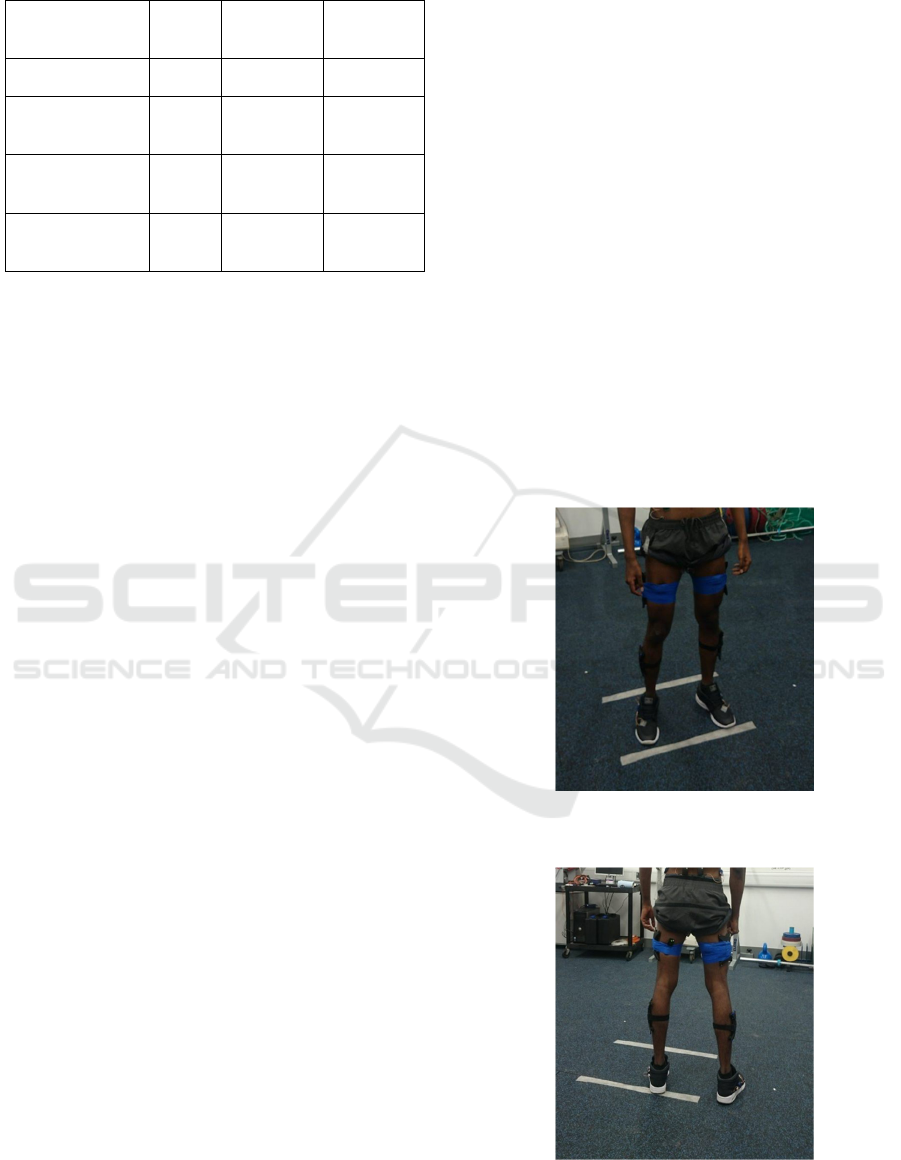
Table 1: Baseline Characteristics of Study Participants.
Characteristic Mean
(±SD)
Minimum
Maximum
Age 22 22
22
Body Mass (kg)
72.35
(±9.8)
60.7
87.6
Height (cm)
178.73
(±3.17)
173.5
183.0
BMI
22.62
(±2.81)
18.7
26.9
2.4 Instrumentation
Surface Electromyography (EMG) data were
collected with DELSYS Trigno Lab Wireless Surface
16 EMG system (16 channel) (DELSYS INC,
Massachusetts, USA). The sampling rate was
2000Hz. Wireless EMG electrodes were applied over
the semitendinosus muscle at the mid-point of the
ischial tuberosity and the medial epicondyle of the
tibia. Electrodes for the biceps femoris muscle were
applied at the mid-point of ischial tuberosity and
lateral epicondyle of the tibia. Electrodes for the
rectus femoris muscle were applied at the mid-point
of the anterior superior iliac spine and the superior
patella. Electrodes were attached using self-adhesive
tape and placement was based on the
recommendations of SENIAM (“The Seniam
Project”, 2020). Raw EMG data was then transferred
to MATLAB (v2009a, Mathworks, Natwick, MA,
USA) where it was filtered rectified and smoothed.
The data from motion analysis was used to
determine ‘Heel Strike ’and ‘Toe Off ’stages of the
gait cycle enabling distinction of the stance and swing
phases of the cycle. This was achieved by mapping
the vertical height of the heel markers and the 5th
metatarsal markers. Kinematics were measured using
a CodaMotion system (Charnwood Dynamics Ltd.,
Leicestershire, United Kingdom). Four CX1 Series
Codamotion 3d Scanners were used to capture the
markers placed on the study subject. Clusters
consisting of four active markers were used on the
lower limbs to minimise marker movement. The
sampling rate was 200Hz. The software used for
measurement and analysis was ODIN Codamotion
3D Modelling & Control Software (v1.05).
2.5 Protocol
Upon arriving at the Human Performance Laboratory,
participants were briefed on proceedings after which
informed consent was given. For each participant
weight, height and age were recorded prior to data
collection. After these baseline measurements, EMG
electrodes were placed onto the relevant muscles. The
medial hamstring EMG data was recorded from the
semitendinosus muscle. The lateral hamstring EMG
data was recorded from the biceps femoris muscle.
The recordings from the previously injured leg will
be compared to the uninjured leg of the individual as
a control. Motion analysis markers were placed
around the subjects pelvis and feet with marker
clusters placed on the lateral aspect of the thighs and
shanks. Once all EMGs and markers were placed,
anatomical landmarks were digitised using a CLSTR-
PTR-02 pointer. The anatomical landmarks digitised
included: lateral femoral epicondyle, lateral
malleolus, medial femoral epicondyle and medial
malleolus (bilaterally).
Figures 1 and 2 below are images of a study
participant post instrumentation setup. They illustrate
the cluster markers on the lateral aspect of the thighs
and shanks bilaterally, and EMG surface electrodes
on the posterior aspect of the thigh.
Figure 1: Study Participant, Post-Instrumentation (Anterior
View).
Figure 2: Study Participant, Post-Instrumentation (Posterior
View).
Does Prior Hamstring Strain Injury Affect Hamstring Muscle Activation Patterns in Amateur Football Players? A Feasibility Study
219
With instrumentation setup complete, participants
were then allowed to familiarise themselves with the
experimental protocol. Participants walked for a
distance of 3 meters without footwear at a self
selected speed to ensure a full gait cycle was
completed. Participants were asked to place their
hands on the alternate shoulder as they walked to
avoid obstruction of marker visibility. This was
repeated 3 times before data collection trials began.
For data collection trials subjects were again asked to
walk for 3 metres at a comfortable speed. This was
repeated until two acceptable trials were obtained.
Criteria for adequate trials was marker visibility
>80% in all markers across a full gait cycle. EMG
data was only analysed from the first full gait cycle
completed during the 3 meter walk with start point
and end point of the gait cycle defined as right foot
‘heel strike ’and left foot ‘toe off ’respectively.
2.6 Statistical Analysis
Data was extracted using Matlab version 9.0
(Mathworks, Inc. Massachusetts, USA). Raw EMG
data was initially processed by application of a notch
filter at 50Hz to remove electrical noise. The signal
was then rectified and smoothed with a 4th order FIR
low-pass filter with a cut off frequency of 10Hz to
produce a ‘linear envelope ’with mean RMS values
calculated. This technique has been used numerous
times in previous studies (Arendt-Nielsen et al., 1991;
Neumann et al., 1996; Ng et al., 1997). EMG data
were taken from the same muscles, on the same day
with subjects acting as their own controls and
comparisons between individuals being made in-
terms of activation ratios. As such, EMG
normalisation was not thought to be necessary
(Soderberg et al., 2000).
The mean root mean square (RMS) for the
processed EMG signals were then calculated for the
stance phase, the swing phase and the complete gait
cycle. Medial:lateral hamstring activations ratio was
defined as the ratio of non-normalised, mean RMS of
EMG wave amplitude between the biceps femoris
and semitendinosus muscles, taken at various stages
of the gait cycle. The primary outcome measure was
mean medial:lateral hamstring activation ratio during
the complete gait cycle. Secondary outcome
measures were medial:lateral ratios during the
‘Stance ’and ‘Swing ’phase. Comparisons were made
between the previously injured legs and control legs
under these three parameters. Student’s independent
two-sided t-test was then carried out to compare data
from previously injured and previously uninjured
(control) legs. Statistical analysis was performed
using SPSS version 17.0 (SPSS Inc, Chicago, IL).
Statistical significance was set at p < 0.05.
3 RESULTS
The inter-subject variation in M:L activity ratios was
relatively high ranging from ratios of 0.66 during
swing phase of the gait cycle to 10.3 in the stance
phase. During the full gait cycle mean hamstring M:L
activation ratios of participants showed very little
discrepancy between previously injured and control
hamstrings, the latter having a lower ratio on average
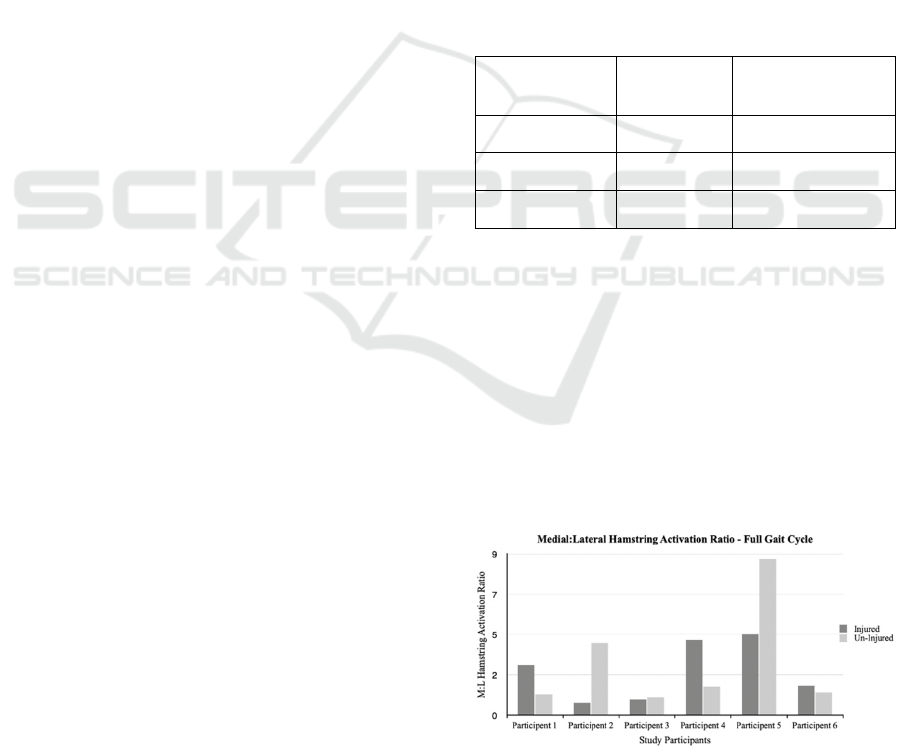
(-0.24 ±2.79). Table 2 illustrates the mean M:L
activity ratios across the gait cycle. Figure 3
graphically represents M:L activation ratios across
the full gait cycle.
Table 2: Mean M:L Hamstring Activation Ratios (±SD)
Across One Complete Gait Cycle.
Injured Side Uninjured (Control)
Side
Stance Phase 2.52 (1.17) 22
Swing Phase 3.10 (2.23)
60.7
Full Gait Cycle 2.54 (1.56)
173.5
Students independent two-sided t test revealed that
there is no significant difference between mean M:L
hamstring activation ratios in hamstrings with prior
strain injuries and previously uninjured hamstrings
across a full gait cycle; t(10)=0.73, p>0.05. There was
no significant difference found between previously
injured and control hamstrings during the stance
phase of the gait cycle. t(10)=0.88, p>0.05.
Moreover, there was no significant difference found
between previously injured and control hamstrings
during the swing phase of the gait cycle; t(10)=0.61,
p>0.05.
Figure 3: Comparing M:L activation ratios of injured
hamstrings vs. controls across a full gait cycle.
icSPORTS 2020 - 8th International Conference on Sport Sciences Research and Technology Support
220

4 DISCUSSION
4.1 Main Findings
The main finding of our study was that there is no
significant difference in hamstring medial:lateral
activation ratios in previously injured hamstrings
compared to non-injured hamstrings. These results
disprove the original research hypothesis. It is
difficult to state whether these results are in keeping
with similar studies as the number of papers
investigating individual hamstring muscle activation
patterns post-injury are very limited. However, a
study by Sole et al. compared EMG activity of gluteal
and thigh muscles of sportspeople with a recent injury
with uninjured controls during a weight-bearing task
(Sole et al, 2011). They found that the EMG onsets of
biceps femoris and medial hamstrings were
significant earlier for the injured group compared to
the control group. Although this study focussed on
EMG onset rather than mean EMG activity, their
results suggest alterations in neuromuscular control
of hamstrings post-injury. Following this, it could be
postulated that injury alters the M:L activity ratios of
hamstrings, which contradicts the findings from our
study.
Emami et al. conducted a study investigating
EMG activity pattern of the lumbo-pelvic muscles
during prone hip extension in athletes with and
without hamstring strain injury (Emami et al., 2014).
Rather than calculating activity ratios, EMG data was
processed and normalised with muscle activity being
expressed as percentage of maximal voluntary
electrical activity (MVE). Their results showed that
there were significant differences in EMG activity of
the gluteus maximus and the medial hamstring
between the injured group and the control group.
However, no significant difference was found in
activity of the lateral hamstring between the two
groups. This would suggest that a previous hamstring
injury will alter the medial:lateral hamstring
activation ratio. This again is not in keeping with the
results of our study.
4.2 Limitations
One of the major limitations to this study was the
small sample size. Adequate sample sizes ensure high
statical power in null hypothesis testing (Liu et al.,
2013). Access to the target population of male
amateur football players with a unilateral hamstring
strain injury occurring in the past 2 years was limited
within the time frame that this study was conducted.
Future work on this topic should be carried out on a
larger scale to further assess the link between
hamstring strain and muscle activation patterns.
Another limitation to this study was the self-
reported nature of the injuries. Gabbe et al.
investigated the validity of self reported sports injury
histories. (Gabbe et al., 2003). Their results showed
that at 12 months post-injury 80% of participants
were able to accurately recall the body regions
injured, but not the exact diagnosis, with only 61% of
participants able to recall the exact body region and
diagnosis of injury sustained. Participants of this
study were included if they had sustained a hamstring
strain any time in the past 24 months. As such details
on the injury including severity, and exact location
had a decreased validity due to probable recall bias.
The inclusion criteria specified only male subjects
could be recruited. This criterion was chosen because
of the different neuromuscular control strategies and
movement patterns in women including lower
hamstring muscle activation (Malinzak et al., 2001).
As such, a limitation to this study is that the findings
are not transferable and can not be applied to females.
Furthermore, EMG data collected in our study
was not normalised. Normalisation was not necessary
for this study and non-normalised signals allowed us
to answer the research question. However this is a
weakness to our study as it limits comparability of our
results to similar studies using normalised EMG
signals.
4.3 Future Work
Future studies could investigate how strain injuries of
the different hamstring components lead to different
physiological response of the hamstrings. It has
previously been suggested that following hamstring
strain the biceps femoris compensates for the lack of
endurance capacity of the semitendinosus, increasing
the re-injury risk (Schuermans et al., 2014).
Furthermore, Opar et al. recently showed that
previously strained hamstrings show less
improvement in eccentric strength following a
training programme when compared to uninjured
hamstrings (Opar et al., 2014). However, it is not
clear whether this is the cause of or the result of the
injury. This is another aspect of this topic that has
potential to be investigated in the future. Fully
understanding the biomechanics and neuromuscular
response following hamstring strain injury is
necessary before prevention and rehabilitation
techniques can be improved. The potential benefits of
research in this area to lower rehabilitation time and
re-injury rates, resulting in less time-off sport.
Does Prior Hamstring Strain Injury Affect Hamstring Muscle Activation Patterns in Amateur Football Players? A Feasibility Study
221

4.4 Conclusion
To conclude, previous hamstring strain injuries do not
result in a significantly different medial:lateral
hamstring activation ratio when compared with
uninjured hamstrings. This is true for both ‘Stance
phase ’and “Swing phase ’of gait cycle as well as
across the entire gait cycle. However, due to various
limitations of this study, further research on this topic
is needed to comprehensively establish the
association between between previous hamstring
injury and medial:lateral hamstring activation ratios.
REFERENCES
Ekstrand, J., Hagglund, M. and Walden, M., 2009. Injury
incidence and injury patterns in professional football:
the UEFA injury study. British Journal of Sports
Medicine, 45(7), pp.553-558.
Chumanov E, Heiderscheit B, Thelen D. The effect of speed
and influence of individual muscles on hamstring
mechanics during the swing phase of sprinting. Journal
of Biomechanics 2007;40(16):3555-3562.
Thelen D, Chumanov E, Best T, et al. Simulation of biceps
femoris musculotendon mechanics during the swing
phase of sprinting. Medicine & Science in Sports &
Exercise 2005;37(11):1931-1938.
Verrall GM, Slavotinek JP, Barnes PG, et al. Clinical risk
factors for hamstring
muscle strain injury: a prospective study with correlation of
injury by magnetic
resonance imaging. British Journal of Sports Medicine
2001;35:435–40.
Brukner P, Nealon A, Morgan C, et al. Recurrent hamstring
muscle injury: applying the limited evidence in the
professional football setting with a seven-point
programme. British Journal of Sports Medicine
2013;48(11):929-938.
Opar D, Serpell B. Is there a potential relationship between
prior hamstring strain injury and increased risk for
future anterior cruciate ligament injury?. Archives of
Physical Medicine and Rehabilitation 2014;95(2):401-
405.
Ardern C, Pizzari T, Wollin M, et al. Hamstrings strength
imbalance in professional football (soccer) players in
Australia. Journal of Strength and Conditioning
Research 2015;29(4):997-1002.
Bourne M, Opar D, Williams M, et al. Eccentric knee flexor
strength and risk of hamstring injuries in rugby union:
A prospective study. The American Journal of Sports
Medicine 2015;43(11):2663-2670.
Sole G, Milosavljevic S, Nicholson H, et al. Altered muscle
activation following hamstring injuries. British Journal
of Sports Medicine 2011;46(2):118-123.
The SENIAM Project [Internet]. SENIAM. 2000 [cited 17
May 2016]. Available from: http://www.seniam.org
Arendt-Nielsen L, Sinkjaer T, Nielsen J, et al.
Electromyographic patterns and knee joint kinematics
during walking at various speeds. Journal
Electromyography and Kinesiology 1991;1:89–95.
Neumann DA. Hip abductor muscle activity in persons with
a hip prosthesis while carrying loads in one hand.
Journal of The American Physical Therapy Association
1996;76:1320–1330.
Ng JK, Richardson CA, Jull GA. Electromyographic
amplitude and frequency changes in the iliocostalis
lumborum and multifidus muscles during a trunk
holding test. Journal of The American Physical
Therapy Association 1997;77:954–961.
Soderberg GL, Knutson LM. A guide for use and
interpretation of kinesiologic electromyographic data.
Journal of The American Physical Therapy Association
2000;80(5), 485-498.
Emami M, Arab AM, Ghamkhar L. The activity pattern of
the lumbo‐ pelvic muscles during prone hip extension
in athletes with and without hamstring strain injury.
International Journal of Sports Physical Therapy
2014;9(3):312-319.
Liu X. Comparing sample size requirements for
significance tests and confidence intervals. Counseling
Outcome Research and Evaluation 2013;4(1):3-12.
Gabbe B, Finch CF, Bennell KL, et al. How valid is a self
reported 12 month sports injury history?. British
Journal of Sports Medicine 2003;37(6):545-547.
Malinzak R, Colby S, Kirkendall D, et al. A comparison of
knee joint motion patterns between men and women in
selected athletic tasks. Clinical Biomechanics
2001;16(5):438-445.
Schuermans J, Van Tiggelen D, Danneels L, et al. Biceps
femoris and semitendinosus-teammates or competitors?
New insights into hamstring injury mechanisms in male
football players: a muscle functional MRI study. British
Journal of Sports Medicine 2014;48(22):1599-1606.
Opar D, Williams M, Timmins R, et al. The effect of
previous hamstring strain injuries on the change in
eccentric hamstring strength during preseason training
in elite australian footballers. The American Journal of
Sports Medicine 2014;43(2):377-384.
icSPORTS 2020 - 8th International Conference on Sport Sciences Research and Technology Support
222
